Percutaneous Nephrostomy versus Retrograde Ureteral Stent for Management of Malignant Ureteral Obstruction in Adults: A Systematic Review of the Literature
Abstract
:Introduction
Methods
Search method for identification of the studies
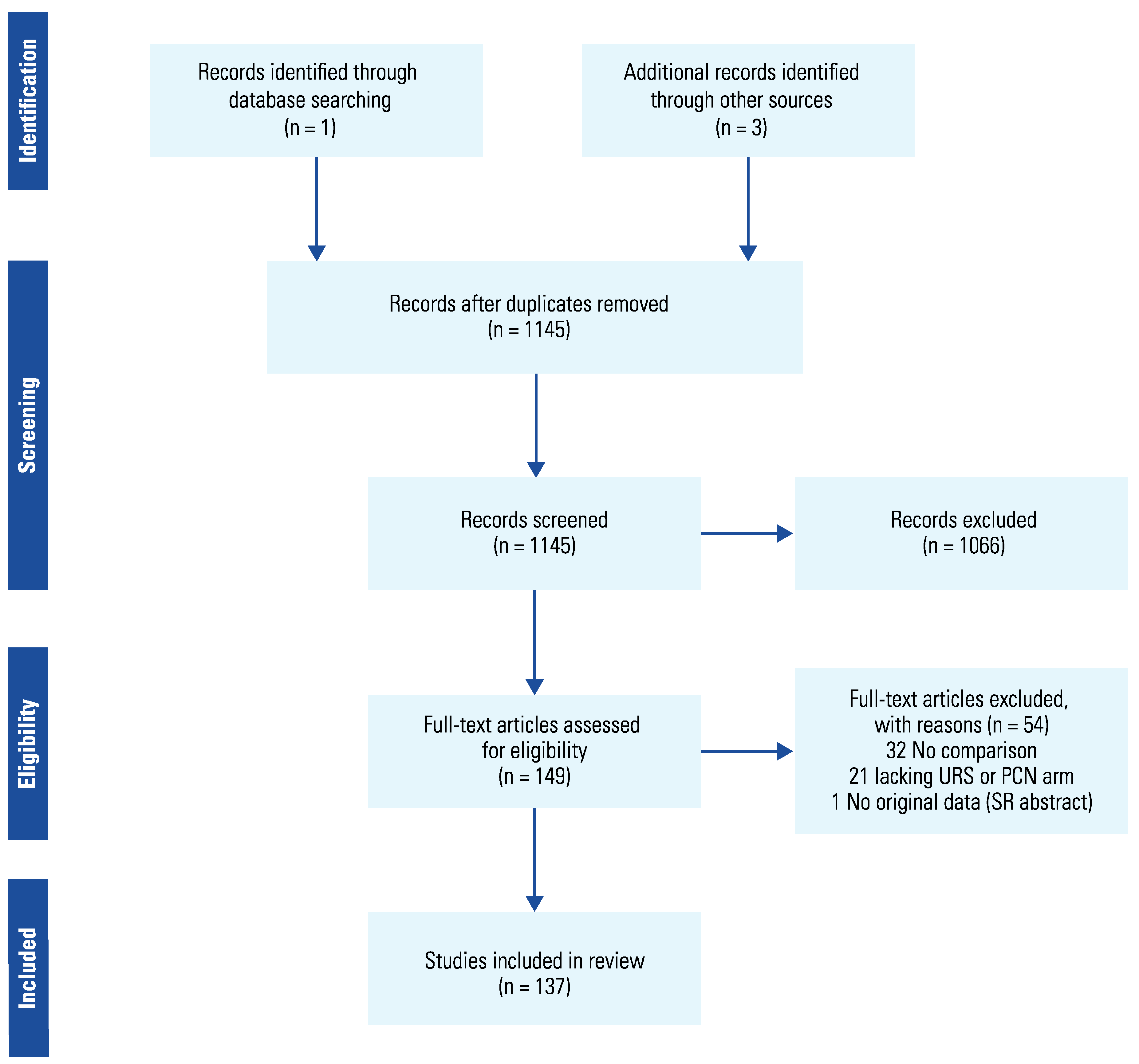
Selection of the studies
Data Extraction
Quality assessment
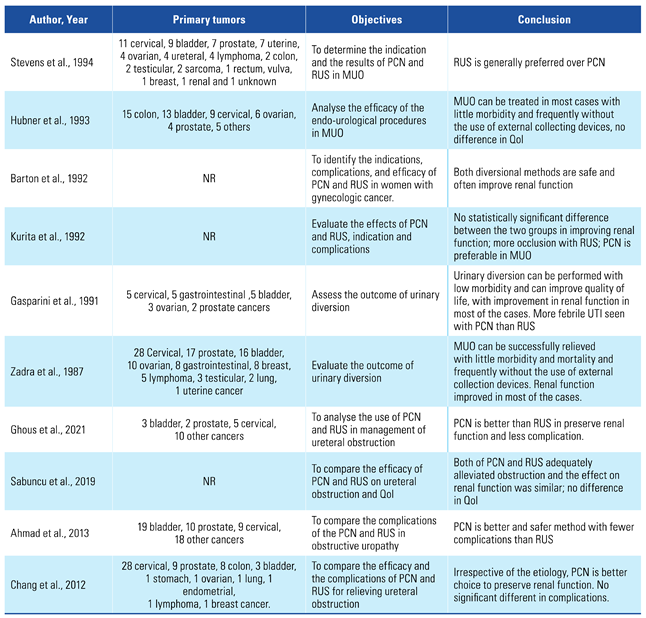
Results and Discussion
Preservation of renal function

{kind=link}



 |
 |
 |
 |
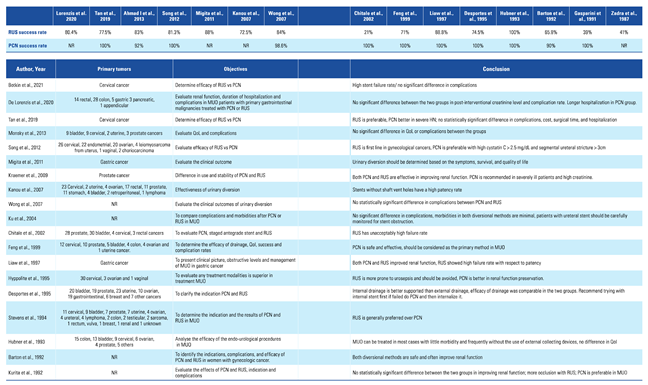
Technical success rate
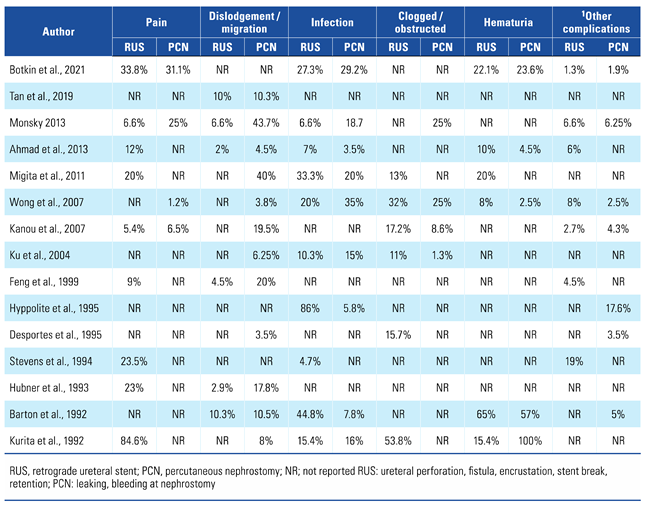
Complication rate
Conversion into another diversional method
Residual hydronephrosis
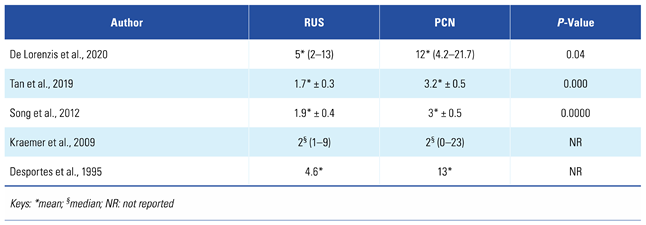
Length of hospital stay
Procedure time
Financial cost
Quality of life assessment post intervention
Limitations
Conclusion
Conflicts of Interest
References
- Kouba, E.; Wallen, E.M.; Pruthi, R.S. Management of ureteral obstruction due to advanced malignancy: optimizing therapeutic and palliative outcomes. J Urol. 2008, 180, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Lund, B.; Hansen, H.H. Hydronephrosis in advanced ovarian carcinoma. Gynecol Oncol. 1989, 35, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Russo, P. Urologic emergencies in the cancer patient. Semin Oncol. 2000, 27, 284. [Google Scholar] [PubMed]
- Holden, S.; McPhee, M.; Grabstald, H. The rationale of urinary diversion in cancer patients. J Urol. 1979, 121, 19. [Google Scholar] [CrossRef] [PubMed]
- Feng, M.I.; Bellman, G.C.; Shapiro, C.E. Management of ureteral obstruction secondary to pelvic malignancies. J Endourol. 1999, 13, 521. [Google Scholar] [CrossRef] [PubMed]
- Sharer, W.; Grayhack, J.T.; Graham, J. Palliative urinary diversion for malignant ureteral obstruction. J Urol. 1978, 120, 162. [Google Scholar] [CrossRef] [PubMed]
- Fiuk, J.; Bao, Y.; Calleary, J.G.; Schwartz, B.F.; Denstedt, J.D. The use of internal stents in chronic ureteral obstruction. J Urol. 2015, 193, 1092–1100. [Google Scholar] [CrossRef] [PubMed]
