
The Role of Nintedanib in the Treatment of Progressive Pulmonary Fibrosis of Autoimmune-Related Interstitial Lung Disease


Abstract
:1. Introduction
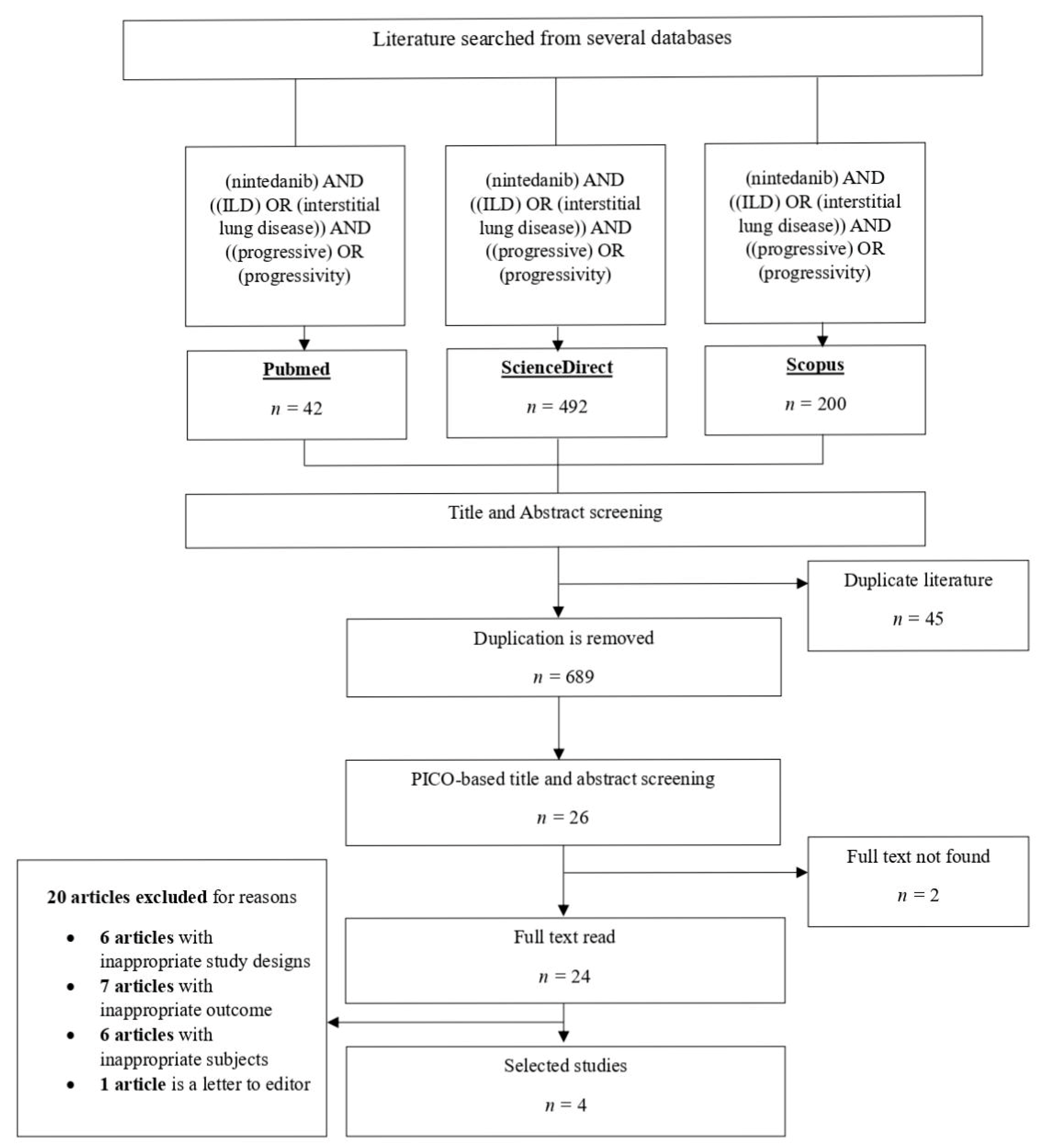
2. Method
3. Result
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Antoine, M.; Mlika, M. Interstitial Lung Disease; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK541084/ (accessed on 27 June 2022).
