
Current Status of Digital Complete Dentures Technology


 ,
, 
Abstract
:1. Introduction
1.1. Digitally Produced Dentures
1.2. Comparing the Additive vs. the Subtractive Method
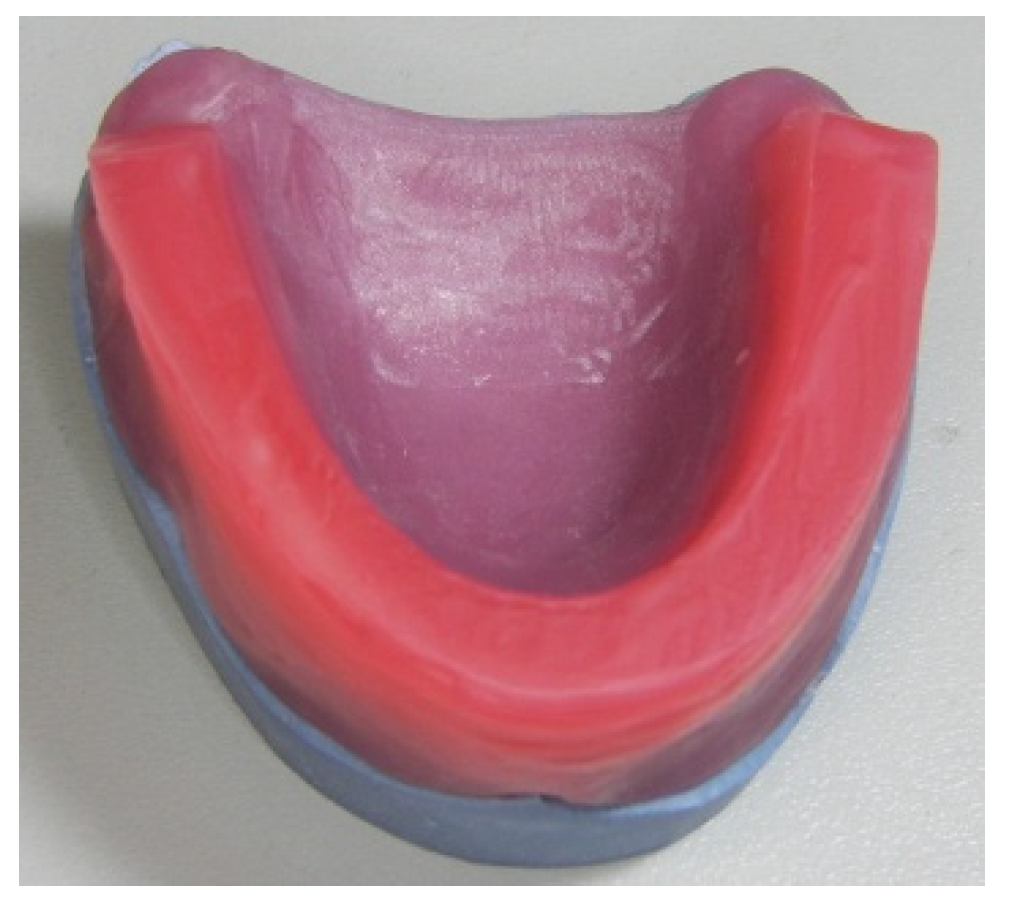
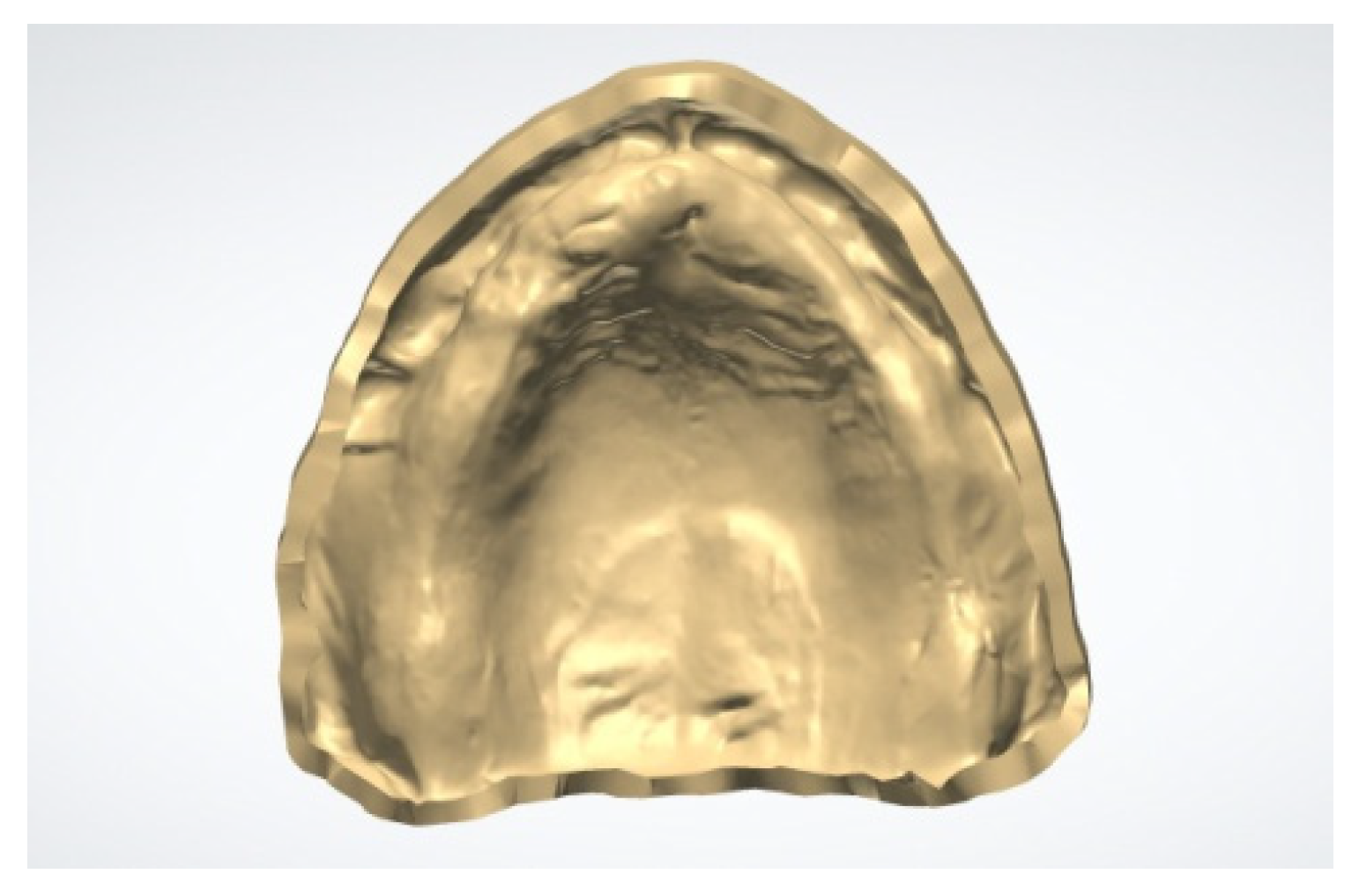
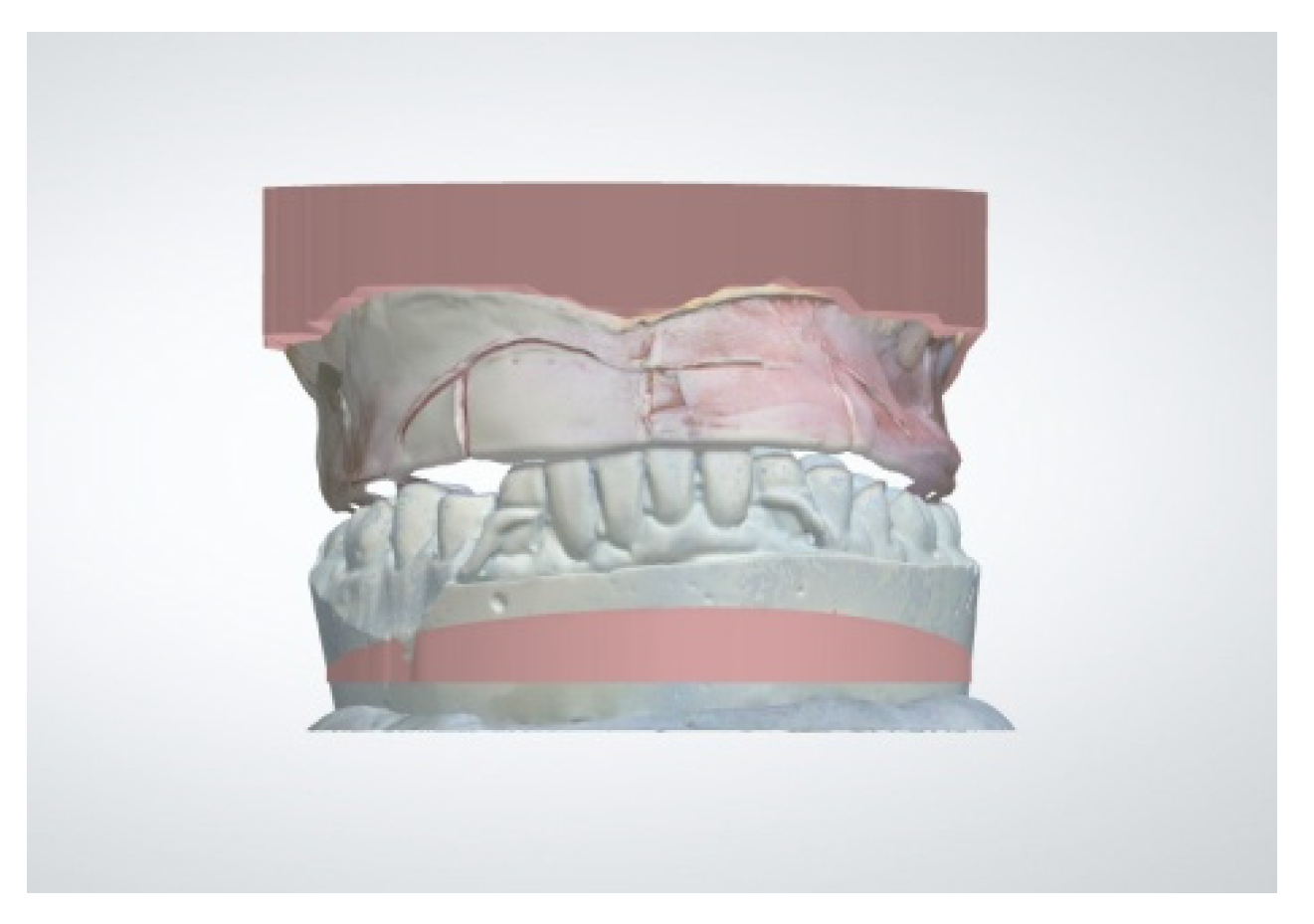
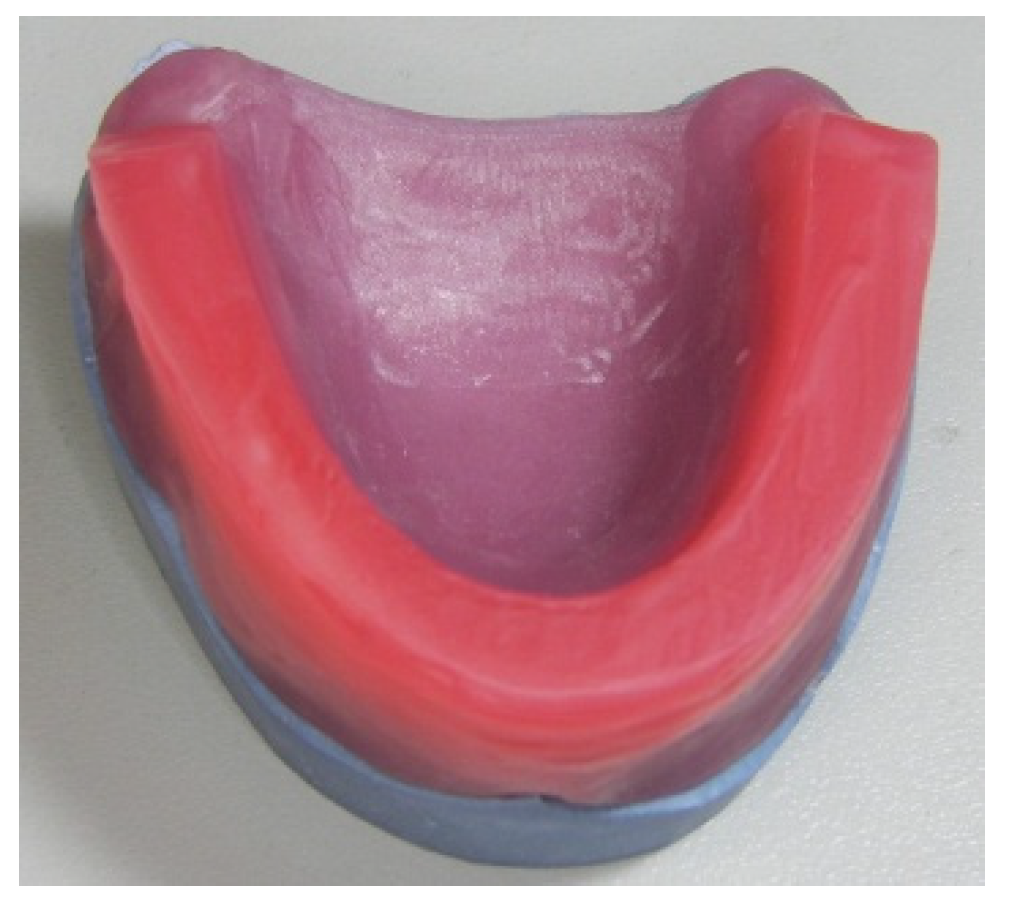
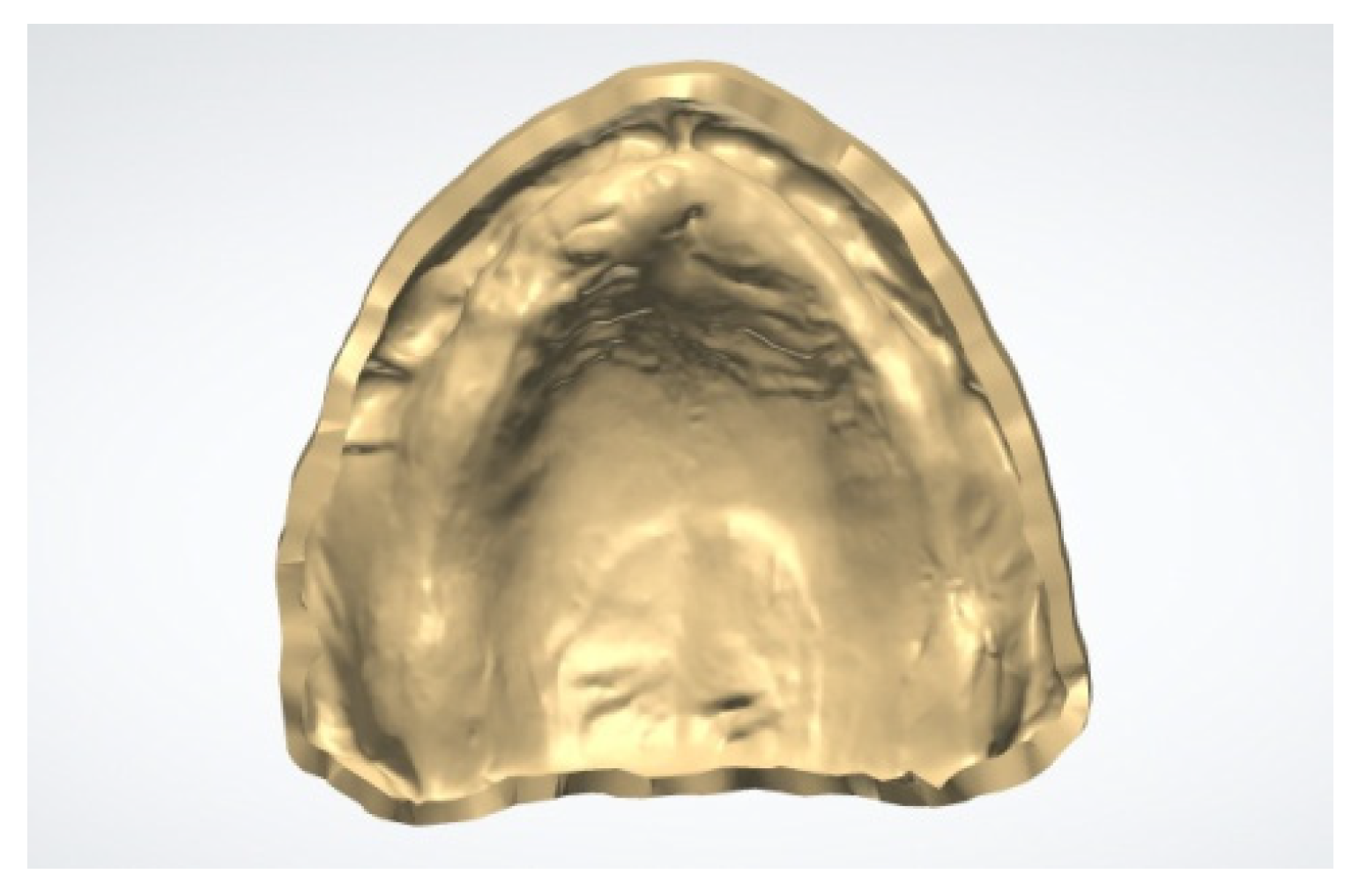
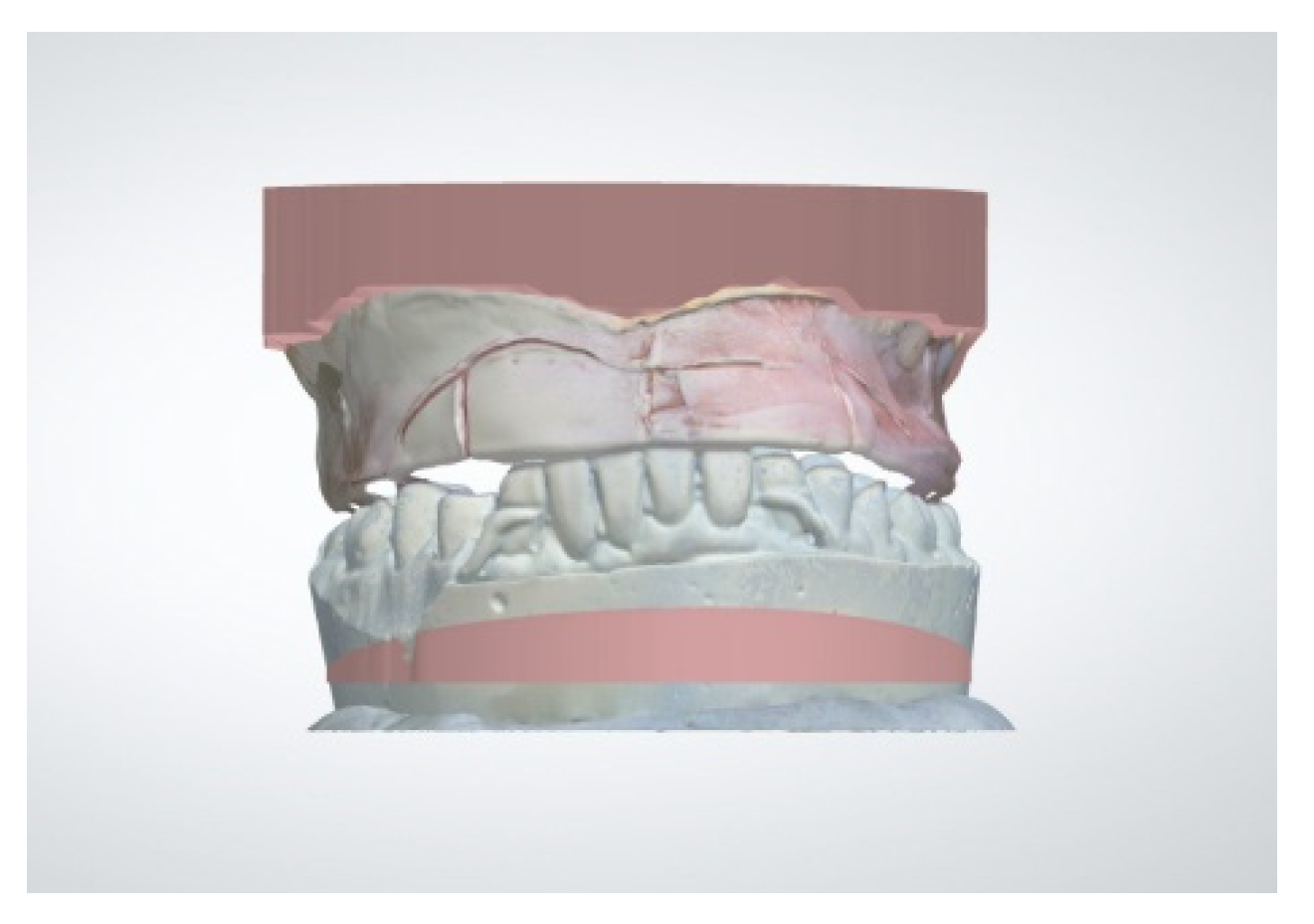
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polzer, I.; Schimmel, M.; Müller, F.; Biffar, R. Edentulism as part of the general health problems of elderly adults. Int. Dent. J. 2010, 60, 143–155. [Google Scholar] [CrossRef]
- Kim, J.J. Revisiting the Removable Partial Denture. Dent. Clin. N. Am. 2019, 63, 263–278. [Google Scholar] [CrossRef]
- Maeda, Y.; Minoura, M.; Tsutsumi, S.; Okada, M.; Nokubi, T. A CAD/CAM system for removable denture. Part. I: Fabrication of complete dentures. Int. J. Prosthodont. 1994, 7, 17–21. [Google Scholar] [PubMed]
- Dental Products Report. Available online: https://www.dentalproductsreport.com/view/future-dentures-digital (accessed on 1 May 2021).
- Goodacre, C.J.; Garbacea, A.; Naylor, W.P.; Daher, T.; Marchack, C.B.; Lowry, J. CAD/CAM fabricated complete dentures: Concepts and clinical methods of obtaining required morphological data. J. Prosthet. Dent. 2012, 107, 34–46. [Google Scholar] [CrossRef]
