
Cystic Artery Bleeding: Imaging Insights and Systematic Review of Endovascular Management

 , ,
, ,  , , ,
, , , 
Abstract
1. Introduction
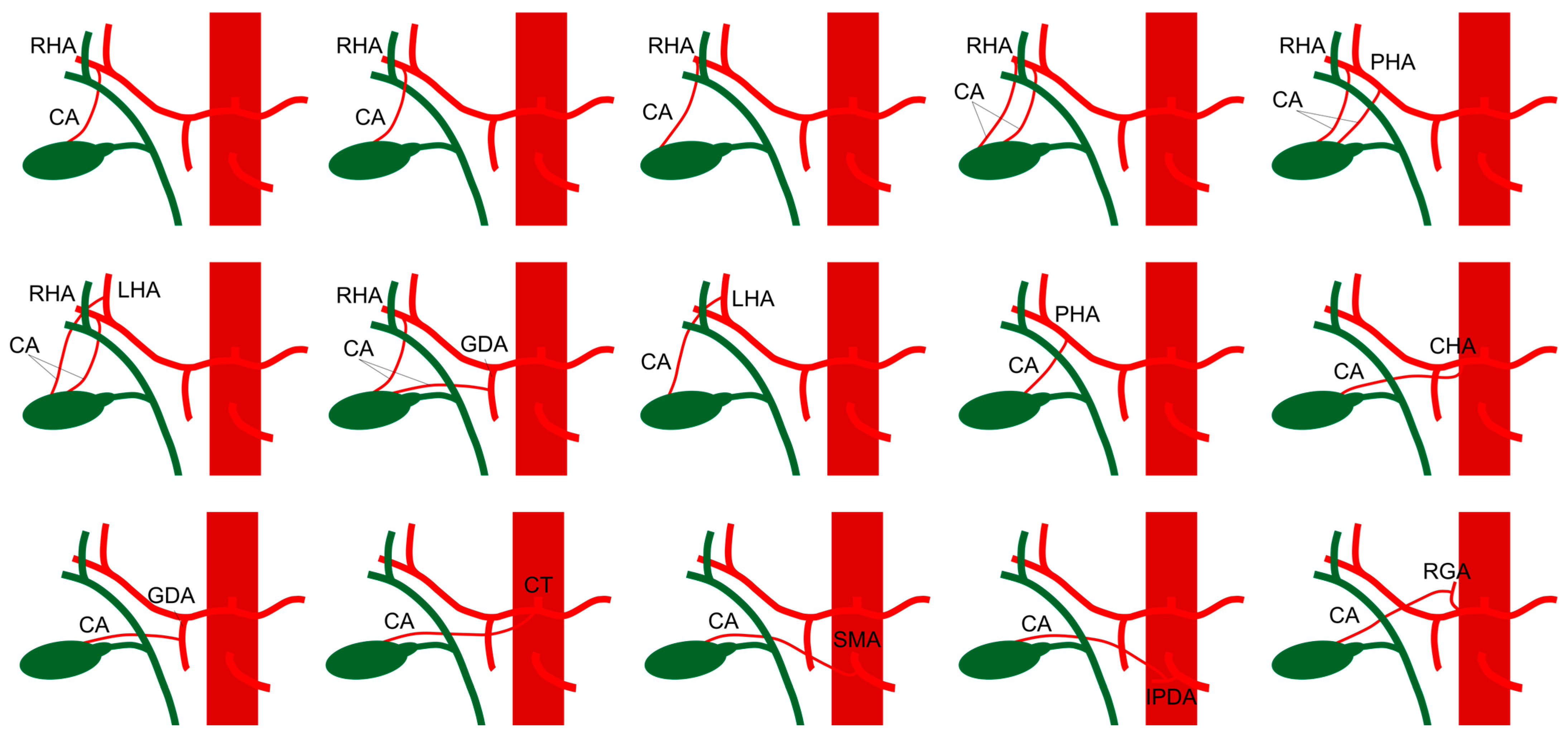
1.1. Cystic Artery Vascular Anatomy
1.2. Etiology and Pathophysiology
1.3. Clinical Manifestations
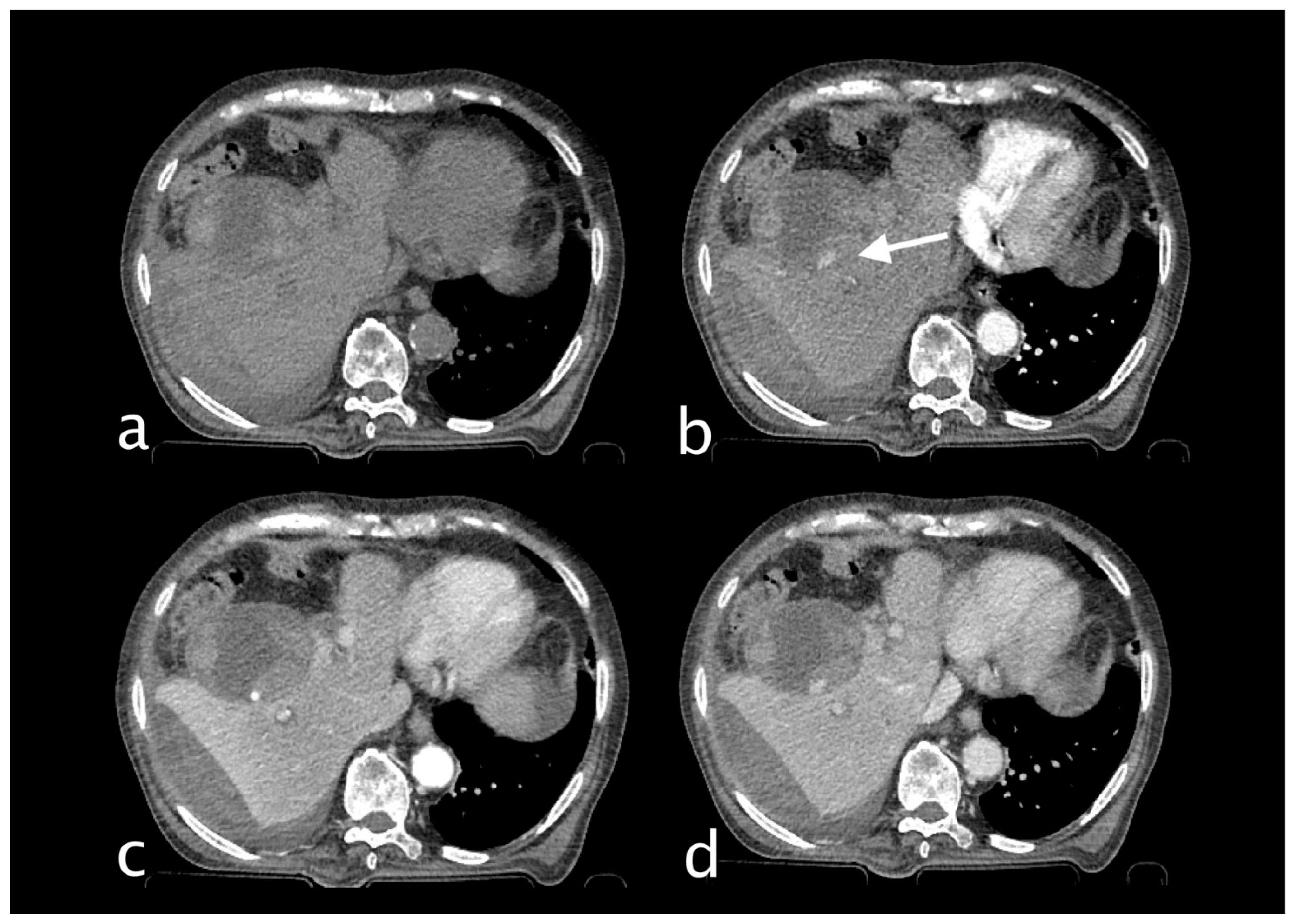
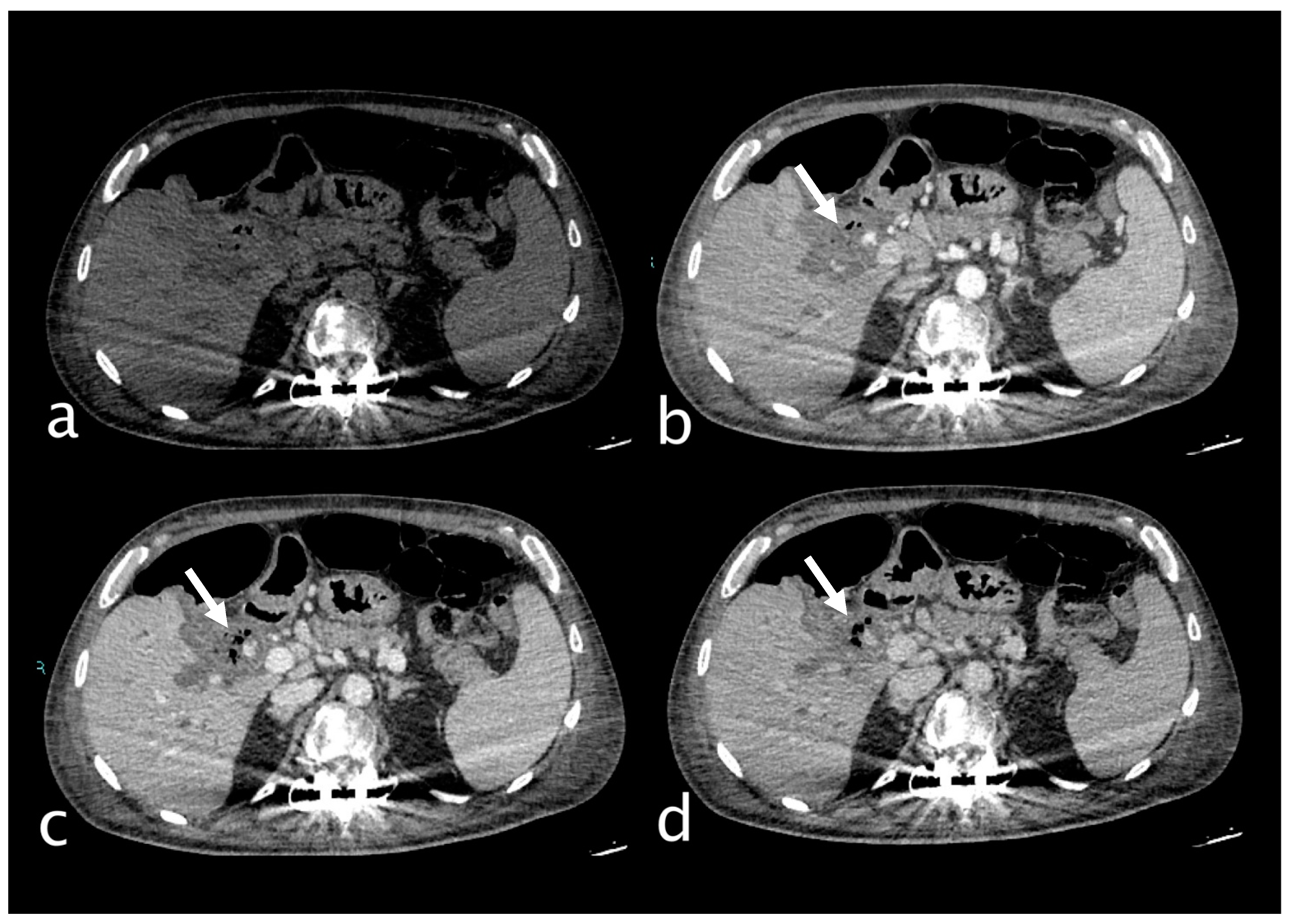
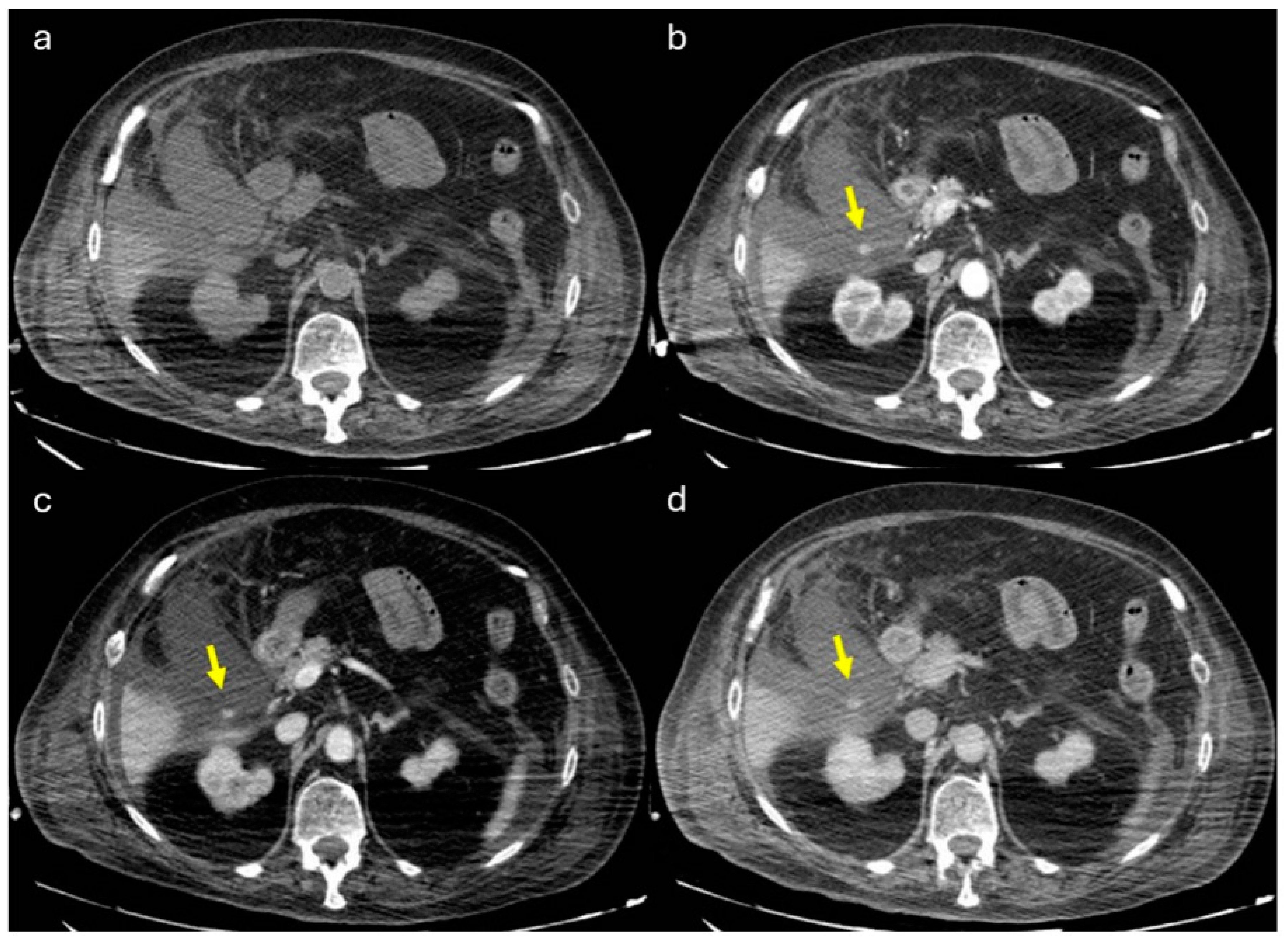
2. Imaging
3. Treatment
3.1. Results
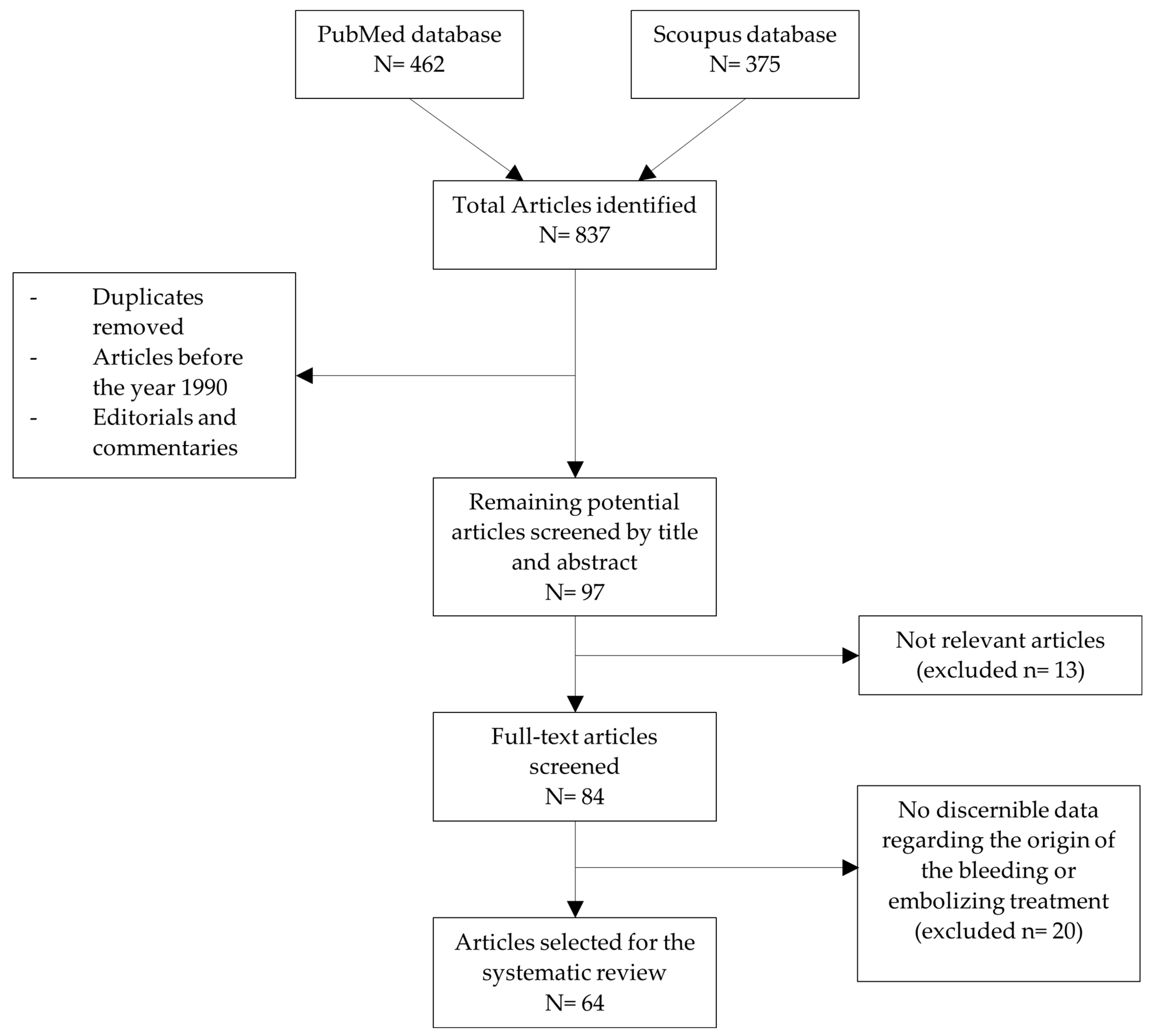
3.1.1. Study Selection and Characteristics
3.1.2. Patient Demographics and Clinical Presentation
3.1.3. Imaging and Diagnostic Findings
3.1.4. Management and Outcomes
3.2. Materials and Methods
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors/Year | Type of the Study | Number of Patients | Sex | Age | Etiology | Main Symptoms | Type of Lesion | Interventional Treatment | Embolic Agents | Procedure-Related Complications | Procedures After Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sarmento Costa M et al., 2024 [33] | case report | 1 | M | 88 | Bouveret syndrome (bilioenteric fistula) | Hematemesis | Pseudoaneurysm | TAE | Coils | N/R | No | Recovered |
| Giurazza F et al., 2024 [34] | technical report | 1 | M | 71 | Acute cholecystitis | N/R | Pseudoaneurysm | PE | NBCA | N/R | No | Recovered |
| Heidari A et al., 2024 [35] | case report | 1 | F | 64 | Acute cholecystitis | Abdominal pain, hematemesis | Pseudoaneurysm | TAE | PVA (500–700 µm) + gelfoam | N/R | Cholecystectomy | Recovered |
| Khawjah A et al., 2024 [2] | case report | 1 | M | 54 | Acute cholecystitis | Abdominal pain, hematemesis, jaundice | Pseudoaneurysm rupture | TAE | Coils + gelfoam | Hepatic ischemia | Cholecystectomy | Recovered |
| Anns MK et al., 2024 [36] | case report | 1 | M | 64 | Iatrogenic (laparoscopic cholecistectomy) | Hematemesis, melena | Pseudoaneurysm | TAE | Coils | N/R | No | Recovered |
| Okamoto S et al., 2024 [37] | case report | 1 | M | 80 | Neoplastic (HCC) | Abdominal pain, melena, jaundice | Pseudoaneurysm rupture | TAE | NBCA + Lipiodol + gelfoam + coils | N/R | No | Recovered |
| Rais A et al., 2024 [13] | case report | 1 | F | 71 | Acute cholecystitis | Abdominal pain | Pseudoaneurysm | TAE | NBCA + Lipiodol | N/R | Cholecystectomy | Recovered |
| Robbie R et al., 2024 [25] | case report | 1 | M | 83 | Acute cholecystitis | Bleeding per rectum | Pseudoaneurysm | TAE | Coils | N/R | No | Recovered |
| Saha B et al., 2024 [38] | case report | 1 | M | 70 | Acute cholecystitis | Abdominal pain | Pseudoaneurysm | TAE | Coils | N/R | Cholecistectomy | Recovered |
| Sibria D et al., 2024 [19] | case report | 1 | F | 38 | Iatrogenic (laparoscopic cholecistectomy) | Abdominal pain, jaundice, bleeding per rectum, melena | Pseudoaneurysm | TAE | Coils | N/R | No | Recovered |
| Mie T et al., 2024 [39] | case report | 1 | F | 78 | Acute cholecystitis | Abdominal pain, jaundice | Pseudoaneurysm rupture | TAE | NBCA + Lipiodol | N/R | No | Recovered |
| Khan H et al., 2023 [40] | case report | 1 | M | 88 | Acute cholecystitis | Abdominal pain, jaundice | Pseudoaneurysm rupture | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Kim HC et al., 2023 [41] | retrospective study | 1 | M | 43 | Acute cholecystitis | Melena | N/R | TAE | blood clot | N/R | Cholecystectomy | Recovered |
| retrospective study | 1 | F | 34 | Iatrogenic (cholecystostomy) | Hemoperitoneum | N/R | TAE | Gelfoam | N/R | N/R | Recovered | |
| retrospective study | 1 | F | 54 | Neoplastic | Melena | N/R | TAE | NBCA | N/R | N/R | Recovered | |
| retrospective study | 1 | F | 49 | Acute cholecystitis | Hematemesis | N/R | TAE | NBCA | Ischemic cholecystitis | N/R | Death from MOF, sepsis | |
| retrospective study | 1 | M | 75 | Acute cholecystitis | Hematochezia | N/R | TAE | NBCA | N/R | N/R | Recovered | |
| retrospective study | 1 | F | 52 | Iatrogenic (RFA) | Hemoperitoneum | N/R | TAE | NBCA | N/R | N/R | Recovered | |
| retrospective study | 1 | F | 71 | Neoplastic | Jaundice | N/R | TAE | NBCA | N/R | N/R | Recovered | |
| retrospective study | 1 | M | 74 | Acute cholecystitis | Blood in cholecystostomy tube | N/R | TAE | NBCA | N/R | N/R | Death from MOF, sepsis | |
| retrospective study | 1 | M | 48 | Trauma | Hemoperitoneum | N/R | TAE | NBCA | Ischemic cholecystitis | N/R | Recovered | |
| retrospective study | 1 | M | 48 | Acute cholecystitis | Blood in cholecystostomy tube | N/R | TAE | NBCA | Ischemic cholecystitis | N/R | Death from MOF, sepsis | |
| retrospective study | 1 | M | 80 | Acute cholecystitis | Hematemesis | N/R | TAE | NBCA | N/R | N/R | Recovered | |
| retrospective study | 1 | F | 78 | Acute cholecystitis | Hematemesis | N/R | TAE | NBCA | N/R | N/R | Death from pneumonia | |
