
Prevalence of Lumbosacral Transition Vertebrae in Symptomatic Adults and the Levels of Degeneration in the Suprajacent Disc


Abstract
1. Introduction
2. Material and Methods
3. Results
4. Discussion
4.1. Prevalence of LSTV
4.2. Degeneration of the Disc Compared to the Suprajacent Disc
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- French, H.D.; Somasundaram, A.J.; Schaefer, N.R.; Laherty, R.W. Lumbosacral transitional vertebrae and its prevalence in the Australian population. Glob. Spine J. 2014, 4, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Konin, G.P.; Walz, D.M. Lumbosacral transitional vertebrae: Classification, imaging findings, and clinical relevance. AJNR Am. J. Neuroradiol. 2010, 31, 1778–1786. [Google Scholar] [CrossRef] [PubMed]
- Castellvi, A.E.; Goldstein, L.A.; Chan, D.P. Lumbosacral transitional vertebrae and their relationship with lumbar extradural defects. Spine 1984, 9, 493–495. [Google Scholar] [CrossRef] [PubMed]
- Bron, J.L.; van Royen, B.J.; Wuisman, P.I. The clinical significance of lumbosacral transitional anomalies. Acta Orthop. Belg. 2007, 73, 687–695. [Google Scholar]
- Nevalainen, M.T.; McCarthy, E.; Morrison, W.B.; Zoga, A.C.; Roedl, J.B. Lumbosacral transitional vertebrae: Significance of local bone marrow edema at the transverse processes. Skelet. Radiol. 2018, 47, 1145–1149. [Google Scholar] [CrossRef]
- Paik, N.C.; Lim, C.S.; Jang, H.S. Numeric and morphological verification of lumbosacral segments in 8280 consecutive patients. Spine 2013, 38, E573–E578. [Google Scholar] [CrossRef]
- Apazidis, A.; Ricart, P.A.; Diefenbach, C.M.; Spivak, J.M. The prevalence of transitional vertebrae in the lumbar spine. Spine J. 2011, 11, 858–862. [Google Scholar] [CrossRef]
- Tang, M.; Yang, X.F.; Yang, S.W.; Han, P.; Ma, Y.M.; Yu, H.; Zhu, B. Lumbosacral transitional vertebra in a population-based study of 5860 individuals: Prevalence and relationship to low back pain. Eur. J. Radiol. 2014, 83, 1679–1682. [Google Scholar] [CrossRef]
- Hughes, R.J.; Saifuddin, A. Numbering of lumbosacral transitional vertebrae on MRI: Role of the iliolumbar ligaments. AJR Am. J. Roentgenol. 2006, 187, W59–W65. [Google Scholar] [CrossRef]
