
Sleep and Adolescent Depression


{kind=link}
Abstract
:1. Introduction
1.1. Why Study Depression in Adolescence?
Prevalence
1.2. Emergence of Major Depressive Disorder
2. Why Sleep and (Adolescent) Depression?
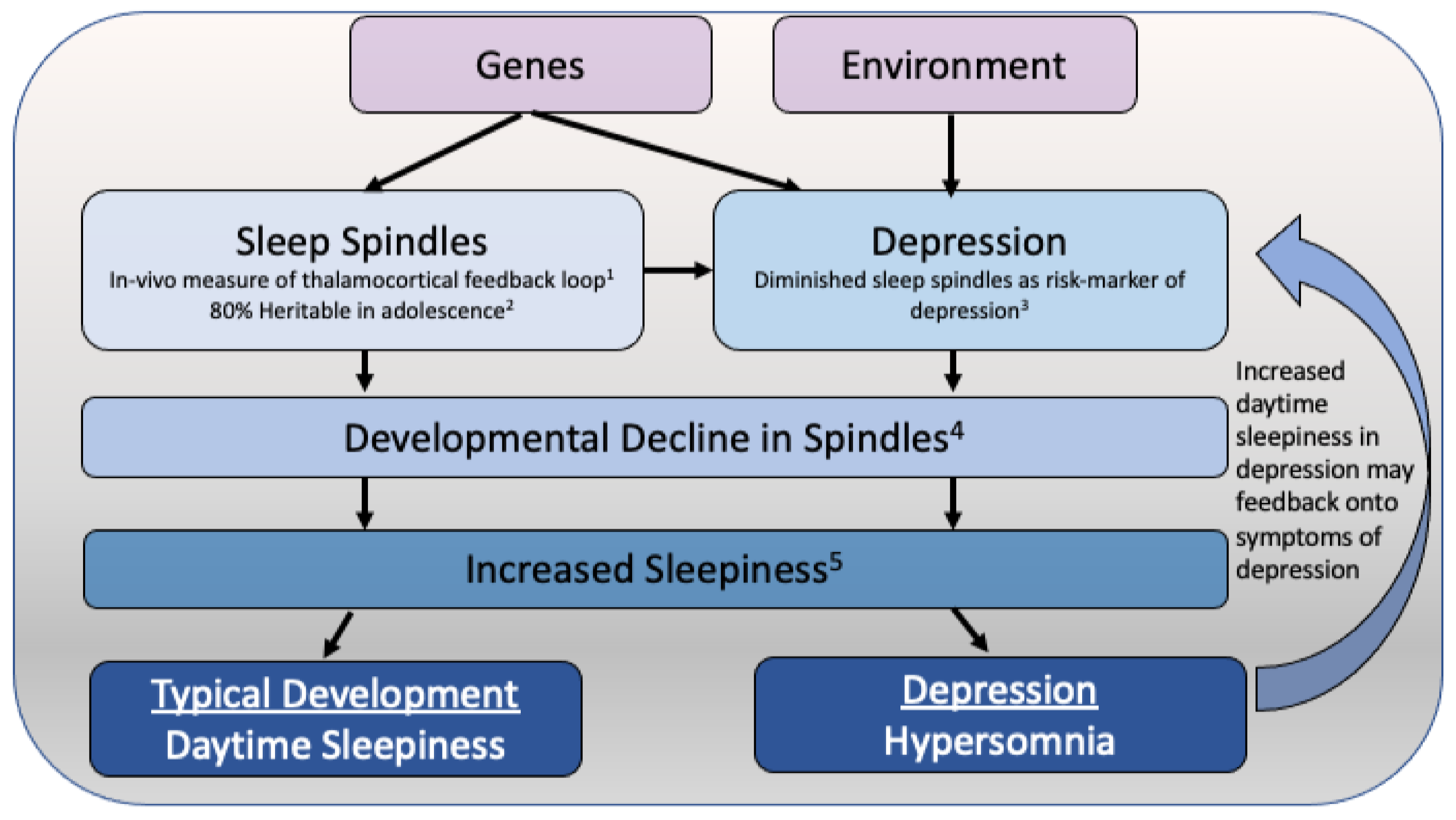
Theoretical Model of Hypersomnia in Adolescent Depression
3. Sleep EEG Neurophysiology
3.1. Slow Wave Activity
3.2. Sleep Spindles
3.3. REM Sleep
4. Sleep and the Sleep EEG as a Biomarker in Depression
5. Sleep and Depression: A Bi-Directional Relationship?
6. Sleep, Depression, Media Use and Physical Activity
7. Sleep Timing and Depression
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2022. [Google Scholar]
- Essau, C.; Dobson, K.S. Epidemiology of depressive disorders. In Depressive Disorders in Children and Adolescents: Epidemiology, Risk Factors, and Treatment; Essau, C.A., Petermann, F., Eds.; Jason Aronson, Inc. Publishers: Lanham, MD, USA, 1999; pp. 69–103. [Google Scholar]
- Mendlewicz, J. Sleep disturbances: Core symptoms of major depressive disorder rather than associated or comorbid disorders. World J. Biol. Psychiatry 2009, 10, 269–275. [Google Scholar] [CrossRef]
- Palagini, L.; Baglioni, C.; Ciapparelli, A.; Gemignani, A.; Riemann, D. REM sleep dysregulation in depression: State of the art. Sleep Med. Rev. 2013, 17, 377–390. [Google Scholar] [CrossRef]
- Alsaad, A.J.; Azhar, Y.; Al Nasser, Y. Depression in Children; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Birmaher, B.; Axelson, D. Course and outcome of bipolar spectrum disorder in children and adolescents: A review of the existing literature. Dev. Psychopathol. 2006, 18, 1023–1035. [Google Scholar] [CrossRef]
- World Health Organization. The Global Burden of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2008; p. 146. [Google Scholar]
- Malhi, G.S.; Mann, J.J. Depression. Lancet 2018, 392, 2299–2312. [Google Scholar] [CrossRef]
- Kessler, R.C.; Bromet, E.J. The epidemiology of depression across cultures. Ann. Rev. Public Health 2013, 34, 119–138. [Google Scholar] [CrossRef]
- Bromet, E.; Andrade, L.H.; Hwang, I.; Sampson, N.A.; Alonso, J.; de Girolamo, G.; de Graaf, R.; Demyttenaere, K.; Hu, C.; Iwata, N.; et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011, 9, 90. [Google Scholar] [CrossRef]
- Selph, S.S.; McDonagh, M.S. Depression in Children and Adolescents: Evaluation and Treatment. Am. Fam. Physician 2019, 100, 609–617. [Google Scholar]
- Thapar, A.; Collishaw, S.; Pine, D.S.; Thapar, A.K. Depression in adolescence. Lancet 2012, 379, 1056–1067. [Google Scholar] [CrossRef]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Heim, C.; Binder, E.B. Current research trends in early life stress and depression: Review of human studies on sensitive periods, gene-environment interactions, and epigenetics. Exp. Neurol. 2012, 233, 102–111. [Google Scholar] [CrossRef]
- 15 Birmaher, B.; Ryan, N.D.; Williamson, D.E.; Brent, D.A.; Kaufman, J.; Dahl, R.E.; Perel, J.; Nelson, B. Childhood and adolescent depression: A review of the past 10 years. Part I. J. Am. Acad. Child Adolesc. Psychiatry 1996, 35, 1427–1439. [Google Scholar] [CrossRef]
- Dopheide, J.A. Recognizing and treating depression in children and adolescents. Am. J. Health Syst. Pharm. 2006, 63, 233–243. [Google Scholar] [CrossRef]
- Mullen, S. Major depressive disorder in children and adolescents. Ment. Health Clin. 2018, 8, 275–283. [Google Scholar] [CrossRef]
- Hawton, K.; Saunders, K.E.A.; O’Connor, R.C. Self-harm and suicide in adolescents. Lancet 2012, 379, 2373–2382. [Google Scholar] [CrossRef]
- Morken, I.S.; Dahlgren, A.; Lunde, I.; Toven, S. The effects of interventions preventing self-harm and suicide in children and adolescents: An overview of systematic reviews. F1000Research 2019, 8, 890. [Google Scholar] [CrossRef]
- Costello, E.J.; Erkanli, A.; Angold, A. Is there an epidemic of child or adolescent depression? J. Child Psychol. Psychiatry 2006, 47, 1263–1271. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Rohde, P.; Seeley, J.R. Major depressive disorder in older adolescents: Prevalence, risk factors, and clinical implications. Clin. Psychol. Rev. 1998, 18, 765–794. [Google Scholar] [CrossRef]