| retrospective study | 1 | F | 78 | Duodenal ulcer | Hematemesis | N/R | TAE | Coils | N/R | Cholecystectomy | Recovered | |
| retrospective study | 1 | M | 67 | Duodenal ulcer | Melena | N/R | TAE | NBCA | N/R | N/R | Recovered | |
| retrospective study | 1 | F | 56 | Duodenal ulcer | Melena | N/R | TAE | Gelfoam | N/R | N/R | Death from MOF, sepsis | |
| retrospective study | 1 | M | 78 | Acute cholecystitis | Abdominal pain | N/R | TAE | NBCA | N/R | Cholecystectomy | Recovered | |
| retrospective study | 1 | M | 64 | Acute cholecystitis | Blood in cholecystostomy tube | N/R | TAE | NBCA | N/R | N/R | Recovered | |
| retrospective study | 1 | M | 80 | Acute cholecystitis | Hemoperitoneum | N/R | TAE | NBCA | N/R | N/R | Death from MOF, sepsis | |
| retrospective study | 1 | M | 85 | Iatrogenic (cholecystostomy) | Blood in cholecystostomy tube | N/R | TAE | NBCA | N/R | N/R | Recovered | |
| retrospective study | 1 | M | 70 | Iatrogenic (cholecystostomy) | Abdominal pain | N/R | TAE | NBCA | N/R | N/R | Recovered | |
| Liu YL et al., 2023 [42] | case report | 1 | M | 81 | Acute cholecystitis | Abdominal pain, melena, hemobilia | Pseudoaneurysm with active bleeding | TAE | Coils | N/R | Cholecystostomy | Recovered |
| Shrivastava A et al., 2023 [26] | case report | 1 | M | 41 | Acute cholecystitis | Abdominal pain, melena | Pseudoaneurysm | TAE | Coils | N/R | Cholecystostomy + cholecystectomy | Recovered |
| Williams T et al., 2023 [43] | case report | 1 | M | 61 | Mirizzi syndrome | Abdominal pain | Pseudoaneurysm | TAE | Coils | N/R | Cholecystostomy | Recovered |
| Zainab R et al., 2023 [44] | case report | 1 | M | 55 | Acute cholecystitis | Abdominal pain, hematemesis, melena | Pseudoaneurysm | TAE | Coils | N/R | N/R | Recovered |
| Itagaki Y et al., 2023 [45] | case report | 1 | F | 70 | Acute cholecystitis | Jaundice | Pseudoaneurysm | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Christodoulou P et al., 2022 [46] | case report | 1 | M | 67 | Iatrogenic (laparoscopic cholecistectomy) | Abdominal pain | Pseudoaneurysm rupture | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Fukushima R et al., 2022 [47] | case report | 1 | F | 73 | Mirizzi syndrome | Abdominal pain, jaundice | Pseudoaneurysm rupture | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Amakye DO et al., 2021 [48] | case report | 1 | M | 66 | Acute cholecystitis (cholecystocolic fistula) | Abdominal pain | Pseudoaneurysm rupture | TAE | Coils | N/R | No | Recovered |
| Mahalingam S et al., 2021 [49] | case report | 1 | M | 52 | Neoplastic (carcinoma gallbladder) | Abdominal pain, hematemesis, melena | Pseudoaneurysm rupture | TAE | NBCA | N/R | Cholecystostomy | Recovered |
| Nguyen D et al., 2021 [50] | case report | 1 | M | 74 | Acute cholecystitis | Abdominal pain, hematemesis, melena | Pseudoaneurysm with active bleeding | TAE | Coils | N/R | Cholecystectomy | Recovered |
| case report | 1 | M | 74 | Acute cholecystitis | N/R | Pseudoaneurysm with active bleeding | TAE | PVA (500–700) + coils | N/R | Cholecystectomy | Recovered | |
| Acharya S et al., 2020 [51] | case report | 1 | F | 62 | Chronic cholecystitis | Abdominal pain, bleeding per rectum | Cystic artery-gallbladder fistula with bleeding | TAE | Coils | N/R | No | Recovered |
| Carey F et al., 2020 [29] | case report | 1 | M | 47 | Acute cholecystitis (cholecystocolic fistula) | Abdominal pain, bleeding per rectum | Pseudoaneurysm with active bleeding | TAE | Coils | N/R | No | Recovered |
| Leshen M et al., 2020 [52] | case report | 1 | M | 16 | Acute cholecystitis | Abdominal pain, hematemesis | Pseudoaneurysm with active bleeding | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Proença AL et al., 2020 [53] | case report | 1 | F | 73 | Iatrogenic (ERCP) | Abdominal pain, hematemesis, melena | Pseudoaneurysm with active bleeding | TAE | NBCA | Hepatic ischemia | Cholecystectomy | Recovered |
| Yam MKH et al., 2020 [54] | case report | 1 | F | 51 | Acute cholecystitis | Abdominal pain, hematemesis, melena | Pseudoaneurysm with active bleeding | TAE | PVA + Coils | N/R | Cholecystostomy + cholecystectomy | Recovered |
| Rossini M et al., 2019 [55] | case report | 1 | M | 66 | Iatrogenic (laparoscopic cholecistectomy) | Abdominal pain, hematemesis, melena | Pseudoaneurysm with active bleeding | TAE | Coils | N/R | No | Recovered |
| Sada DM et al., 2019 [56] | case report | 1 | M | 69 | Iatrogenic (cholecystostomy) | Abdominal pain | Pseudoaneurysm with active bleeding | TAE | Onyx | N/R | No | Postoperative death |
| Tanaka T et al., 2019 [57] | case report | 1 | F | 80 | Acute cholecystitis | Abdominal pain, melena | Pseudoaneurysm rupture | TAE | Coils | N/R | Endoscopic biliary drainage | Recovered |