- Wigh, R.E.; Anthony, H.F., Jr. Transitional lumbosacral discs. probability of herniation. Spine 1981, 6, 168–171. [Google Scholar] [CrossRef]
- Hanhivaara, J.; Maatta, J.H.; Niinimaki, J.; Nevalainen, M.T. Lumbosacral transitional vertebrae are associated with lumbar degeneration: Retrospective evaluation of 3855 consecutive abdominal CT scans. Eur. Radiol. 2020, 30, 3409–3416. [Google Scholar] [CrossRef]
- Luoma, K.; Vehmas, T.; Raininko, R.; Luukkonen, R.; Riihimaki, H. Lumbosacral transitional vertebra: Relation to disc degeneration and low back pain. Spine 2004, 29, 200–205. [Google Scholar] [CrossRef]
- Farshad-Amacker, N.A.; Herzog, R.J.; Hughes, A.P.; Aichmair, A.; Farshad, M. Associations between lumbosacral transitional anatomy types and degeneration at the transitional and adjacent segments. Spine J. 2015, 15, 1210–1216. [Google Scholar] [CrossRef]
- Vergauwen, S.; Parizel, P.M.; van Breusegem, L.; Van Goethem, J.W.; Nackaerts, Y.; Van den Hauwe, L.; De Schepper, A.M. Distribution and incidence of degenerative spine changes in patients with a lumbo-sacral transitional vertebra. Eur. Spine J. 1997, 6, 168–172. [Google Scholar] [CrossRef]
- Aihara, T.; Takahashi, K.; Ogasawara, A.; Itadera, E.; Ono, Y.; Moriya, H. Intervertebral disc degeneration associated with lumbosacral transitional vertebrae: A clinical and anatomical study. J. Bone Jt. Surg. Br. 2005, 87, 687–691. [Google Scholar] [CrossRef]
- Sekharappa, V.; Amritanand, R.; Krishnan, V.; David, K.S. Lumbosacral transition vertebra: Prevalence and its significance. Asian Spine J. 2014, 8, 51–58. [Google Scholar] [CrossRef]
- Pfirrmann, C.W.; Metzdorf, A.; Zanetti, M.; Hodler, J.; Boos, N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine 2001, 26, 1873–1878. [Google Scholar] [CrossRef]
- Griffith, J.F.; Wang, Y.X.; Antonio, G.E.; Choi, K.C.; Yu, A.; Ahuja, A.T.; Leung, P.C. Modified Pfirrmann grading system for lumbar intervertebral disc degeneration. Spine 2007, 32, E708–E712. [Google Scholar] [CrossRef]