- Lopez, J.; Hoffmann, R.; Armitage, R. Reduced sleep spindle activity in early-onset and elevated risk for depression. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 934–943. [Google Scholar] [CrossRef]
- Zisook, S.; Rush, A.J.; Albala, A.; Alpert, J.; Balasubramani, G.K.; Fava, M.; Husain, M.; Sackeim, H.; Trivedi, M.; Wisniewski, S. Factors that differentiate early vs. later onset of major depression disorder. Psychiatry Res. 2004, 129, 127–140. [Google Scholar] [CrossRef]
- Bertha, E.A.; Balázs, J. Subthreshold depression in adolescence: A systematic review. Eur. Child Adolesc. Psychiatry 2013, 22, 589–603. [Google Scholar] [CrossRef]
- Kessler, R.C.; McGonagle, K.A.; Zhao, S.; Nelson, C.B.; Hughes, M.; Eshleman, S.; Wittchen, H.U.; Kendler, K.S. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch. Gen. Psychiatry 1994, 51, 8–19. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Rohde, P.; Seeley, J.R. Psychosocial characteristics of adolescents with a history of suicide attempt. J. Am. Acad. Child Adolesc. Psychiatry 1993, 32, 60–68. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Duncan, E.M.; Stanton, A.K.; Hautzinger, M. Age at first onset for non-bipolar depression. J. Abnorm. Psychol. 1986, 95, 378–383. [Google Scholar] [CrossRef]
- Shorey, S.; Ng, E.D.; Wong, C.H.J. Global prevalence of depression and elevated depressive symptoms among adolescents: A systematic review and meta-analysis. Br. J. Clin. Psychol. 2022, 61, 287–305. [Google Scholar] [CrossRef]
- Blakemore, S.-J. Adolescence and mental health. Lancet 2019, 393, 2030–2031. [Google Scholar] [CrossRef]
- Uccella, S.; Cordani, R.; Salfi, F.; Gorgoni, M.; Scarpelli, S.; Gemignani, A.; Geoffroy, P.A.; De Gennaro, L.; Palagini, L.; Ferrara, M.; et al. Sleep Deprivation and Insomnia in Adolescence: Implications for Mental Health. Brain Sci. 2023, 13, 569. [Google Scholar] [CrossRef]
- Kovacs, M.; Feinberg, T.L.; Crouse-Novak, M.A.; Paulauskas, S.L.; Finkelstein, R. Depressive Disorders in Childhood: I. A Longitudinal Prospective Study of Characteristics and Recovery. Arch. Gen. Psychiatry 1984, 41, 229–237. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Clarke, G.N.; Seeley, J.R.; Rohde, P. Major depression in community adolescents: Age at onset, episode duration, and time to recurrence. J. Am. Acad. Child Adolesc. Psychiatry 1994, 33, 809–818. [Google Scholar] [CrossRef]
- McCauley, E.; Myers, K.; Mitchell, J.; Calderon, R.; Schloredt, K.; Treder, R. Depression in young people: Initial presentation and clinical course. J. Am. Acad. Child Adolesc. Psychiatry 1993, 32, 714–722. [Google Scholar] [CrossRef]
- Douglas, J.; Scott, J. A systematic review of gender-specific rates of unipolar and bipolar disorders in community studies of pre-pubertal children. Bipolar Disord. 2014, 16, 5–15. [Google Scholar] [CrossRef]
- Hyde, J.S.; Mezulis, A.H.; Abramson, L.Y. The ABCs of depression: Integrating affective, biological, and cognitive models to explain the emergence of the gender difference in de-pression. Psychol. Rev. 2008, 115, 291–313. [Google Scholar] [CrossRef] [PubMed]
- Magklara, K.; Bellos, S.; Niakas, D.; Stylianidis, S.; Kolaitis, G.; Mavreas, V.; Skapinakis, P. Depression in late adolescence: A cross-sectional study in senior high schools in Greece. BMC Psychiatry 2015, 15, 199. [Google Scholar] [CrossRef] [PubMed]
- Nolen-Hoeksema, S.; Girgus, J.S. The emergence of gender differences in depression during adolescence. Psychol. Bull. 1994, 115, 424–443. [Google Scholar] [CrossRef] [PubMed]
- Riecher-Rössler, A. Sex and gender differences in mental disorders. Lancet Psychiatry 2017, 4, 8–9. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Zhou, F.; Hou, W.; Heybati, K.; Lohit, S.; Abbas, U.; Silver, Z.; Wong, C.Y.; Chang, O.; Huang, E.; et al. Prevalence of mental health symptoms in children and adolescents during the COVID-19 pandemic: A meta-analysis. Ann. N. Y. Acad. Sci. 2023, 1520, 53–73. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Riemann, D.; Berger, M.; Voderholzer, U. Sleep and depression—Results from psychobiological studies: An overview. Biol. Psychol. 2001, 57, 67–103. [Google Scholar] [CrossRef]