| Kuzman MS et al., 2018 [58] | case report | 1 | F | 25 | Acute cholecystitis | Abdominal pain | Pseudoaneurysm | TAE | NBCA + Coils | N/R | Cholecystostomy + cholecystectomy | Recovered |
| Sunkara PRV et al., 2018 [14] | case report | 1 | M | 56 | Acute cholecystitis | Abdominal pain | Pseudoaneurysm rupture | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Machado NO et al., 2017 [10] | case report | 1 | F | 70 | Iatrogenic (laparoscopic cholecistectomy) | Abdominal pain | Pseudoaneurysm with active bleeding | TAE | Coils | N/R | No | Recovered |
| Maddineni S et al., 2017 [59] | case report | 1 | F | 54 | Acute cholecystitis | Abdominal pain, melena | Pseudoaneurysm with active bleeding | TAE | Thrombin + Coils | N/R | Cholecystostomy | Death due to non-procedure-related complications |
| Tapnio RH et al., 2017 [60] | case report | 1 | F | 91 | Acute cholecystitis | Abdominal pain | Pseudoaneurysm with active bleeding | TAE | Coils | N/R | Cholecystectomy | Recovered |
| case report | 1 | M | 61 | Acute cholecystitis | Abdominal pain | Pseudoaneurysm with active bleeding | TAE | Coils + gelfoam | N/R | Cholecystectomy | Recovered | |
| case report | 1 | M | 91 | Acute cholecystitis | Abdominal pain | Pseudoaneurysm | TAE | Coils | N/R | Cholecystostomy | Recovered | |
| Thillai M et al., 2017 [61] | case report | 1 | M | 33 | Acute pancreatitis | Melena | Pseudoaneurysm with active bleeding | TAE | Gelfoam | N/R | Cholecystostomy | Recovered |
| Trombatore C et al., 2017 [62] | case report | 1 | M | 64 | Acute cholecystitis | Abdominal pain, jaundice | Pseudoaneurysm with active bleeding | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Hall TC et al., 2016 [63] | case report | 1 | M | 88 | Acute cholecystitis | Abdominal pain, melena | Pseudoaneurysm with active bleeding | TAE | NBCA + Lipiodol + gelfoam + coils | N/R | No | Recovered |
| Liu B et al., 2016 [64] | case report | 1 | M | 82 | Iatrogenic (laparoscopic cholecistectomy) | Hemobilia | Pseudoaneurysm with active bleeding | TAE | Coils + stent | N/R | No | Recovered |
| Shelmerdine SC et al., 2015 [31] | case report | 1 | M | 72 | Acute cholecystitis | Abdominal pain, hematemesis, melena | Pseudoaneurysm with active bleeding | TAE | Coils | N/R | No | Recovered |
| Aljiffry MM et al., 2014 [65] | case report | 1 | M | 57 | Acute cholecystitis | Abdominal pain | Active bleeding from cystic artery | TAE | Gelfoam | N/R | Cholecystectomy | Recovered |
| Kulkarni V et al., 2014 [15] | case report | 1 | M | 55 | Mirizzi syndrome | Abdominal pain, jaundice, melena | Pseudoaneurysm | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Kumar A et al., 2014 [66] | case report | 1 | F | 45 | Iatrogenic (laparoscopic cholecistectomy) | Hemobilia | Pseudoaneurysm with active bleeding | PE | Thrombin (400 units) | N/R | No | Recovered |
| Mokrane FZ et al., 2013 [67] | case report | 1 | M | 67 | Acute cholecystitis | Hematemesis | Pseudoaneurysm with active bleeding | TAE | Coils | N/R | No | Recovered |
| Nana GR et al., 2013 [68] | case report | 1 | M | 74 | Acute cholecystitis | Abdominal pain, hematemesis, jaundice | Pseudoaneurysm | TAE | Coils | N/R | Cholecystostomy | Recovered |
| case report | 1 | F | 79 | Acute cholecystitis | Abdominal pain, melena, jaundice | Pseudoaneurysm | TAE | Coils | N/R | No | Recovered | |
| Priya H et al., 2013 [17] | case report | 1 | M | 22 | Spontaneous | Abdominal pain, hematemesis, melena, jaundice | Fistula (cystic artery-gallbladder) | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Chong JJR et al., 2012 [69] | case report | 1 | M | 56 | Acute cholecystitis | Abdominal pain, hematemesis | Pseudoaneurysm | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Petrou A et al., 2012 [70] | case report | 1 | F | 34 | Iatrogenic (laparoscopic cholecistectomy) | Abdominal pain, hematemesis | Pseudoaneurysm | TAE | Coils | N/R | Ligation of right hepatic artery | Recovered |
| Siddiqui NA et al., 2011 [30] | case report | 1 | M | 58 | Acute cholecystitis | Abdominal pain, jaundice | Pseudoaneurysm | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Desai AU et al., 2010 [71] | case report | 1 | F | 78 | Chronic cholecystitis | Abdominal pain, melena, jaundice | Pseudoaneurysm | TAE | Coils | N/R | No | Recovered |
| Hague J et al., 2010 [72] | case series | 1 | M | 83 | Acute cholecystitis | Abdominal pain, hemoperitoneum | Pseudoaneurysm | TAE | Coils | N/R | No | Recovered |
| case series | 1 | M | 79 | Acute cholecystitis | Abdominal pain, hemobilia | Pseudoaneurysm | TAE | Coils | N/R | No | Recovered | |