- Kattadiyil, M.T.; Goodacre, C.J.; Baba, N.Z. CAD/CAM complete dentures: A review of two commercial fabrication systems. J. Calif. Dent. Assoc. 2013, 41, 407–416. [Google Scholar] [PubMed]
- Infante, L.; Yilmaz, B.; McGlumphy, E.; Finger, I. Fabricating complete dentures with CAD/CAM technology. J. Prosthet. Dent. 2014, 111, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Inokoshi, M.; Kanazawa, M.; Minakuchi, S. Evaluation of a complete denture trial method applying rapid prototyping. Dent. Mater. J. 2012, 31, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Deak, A.; Marinello, C.P. CAD-CAM-Anwendung in der Totalprothetik CAD-CAM-Anwendung in der Totalprothetik CAD-CAM-Anwendung in der Totalprothetik. Swiss Dent. J. 2015, 125, 713–728, (In French/German). [Google Scholar] [PubMed]
- Bonnet, G.; Batisse, C.; Bessadet, M.; Nicolas, E.; Veyrune, J.L. A new digital denture procedure: A first practitioners appraisal. BMC Oral Health 2017, 17, 155. [Google Scholar] [CrossRef] [Green Version]
- Janeva, N.M.; Kovacevska, G.; Elencevski, S.; Panchevska, S.; Mijoska, A.; Lazarevska, B. Advantages of CAD/CAM versus Conventional Complete Dentures—A Review. Open Access Maced. J. Med. Sci. 2018, 6, 1498–1502. [Google Scholar] [CrossRef] [Green Version]
- Steinmassl, O.; Dumfahrt, H.; Grunert, I.; Steinmassl, P.A. CAD/CAM produces dentures with improved fit. Clin. Oral Investig. 2018, 22, 2829–2835. [Google Scholar] [CrossRef] [Green Version]