- Urrila, A.S.; Karlsson, L.; Kiviruusu, O.; Pelkonen, M.; Strandholm, T.; Marttunen, M. Sleep complaints among adolescent outpatients with major depressive disorder. Sleep Med. 2012, 13, 816–823. [Google Scholar] [CrossRef]
- Nutt, D.; Wilson, S.; Paterson, L. Sleep disorders as core symptoms of depression. Dialogues Clin. Neurosci. 2008, 10, 329–336. [Google Scholar] [CrossRef]
- Urrila, A.S.; Paunio, T.; Palomäki, E.; Marttunen, M. Sleep in adolescent depression: Physiological perspectives. Acta Physiol. 2015, 213, 758–777. [Google Scholar] [CrossRef]
- Carskadon, M.A. Sleep in adolescents: The perfect storm. Pediatr. Clin. N. Am. 2011, 58, 637–647. [Google Scholar] [CrossRef] [PubMed]
- Crowley, S.J.; Acebo, C.; Carskadon, M.A. Sleep, circadian rhythms, and delayed phase in adolescence. Sleep Med. 2007, 8, 602–612. [Google Scholar] [CrossRef] [PubMed]
- Hagenauer, M.H.; Perryman, J.I.; Lee, T.M.; Carskadon, M.A. Adolescent changes in the homeostatic and circadian regulation of sleep. Dev. Neurosci. 2009, 31, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Hagenauer, M.H.; Lee, T.M. The neuroendocrine control of the circadian system: Adolescent chronotype. Front. Neuroendocrinol. 2012, 33, 211–229. [Google Scholar] [CrossRef] [PubMed]
- Illingworth, G. The challenges of adolescent sleep. Interface Focus 2020, 10, 20190080. [Google Scholar] [CrossRef] [PubMed]
- Kalak, N.; Lemola, S.; Brand, S.; Holsboer-Trachsler, E.; Grob, A. Sleep duration and subjective psychological well-being in adolescence: A longitudinal study in Switzerland and Norway. Neuropsychiatr. Dis. Treat. 2014, 10, 1199–1207. [Google Scholar]
- Kaplan, K.A.; Harvey, A.G. Hypersomnia across mood disorders: A review and synthesis. Sleep Med. Rev. 2009, 13, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Steiger, A.; Kimura, M. Wake and sleep EEG provide biomarkers in depression. J. Psychiatr. Res. 2010, 44, 242–252. [Google Scholar] [CrossRef]
- Williamson, D.E.; Birmaher, B.; Brent, D.A.; Balach, L.; Dahl, R.E.; Ryan, N.D. Atypical Symptoms of Depression in a Sample of Depressed Child and Adolescent Outpatients. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 1253–1259. [Google Scholar] [CrossRef]
- Yorbik, O.; Birmaher, B.; Axelson, D.; Williamson, D.E.; Ryan, N.D. Clinical characteristics of depressive symptoms in children and adolescents with major depressive disorder. J. Clin. Psychiatry 2004, 65, 1654–1659, quiz 1760–1761. [Google Scholar] [CrossRef]
- Dauvilliers, Y.; Lopez, R.; Ohayon, M.; Bayard, S. Hypersomnia and depressive symptoms: Methodological and clinical aspects. BMC Med. 2013, 11, 78. [Google Scholar] [CrossRef] [PubMed]
- Campbell, I.G.; Zhang, Z.Y.; Grimm, K.J. Sleep restriction effects on sleep spindles in ado-lescents and relation of these effects to subsequent daytime sleepiness and cognition. Sleep 2023, 46, zsad071. [Google Scholar] [CrossRef] [PubMed]
- Carskadon, M.A. Patterns of sleep and sleepiness in adolescents. Pediatrician 1990, 17, 5–12. [Google Scholar] [PubMed]
- Contreras, D.; Destexhe, A.; Sejnowski, T.J.; Steriade, M. Control of Spatiotemporal Coherence of a Thalamic Oscillation by Corticothalamic Feedback. Science 1996, 274, 771–774. [Google Scholar] [CrossRef] [PubMed]
- Rusterholz, T.; Hamann, C.; Markovic, A.; Schmidt, S.J.; Achermann, P.; Tarokh, L. Nature and Nurture: Brain Region-Specific Inheritance of Sleep Neurophysiology in Adolescence. J. Neurosci. 2018, 38, 9275–9285. [Google Scholar] [CrossRef] [PubMed]
- McClain, I.J.; Lustenberger, C.; Achermann, P.; Lassonde, J.M.; Kurth, S.; LeBourgeois, M.K. Developmental Changes in Sleep Spindle Characteristics and Sigma Power across Early Childhood. Neural Plast. 2016, 2016, 3670951. [Google Scholar] [CrossRef] [PubMed]
- Rechtschaffen, A.; Kales, A. A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects; United States Government Printing Office: Washington, DC, USA, 1968.