- Miyazaki, M.; Hong, S.W.; Yoon, S.H.; Morishita, Y.; Wang, J.C. Reliability of a magnetic resonance imaging-based grading system for cervical intervertebral disc degeneration. J. Spinal Disord. Tech. 2008, 21, 288–292. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 2016, 20, 37–46. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Park, C.M.; Kim, K.A.; Hong, S.J.; Seol, H.Y.; Kim, B.H.; Kim, J.H. Identification and prediction of transitional vertebrae on imaging studies: Anatomical significance of paraspinal structures. Clin. Anat. 2007, 20, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Malanga, G.A.; Cooke, P.M. Segmental anomaly leading to wrong level disc surgery in cauda equina syndrome. Pain Physician 2004, 7, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Ucar, D.; Ucar, B.Y.; Cosar, Y.; Emrem, K.; Gumussuyu, G.; Mutlu, S.; Mutlu, B.; Cacan, M.A.; Mertsoy, Y.; Gumus, H. Retrospective cohort study of the prevalence of lumbosacral transitional vertebra in a wide and well-represented population. Arthritis 2013, 2013, 461425. [Google Scholar] [CrossRef]
- Gopalan, B.; Yerramshetty, J.S. Lumbosacral Transitional Vertebra-Related Low Back Pain: Resolving the Controversy. Asian Spine J. 2018, 12, 407–415. [Google Scholar] [CrossRef]
- Ravikanth, R.; Majumdar, P. Bertolotti’s syndrome in low-backache population: Classification and imaging findings. Ci Ji Yi Xue Za Zhi 2019, 31, 90–95. [Google Scholar] [CrossRef]
- Daniel, P.; Joel, J.J.; Rana, P. Lumbosacral transitional vertebrae in patients with low back pain: Radiological classification and morphometric analysis. J. Anat. Soc. 2019, 68, 123–128. [Google Scholar] [CrossRef]
- Nakagawa, T.; Hashimoto, K.; Tsubakino, T.; Hoshikawa, T.; Inawashiro, T.; Tanaka, Y. Lumbosacral Transitional Vertebrae Cause Spinal Level Misconception in Surgeries for Degenerative Lumbar Spine Disorders. Tohoku J. Exp. Med. 2017, 242, 223–228. [Google Scholar] [CrossRef]
- Landauer, F.; Trieb, K. Diagnostic Limitations and Aspects of the Lumbosacral Transitional Vertebrae (LSTV). Appl. Sci. 2022, 12, 830. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Descriptive Statistics * |
|---|---|
| Number of Patients | 545 |
| Age (years) | 57.6 ± 18.3 |