| case series | 1 | M | 83 | Acute cholecystitis | Abdominal pain, melena | Pseudoaneurysm | TAE | Coils | N/R | No | Death from esophageal carcinoma within 2 months | |
| Nkwam N et al., 2010 [73] | case report | 1 | M | 71 | Acute cholecystitis | Abdominal pain | Pseudoaneurysm | TAE | Coils | N/R | Cholecystostomy | Recovered |
| Osada H et al., 2010 [3] | case report | 1 | M | 62 | Trauma | Asymptomatic | Pseudoaneurysm | TAE | Coils | N/R | No | Recovered |
| Contini S et al., 2009 [74] | case report | 1 | M | 58 | Chronic cholecystitis | Abdominal pain, melena, jaundice | Active bleeding | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Mullen R et al., 2009 [75] | case series | 1 | F | 75 | Chronic cholecystitis | Abdominal pain, hematemesis, melena | Pseudoaneurysm | TAE | Coils | N/R | No | Recovered |
| case series | 1 | M | 82 | Acute cholecystitis | Abdominal pain | Pseudoaneurysm | TAE | Coils | N/R | No | Recovered | |
| Ouazzani A et al., 2009 [16] | case report | 1 | M | 74 | Spontaneous | Abdominal pain | Active bleeding (rupture) | TAE | Particles (500–700 µm) | Ischemic cholecystitis | Cholecystectomy | Recovered |
| Nakase Y et al., 2008 [20] | case report | 1 | F | 63 | Iatrogenic (laparoscopic cholecistectomy) | Abdominal pain, melena, hematemesis | Pseudoaneurysm | TAE | NBCA + Coils | Liver abscess treated with antibiotics | No | Recovered |
| Shimada K et al., 2008 [76] | case report | 1 | M | 68 | Xanthogranulomatous cholecystitis | Jaundice, hemobilia | Pseudoaneurysm | TAE | Coils | N/R | Extended right hepatectomy | Recovered |
| Osada H et al., 2007 [77] | case report | 1 | F | 78 | Arteriovenous malformation | Asymptomatic | Arteriovenous malformation | TAE | Coils | N/R | No | Blood flow in AVM persisted; patient developed HCC recurrence after 4 years |
| Saluja SS et al., 2007 [78] | case report | 1 | F | 43 | Acute cholecystitis | Hematemesis, melena | Pseudoaneurysm | TAE | Coils + gelfoam | A day later the patient had increasing abdominal pain and appearance of peritoneal signs localized to the RUQ of the abdomen | Cholecystectomy | Recovered |
| Maeda A et al., 2002 [79] | case report | 1 | M | 62 | Acute cholecystitis | Abdominal pain, jaundice | Pseudoaneurysm | TAE | Coils | N/R | Cholecystectomy | Recovered |
| Delgadillo X et al., 1999 [80] | case report | 1 | M | 28 | Acute pancreatitis | Abdominal pain, hematemesis | Pseudoaneurysm | TAE | Coils | N/R | No | Recovered |
| England RE et al., 1998 [81] | case report | 1 | F | 71 | Acute cholecystitis | Abdominal pain, jaundice | Pseudoaneurysm | TAE | Coils | N/R | No | Death from MOF, sepsis |
References
- Taghavi, S.M.J.; Kumar, M.J.; Prabha, R.D.; Puhalla, H.; Sommerville, C. Cystic Artery Pseudoaneurysm: Current Review of Aetiology, Presentation, and Management. Surg. Res. Pract. 2021, 2021, 4492206. [Google Scholar] [CrossRef] [PubMed]
- Khawjah, A.; Khair, M.M.; Goubran, R. An unusual case of acute cholecystitis complicated by haemobilia and Mirizzi-like obstruction: A case report and review of literature. Ann. Med. Surg. 2024, 86, 3646–3651. [Google Scholar] [CrossRef]
- Osada, H.; Ohno, H.; Watanabe, W.; Okada, T.; Nakada, K.; Honda, N. Cystic artery bleeding due to blunt gallbladder injury: Computed tomography findings and treatment with transcatheter arterial embolization. Jpn. J. Radiol. 2010, 28, 162–165. [Google Scholar] [CrossRef]
- Hugh, T.B.; Kelly, M.D.; Li, B. Laparoscopic anatomy of the cystic artery. Am. J. Surg. 1992, 163, 593–595. [Google Scholar] [CrossRef]
- Andall, R.G.; Matusz, P.; du Plessis, M.; Ward, R.; Tubbs, R.S.; Loukas, M. The clinical anatomy of cystic artery variations: A review of over 9800 cases. Surg. Radiol. Anat. SRA 2016, 38, 529–539. [Google Scholar] [CrossRef]
- Ara, H.; Fakoya, A.O. Novel Variations in the Celiac and Hepatobiliary Arterial Anatomy: A Cadaveric Case Report. Cureus 2024, 16, e60813. [Google Scholar] [CrossRef] [PubMed]
- Asghar, A.; Priya, A.; Prasad, N.; Patra, A.; Agrawal, D. Variations in morphology of cystic artery: Systematic review and meta-analysis. Clin. Ter. 2024, 175, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Balija, M.; Huis, M.; Nikolić, V.; Štulhofer, M. Laparoscopic visualization of the cystic artery anatomy. World J. Surg. 1999, 23, 703–707, discussion 707. [Google Scholar] [CrossRef]
- Gupta, R.M.; Kumar, A.; Hariprasad, C.P.; Kumar, M. Anatomical variations of cystic artery, cystic duct, and gall bladder and their associated intraoperative and postoperative complications: An observational study. Ann. Med. Surg. 2023, 85, 3880–3886. [Google Scholar] [CrossRef]