- Moser, D.; Anderer, P.; Gruber, G.; Parapatics, S.; Loretz, E.; Boeck, M.; Kloesch, G.; Heller, E.; Schmidt, A.; Danker-Hopfe, H.; et al. Sleep classification according to AASM and Rechtschaffen & Kales: Effects on sleep scoring parameters. Sleep 2009, 32, 139–149. [Google Scholar]
- Mayers, A.G.; Baldwin, D.S. The relationship between sleep disturbance and depression. Int. J. Psychiatry Clin. Pract. 2006, 10, 2–16. [Google Scholar] [CrossRef]
- Pillai, V.; Kalmbach, D.A.; Ciesla, J.A. A Meta-Analysis of Electroencephalographic Sleep in Depression: Evidence for Genetic Biomarkers. Biol. Psychiatry 2011, 70, 912–919. [Google Scholar] [CrossRef]
- Appelboom-Fondu, J.; Kerkhofs, M.; Mendlewicz, J. Depression in adolescents and young adults—Polysomnographic and neuroendocrine aspects. J. Affect. Disord. 1988, 14, 35–40. [Google Scholar] [CrossRef]
- Goetz, R.R.; Puig-Antich, J.; Ryan, N.; Rabinovich, H.; Ambrosini, P.J.; Nelson, B.; Krawiec, V. Electroencephalographic sleep of adolescents with major depression and normal controls. Arch. Gen. Psychiatry 1987, 44, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Lovato, N.; Gradisar, M. A meta-analysis and model of the relationship between sleep and depression in adolescents: Recommendations for future research and clinical practice. Sleep Med. Rev. 2014, 18, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Rao, U.; Poland, R.E. Electroencephalographic Sleep and Hypothalamic–Pituitary–Adrenal Changes from Episode to Recovery in Depressed Adolescents. J. Child Adolesc. Psychopharmacol. 2008, 18, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Armitage, R.; Emslie, G.J.; Hoffmann, R.F.; Rintelmann, J.; Rush, A.J. Delta sleep EEG in depressed adolescent females and healthy controls. J. Affect. Disord. 2001, 63, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Goetz, R.R.; Wolk, S.I.; Coplan, J.D.; Ryan, N.D.; Weissman, M.M. Premorbid poly-somnographic signs in depressed adolescents: A reanalysis of EEG sleep after longitudinal follow-up in adulthood. Biol. Psychiatry 2001, 49, 930–942. [Google Scholar] [CrossRef] [PubMed]
- Dahl, R.E.; Puig-Antich, J.; Ryan, N.D.; Nelson, B.; Dachille, S.; Cunningham, S.L.; Trubnick, L.; Klepper, T.P. EEG sleep in adolescents with major depression: The role of suicidality and inpatient status. J. Affect. Disord. 1990, 19, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Emslie, G.J.; Rush, A.J.; Weinberg, W.A.; Rintelmann, J.W.; Roffwarg, H.P. Children with Major Depression Show Reduced Rapid Eye Movement Latencies. Arch. Gen. Psychiatry 1990, 47, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Kupfer, D.J. REM latency: A psychobiologic marker for primary depressive disease. Biol. Psychiatry 1976, 11, 159–174. [Google Scholar]
- Emslie, G.J.; Armitage, R.; Weinberg, W.A.; John Rush, A.; Mayes, T.L.; Hoffmann, R.F. Sleep polysomnography as a predictor of recurrence in children and adolescents with major depressive disorder. Int. J. Neuropsychopharmacol. 2001, 4, 159–168. [Google Scholar] [CrossRef]
- Frey, S.; Birchler-Pedross, A.; Hofstetter, M.; Brunner, P.; Götz, T.; Münch, M.; Blatter, K.; Knoblauch, V.; Wirz-Justice, A.; Cajochen, C. Young women with major depression live on higher homeostatic sleep pressure than healthy controls. Chronobiol. Int. 2012, 29, 278–294. [Google Scholar] [CrossRef]
- Tesler, N.; Gerstenberg, M.; Franscini, M.; Jenni, O.G.; Walitza, S.; Huber, R. Increased frontal sleep slow wave activity in adolescents with major depression. Neuroimage Clin. 2015, 10, 250–256. [Google Scholar] [CrossRef]
- Campbell, I.G.; Feinberg, I. Longitudinal trajectories of non-rapid eye movement delta and theta EEG as indicators of adolescent brain maturation. Proc. Natl. Acad. Sci. USA 2009, 106, 5177–5180. [Google Scholar] [CrossRef]
- Colrain, I.M.; Baker, F.C. Changes in sleep as a function of adolescent development. Neuropsychol. Rev. 2011, 21, 5–21. [Google Scholar] [CrossRef]
- Tarokh, L.; Van Reen, E.; LeBourgeois, M.; Seifer, R.; Carskadon, M.A. Sleep EEG provides evidence that cortical changes persist into late adolescence. Sleep 2011, 34, 1385–1393. [Google Scholar] [CrossRef]
- Tarokh, L.; Carskadon, M.A. Developmental changes in the human sleep EEG during early adolescence. Sleep 2010, 33, 801–809. [Google Scholar] [CrossRef]
- Feinberg, I.; Floyd, T.C. Systematic trends across the night in human sleep cycles. Psychophysiology 1979, 16, 283–291. [Google Scholar] [CrossRef]
- Augustinavicius, J.L.S.; Zanjani, A.; Zakzanis, K.K.; Shapiro, C.M. Polysomnographic features of early-onset depression: A meta-analysis. J. Affect. Disord. 2014, 158, 11–18. [Google Scholar] [CrossRef]
- Achermann, P.; Borbély, A.A. Simulation of human sleep: Ultradian dynamics of electroencephalographic slow-wave activity. J. Biol. Rhythms 1990, 5, 141–157. [Google Scholar] [CrossRef]