- Gulati, M. Diagnostic assessment of patients with interstitial lung disease. Prim. Care Respir. J. 2011, 20, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Cheesma, G.S.; Quismorio, F.P. Interstitial lung disease in systemic lupus erythematosus. Curr. Opin. Pulm. Med. 2000, 6, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Remy-Jardin, M.; Richeldi, L.; Thomson, C.C.; Inoue, Y.; Johkoh, T.; Kreuter, M.; Lynch, D.A.; Maher, T.M.; Martinez, F.J.; et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: An official ATS/ERS/JRS/ALAT clinical practice guideline. Am. J. Respir. Crit. Care Med. 2022, 205, e18–e47. [Google Scholar] [CrossRef] [PubMed]
- Richeldi, L.; Varone, F.; Bergna, M.; de Andrade, J.; Falk, J.; Hallowell, R.; Jouneau, S.; Kondoh, Y.; Morrow, L.; Randerath, W.; et al. Pharmacological management of progressive-fibrosing interstitial lung diseases: A review of the current evidence. Eur. Respir. Rev. 2018, 27, 180074. [Google Scholar] [CrossRef] [PubMed]
- Kondoh, Y.; Taniguchi, H.; Yokoi, T.; Nishiyama, O.; Ohishi, T.; Kato, T.; Suzuki, K.; Suzuki, R. Cyclophosphamide and low-dose prednisolone in idiopathic pulmonary fibrosis and fibrosing nonspecific interstitial pneumonia. Eur. Respir. J. 2005, 25, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Johannson, K.A.; Chaudhuri, N.; Adegunsoye, A.; Wolters, P.J. Treatment of fibrotic interstitial lung disease: Current approaches and future directions. Lancet 2021, 398, 1450–1460. [Google Scholar] [CrossRef] [PubMed]
- Wind, S.; Schmid, U.; Freiwald, M.; Marzin, K.; Lotz, R.; Ebner, T.; Stopfer, P.; Dallinger, C. Clinical pharmacokinetics and pharmacodynamics of nintedanib. Clin. Pharmacokinet. 2019, 58, 1131–1147. [Google Scholar] [CrossRef]
- Wollin, L.; Distler, J.H.W.; Redente, E.F.; Riches, D.W.H.; Stowasser, S.; Schlenker-Herceg, R.; Maher, T.M.; Kolb, M. Potential of nintedanib in treatment of progressive fibrosing interstitial lung diseases. Eur. Respir. J. 2019, 54, 1900161. [Google Scholar] [CrossRef]
- Matteson, E.L.; Kelly, C.; Distler, J.H.; Hoffmann-Vold, A.M.; Seibold, J.R.; Mittoo, S.; Dellaripa, P.F.; Aringer, M.; Pope, J.; Distler, O.; et al. Nintedanib in patients with autoimmune disease–related progressive fibrosing interstitial lung diseases: Subgroup analysis of the inbuild trial. Arthritis Rheumatol. 2022, 74, 1039–1047. [Google Scholar] [CrossRef]
- Highland, K.B.; Distler, O.; Kuwana, M.; Allanore, Y.; Assassi, S.; Azuma, A.; Bourdin, A.; Denton, C.P.; Distler, J.H.; Hoffmann-Vold, A.M.; et al. Efficacy and safety of nintedanib in patients with systemic sclerosis-associated interstitial lung disease treated with mycophenolate: A subgroup analysis of the SENSCIS trial. Lancet Respir. Med. 2021, 9, 96–106. [Google Scholar] [CrossRef]
- Kuwana, M.; Ogura, T.; Makino, S.; Homma, S.; Kondoh, Y.; Saito, A.; Ugai, H.; Gahlemann, M.; Takehara, K.; Azuma, A. Nintedanib in patients with systemic sclerosis-associated interstitial lung disease: A Japanese population analysis of the SENSCIS trial. Mod. Rheumatol. 2021, 31, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Azuma, A.; Chung, L.; Behera, D.; Chung, M.; Kondoh, Y.; Ogura, T.; Okamoto, M.; Swarnakar, R.; Zeng, X.; Zou, H.; et al. Efficacy and safety of nintedanib in Asian patients with systemic sclerosis-associated interstitial lung disease: Subgroup analysis of the SENSCIS trial. Respir. Investig. 2021, 59, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Ponce, M.C.; Sharma, S. Pulmonary Function Tests; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK482339/ (accessed on 27 June 2022).