- Machado, N.O.; Al-Zadjali, A.; Kakaria, A.K.; Younus, S.; Rahim, M.A.; Al-Sukaiti, R. Hepatic or Cystic Artery Pseudoaneurysms Following a Laparoscopic Cholecystectomy: Literature review of aetiopathogenesis, presentation, diagnosis and management. Sultan Qaboos Univ. Med. J. 2017, 17, e135–e146. [Google Scholar] [CrossRef]
- Wen, F.; Dong, Y.; Li, W.; Guo, Q.Y. Hemobilia After Laparoscopic Cholecystectomy: Imaging Features and Management of an Unusual Complication. Surg. Laparosc. Endosc. Percutaneous Tech. 2016, 26, e18–e24. [Google Scholar] [CrossRef]
- She, W.; Tsang, S.; Poon, R.; Cheung, T. Gastrointestinal bleeding of obscured origin due to cystic artery pseudoaneurysm. Asian J. Surg. 2017, 40, 320–323. [Google Scholar] [CrossRef]
- Rais, A.; Benabderrazik, B.; El Bouardi, N.; Akammar, A.; Haloua, M.; Alami, B.; Alaoui, M.Y.L.; Boubou, M.; Maaroufi, M. Cholecystitis-related cystic artery pseudoaneurysm: Case report. Radiol. Case Rep. 2024, 19, 2156–2159. [Google Scholar] [CrossRef]
- Praveen Kumar Sunkara, P.R.V.; Shah, P.K.; Rakshit, K.; Choudhary, S.R.; Bohidar, N.P.; Dubey, S.K. Rupture of Cystic Artery Pseudoaneurysm: A Rare Complication of Acute Cholecystitis. Indian J Surg. 2018, 80, 87–89. [Google Scholar] [CrossRef]
- Kulkarni, V.; Deshmukh, H.; Gupta, R. Pseudoaneurysm of anomalous cystic artery due to calculous cholecystitis. BMJ Case Rep. 2014, 2014, bcr2014207069. [Google Scholar] [CrossRef] [PubMed]
- Ouazzani, A.; Bataille, D.; Boutkhil, A.; Guérin, E.; Lefebvre, J.-C.; Vaneukem, P. Spontaneous Cystic Artery Rupture: A Rare Cause of Haemoperitoneum. Acta Chir. Belg. 2009, 109, 106–108. [Google Scholar] [CrossRef] [PubMed]
- Priya, H.; Anshul, G.; Alok, T.; Saurabh, K.; Ranjit, N.; Romesh, L.; Deborshi, S. Emergency cholecystectomy and hepatic arterial repair in a patient presenting with haemobilia and massive gastrointestinal haemorrhage due to a spontaneous cystic artery gallbladder fistula masquerading as a pseudoaneurysm. BMC Gastroenterol. 2013, 13, 43. [Google Scholar] [CrossRef]
- Patil, N.S.; Kumar, A.H.; Pamecha, V.; Gattu, T.; Falari, S.; Sinha, P.K.; Mohapatra, N. Cystic artery pseudoaneurysm—A rare complication of acute cholecystitis: Review of literature. Surg. Endosc. 2022, 36, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Sibria, D.; Elawad, M.; Aker, L.J.; Barah, A.; Almokdad, O.; Ladumor, S.B.; Mohamed, M.A.; Al Rashid, A.A.; Alahmad, Y.M.; Kambal, A.; et al. Cystic Artery Stump Pseudoaneurysm Following Laparoscopic Cholecystectomy: A Case Report. Cureus 2024, 16, e64551. [Google Scholar] [CrossRef]
- Nakase, Y.; Takagi, T.; Fukumoto, K.; Kassai, K.; Yamagami, T.; Itani, K.; Miyagaki, T. Hemobilia and cystic artery stump pseudoaneurysm associated with liver abscess after a laparoscopic cholecystectomy: Report of a case. Surg. Today 2008, 38, 567–571. [Google Scholar] [CrossRef]
- Lin, K.-T.; Lin, Z.-Y.; Huang, C.-C.; Yu, S.-Y.; Huang, J.-L.; Lin, J.-H.; Lin, Y.-R. Prehospital ultrasound scanning for abdominal free fluid detection in trauma patients: A systematic review and meta-analysis. BMC Emerg. Med. 2024, 24, 7. [Google Scholar] [CrossRef] [PubMed]
- Netherton, S.; Milenkovic, V.; Taylor, M.; Davis, P.J. Diagnostic accuracy of eFAST in the trauma patient: A systematic review and meta-analysis. CJEM 2019, 21, 727–738. [Google Scholar] [CrossRef]
- Tamburrini, S.; Consoli, L.; Garrone, M.; Sfuncia, G.; Lugarà, M.; Coppola, M.G.; Piccirillo, M.; Toto, R.; Stella, S.M.; Sofia, S.; et al. The “Black Pattern”, a Simplified Ultrasound Approach to Non-Traumatic Abdominal Emergencies. Tomography 2022, 8, 798–814. [Google Scholar] [CrossRef]
- Taouk, J.; Lacomblez, D.; Bosschaert, P. Doppler Ultrasound Diagnosis of Cystic Artery Pseudo-Aneurysm Causing Hemobilia. J. Belg. Soc. Radiol. 2024, 108, 50. [Google Scholar] [CrossRef]
- Robbie, R.; Amrita, R.; Adrian, C.; Alexander, S.; Shastri, S.; Maharaj, P. Cystic artery pseudoaneurysm. Radiol. Case Rep. 2024, 19, 1413–1418. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, A.; Jindal, G.; Khan, L.; Chaube, R. A Rare Case of Cystic Artery Pseudoaneurysm because of Cholecystitis Managed with Non-invasive Technique. Middle East J. Dig. Dis. 2023, 15, 285–288. [Google Scholar] [CrossRef]
- Scaglione, M.; Masala, S.; Iacobellis, F.; Tonerini, M.; Sica, G.; Liguori, C.; Saba, L.; Tamburrini, S. Imaging in Non-Traumatic Emergencies. Tomography 2023, 9, 1133–1136. [Google Scholar] [CrossRef]
- Wittenberg, A.; Minotti, A.J. CT Diagnosis of Traumatic Gallbladder Injury. AJR Am. J. Roentgenol. 2005, 185, 1573–1574. [Google Scholar] [CrossRef]
- Carey, F.; Rault, M.; Crawford, M.; Lewis, M.; Tan, K. Case report: Cystic artery pseudoaneurysm presenting as a massive per rectum bleed treated with percutaneous coil embolization. CVIR Endovasc. 2020, 3, 8. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, N.A.; Chawla, T.; Nadeem, M. Cystic artery pseudoaneurysm secondary to acute cholecystitis as cause of haemobilia. Case Rep. 2011, 2011, bcr0720114480. [Google Scholar] [CrossRef]