- Srinivasan, M.; Cantin, Y.; Mehl, A.; Gjengedal, H.; Müller, F.; Schimmel, M. CAD/CAM milled removable complete dentures: An in vitro evaluation of trueness. Clin. Oral Investig. 2017, 21, 2007–2019. [Google Scholar] [CrossRef] [Green Version]
- Schlenz, M.A.; Schmidt, A.; Wöstmann, B.; Rehmann, P. Clinical performance of computer-engineered complete dentures: A retrospective pilot study. Quintessence Int. 2019, 50, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Schwindling, F.S.; Stober, T. A comparison of two digital techniques for the fabrication of complete removable dental prostheses: A pilot clinical study. J. Prosthet. Dent. 2016, 116, 756–763. [Google Scholar] [CrossRef]
- John, A.V.; Abraham, G.; Alias, A. Two-visit CAD/CAM milled dentures in the rehabilitation of edentulous arches: A case series. J. Indian Prosthodont. Soc. 2019, 19, 88–92. [Google Scholar] [CrossRef]
- Kattadiyil, M.T.; Jekki, R.; Goodacre, C.J.; Baba, N.Z. Comparison of treatment outcomes in digital and conventional complete removable dental prosthesis fabrications in a predoctoral setting. J. Prosthet. Dent. 2015, 114, 818–825. [Google Scholar] [CrossRef]
- Arakawa, I.; Al-Haj Husain, N.; Srinivasan, M.; Maniewicz, S.; Abou-Ayash, S.; Schimmel, M. Clinical outcomes and costs of conventional and digital complete dentures in a university clinic: A retrospective study. J. Prosthet. Dent. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Kattadiyil, M.T.; Mursic, Z.; AlRumaih, H.; Goodacre, C.J. Intraoral scanning of hard and soft tissues for partial removable dental prosthesis fabrication. J. Prosthet. Dent. 2014, 112, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Lo Russo, L.; Salamini, A. Single-arch digital removable complete denture: A workflow that starts from the intraoral scan. J. Prosthet. Dent. 2018, 120, 20–24. [Google Scholar] [CrossRef]
- Lo Russo, L.; Salamini, A.; Troiano, G.; Guida, L. Digital dentures: A protocol based on intraoral scans. J. Prosthet. Dent. 2021, 125, 597–602. [Google Scholar] [CrossRef]
- Chebib, N.; Kalberer, N.; Srinivasan, M.; Maniewicz, S.; Perneger, T.; Müller, F. Edentulous jaw impression techniques: An in vivo comparison of trueness. J. Prosthet. Dent. 2019, 121, 623–630. [Google Scholar] [CrossRef]
- Lo Russo, L.; Caradonna, G.; Troiano, G.; Salamini, A.; Guida, L.; Ciavarella, D. Three-dimensional differences between intraoral scans and conventional impressions of edentulous jaws: A clinical study. J. Prosthet. Dent. 2020, 123, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Lo Russo, L.; Caradonna, G.; Salamini, A.; Guida, L. A single procedure for the registration of maxillo-mandibular relationships and alignment of intraoral scans of edentulous maxillary and mandibular arches. J. Prosthodont. Res. 2020, 64, 55–59. [Google Scholar] [CrossRef]