| BMI (kg/m2) | 26.0 ± 5.3 |
| Gender | |
| Male | 277 (50.8%) |
| Female | 268 (49.2%) |
| Race | |
| Chinese | 420 (77.1%) |
| Malay | 40 (7.3%) |
| Indian | 37 (6.8%) |
| Others | 48 (8.8%) |
| Presence of LSTV | 106 (19.4%) |
| Male | 61 (58%) |
| Female | 45 (42%) |
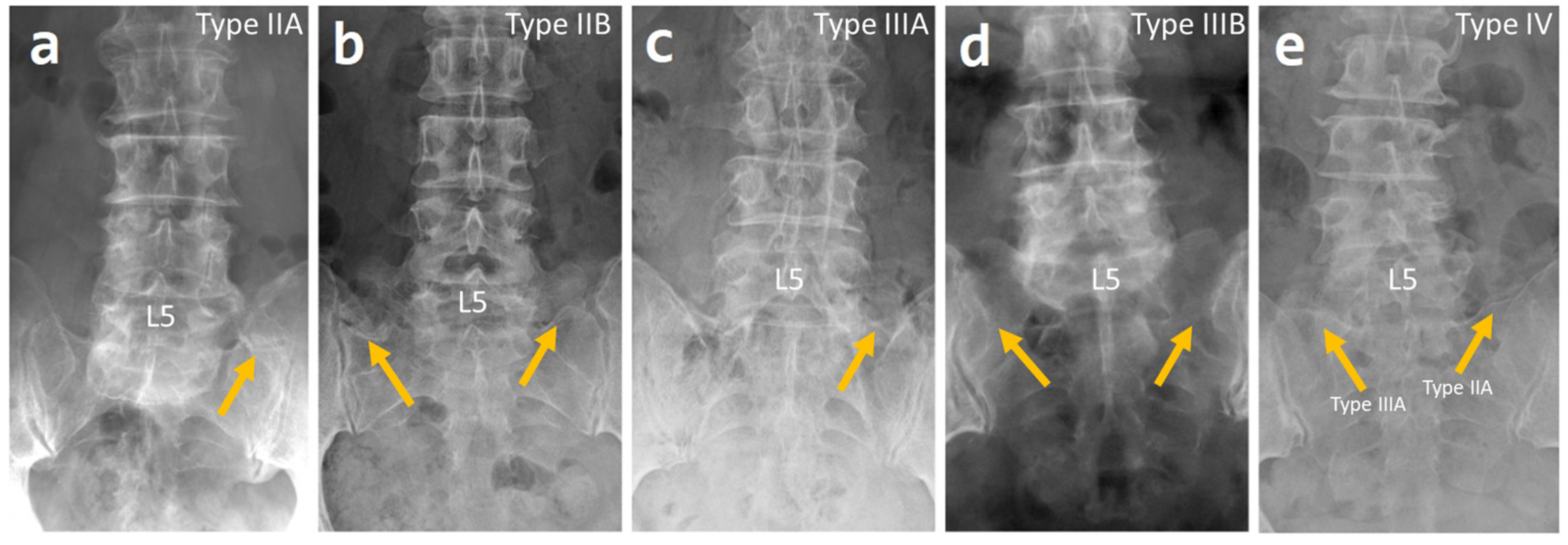
| Castellvi Classification | |
| Type IIA | 46 (44%) |
| Type IIB | 17 (16%) |
| Type IIIA | 9 (8.3%) |
| Type IIIB | 30 (27.5%) |
| Type IV | 4 (3.7%) |
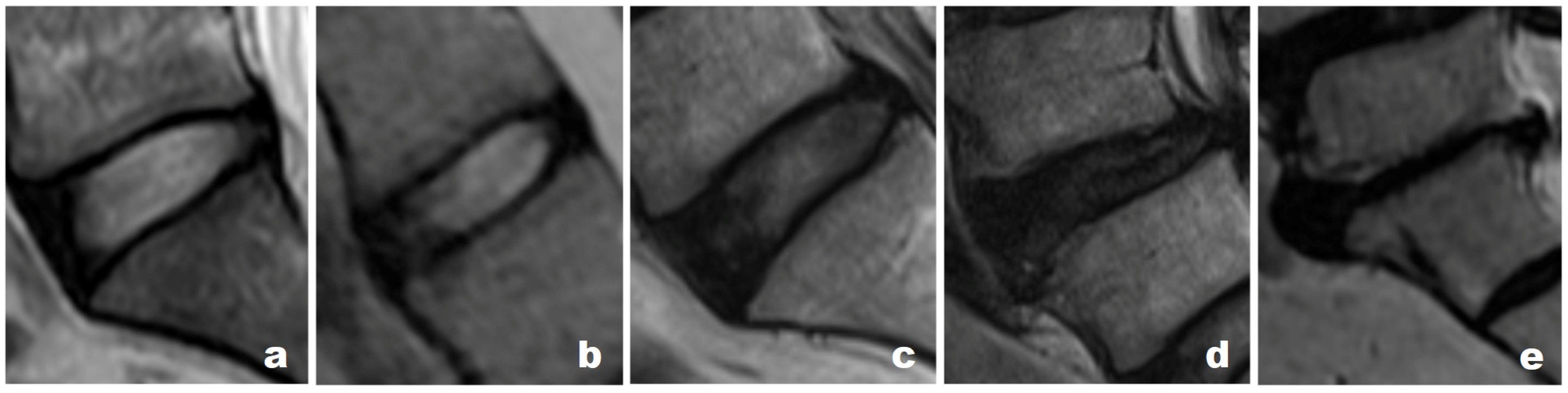
| Pfirrmann grading at LSTV level (n = 106) | |
| Grade II | 3 (3%) |
| Grade III | 26 (25%) |
| Grade IV | 67 (63%) |
| Grade V | 10 (9%) |
| Pfirrmann Grading | Number of Patients as per Pfirrmann Grading * | Statistical Significance (p) c | |
|---|---|---|---|
| LSTV Patients a (n = 106) | Non-LSTV Patients b (n = 439) | ||
| Grade I | 0 (0%) | 2 (0.5%) | 1 |
| Grade II | 1 (1%) | 31 (7%) | 0.01 |
| Grade III | 16 (15%) | 121(28%) | 0.008 |
| Grade IV | 82 (77%) | 275 (63%) | 0.004 |
| Grade V | 7 (7%) | 10 (2%) | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, J.; Betzler, B.K.; Kaliya-Perumal, A.-K.; Oh, J.Y.-L. Prevalence of Lumbosacral Transition Vertebrae in Symptomatic Adults and the Levels of Degeneration in the Suprajacent Disc. Surgeries 2023, 4, 120-126. https://doi.org/10.3390/surgeries4010013
Song J, Betzler BK, Kaliya-Perumal A-K, Oh JY-L. Prevalence of Lumbosacral Transition Vertebrae in Symptomatic Adults and the Levels of Degeneration in the Suprajacent Disc. Surgeries. 2023; 4(1):120-126. https://doi.org/10.3390/surgeries4010013
Chicago/Turabian StyleSong, Joshua, Brjan Kaiji Betzler, Arun-Kumar Kaliya-Perumal, and Jacob Yoong-Leong Oh. 2023. "Prevalence of Lumbosacral Transition Vertebrae in Symptomatic Adults and the Levels of Degeneration in the Suprajacent Disc" Surgeries 4, no. 1: 120-126. https://doi.org/10.3390/surgeries4010013
APA StyleSong, J., Betzler, B. K., Kaliya-Perumal, A.-K., & Oh, J. Y.-L. (2023). Prevalence of Lumbosacral Transition Vertebrae in Symptomatic Adults and the Levels of Degeneration in the Suprajacent Disc. Surgeries, 4(1), 120-126. https://doi.org/10.3390/surgeries4010013