- Ranu, H.; Wilde, M.; Madden, B. Pulmonary function tests. Ulster Med. J. 2011, 80, 84–90. [Google Scholar] [PubMed]
- Flaherty, K.R.; Kolb, M.; Vancheri, C.; Tang, W.; Conoscenti, C.S.; Richeldi, L. Stability or improvement in forced vital capacity with nintedanib in patients with idiopathic pulmonary fibrosis. ERJ 2018, 52, 1702593. [Google Scholar] [CrossRef] [PubMed]
- Lamb, Y.N. Nintedanib: A review in fibrotic interstitial lung diseases. Drugs 2021, 81, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Allison, A.C.; Eugui, E.M. Mycophenolate mofetil and its mechanisms of action. Int. Immunopharmacol. 2000, 47, 85–118. [Google Scholar] [CrossRef] [PubMed]
- Gensler, L.S. Glucocorticoids: Complications to anticipate and prevent. Neurohospitalist 2013, 3, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Seibold, J.R.; Maher, T.M.; Highland, K.B.; Assassi, S.; Azuma, A.; Hummers, L.K.; Costabel, U.; Von Wangenheim, U.; Kohlbrenner, V.; Gahlemann, M.; et al. Safety and tolerability of nintedanib in patients with systemic sclerosis-associated interstitial lung disease: Data from the SENSCIS trial. Ann. Rheum. Dis. 2020, 79, 1478–1484. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Patient/Problem (P) | Intervention (I) | Comparison (C) | Outcome (O) |
|---|---|---|---|
| Patients with autoimmune disease and proven ILD | Nintedanib | Placebo/none | ILD progression |
| Type of clinical question | Therapy | ||
| Study design | RCT, systematic review and/or meta-analysis | ||
| Database | Search Strategy | Results |
|---|---|---|
| PubMed | (nintedanib) AND ((ILD) OR (interstitial lung disease)) AND ((progressive) OR (progressivity)) | 42 |
| ScienceDirect | (nintedanib) AND ((ILD) OR (interstitial lung disease)) AND ((progressive) OR (progressivity)) | 492 |
| Scopus | (nintedanib) AND ((ILD) OR (interstitial lung disease)) AND ((progressive) OR (progressivity)) | 200 |
| Author (Year) | Study Design | Population | Intervention | Outcome | Results | |
|---|---|---|---|---|---|---|
| Matteson E.L., Kelly C., Distler J.H.W., Seibold J.R., Mittoo S. et al., (2022) | Randomized controlled trial | Patients with a fibrosing autoimmune-disease-related interstitial lung disease (ILD) | I: patients who received nintedanib 150 mg twice a day C: patients who received placebo | Rate of decline in FVC and adverse events over 52 weeks in the subgroup with autoimmune-disease-related ILDs |
| |
| Highland K.B., Distler O., Kuwana M., Allanore Y., Assassi S et al., (2021) | Randomized controlled trial | Patients aged 18 years or older with systemic-sclerosis-associated interstitial lung disease (SSc-ILD) and onset of first non-Raynaud’s symptom less than 7 years prior to study | I: patients who received 150 mg of oral nintedanib twice daily C: patients who received placebo | The rate of decline in FVC over 52 weeks according to mycophenolate use at baseline |
| |