- Donat, S.M.; Russo, P. Ureteral decompression in advanced nonurologic malignancies. Ann Surg Oncol. 1996, 3, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Cronan, J.J. Contemporary concepts in imaging urinary tract obstruction. Radiol Clin North Am. 1991, 29, 527. [Google Scholar] [CrossRef]
- Hyams, E.S.; Shah, O. Malignant extrinsic ureteral obstruction: a survey of urologists and medical oncologists regarding treatment patterns and preferences. Urology (Ridgewood, N.J.) 2008, 72, 51–56. [Google Scholar] [CrossRef]
- Ganatra, A.M.; Loughlin, K.R. The management of malignant ureteral obstruction treated with ureteral stents. J Urol. 2005, 174, 2125. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, E.M.; Nason, G.J.; Kiely, E.A. Urological Management of Extramural Malignant Ureteric Obstruction: A Survey of Irish Urologists. Curr Urol. 2017, 11, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.; Tao, Z.; Bian, X.; Zhao, Y.; Wang, N.; Chen, X.; et al. Ureteral stent placement and percutaneous nephrostomy in the management of hydronephrosis secondary to cervical cancer. Eur J Obstet Gynecol Reprod Biol. 2019, 241, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Monsky, W.L.; Molloy, C.; Jin, B.; Nolan, T.; Fernando, D.; Loh, S.; et al. Quality-of-life assessment after palliative interventions to manage malignant ureteral obstruction. Cardiovasc Intervent Radiol. 2013, 36, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Fei, X.; Song, Y. Percutaneous nephrostomy versus indwelling ureteral stent in the management of gynecological malignancies. Int J Gynecol Cancer. 2012, 22, 697–702. [Google Scholar]
- Migita, K.; Watanabe, A.; Samma, S.; Ohyama, T.; Ishikawa, H.; Kagebayashi, Y. Clinical outcome and management of ureteral obstruction secondary to gastric cancer. World J Surg. 2011, 35, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, P.C.; Borre, M. Relief of upper urinary tract obstruction in patients with cancer of the prostate [article in Danish]. Ugeskr Laeger. 2009, 171, 873–876. [Google Scholar] [PubMed]