- Achermann, P.; Borbély, A.A. Dynamics of EEG slow wave activity during physiological sleep and after administration of benzodiazepine hypnotics. Hum. Neurobiol. 1987, 6, 203–210. [Google Scholar]
- Borbély, A.A.; Achermann, P. Sleep homeostasis and models of sleep regulation. J. Biol. Rhythms 1999, 14, 557–568. [Google Scholar]
- Borbély, A.A. A two process model of sleep regulation. Hum. Neurobiol. 1982, 1, 195–204. [Google Scholar]
- Dijk, D.-J. Regulation and Functional Correlates of Slow Wave Sleep. J. Clin. Sleep Med. 2009, 5, S6–S15. [Google Scholar] [CrossRef]
- Borbély, A.A.; Wirz-Justice, A. Sleep, sleep deprivation and depression. A hypothesis de-rived from a model of sleep regulation. Hum. Neurobiol. 1982, 1, 205–210. [Google Scholar]
- Reynolds, C.F.; Shaw, D.H.; Newton, T.F.; Coble, P.A.; Kupfer, D.J. EEG sleep in outpatients with generalized anxiety: A preliminary comparison with depressed outpatients. Psychiatry Res. 1983, 8, 81–89. [Google Scholar] [CrossRef]
- Reynolds, C.F.; Newton, T.F.; Shaw, D.H.; Coble, P.A.; Kupfer, D.J. Electroencephalographic sleep findings in depressed outpatients. Psychiatry Res. 1982, 6, 65–75. [Google Scholar] [CrossRef]
- Reynolds, C.F.; Kupfer, D.J.; Hoch, C.C.; Houck, P.R.; Stack, J.A.; Berman, S.R.; Campbell, P.I.; Zimmer, B. Sleep deprivation as a probe in the elderly. Arch. Gen. Psychiatry 1987, 44, 982–990. [Google Scholar] [CrossRef]
- Armitage, R.; Hoffmann, R.; Fitch, T.; Trivedi, M.; Rush, A.J. Temporal characteristics of delta activity during NREM sleep in depressed outpatients and healthy adults: Group and sex effects. Sleep 2000, 23, 607–617. [Google Scholar] [CrossRef]
- Armitage, R.; Hoffmann, R.; Trivedi, M.; Rush, A.J. Slow-wave activity in NREM sleep: Sex and age effects in depressed outpatients and healthy controls. Psychiatry Res. 2000, 95, 201–213. [Google Scholar] [CrossRef]
- Borbély, A.A.; Tobler, I.; Loepfe, M.; Kupfer, D.J.; Ulrich, R.F.; Grochocinski, V.; Doman, J.; Matthews, G. All-night spectral analysis of the sleep EEG in untreated depressives and normal controls. Psychiatry Res. 1984, 12, 27–33. [Google Scholar] [CrossRef]
- Kupfer, D.J.; Frank, E.; Ehlers, C.L. EEG sleep in young depressives: First and second night effects. Biol. Psychiatry 1989, 25, 87–97. [Google Scholar] [CrossRef]
- Armitage, R. Microarchitectural findings in sleep EEG in depression: Diagnostic implications. Biol. Psychiatry 1995, 37, 72–84. [Google Scholar] [CrossRef]
- Plante, D.T.; Goldstein, M.R.; Landsness, E.C.; Peterson, M.J.; Riedner, B.A.; Ferrarelli, F.; Wanger, T.; Guokas, J.J.; Tononi, G.; Benca, R.M. and sex-related differences in sleep spindles in major depressive disorder: A high-density EEG investigation. J. Affect. Disord. 2013, 146, 120–125. [Google Scholar] [CrossRef]
- Baker, F.C.; Turlington, S.R.; Colrain, I. Developmental changes in the sleep electroencephalogram of adolescent boys and girls. J. Sleep Res. 2012, 21, 59–67. [Google Scholar] [CrossRef]
- Feinberg, I.; Higgins, L.M.; Khaw, W.Y.; Campbell, I.G. The adolescent decline of NREM delta, an indicator of brain maturation, is linked to age and sex but not to pubertal stage. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2006, 291, R1724–R1729. [Google Scholar] [CrossRef]
- Lopez, J.; Hoffmann, R.; Emslie, G.; Armitage, R. Sex Differences in Slow-wave Electro-encephalographic Activity (SWA) in Adolescent Depression. Ment. Illn. 2012, 4, e4. [Google Scholar]
- Baker, F.C.; Willoughby, A.R.; de Zambotti, M.; Franzen, P.L.; Prouty, D.; Javitz, H.; Hasler, B.; Clark, D.B.; Colrain, I.M. Age-Related Differences in Sleep Architecture and Electroencephalogram in Adolescents in the National Consortium on Alcohol and Neurodevelopment in Adolescence Sample. Sleep 2016, 39, 1429–1439. [Google Scholar] [CrossRef]
- Park, S.-C.; Kim, J.-M.; Jun, T.-Y.; Lee, M.-S.; Kim, J.-B.; Yim, H.-W.; Park, Y.C. How many different symptom combinations fulfil the diagnostic criteria for major depressive disorder? Results from the CRESCEND study. Nord. J. Psychiatry 2017, 71, 217–222. [Google Scholar] [CrossRef]
- Borbély, A. The two-process model of sleep regulation: Beginnings and outlook. J. Sleep Res. 2022, 31, e13598. [Google Scholar] [CrossRef]
- Borbély, A.A.; Daan, S.; Wirz-Justice, A.; Deboer, T. The two-process model of sleep regulation: A reappraisal. J. Sleep Res. 2016, 25, 131–143. [Google Scholar] [CrossRef]
- Fernandez, L.M.J.; Lüthi, A. Sleep Spindles: Mechanisms and Functions. Physiol. Rev. 2020, 100, 805–868. [Google Scholar] [CrossRef]
- Ricci, A.; He, F.; Younes, M.; Calhoun, S.; Fang, J.; Houser, L.; Vgontzas, A.; Liao, D.; Bixler, E.; Fernandez-Mendoza, J. Sex Differences in the Maturational Trajectories of Sleep Spindles in the Transition from Childhood to Adolescence. Sleep 2021, 44, A62. [Google Scholar] [CrossRef]
- Steriade, M. Neuronal Substrates of Sleep and Epilepsy; Cambridge University Press: Cambridge, UK, 2003. [Google Scholar]