- Lo Russo, L.; Di Gioia, C.; Salamini, A.; Guida, L. Integrating intraoral, perioral, and facial scans into the design of digital dentures. J. Prosthet. Dent. 2020, 123, 584–588. [Google Scholar] [CrossRef]
- Lepidi, L.; Galli, M.; Mastrangelo, F.; Venezia, P.; Joda, T.; Wang, H.L.; Li, J. Virtual Articulators and Virtual Mounting Procedures: Where Do We Stand? J. Prosthodont. 2021, 30, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Exocad. Available online: https://exocad.com/our-products/exocad-dentalcad/virtual-articulator (accessed on 9 May 2021).
- 3shape. Available online: https://www.3shape.com/en/scanners/lab (accessed on 9 May 2021).
- Park, J.H.; Lee, G.H.; Moon, D.N.; Kim, J.C.; Park, M.; Lee, K.M. A digital approach to the evaluation of mandibular position by using a virtual articulator. J. Prosthet. Dent. 2021, 125, 849–853. [Google Scholar] [CrossRef]
- Li, J.; Chen, Z.; Decker, A.M.; Wang, H.L.; Joda, T.; Mendonca, G.; Lepidi, L. Trueness and Precision of Economical Smartphone-Based Virtual Facebow Records. J. Prosthodont. 2021. [Google Scholar] [CrossRef] [PubMed]
- Yau, H.T.; Liao, S.W.; Chang, C.H. Modeling of digital dental articulator and its accuracy verification using optical measurement. Comput. Methods Programs Biomed. 2020, 196, 105646. [Google Scholar] [CrossRef]
- Li, L.; Sun, Y.; Wang, Y.; Li, W.; Dai, N.; Tian, S.; Cui, H. Accuracy of a Novel Virtual Articulator for Recording Three-Dimensional Dentition. Int. J. Prosthodont. 2020, 33, 441–451. [Google Scholar] [CrossRef]
