
Neurological Diseases Define the Cytokine Profile in CFS during SARS-CoV-2 Infection in Highly Ill Patients

Abstract
1. Introduction
2. Relevant Section
3. Discussion
4. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harapan, B.N.; Yoo, H.J. Neurological symptoms, manifestations, and complications associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19). J. Neurol. 2021, 268, 3059–3071. [Google Scholar] [CrossRef]
- Méndez-García, L.A.; Escobedo, G.; Minguer-Uribe, A.G.; Viurcos-Sanabria, R.; Aguayo-Guerrero, J.A.; Carrillo-Ruiz, J.D.; Solleiro-Villavicencio, H. Role of the renin-angiotensin system in the development of COVID-19-associated neurological manifestations. Front. Cell. Neurosci. 2022, 16, 488. [Google Scholar] [CrossRef]
- Zubair, A.S.; McAlpine, L.S.; Gardin, T.; Farhadian, S.; Kuruvilla, D.E.; Spudich, S. Neuropathogenesis and Neurologic Manifestations of the Coronaviruses in the Age of Coronavirus Disease 2019: A Review. JAMA Neurol. 2020, 77, 1018–1027. [Google Scholar] [CrossRef]
- Ju, J.; Su, Y.; Zhou, Y.; Wei, H.; Xu, Q. The SARS-CoV-2 envelope protein disrupts barrier function in an in vitro human blood-brain barrier model. Front. Cell. Neurosci. 2022, 16, 432. [Google Scholar] [CrossRef]
- Taipa, R.; das Neves, S.P.; Sousa, A.L.; Fernandes, J.; Pinto, C.; Correia, A.P.; Santos, E.; Pinto, P.S.; Carneiro, P.; Costa, P.; et al. Proinflammatory and anti-inflammatory cytokines in the CSF of patients with Alzheimer’s disease and their correlation with cognitive decline. Neurobiol. Aging 2019, 76, 125–132. [Google Scholar] [CrossRef]
- Rizo-Téllez, S.A.; Méndez-García, L.A.; Flores-Rebollo, C.; Alba-Flores, F.; Alcántara-Suárez, R.; Manjarrez-Reyna, A.N.; Baltazar-López, N.; Hernández-Guzmán, V.A.; León-Pedroza, J.I.; Zapata-Arenas, R.; et al. The Neutrophil-to-Monocyte Ratio and Lymphocyte-to-Neutrophil Ratio at Admission Predict In-Hospital Mortality in Mexican Patients with Severe SARS-CoV-2 Infection (COVID-19). Microorganisms 2020, 8, 1560. [Google Scholar] [CrossRef]
- Venet, M.; Ribeiro, M.S.; Décembre, E.; Bellomo, A.; Joshi, G.; Nuovo, C.; Villard, M.; Cluet, D.; Perret, M.; Pescamona, R.; et al. Severe COVID-19 patients have impaired plasmacytoid dendritic cell-mediated control of SARS-CoV-2. Nat. Commun. 2023, 14, 694. [Google Scholar] [CrossRef]
- Zhang, S.; Asquith, B.; Szydlo, R.; Tregoning, J.S.; Pollock, K.M. Peripheral T cell lymphopenia in COVID-19: Potential mechanisms and impact. Immunother. Adv. 2021, 1, ltab015. [Google Scholar] [CrossRef]
- Deschler, S.; Kager, J.; Erber, J.; Fricke, L.; Koyumdzhieva, P.; Georgieva, A.; Lahmer, T.; Wiessner, J.R.; Voit, F.; Schneider, J.; et al. Mucosal-Associated Invariant T (MAIT) Cells Are Highly Activated and Functionally Impaired in COVID-19 Patients. Viruses 2021, 13, 241. [Google Scholar] [CrossRef]
- Xue, G.; Jiang, M.; Zhao, R.; Le, A.; Li, J. Elevated frequencies of CD14+HLA-DRlo/neg MDSCs in COVID-19 patients. Aging 2021, 13, 6236–6246. [Google Scholar] [CrossRef]
- Guartazaca-Guerrero, S.; Rodríguez-Morales, J.; Rizo-Téllez, S.A.; Solleiro-Villavicencio, H.; Hernández-Valencia, A.F.; Carrillo-Ruiz, J.D.; Escobedo, G.; Méndez-García, G.E.A.L.A. High Levels of IL-8 and MCP-1 in Cerebrospinal Fluid of COVID-19 Patients with Cerebrovascular Disease. Exp. Neurobiol. 2021, 30, 256–261. [Google Scholar] [CrossRef]
- Rodríguez-Morales, J.; Guartazaca-Guerrero, S.; Rizo-Téllez, S.A.; Viurcos-Sanabria, R.; Barrón, E.V.; Hernán-dez-Valencia, A.F.; Nava, P.; Escobedo, G.; Carrillo-Ruiz, J.D.; Méndez-García, L.A. Blood-brain Barrier Damage is Pivotal for SARS-CoV-2 Infection to the Central Nervous System. Exp. Neurobiol. 2022, 31, 270–276. [Google Scholar] [CrossRef]