- Khazipov, R.; Sirota, A.; Leinekugel, X.; Holmes, G.L.; Ben-Ari, Y.; Buzsáki, G. Early motor activity drives spindle bursts in the developing somatosensory cortex. Nature 2004, 432, 758–761. [Google Scholar] [CrossRef]
- Fogel, S.M.; Smith, C.T. The function of the sleep spindle: A physiological index of intelli-gence and a mechanism for sleep-dependent memory consolidation. Neurosci. Biobehav. Rev. 2011, 35, 1154–1165. [Google Scholar] [CrossRef]
- De Maertelaer, V.; Hoffman, G.; Lemaire, M.; Mendlewicz, J. Sleep spindle activity changes in patients with affective disorders. Sleep 1987, 10, 443–451. [Google Scholar] [CrossRef]
- Hamann, C.; Rusterholz, T.; Studer, M.; Kaess, M.; Tarokh, L. Association between depres-sive symptoms and sleep neurophysiology in early adolescence. J. Child Psychol. Psychiatry 2019, 60, 1334–1342. [Google Scholar] [CrossRef]
- Sesso, G.; Bat-Pitault, F.; Guyon, A.; Plancoulaine, S.; Banfi, T.; Milioli, G.; Parrino, L.; Faraguna, U.; Franco, P. Electrophysiological and microstructural features of sleep in children at high risk for depression: A preliminary study. Sleep Med. 2017, 36, 95–103. [Google Scholar] [CrossRef]
- Mikoteit, T.; Brand, S.; Perren, S.; von Wyl, A.; von Klitzing, K.; Kurath, J.; Holsboer-Trachsler, E.; Hatzinger, M. Visually detected non-rapid eye movement stage 2 sleep spindle density at age five years predicted prosocial behavior positively and hyperactivity scores negatively at age nine years. Sleep Med. 2018, 48, 101–106. [Google Scholar] [CrossRef]
- Mikoteit, T.; Brand, S.; Perren, S.; von Wyl, A.; von Klitzing, K.; Kurath, J.; Holsboer-Trachsler, E.; Hatzinger, M. Visually detected NREM Stage 2 sleep spindles in kindergarten children are associated with current and future emotional and behavioural characteristics. J. Sleep Res. 2013, 22, 129–136. [Google Scholar] [CrossRef]
- Ferrarelli, F.; Huber, R.; Peterson, M.J.; Massimini, M.; Murphy, M.; Riedner, B.A.; Watson, A.; Bria, P.; Tononi, G. Reduced sleep spindle activity in schizophrenia patients. Am. J. Psychiatry 2007, 164, 483–492. [Google Scholar] [CrossRef]
- Reynolds, C.F.; Kupfer, D.J.; Taska, L.S.; Hoch, C.C.; Spiker, D.G.; Sewitch, D.E.; Zimmer, B.; Marin, R.S.; Nelson, J.P.; Martin, D. EEG sleep in elderly depressed, demented, and healthy subjects. Biol. Psychiatry 1985, 20, 431–442. [Google Scholar] [CrossRef]
- Huupponen, E.; Himanen, S.-L.; Värri, A.; Hasan, J.; Lehtokangas, M.; Saarinen, J. A study on gender and age differences in sleep spindles. Neuropsychobiology 2002, 45, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Markovic, A.; Kaess, M.; Tarokh, L. Gender differences in adolescent sleep neurophysiology: A high-density sleep EEG study. Sci. Rep. 2020, 10, 15935. [Google Scholar] [CrossRef] [PubMed]
- Zajkowska, Z.; Walsh, A.; Zonca, V.; Gullett, N.; Pedersen, G.A.; Kieling, C.; Swartz, J.R.; Karmacharya, R.; Fisher, H.L.; Kohrt, B.A.; et al. A systematic review of the association between biological markers and environmental stress risk factors for adolescent depression. J. Psychiatr. Res. 2021, 138, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Rao, U.; Hammen, C.L.; Poland, R.E. Risk Markers for Depression in Adolescents: Sleep and HPA Measures. Neuropsychopharmacology 2009, 34, 1936–1945. [Google Scholar] [CrossRef]
- Fava, M. Diagnosis and definition of treatment-resistant depression. Biol. Psychiatry 2003, 53, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Zwolińska, W.; Dmitrzak-Węglarz, M.; Słopień, A. Biomarkers in Child and Adolescent Depression. Child Psychiatry Hum. Dev. 2023, 54, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Dharmadhikari, A.S.; Tandle, A.L.; Jaiswal, S.V.; Sawant, V.A.; Vahia, V.N.; Jog, N. Frontal Theta Asymmetry as a Biomarker of Depression. East Asian Arch. Psychiatry 2018, 28, 17–22. [Google Scholar]
- McVoy, M.; Lytle, S.; Fulchiero, E.; Aebi, M.E.; Adeleye, O.; Sajatovic, M. A systematic review of quantitative EEG as a possible biomarker in child psychiatric disorders. Psychiatry Res. 2019, 279, 331–344. [Google Scholar] [CrossRef]
- Verrusio, W.; Ettorre, E.; Vicenzini, E.; Vanacore, N.; Cacciafesta, M.; Mecarelli, O. The Mozart Effect: A quantitative EEG study. Conscious Cogn. 2015, 35, 150–155. [Google Scholar] [CrossRef]