- Bae, M.; Park, J.W.; Kim, N. Fully automated estimation of arch forms in cone-beam CT with cubic B-spline approximation: Evaluation of digital dental models with missing teeth. Comput. Biol. Med. 2021, 131, 104256. [Google Scholar] [CrossRef]
- Yu, X.; Cheng, X.; Dai, N.; Chen, H.; Yu, C.; Sun, Y. Study on digital teeth selection and virtual teeth arrangement for complete denture. Comput. Methods Programs Biomed. 2018, 155, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Schweiger, J.; Stumbaum, J.; Edelhoff, D.; Güth, J.F. Systematics and concepts for the digital production of complete dentures: Risks and opportunities. Int. J. Comput. Dent. 2018, 21, 41–56. [Google Scholar] [PubMed]
- Sachs, E.; Cima, M.; Cornie, J. Three-Dimensional Printing: Rapid Tooling and Prototypes Directly from a CAD Model. CIRP Ann. 1990, 39, 201–204. [Google Scholar] [CrossRef]
- Shaiba, F.; Abid, H.; Shashi, B.; Mohd, J.; Sunil, K.M.; Someet, S. Exploring the significant applications of Internet of Things (IoT) with 3D printing using advanced materials in medical field. Mater. Today Proc. 2021, 45, 4844–4851. [Google Scholar] [CrossRef]
- DC Dentalcompare. Dental 3D Printers. Available online: https://www.dentalcompare.com/Dental-Lab-Products/24989-Dental-Laboratory-3D-Printers/ (accessed on 28 April 2021).