- Shelmerdine, S.C.; Ameli-Renani, S.; Lynch, J.O.; Gonsalves, M. Transarterial catheter embolisation for an unusual cause of upper gastrointestinal haemorrhage. BMJ Case Rep. 2015, 2015, bcr2014206837. [Google Scholar] [CrossRef]
- Ini’, C.; Distefano, G.; Sanfilippo, F.; Castiglione, D.G.; Falsaperla, D.; Giurazza, F.; Mosconi, C.; Tiralongo, F.; Foti, P.V.; Palmucci, S.; et al. Embolization for acute nonvariceal bleeding of upper and lower gastrointestinal tract: A systematic review. CVIR Endovasc. 2023, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Sarmento Costa, M.; Gravito-Soares, M.; Gravito-Soares, E.; Figueiredo, P. Unexpected cause of upper gastrointestinal bleeding: Beyond the typical complications of gallstone disease. Rev. Esp. Enfermedades Dig. 2024. [Google Scholar] [CrossRef] [PubMed]
- Giurazza, F.; Corvino, F.; Pane, F.; Di Serafino, M.; Niola, R. Combined DSA- and US-guided management of acute bleeding: Effectiveness of percutaneous glue embolization in six cases. J. Ultrasound 2024, 27, 179–184. [Google Scholar] [CrossRef]
- Heidari, A.; Ghane, Y.; Heidari, N.; Kasraianfard, A.; Kargar, M.; Moradi, A.M. Successful management of a ruptured cystic artery pseudoaneurysm with embolization and cholecystectomy: A case report. Clin. Case Rep. 2024, 12, e9427. [Google Scholar] [CrossRef]
- Anns, K.M.; Khan, F.; Aman, M.; Shahid, J.; Haq, T.U.I.; Memon, W.A.; Saeed, M.A.; Khalid, A.; Ahmed, K.A.H.M.; Akram, S. Pseudoaneurysm of cystic artery stump after laparoscopic cholecystectomy managed successfully with branch hepatic artery embolization using jail technique. J. Surg. Case Rep. 2024, 2024, rjae152. [Google Scholar] [CrossRef]
- Okamoto, S.; Matsui, Y.; Komoto, S.; Hiraki, T. Transarterial Embolization for Cystic Artery Pseudoaneurysm Caused by Hepatocellular Carcinoma Rupture in the Gallbladder: A Case Report. Cureus 2024, 16, e56400. [Google Scholar] [CrossRef]
- Saha, B.; Parasar, K.; Kodali, R.; Anwar, S. Ruptured cystic artery pseudoaneurysm: A clinical insight. BMJ Case Rep. 2024, 17, e259152. [Google Scholar] [CrossRef]
- Mie, T.; Sasaki, T.; Matsueda, K.; Okamoto, T.; Hirai, T.; Ishitsuka, T.; Yamada, M.; Nakagawa, H.; Furukawa, T.; Takeda, T.; et al. Ruptured cystic artery pseudoaneurysm after self-expandable metal stent placement for malignant biliary obstruction. DEN Open 2024, 4, e304. [Google Scholar] [CrossRef]
- Khan, H.; Lourdusamy, V.; Bansal, R. Cystic Artery Pseudoaneurysm Secondary to Cholecystitis: A Rare Cause of Hemobilia. Cureus 2023, 15, e39161. [Google Scholar]
- Kim, H.-C.; Jeong, Y.S.; Han, K.; Kim, G.M. Transcatheter arterial embolization of cystic artery bleeding. Front. Surg. 2023, 10, 1160149. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-L.; Hsieh, C.-T.; Yeh, Y.-J.; Liu, H. Cystic artery pseudoaneurysm: A case report. World J. Clin. Cases 2023, 11, 242–248. [Google Scholar] [CrossRef]
- Williams, T.; Maher, A.; Redmond, K.; Yeung, S.; Ko, B.S. Hemobilia in the setting of cystic artery pseudoaneurysm secondary to type I Mirizzi syndrome. Clin. J. Gastroenterol. 2023, 16, 605–609. [Google Scholar] [CrossRef]
- Zainab, R.; Tahir, M.M.; Khalid, D.; Ali, M.; Zaidi, M.; Abro, K. Transarterial embolisation of cystic artery pseudo aneurysm: A rare complication of acute cholecystitis. J. Pak. Med. Assoc. 2023, 73, 1106–1107. [Google Scholar]
- Itagaki, Y.; Yamamoto, K.; Kikuchi, T.; Takano, H.; Nishigami, K.; Fukunaga, A.; Ichimura, T.; Manase, H.; Hirano, S. Laparoscopic cholecystectomy after transcatheter arterial embolisation for haemobilia due to a pseudoaneurysm in the gallbladder: A case report. SAGE Open Med. Case Rep. 2023, 11, 2050313X231166777. [Google Scholar] [CrossRef]
- Christodoulou, P.; Liapis, S.-C. Early Rupture of Iatrogenic Cystic Artery Pseudoaneurysm After Unsuccessful Laparoscopic Cholecystectomy: A Case Report. Cureus 2022, 14, e22865. [Google Scholar] [CrossRef]
- Fukushima, R.; Ishii, N.; Harimoto, N.; Araki, K.; Watanabe, A.; Tsukagoshi, M.; Hagiwara, K.; Yamanaka, T.; Shirabe, K. A case of Mirizzi syndrome accompanied by a pseudoaneurysm that ruptured into the gallbladder: Successfully treated by embolization of aneurysm and sequential surgery. Surg. Case Rep. 2022, 8, 111. [Google Scholar] [CrossRef] [PubMed]
- Amakye, D.O.; Atemnkeng, N.; Hama, E.; Person, E.B. A Case of Massive Lower Gastrointestinal Bleed from a Cystic Artery Pseudoaneurysm Bleeding through a Cholecystocolic Fistula. Am. J. Case Rep. 2021, 22, e931921-1–e931921-4. [Google Scholar] [CrossRef] [PubMed]