- Wichniak, A.; Wierzbicka, A.; Jernajczyk, W. Sleep as a biomarker for depression. Int. Rev. Psychiatry 2013, 25, 632–645. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.I.; Lipinski, J.F.; Frankenburg, F.R.; Grochocinski, V.J.; Kupfer, D.J. Electroencephalographic sleep in mania. Arch. Gen. Psychiatry 1988, 45, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Reich, L.; Weiss, B.L.; Coble, P.; McPartland, R.; Kupfer, D.J. Sleep disturbance in schizophrenia. A revisit. Arch. Gen. Psychiatry 1975, 32, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Zarcone, V.P.; Benson, K.L.; Berger, P.A. Abnormal rapid eye movement latencies in schizophrenia. Arch. Gen. Psychiatry 1987, 44, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Uhde, T.W.; Roy-Byrne, P.; Gillin, J.C.; Mendelson, W.B.; Boulenger, J.P.; Vittone, B.J.; Post, R.M. The sleep of patients with panic disorder: A preliminary report. Psychiatry Res. 1984, 12, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Insel, T.R.; Gillin, J.C.; Moore, A.; Mendelson, W.B.; Loewenstein, R.J.; Murphy, D.L. The sleep of patients with obsessive-compulsive disorder. Arch. Gen. Psychiatry 1982, 39, 1372–1377. [Google Scholar] [CrossRef]
- Katz, J.L.; Kuperberg, A.; Pollack, C.P.; Walsh, B.T.; Zumoff, B.; Weiner, H. Is there a relationship between eating disorder and affective disorder? New evidence from sleep recordings. Am. J. Psychiatry 1984, 141, 753–759. [Google Scholar]
- Armitage, R.; Hoffmann, R.F.; Emslie, G.J.; Weinberg, W.A.; Mayes, T.L.; Rush, A.J. Sleep microarchitecture as a predictor of recurrence in children and adolescents with depression. Int. J. Neuropsychopharmacol. 2002, 5, 217–228. [Google Scholar] [CrossRef]
- Markovic, A.; Kaess, M.; Tarokh, L. Heritability of REM sleep neurophysiology in adolescence. Transl. Psychiatry 2022, 12, 399. [Google Scholar] [CrossRef]
- Markovic, A.; Achermann, P.; Rusterholz, T.; Tarokh, L. Heritability of Sleep EEG Topography in Adolescence: Results from a Longitudinal Twin Study. Sci. Rep. 2018, 8, 7334. [Google Scholar] [CrossRef]
- Roberts, R.E.; Duong, H.T. Depression and insomnia among adolescents: A prospective perspective. J. Affect. Disord. 2013, 148, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Alvaro, P.K.; Roberts, R.M.; Harris, J.K.; Bruni, O. The direction of the relationship between symptoms of insomnia and psychiatric disorders in adolescents. J. Affect. Disord. 2017, 207, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Sivertsen, B.; Harvey, A.G.; Lundervold, A.J.; Hysing, M. Sleep problems and depression in adolescence: Results from a large population-based study of Norwegian adolescents aged 16–18 years. Eur. Child Adolesc. Psychiatry 2014, 23, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Roane, B.M.; Taylor, D.J. Adolescent insomnia as a risk factor for early adult depression and substance abuse. Sleep 2008, 31, 1351–1356. [Google Scholar]
- Joseph, V.A.; Kreski, N.T.; Keyes, K.M. Sleep deprivation and suicide risk among minoritized US adolescents. BMC Psychiatry 2023, 23, 638. [Google Scholar] [CrossRef]
- Haghish, E.F.; Nes, R.B.; Obaidi, M.; Qin, P.; Stänicke, L.I.; Bekkhus, M.; Laeng, B.; Czajkowski, N. Unveiling Adolescent Suicidality: Holistic Analysis of Protective and Risk Factors Using Multiple Machine Learning Algorithms. J. Youth Adolesc. 2023. [Google Scholar] [CrossRef]
- Nguyen, T.P.; Lerch, S.; Maggetti, A.; Reichl, C.; Tarokh, L.; Kaess, M. The relationship between sleep disturbance and self-harming behaviours in high-risk clinical adolescents. J. Psychiatr. Res. 2023, 158, 81–87. [Google Scholar] [CrossRef]
- Tarokh, L.; Saletin, J.M.; Carskadon, M.A. Sleep in adolescence: Physiology, cognition and mental health. Neurosci. Biobehav. Rev. 2016, 70, 182–188. [Google Scholar] [CrossRef]
- Crowley, S.J.; Wolfson, A.R.; Tarokh, L.; Carskadon, M.A. An update on adolescent sleep: New evidence informing the perfect storm model☆. J. Adolesc. 2018, 67, 55–65. [Google Scholar] [CrossRef]
- Perlis, M.L.; Giles, D.E.; Mendelson, W.B.; Bootzin, R.R.; Wyatt, J.K. Psychophysiological insomnia: The behavioural model and a neurocognitive perspective. J. Sleep Res. 1997, 6, 179–188. [Google Scholar] [CrossRef]
- Riemann, D.; Spiegelhalder, K.; Feige, B.; Voderholzer, U.; Berger, M.; Perlis, M.; Nissen, C. The hyperarousal model of insomnia: A review of the concept and its evidence. Sleep Med. Rev. 2010, 14, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, F.; Argente, D.; Lippi, F. A Simple Planning Problem for COVID-19 Lock-down, Testing, and Tracing. Am. Econ. Rev. Insights 2021, 3, 367–382. [Google Scholar] [CrossRef]
- Richter, S.A.; Ferraz-Rodrigues, C.; Schilling, L.B.; Camargo, N.F.; Nunes, M.L. Effects of the COVID-19 pandemic on sleep quality in children and adolescents: A systematic review and meta-analysis. J. Sleep Res. 2023, 32, e13720. [Google Scholar] [CrossRef] [PubMed]
- da Silva, B.B.L.; de Melo, M.C.F.; Studart-Pereira, L.M. Adolescents’ sleep quality during the COVID-19 pandemic. Sleep Sci. 2022, 15, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Gradisar, M.; Kahn, M.; Micic, G.; Short, M.; Reynolds, C.; Orchard, F.; Bauducco, S.; Bartel, K.; Richardson, C. Sleep’s role in the development and resolution of adolescent depression. Nat. Rev. Psychol. 2022, 1, 512–523. [Google Scholar] [CrossRef] [PubMed]