- DC Dentalcompare. Chairside 3D Printers. Available online: https://www.dentalcompare.com/Quick-Picks/348533-Chairside-3D-Printers/ (accessed on 28 April 2021).
- Steinmassl, P.A.; Klaunzer, F.; Steinmassl, O.; Dumfahrt, H.; Grunert, I. Evaluation of Currently Available CAD/CAM Denture Systems. Int. J. Prosthodont. 2017, 30, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Tzeng, J.J.; Yang, T.S.; Lee, W.F.; Chen, H.; Chang, H.M. Mechanical Properties and Biocompatibility of Urethane Acrylate-Based 3D-Printed Denture Base Resin. Polymers 2021, 13, 822. [Google Scholar] [CrossRef]
- Chen, S.; Yang, J.; Jia, Y.-G.; Lu, B.; Ren, L. A Study of 3D-Printable Reinforced Composite Resin: PMMA Modified with Silver Nanoparticles Loaded Cellulose Nanocrystal. Materials 2018, 11, 2444. [Google Scholar] [CrossRef] [Green Version]
- Liao, W.; Zheng, S.; Chen, S.; Zhao, L.; Huang, X.; Huang, L.; Kang, S. Surface silanization and grafting reaction of nano-silver loaded zirconium phosphate and properties strengthen in 3D-printable dental base composites. J. Mech. Behav. Biomed. Mater. 2020, 110, 103864. [Google Scholar] [CrossRef]
- Badger, G.R.; Fryer, C.E.; Giannini, P.J.; Townsend, J.A.; Huja, S. Helping Dental Students Make Informed Decisions About Private Practice Employment Options in a Changing Landscape. J. Dent. Educ. 2015, 79, 1396–1401. [Google Scholar] [CrossRef]
- Barber, M.; Wiesen, R.; Arnold, S.; Taichman, R.S.; Taichman, L.S. Perceptions of business skill development by graduates of the University of Michigan Dental School. J. Dent. Educ. 2011, 75, 505–517. [Google Scholar] [CrossRef]
- Willis, D.O. Business Basics for Dentists; Wiley-Blackwell: Ames, IA, USA, 2013; pp. 161–172, 319–351. [Google Scholar]
- Fernandez, M.A.; Nimmo, A.; Behar-Horenstein, L.S. Digital Denture Fabrication in Pre- and Postdoctoral Education: A Survey of U.S. Dental Schools. J. Prosthodont. 2016, 25, 83–90. [Google Scholar] [CrossRef]
- Goodacre, C.J.; Goodacre, B.J.; Baba, N.Z. Should Digital Complete Dentures Be Part of A Contemporary Prosthodontic Education? J. Prosthodont. 2021, 30, 163–169. [Google Scholar] [CrossRef]
- Smith, P.B.; Perry, J.; Elza, W. Economic and Clinical Impact of Digitally Produced Dentures. J. Prosthodont. 2021, 30, 108–112. [Google Scholar] [CrossRef]
- Hazeveld, A.; Huddleston Slater, J.J.; Ren, Y. Accuracy and reproducibility of dental replica models reconstructed by different rapid prototyping techniques. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Bilgin, M.S.; Baytaroğlu, E.N.; Erdem, A.; Dilber, E. A review of computer-aided design/computer-aided manufacture techniques for removable denture fabrication. Eur. J. Dent. 2016, 10, 286–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srinivasan, M.; Gjengedal, H.; Cattani-Lorente, M.; Moussa, M.; Durual, S.; Schimmel, M.; Müller, F. CAD/CAM milled complete removable dental prostheses: An in vitro evaluation of biocompatibility, mechanical properties, and surface roughness. Dent. Mater. J. 2018, 37, 526–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinmassl, P.A.; Wiedemair, V.; Huck, C.; Klaunzer, F.; Steinmassl, O.; Grunert, I.; Dumfahrt, H. Do CAD/CAM dentures really release less monomer than conventional dentures? Clin. Oral Investig. 2017, 21, 1697–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zirkonzahn. Available online: https://zirkonzahn.com/en/products/millable-materials/tecno-med-mineral (accessed on 28 April 2021).
- Ivoclar Digital. Available online: https://www.ivoclardigital.com/en/laboratory/material/removable-prosthetics (accessed on 28 April 2021).
- Vita. Available online: https://www.vita-zahnfabrik.com/en/VITA-VIONIC-SOLUTIONS-Digital-prosthetics-are-now-available-for-practical-use-51503,57329.html (accessed on 28 April 2021).
- Avadent Digital Dental Solutions. Available online: https://www.avadent.com/products/solutions/ (accessed on 28 April 2021).
- Baltic Denture System. Available online: https://www.baltic-denture-system.de/en/ (accessed on 28 April 2021).