- Mahalingam, S.; Shaikh, O.H.; Kumbhar, U.S.; Mohan, A. Cystic artery pseudoaneurysm due to carcinoma of the gallbladder. BMJ Case Rep. 2021, 14, e241714. [Google Scholar] [CrossRef]
- Nguyen, D.; Goodwin, J.S.; Bhowmik, N.; Boiteau, G.; Potts, J. Acute Hemorrhagic Cholecystitis with Large Hemoperitoneum: Treatment with Microcoil Embolization and Subsequent Cholecystectomy. J. Radiol. Case Rep. 2021, 15, 25–34. [Google Scholar] [CrossRef]
- Acharya, S.; Mukherjee, I.; Anwar, S.; Lan, G.; Polavarapu, A. Haemobilia Secondary to Spontaneous Cystic Artery-Gallbladder Fistula: A Unique Gastrointestinal Anomaly. Cureus 2020, 12, e9457. [Google Scholar] [CrossRef] [PubMed]
- Leshen, M.; Hubert, J.; Cantos, A. Pediatric cystic artery pseudoaneurysm embolization. Clin. Imaging 2020, 61, 80–83. [Google Scholar] [CrossRef]
- Proença, A.L.; Gomes, F.V.; Costa, N.; Bilhim, T.; Luz, J.H.; Coimbra, É. Transarterial Embolization of Iatrogenic Cystic Artery Pseudoaneurysm. GE-Port. J. Gastroenterol. 2020, 27, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Yam, M.K.; Sim, S.W.; Tam, K.Y.; Li, Y.L. A 51-year-old female presenting with shock due to hemorrhagic cholecystitis. Radiol. Case Rep. 2020, 15, 2547–2549. [Google Scholar] [CrossRef]
- Rossini, M.; Bonati, E.; Cozzani, F.; Marcato, C.; Del Rio, P. Hemobilia due to cystic artery pseudoaneurysm following cholecystectomy: Diagnosis and management, a case report. Acta Biomed. 2019, 90, 595–598. [Google Scholar] [CrossRef]
- Sada, D.M.; Metwalli, Z.A. Cystic Artery Hemorrhage after Cholecystostomy Catheter Exchange Treated with Transcatheter Embolization. Semin. Interv. Radiol. 2019, 36, 108–110. [Google Scholar] [CrossRef]
- Tanaka, T.; Takakura, K.; Maruyama, Y.; Hidaka, A.; Nakano, M.; Torisu, Y.; Saruta, M. Hemobilia Derived from Cystic Artery Pseudoaneurysm. Case Rep. Gastroenterol. 2019, 13, 89–94. [Google Scholar] [CrossRef]
- Kuzman, M.S.; Adiamah, A.; Higashi, Y.; Gomez, D. Rare case of cystic artery pseudoaneurysm. BMJ Case Rep. 2018, 2018, bcr-2017-223789. [Google Scholar] [CrossRef] [PubMed]
- Maddineni, S.; Lim, M.M.D.; McCabe, S.; Rozenblit, G. Transcatheter embolization of a cystic artery pseudoaneurysm in a cirrhotic patient with perforated acute cholecystitis. Indian J. Radiol. Imaging 2017, 27, 521–523. [Google Scholar] [CrossRef]
- Tapnio, R.H.; Kolber, M.K.; Shukla, P.A.; Berkowitz, E. Transcatheter Embolization of Cystic Artery Pseudoaneurysms Secondary to Acute Cholecystitis. Vasc. Endovasc. Surg. 2017, 51, 498–500. [Google Scholar] [CrossRef]
- Thillai, M.; Sethi, P.; Menon, R.N.; Kader, N.P. Cystic artery pseudoaneurysm following acute necrotising pancreatitis. BMJ Case Rep. 2017, 2017, bcr-2016-218891. [Google Scholar] [CrossRef] [PubMed]
- Trombatore, C.; Scilletta, R.; Bellavia, N.; Trombatore, P.; Lio, V.M.S.; Petrillo, G.; Di Cataldo, A. Acute hemobilia from a pseudoaneurysm of the cystic artery arising from the left hepatic artery: Case report and literature review. Int. J. Surg. Case Rep. 2017, 37, 60–64. [Google Scholar] [CrossRef]
- Hall, T.C.; De Rover, W.S.; Habib, S.; Kumaran, M. Cystic artery pseudoaneurysm secondary to acute cholecystitis: An unusual cause for haemobilia. BJR|Case Rep. 2016, 2, 20150423. [Google Scholar] [CrossRef]
- Liu, B.; Lewis, A.R.; Ward, T.J. Cystic Artery Pseudoaneurysm. J. Vasc. Interv. Radiol. 2016, 27, 694. [Google Scholar] [CrossRef] [PubMed]
- Aljiffry, M.M.; Almulhim, A.N.; Jamal, M.H.; Hassanain, M.M. Acute cholecystitis presenting with massive intra-abdominal haemorrhage. J. Surg. Case Rep. 2014, 2014, rju019. [Google Scholar] [CrossRef]
- Kumar, A.; Sheikh, A.; Partyka, L.; Contractor, S. Cystic artery pseudoaneurysm presenting as a complication of laparoscopic cholecystectomy treated with percutaneous thrombin injection. Clin. Imaging 2014, 38, 522–525. [Google Scholar] [CrossRef]
- Mokrane, F.-Z.; Alba, C.G.; Lebbadi, M.; Mejdoubi, M.; Moulabbi, M.; Lombard, F.; Lengellé, F.; Aveillan, M. Pseudoaneurism of the cystic artery treated with hyperselective embolisation alone. Diagn. Interv. Imaging 2013, 94, 641–643. [Google Scholar] [CrossRef] [PubMed]
- Nana, G.R.; Gibson, M.; Speirs, A.; Ramus, J.R. Upper gastrointestinal bleeding: A rare complication of acute cholecystitis. Int. J. Surg. Case Rep. 2013, 4, 761–764. [Google Scholar] [CrossRef]
- Chong, J.J.; O’Connell, T.; Munk, P.L.; Yang, N.; Harris, A.C. Case of the Month #176: Pseudoaneurysm of the Cystic Artery. Can. Assoc. Radiol. J. 2012, 63, 153–155. [Google Scholar] [CrossRef]
- Petrou, A.; Brennan, N.; Soonawalla, Z.; Silva, M.A. Hemobilia Due to Cystic Artery Stump Pseudoaneurysm Following Laparoscopic Cholecystectomy: Case Presentation and Literature Review. Int. Surg. 2012, 97, 140–144. [Google Scholar] [CrossRef]