- Kanou, T.; Fujiyama, C.; Nishimura, K.; Tokuda, Y.; Uozumi, J.; Masaki, Z. Management of extrinsic malignant ureteral obstruction with urinary diversion. Int J Urol. 2007, 14, 689–692. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.; Cleeve, L.K.; Milner, A.D.; Pitman, A.G. Malignant ureteral obstruction: outcomes after intervention. Have things changed? J Urol. 2007, 178, 178–183. [Google Scholar]
- Ku, J.H.; Lee, S.W.; Jeon, H.G.; Kim, H.H.; Oh, S. Percutaneous nephrostomy versus indwelling ureteral stents in the management of extrinsic ureteral obstruction in advanced malignancies: are there differences? Urology 2004, 64, 895–899. [Google Scholar] [CrossRef]
- Chitale, S.V.; Scott-Barrett, S.; Ho, E.T.S.; Burgess, N.A. The management of ureteric obstruction secondary to malignant pelvic disease. Clin Radiol. 2002, 57, 1118–1121. [Google Scholar] [CrossRef]
- Liaw, C.C.; Chuang, C.K.; Chen, J.S.; Chang, H.K. Gastric cancer with obstructive uropathy: clinical experience with 17 cases. Changgeng Yi Xue Za Zhi. 1997, 20, 286–292. [Google Scholar]
- Hyppolite, J.C.; Daniels, I.D.; Friedman, E.A. Obstructive uropathy in gynecologic malignancy. Detrimental effect of intraureteral stent placement and value of percutaneous nephrostomy. ASAIO J. 1995, 41, 318–323. [Google Scholar] [CrossRef]
- Desportes, L.; Blanchet, P.; Benoit, G.; Lecouturier, S.; Langloys, J.; Decaux, A.; et al. Neoplasic ureteral obstruction: drainage by percutaneous nephrostomy or double J stent [Article in French]. Presse Med. 1995, 24, 1332–1336. [Google Scholar] [PubMed]
- Stevens, A.; van Driel, M.F.; Klein, J.P.; de Ruiter, A.J.; Mensink, H.J. Endo-urological drainage in urinary outflow obstruction caused by cancer [Article in Dutch]. Ned Tijdschr Geneeskd. 1994, 138, 522–525. [Google Scholar] [PubMed]
- Hubner, W.A.; Plas, E.G.; Porpaczy, P. Hydronephrosis in malignant tumors: rationale and efficiency of endo-urological diversions. Eur J Surg Oncol. 1993, 19, 27–32. [Google Scholar]