- Jurado, C.A.; Tsujimoto, A.; Alhotan, A.; Villalobos-Tinoco, J.; AlShabib, A. Digitally Fabricated Immediate Complete Dentures: Case Reports of Milled and Printed Dentures. Int. J. Prosthodont. 2020, 33, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Anadioti, E.; Musharbash, L.; Blatz, M.B.; Papavasiliou, G.; Kamposiora, P. 3D printed complete removable dental prostheses: A narrative review. BMC Oral Health 2020, 20, 343. [Google Scholar] [CrossRef]
- Herpel, C.; Tasaka, A.; Higuchi, S.; Finke, D.; Kühle, R.; Odaka, K.; Rues, S.; Lux, C.J.; Yamashita, S.; Rammelsberg, P.; et al. Accuracy of 3D printing compared with milling—A multi-center analysis of try-in dentures. J. Dent. 2021, 110, 103681. [Google Scholar] [CrossRef]
- Unkovskiy, A.; Schmidt, F.; Beuer, F.; Li, P.; Spintzyk, S.; Kraemer Fernandez, P. Stereolithography vs. Direct Light Processing for Rapid Manufacturing of Complete Denture Bases: An In Vitro Accuracy Analysis. J. Clin. Med. 2021, 10, 1070. [Google Scholar] [CrossRef] [PubMed]
- Pham, D.M.; Gonzalez, M.D.; Ontiveros, J.C.; Kasper, F.K.; Frey, G.N.; Belles, D.M. Wear Resistance of 3D Printed and Prefabricated Denture Teeth Opposing Zirconia. J. Prosthodont. 2021. [Google Scholar] [CrossRef]
- Cha, H.S.; Park, J.M.; Kim, T.H.; Lee, J.H. Wear resistance of 3D-printed denture tooth resin opposing zirconia and metal antagonists. J. Prosthet. Dent. 2020, 124, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, M.; Kamnoedboon, P.; McKenna, G.; Angst, L.; Schimmel, M.; Özcan, M.; Müller, F. CAD-CAM Removable Complete Dentures: A systematic review and meta-analysis of trueness of fit, biocompatibility, mechanical properties, surface characteristics, color stability, time-cost analysis, clinical and patient-reported outcomes. J. Dent. 2021, in press. [Google Scholar] [CrossRef]
- Chaturvedi, S.; Addas, M.K.; Alqahtani, N.M.; Al Ahmari, N.M.; Alfarsi, M.A. Clinical analysis of CAD-CAM milled and printed complete dentures using computerized occlusal force analyser. Technol. Health Care 2021, 29, 797–811. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.J.E.; Uy, C.E.; Plaksina, P.; Ramani, R.S.; Ganjigatti, R.; Waddell, J.N. Bond Strength of Denture Teeth to Heat-Cured, CAD/CAM and 3D Printed Denture Acrylics. J. Prosthodont. 2020, 29, 415–421. [Google Scholar] [CrossRef]
- Available online: http://www.gerodontology.gr/en/public.html (accessed on 5 August 2021).
- Clark, W.A.; Brazile, B.; Matthews, D.; Solares, J.; De Kok, I.J. A Comparison of Conventionally Versus Digitally Fabricated Denture Outcomes in a Dental Clinic. J. Prosthodont. 2021, 30, 47–50. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stereolithography | Digital Light Processing | MultiJet/PolyJet Printing | |
|---|---|---|---|
| Acronym | SLA | DLP | - |
| Production Time | Usually longer than DLP | Short print cycles | Color combinations prolong printing cycles |
| Light source | UV LASER 1 | Specialized light projectors | UV light |
| Bath tank | Yes | Yes | No |
| Supports needed | Yes | Yes | No |
| Zirkonzahn Denture System™ | Ivoclar® Digital Denture | Vita Vionic™ | AvaDent® Digital Dentures | Baltic Denture System™ | |
|---|---|---|---|---|---|
| Monolithic CD | - | Yes | - | Yes | - |
| Resin puck for denture base with preformed teeth set-ups | - | - | - | - | Yes |
| Resin puck for denture base | Yes | Yes | Yes | Yes | - |
| Resin puck for denture teeth | - | Yes | - | - | - |
| Whole dental arch fabrication/adjustment | - | Yes | - | - | Yes |
| Compatibility with prefabricated teeth | Yes | - | Yes | Yes | - |
| Teeth hand bonding | Yes | Yes (if separately produced) | Yes | Yes | - |
| Hand characterization | Yes | - | - | - | - |
| Hand polishing | Yes | Yes | Yes | Yes | Yes |
| Light-colored pucks for try-in dentures | Yes | - | - | Yes | - |
| Appropriate for all jaw relationships | Yes | Yes | Yes | Yes | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villias, A.; Karkazis, H.; Yannikakis, S.; Theocharopoulos, A.; Sykaras, N.; Polyzois, G. Current Status of Digital Complete Dentures Technology. Prosthesis 2021, 3, 229-244. https://doi.org/10.3390/prosthesis3030023
Villias A, Karkazis H, Yannikakis S, Theocharopoulos A, Sykaras N, Polyzois G. Current Status of Digital Complete Dentures Technology. Prosthesis. 2021; 3(3):229-244. https://doi.org/10.3390/prosthesis3030023
Chicago/Turabian StyleVillias, Aristeidis, Hercules Karkazis, Stavros Yannikakis, Antonios Theocharopoulos, Nikitas Sykaras, and Gregory Polyzois. 2021. "Current Status of Digital Complete Dentures Technology" Prosthesis 3, no. 3: 229-244. https://doi.org/10.3390/prosthesis3030023
APA StyleVillias, A., Karkazis, H., Yannikakis, S., Theocharopoulos, A., Sykaras, N., & Polyzois, G. (2021). Current Status of Digital Complete Dentures Technology. Prosthesis, 3(3), 229-244. https://doi.org/10.3390/prosthesis3030023