1. Introduction
The aim of this paper is to describe a case of a young female patient with oral pain caused by the presence of bilateral mandibular tori. The tori are exostoses formed by a dense cortical and limited amount of bone marrow, covered with a thin and poorly vascularized mucosa. These common intraoral exostoses (prevalence 20–25%) are usually located on the palatal midline or on the lingual side of mandibular bone. In most cases this kind of exostoses don’t cause pain or other symptoms and they aren’t considered pathological. They can affect pronunciation and interfere with swallowing. The development of tori can be due to genetic, environmental and functional factors.
2. Case
A 34-years-old woman presented at the oral medicine department of the San Paolo Hospital in Milan. The patient reported long-lasting oral pain, exacerbated by mastication and swallowing and the previous presence of ulceration of the oral mucosa. The clinical oral examination showed a thin layer of oral mucosa covering bilateral double prominent mandibular tori, aching on palpation (Figure 1). The anterior ones measured 8 mm, the posterior one located on the left side measured 15 mm and the one on the right side measured 18 mm. Although tori removal is not always mandatory, according to the clinical features and the history of persistent pain, we decided to proceed with surgical removal.
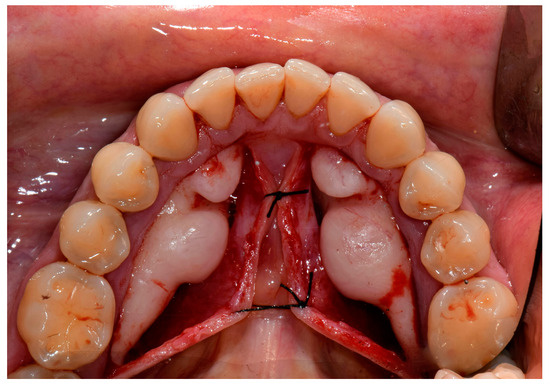
Figure 1.
Mandibular tori.
3. Treatment
The surgery was conducted under local anesthesia. After a paramarginal incision, a mucoperiostal lingual flap from 19 to 30 tooth, the removal of exostosis was performed by piezoelectric surgery and sutures were placed (Figure 2). The samples were sent to pathological anatomy department for histological analysis. Postoperative medication will consist of antibiotics, analgesics and anti-inflammatory medicine.
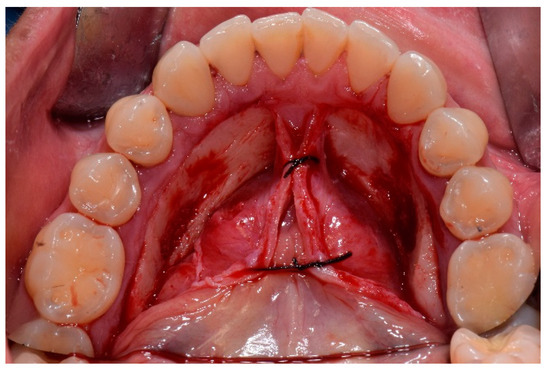
Figure 2.
Post-operatory picture, after tori removal.
After two weeks the patient arranged a new appointment. She referred an improvement of the symptoms. At the clinical examination soft tissue healthiness, completely healing of the surgical wound and no sign of inflammation were observed.
4. Conclusions
Although tori removal is not always necessary, there are situations in which it could be indicated: prosthetic rehabilitation or necessity of autologous bone graft. In the event that the patient reports long-lasting oral pain due to the exostosis, the removal is strongly recommended.
Conflicts of Interest
The authors declare no conflict of interest.
References
- García-García, A.S.; Martínez-González, J.M.; Gómez-Font, R.; Soto-Rivadeneira, A.; Oviedo-Roldán, L. Current status of the torus palatinus and torus mandibularis. Med. Oral Patol. Oral Cir. Bucal 2010, 15, e353–e360. [Google Scholar] [CrossRef] [PubMed]
- Seah, Y.H. Torus palatinus and torus mandibularis: A review of the literature. Aust. Dental J. 1995, 40, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Jainkittivong, A.; Langlais, R.P. Buccal and palatal exostoses: Pre-valence and concurrence with tori. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2000, 90, 48–53. [Google Scholar] [CrossRef] [PubMed]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).