- Barton, D.P.J.; Morse, S.S.; Fiorica, J.V.; Hoffman, M.S.; Roberts, W.S.; Cavanagh, D. Percutaneous nephrostomy and ureteral stenting in gynecologic malignancies. Obstet Gynecol. 1992, 80, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Kurita, Y.; Ihara, H.; Kageyama, S.; Ueda, D.; Ushiyama, T.; Ohta, N.; et al. Percutaneous nephrostomy versus the placement of double pigtail ureteral stent for the treatment of postrenal failure secondary to malignancies [Article in Japanese]. Nihon Jinzo Gakkai Shi. 1992, 34, 909–912. [Google Scholar]
- Gasparini, M.; Carroll, P.; Stoller, M. Palliative percutaneous and endoscopic urinary diversion for malignant ureteral obstruction. Urology 1991, 38, 408–412. [Google Scholar] [CrossRef]
- Zadra, J.A.; Jewett, M.A.; Keresteci, A.G.; Rankin, J.T.; St Louis, E.; Grey, R.R.; et al. Nonoperative urinary diversion for malignant ureteral obstruction. Cancer 1987, 60, 1353–1357. [Google Scholar] [CrossRef]
- Botkin, H.E.; Faidley, K.N.; Loeffler, B.T.; Mott, S.L.; Hill, E.K.; Erickson, B.A. Longitudinal outcomes from conservative management of cervical cancer associated ureteral obstruction. Urology 2021, 158, 208–214. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzis, E.; Lievore, E.; Turetti, M.; Gallioli, A.; Galassi, B.; Boeri, L.; et al. Ureteral stent and percutaneous nephrostomy in managing malignant ureteric obstruction of gastrointestinal origin: a 10 years’ experience. Gastrointest Disord (Basel). 2020, 2, 456–468. [Google Scholar] [CrossRef]
- Ghous, M.H.; Afzal, S.; Malik, S.M.; Arooj, M. Analysis of use of percutaneous nephrostomy and ureteral stenting in management of ureteral obstruction. Pak J Med Sci. 2021, 15, 3024–3027. [Google Scholar] [CrossRef]
- The effect of ureteral double J stent and percutaneous nephrostomy catheter use on renal function and quality of life in patients with unilateral hydronephrosis without renal insufficiency. Conference: 5th Meeting of the EAU Section of Urolithiasis. Italy. Eur Urol. 2019; 18, (Suppl. 7), e3006.