- Desai, A.; Saunders, M.; Anderson, H.; Howlett, D. Successful Transcatheter Arterial Embolisation of a Cystic Artery Pseudoaneurysm Secondary to Calculus Cholecystitis: A Case Report. J. Radiol. Case Rep. 2010, 4, 18–22. [Google Scholar] [CrossRef]
- Hague, J.; Brennand, D.; Raja, J.; Amin, Z. Cystic Artery Pseudoaneurysms in Hemorrhagic Acute Cholecystitis. Cardiovasc. Interv. Radiol. 2010, 33, 1287–1290. [Google Scholar] [CrossRef] [PubMed]
- Nkwam, N.; Heppenstall, K. Unruptured Pseudoaneurysm of the cystic artery associated with acute calculus cholecystitis. J. Surg. Case Rep. 2010, 2010, 4. [Google Scholar] [CrossRef]
- Contini, S.; Uccelli, M.; Sassatelli, R.; Pinna, F.; Corradi, D. Gallbladder ulcer eroding the cystic artery: A rare cause of hemobilia. Am. J. Surg. 2009, 198, e17–e19. [Google Scholar] [CrossRef] [PubMed]
- Mullen, R.; Suttie, S.A.; Bhat, R.; Evgenikos, N.; Yalamarthi, S.; McBride, K.D. Microcoil Embolisation of Mycotic Cystic Artery Pseudoaneurysm: A Viable Option in High-Risk Patients. Cardiovasc. Interv. Radiol. 2009, 32, 1275–1279. [Google Scholar] [CrossRef] [PubMed]
- Shimada, K.; Sakamoto, Y.; Esaki, M.; Kosuge, T. Pseudoaneurysm of the Cystic Artery Associated with Xanthogranulomatous Cholecystitis. Dig. Surg. 2008, 25, 8–9. [Google Scholar] [CrossRef]
- Osada, H.; Honda, N.; Takahashi, T.; Oku, S.; Watanabe, W.; Okada, T.; Ohno, H.; Hondo, M.; Nishimura, K. Arteriovenous malformation of the gallbladder: CT and angiographic findings. Radiat. Med. 2007, 25, 73–75. [Google Scholar] [CrossRef]
- Saluja, S.S.; Ray, S.; Gulati, M.S.; Pal, S.; Sahni, P.; Chattopadhyay, T.K. Acute cholecystitis with massive upper gastrointestinal bleed: A case report and review of the literature. BMC Gastroenterol. 2007, 7, 12. [Google Scholar] [CrossRef]
- Maeda, A.; Kunou, T.; Saeki, S.; Aono, K.; Murata, T.; Niinomi, N.; Yokoi, S. Pseudoaneurysm of the cystic artery with hemobilia treated by arterial embolization and elective cholecystectomy. J. Hepato-Biliary-Pancreat. Surg. 2002, 9, 755–758. [Google Scholar] [CrossRef]
- Delgadillo, X.; Berney, T.; de Perrot, M.; Didier, D.; Morel, P. Successful Treatment of a Pseudoaneurysm of the Cystic Artery with Microcoil Embolization. J. Vasc. Interv. Radiol. JVIR 1999, 10, 789–792. [Google Scholar] [CrossRef]
- England, R.; Marsh, P.; Ashleigh, R.; Martin, D. Case report: Pseudoaneurysm of the cystic artery: A rare cause of haemobilia. Clin. Radiol. 1998, 53, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Akatsu, T.; Tanabe, M.; Shimizu, T.; Handa, K.; Kawachi, S.; Aiura, K.; Ueda, M.; Shimazu, M.; Kitajima, M. Pseudoaneurysm of the Cystic Artery Secondary to Cholecystitis as a Cause of Hemobilia: Report of a Case. Surg. Today 2007, 37, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Chen, L.; Zhao, B.; Huang, H.; Lu, Z.; Su, H. Transcatheter arterial embolization for massive hemobilia with N-butyl cyanoacrylate (NBCA) Glubran 2. Acta Radiol. 2022, 63, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Saldinger, P.F.; Wang, J.Y.; Boyd, C.; Lang, E. Cystic artery stump pseudoaneurysm following laparoscopic cholecystectomy. Surgery 2002, 131, 585–586. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiralongo, F.; Castiglione, D.G.; Comune, R.; Palmucci, S.; Bortolotto, C.; De Simone, F.; Pezzullo, F.; Ferrandino, G.; Sica, G.; Ricci, P.; et al. Cystic Artery Bleeding: Imaging Insights and Systematic Review of Endovascular Management. Gastrointest. Disord. 2025, 7, 20. https://doi.org/10.3390/gidisord7010020
Tiralongo F, Castiglione DG, Comune R, Palmucci S, Bortolotto C, De Simone F, Pezzullo F, Ferrandino G, Sica G, Ricci P, et al. Cystic Artery Bleeding: Imaging Insights and Systematic Review of Endovascular Management. Gastrointestinal Disorders. 2025; 7(1):20. https://doi.org/10.3390/gidisord7010020
Chicago/Turabian StyleTiralongo, Francesco, Davide Giuseppe Castiglione, Rosita Comune, Stefano Palmucci, Chandra Bortolotto, Fiore De Simone, Filomena Pezzullo, Giovanni Ferrandino, Giacomo Sica, Paolo Ricci, and et al. 2025. "Cystic Artery Bleeding: Imaging Insights and Systematic Review of Endovascular Management" Gastrointestinal Disorders 7, no. 1: 20. https://doi.org/10.3390/gidisord7010020
APA StyleTiralongo, F., Castiglione, D. G., Comune, R., Palmucci, S., Bortolotto, C., De Simone, F., Pezzullo, F., Ferrandino, G., Sica, G., Ricci, P., Scaglione, M., Basile, A., & Tamburrini, S. (2025). Cystic Artery Bleeding: Imaging Insights and Systematic Review of Endovascular Management. Gastrointestinal Disorders, 7(1), 20. https://doi.org/10.3390/gidisord7010020