| Kuwana M., Ogura T., Makino S., Homma S., Kondoh Y. et al., (2020) | Randomized controlled trial | Patients from Japan aged 20 years or older and patients from other countries aged 18 years or older who had a diagnosis of SSc, onset of the first non-Raynaud’s symptom within 7 years prior to study, >10% lung fibrosis within 12 months FVC > 40% and diffusion capacity of lung for carbon monoxide | I: patients who received oral nintedanib 150 mg twice daily C: patients who received placebo | Efficacy and safety of nintedanib in Japanese patients with systemic-sclerosis-associated interstitial lung disease (SSc-ILD) |
| |
| Azuma A., Chung L., Behera D., Chung M., Kondoh Y. et al., (2021) | Randomized controlled trial | SSc patient with onset of first non-Raynaud’s symptom less than 7 years prior to study and extent of fibrotic ILD > 10% | I: patients who received nintedanib 150 mg twice daily C: patients who received placebo | Efficacy and safety of nintedanib in patients of Asian race |
|
| Questions | Matteson E.L., Kelly C., Distler J.H.W., Seibold J.R., Mittoo S. et al., (2022) | Highland K.B., Distler O., Kuwana M., Allanore Y., Assassi S. et al., (2021) | Kuwana M., Ogura T., Makino S., Homma S., Kondoh Y. et al., (2020) | Azuma A., Chung L., Behera D., Chung M., Kondoh Y. et al., (2021) |
|---|---|---|---|---|
| Was the assignment of patient to treatments randomised? | Yes | Yes | Yes | Yes |
| Were the groups similar at the start of the trial? | Yes | Yes | Yes | Yes |
| Aside from the allocated treatment, were groups treated equally? | Yes | Yes | Yes | Yes |
| Were all patients who entered the trial accounted for? And were they analysed in the group which they were randomised? | Unclear | No | Yes | Yes |
| Were measures objective or were the patients and clinicians kept “blind” to which treatment was being received? | Yes | Yes | Yes | Yes |
| Questions | Matteson E.L., Kelly C., Distler J.H.W., Seibold J.R., Mittoo S. et al., (2022) | Highland K.B., Distler O., Kuwana M., Allanore Y., Assassi S. et al., (2021) | Kuwana M., Ogura T., Makino S., Homma S., Kondoh Y. et al., (2020) | Azuma A., Chung L., Behera D., Chung M., Kondoh Y. et al., (2021) |
|---|---|---|---|---|
| Is my patient so different to those in the study that the results cannot apply? | No | No | No | No |
| Is the treatment feasible in my setting? | Yes | Yes | Yes | Yes |
| Will the potential benefits of treatment outweigh the potential harms of treatment for my patient? | Yes | Yes | Yes | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ardan, A.R.; Nurwidya, F. The Role of Nintedanib in the Treatment of Progressive Pulmonary Fibrosis of Autoimmune-Related Interstitial Lung Disease. J. Respir. 2023, 3, 200-207. https://doi.org/10.3390/jor3040019
Ardan AR, Nurwidya F. The Role of Nintedanib in the Treatment of Progressive Pulmonary Fibrosis of Autoimmune-Related Interstitial Lung Disease. Journal of Respiration. 2023; 3(4):200-207. https://doi.org/10.3390/jor3040019
Chicago/Turabian StyleArdan, Aulia Rahman, and Fariz Nurwidya. 2023. "The Role of Nintedanib in the Treatment of Progressive Pulmonary Fibrosis of Autoimmune-Related Interstitial Lung Disease" Journal of Respiration 3, no. 4: 200-207. https://doi.org/10.3390/jor3040019
APA StyleArdan, A. R., & Nurwidya, F. (2023). The Role of Nintedanib in the Treatment of Progressive Pulmonary Fibrosis of Autoimmune-Related Interstitial Lung Disease. Journal of Respiration, 3(4), 200-207. https://doi.org/10.3390/jor3040019