- Ahmad, I.; Pansota, M.; Saeed Tariq, M.; Shahzad Saleem, M.; Ali Tabassum, S.; Hussain, A. Comparison between double J (DJ) ureteral stenting and percutaneous nephrostomy (PCN) in obstructive uropathy. Pak J Med Sci. 2013, 29, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.C.; Tang, S.H.; Chuang, F.P.; Wu, S.T.; Sun, G.H.; Yu, D.S.; et al. Comparison between the use of percutaneous nephrostomy and internal ureteral stenting in the management of long-term ureteral obstructions. Urol Sci. 2012, 23, 82–84. [Google Scholar] [CrossRef]
- Docimo, S.G.; Dewolf, W.C. High failure rate of indwelling ureteral stents in patients with extrinsic obstruction: experience at 2 institutions. J Urol. 1989, 142 Pt 1, 277. [Google Scholar] [CrossRef]
- Jenkins, C.N.J.; Marcus, A.J. The value of antegrade stenting for lower ureteric obstruction. J R Soc Med. 1995, 88, 446–449. [Google Scholar]
- Song, S.H.; Pak, S.; Jeong, I.G.; Kim, K.S.; Park, H.K.; Kim, C.; et al. Outcomes of stent-change therapy for bilateral malignancy-related ureteral obstruction. Int Urol Nephrol. 2015, 47, 19–24. [Google Scholar] [CrossRef]
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2023 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.
Share and Cite
Eshumani, W.; Roumiguié, M.; Black, P. Percutaneous Nephrostomy versus Retrograde Ureteral Stent for Management of Malignant Ureteral Obstruction in Adults: A Systematic Review of the Literature. Soc. Int. Urol. J. 2023, 4, 401-414. https://doi.org/10.48083/AYKF2124
Eshumani W, Roumiguié M, Black P. Percutaneous Nephrostomy versus Retrograde Ureteral Stent for Management of Malignant Ureteral Obstruction in Adults: A Systematic Review of the Literature. Société Internationale d’Urologie Journal. 2023; 4(5):401-414. https://doi.org/10.48083/AYKF2124
Chicago/Turabian StyleEshumani, Walid, Mathieu Roumiguié, and Peter Black. 2023. "Percutaneous Nephrostomy versus Retrograde Ureteral Stent for Management of Malignant Ureteral Obstruction in Adults: A Systematic Review of the Literature" Société Internationale d’Urologie Journal 4, no. 5: 401-414. https://doi.org/10.48083/AYKF2124
APA StyleEshumani, W., Roumiguié, M., & Black, P. (2023). Percutaneous Nephrostomy versus Retrograde Ureteral Stent for Management of Malignant Ureteral Obstruction in Adults: A Systematic Review of the Literature. Société Internationale d’Urologie Journal, 4(5), 401-414. https://doi.org/10.48083/AYKF2124