- Twenge, J.M.; Blake, A.B.; Haidt, J.; Campbell, W.K. Commentary: Screens, Teens, and Psychological Well-Being: Evidence from Three Time-Use-Diary Studies. Front. Psychol. 2020, 11, 181. [Google Scholar] [CrossRef] [PubMed]
- Twenge, J.M.; Martin, G.N.; Spitzberg, B.H. Trends in U.S. Adolescents’ media use, 1976–2016: The rise of digital media, the decline of TV, and the (near) demise of print. Psychol. Pop. Media Cult. 2019, 8, 329–345. [Google Scholar] [CrossRef]
- Twenge, J.M.; Martin, G.N.; Campbell, W.K. Decreases in psychological well-being among American adolescents after 2012 and links to screen time during the rise of smartphone technology. Emotion 2018, 18, 765–780. [Google Scholar] [CrossRef]
- Hale, L.; Kirschen, G.W.; LeBourgeois, M.K.; Gradisar, M.; Garrison, M.M.; Montgomery-Downs, H.; Kirschen, H.; McHale, S.M.; Chang, A.-M.; Buxton, O.M. Youth screen media habits and sleep: Sleep-friendly screen-behavior recommendations for clinicians, educators, and parents. Child Adolesc. Psychiatr. Clin. N. Am. 2018, 27, 229–245. [Google Scholar] [CrossRef]
- Kerr, S.; Kingsbury, M. Online digital media use and adolescent mental health. Health Rep. 2023, 34, 17–28. [Google Scholar]
- Lang, C.; Kalak, N.; Brand, S.; Holsboer-Trachsler, E.; Pühse, U.; Gerber, M. The relationship between physical activity and sleep from mid adolescence to early adulthood. A systematic review of methodological approaches and meta-analysis. Sleep Med. Rev. 2016, 28, 32–45. [Google Scholar] [CrossRef] [PubMed]
- Kalak, N.; Gerber, M.; Kirov, R.; Mikoteit, T.; Yordanova, J.; Pühse, U.; Holsboer-Trachsler, E.; Brand, S. Daily morning running for 3 weeks improved sleep and psychological functioning in healthy adolescents compared with controls. J. Adolesc. Health 2012, 51, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Castiglione-Fontanellaz, C.E.G.; Timmers, T.T.; Lerch, S.; Hamann, C.; Kaess, M.; Tarokh, L. Sleep and physical activity: Results from a long-term actigraphy study in adolescents. BMC Public Health 2022, 22, 1328. [Google Scholar] [CrossRef] [PubMed]
- De Leeuw, M.; Verhoeve, S.I.; van der Wee, N.J.A.; van Hemert, A.M.; Vreugdenhil, E.; Coomans, C.P. The role of the circadian system in the etiology of depression. Neurosci. Biobehav. Rev. 2023, 153, 105383. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, C.L.; Frank, E.; Kupfer, D.J. Social zeitgebers and biological rhythms. A unified approach to understanding the etiology of depression. Arch. Gen. Psychiatry 1988, 45, 948–952. [Google Scholar] [CrossRef] [PubMed]
- Czeisler, C.A.; Kronauer, R.E.; Mooney, J.J.; Anderson, J.L.; Allan, J.S. Biologic Rhythm Disorders, Depression, and Phototherapy: A New Hypothesis. Psychiatr. Clin. 1987, 10, 687–709. [Google Scholar]
- Claudio, A.; Andrea, F. Circadian neuromarkers of mood disorders. J. Affect. Disord. Rep. 2022, 10, 100384. [Google Scholar] [CrossRef]
- Ballard, R.; Parkhurst, J.; Julian, K.; Pasetes, L.N.; Fawcett, A.; Li, A.; Goel, N.; Sit, D.K. Light Therapy for Adolescent Depression: A Scoping Review. Curr. Psychiatry Rep. 2023, 25, 373–386. [Google Scholar] [CrossRef]
- Phillips, A.J.K.; Clerx, W.M.; O’Brien, C.S.; Sano, A.; Barger, L.K.; Picard, R.W.; Lockley, S.W.; Klerman, E.B.; Czeisler, C.A. Irregular sleep/wake patterns are associated with poorer academic performance and delayed circadian and sleep/wake timing. Sci. Rep. 2017, 7, 3216. [Google Scholar] [CrossRef]
- Castiglione-Fontanellaz, C.E.G.; Schaufler, S.; Wild, S.; Hamann, C.; Kaess, M.; Tarokh, L. Sleep regularity in healthy adolescents: Associations with sleep duration, sleep quality, and mental health. J. Sleep Res. 2023, 32, e13865. [Google Scholar] [CrossRef]
- Mathew, G.M.; Reichenberger, D.A.; Master, L.; Buxton, O.M.; Chang, A.-M.; Hale, L. Actigraphic Sleep Variability is Associated with Lower Positive Mood in Adolescents. J. Adolesc. Health 2023, 73, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.P.; Sidol, C.A.; Van Dyk, T.R.; Epstein, J.N.; Beebe, D.W. Intraindividual variability of sleep/wake patterns in relation to child and adolescent functioning: A systematic review. Sleep Med. Rev. 2017, 34, 94–121. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castiglione-Fontanellaz, C.E.G.; Tarokh, L. Sleep and Adolescent Depression. Clin. Transl. Neurosci. 2024, 8, 3. https://doi.org/10.3390/ctn8010003
Castiglione-Fontanellaz CEG, Tarokh L. Sleep and Adolescent Depression. Clinical and Translational Neuroscience. 2024; 8(1):3. https://doi.org/10.3390/ctn8010003
Chicago/Turabian StyleCastiglione-Fontanellaz, Chiara E. G., and Leila Tarokh. 2024. "Sleep and Adolescent Depression" Clinical and Translational Neuroscience 8, no. 1: 3. https://doi.org/10.3390/ctn8010003
APA StyleCastiglione-Fontanellaz, C. E. G., & Tarokh, L. (2024). Sleep and Adolescent Depression. Clinical and Translational Neuroscience, 8(1), 3. https://doi.org/10.3390/ctn8010003