- Kuzior, H.; Fiebich, B.L.; Yousif, N.M.; Saliba, S.W.; Ziegler, C.; Nickel, K.; Maier, S.J.; Süß, P.; Runge, K.; Matysik, M.; et al. Increased IL-8 concentrations in the cerebrospinal fluid of patients with unipolar depression. Compr. Psychiatry 2020, 102, 152196. [Google Scholar] [CrossRef]
- Martínez, H.; Escamilla-Ocañas, C.; Camara-Lemarroy, C.; González-Garza, M.; Moreno-Cuevas, J.; Sarreón, M.G. Increased cerebrospinal fluid levels of cytokines monocyte chemoattractant protein-1 (MCP-1) and macrophage inflammatory protein-1β (MIP-1β) in patients with amyotrophic lateral sclerosis. Neurologia 2020, 35, 165–169. [Google Scholar] [CrossRef]
- Guasp, M.; Muñoz-Sánchez, G.; Martínez-Hernández, E.; Santana, D.; Carbayo, Á.; Naranjo, L.; Bolós, U.; Framil, M.; Saiz, A.; Balasa, M.; et al. CSF Biomarkers in COVID-19 Associated Encephalopathy and Encephalitis Predict Long-Term Outcome. Front. Immunol. 2022, 13, 1600. [Google Scholar] [CrossRef]
- Montazersaheb, S.; Khatibi, S.M.H.; Hejazi, M.S.; Tarhriz, V.; Farjami, A.; Sorbeni, F.G.; Farahzadi, R.; Ghasemnejad, T. COVID-19 infection: An overview on cytokine storm and related interventions. Virol. J. 2022, 19, 92. [Google Scholar] [CrossRef]
- Dekay, J.T.; Emery, I.F.; Rud, J.; Eldridge, A.; Lord, C.; Gagnon, D.J.; May, T.L.; Herrera, V.L.M.; Ruiz-Opazo, N.; Riker, R.R.; et al. DEspRhigh neutrophils are associated with critical illness in COVID-19. Sci. Rep. 2021, 11, 22463. [Google Scholar] [CrossRef]
- De Stricker Borch, J.; Haslund-Vinding, J.; Vilhardt, F.; Maier, A.D.; Mathiesen, T. Meningioma–Brain Crosstalk: A Scoping Review. Cancers 2021, 13, 4267. [Google Scholar] [CrossRef]
- Albulescu, R.; Codrici, E.; Popescu, I.D.; Mihai, S.; Necula, L.G.; Petrescu, D.; Teodoru, M.; Tanase, C.P. Cytokine patterns in brain tumour progression. Mediat. Inflamm. 2013, 2013, 979748. [Google Scholar] [CrossRef]
- Ziai, W.C.; Parry-Jones, A.R.; Thompson, C.B.; Sansing, L.H.; Mullen, M.T.; Murthy, S.B.; Mould, A.; Nekoovaght-Tak, S.; Hanley, D.F. Early inflammatory cytokine expression in cerebrospinal fluid of patients with spontaneous intraventricular hemorrhage. Biomolecules 2021, 11, 1123. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Lukiw, W.J. SARS-CoV-2 Neuroinvasion, Inflammatory Neurodegeneration and Alzheimer’s Disease. Front. Cell. Neurosci. 2022, 16, 322. [Google Scholar] [CrossRef]
- Romagnolo, A.; Balestrino, R.; Imbalzano, G.; Ciccone, G.; Riccardini, F.; Artusi, C.A.; Bozzali, M.; Ferrero, B.; Montalenti, E.; Montanaro, E.; et al. Neurological comorbidity and severity of COVID-19. J. Neurol. 2020, 268, 762–769. [Google Scholar] [CrossRef]
- Jarvis, J.N.; Meintjes, G.; Bicanic, T.; Buffa, V.; Hogan, L.; Mo, S.; Tomlinson, G.; Kropf, P.; Noursadeghi, M.; Harrison, T.S. Cerebrospinal Fluid Cytokine Profiles Predict Risk of Early Mortality and Immune Reconstitution Inflammatory Syndrome in HIV-Associated Cryptococcal Meningitis. PLoS Pathog. 2015, 11, e1004754. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Gender | Age (Years) | Pre-Existing Neurological Disease | Respiratory/Neurological Symptoms Due to COVID-19 | Neurological Symptoms at Arrival to the Hospital | Presence of SARS-CoV-2 Nasopharyngeal/CSF | Deregulated Biochemical Parameters | Immunological Parameters | Cytokine Profile in CSF | ||
|---|---|---|---|---|---|---|---|---|---|---|
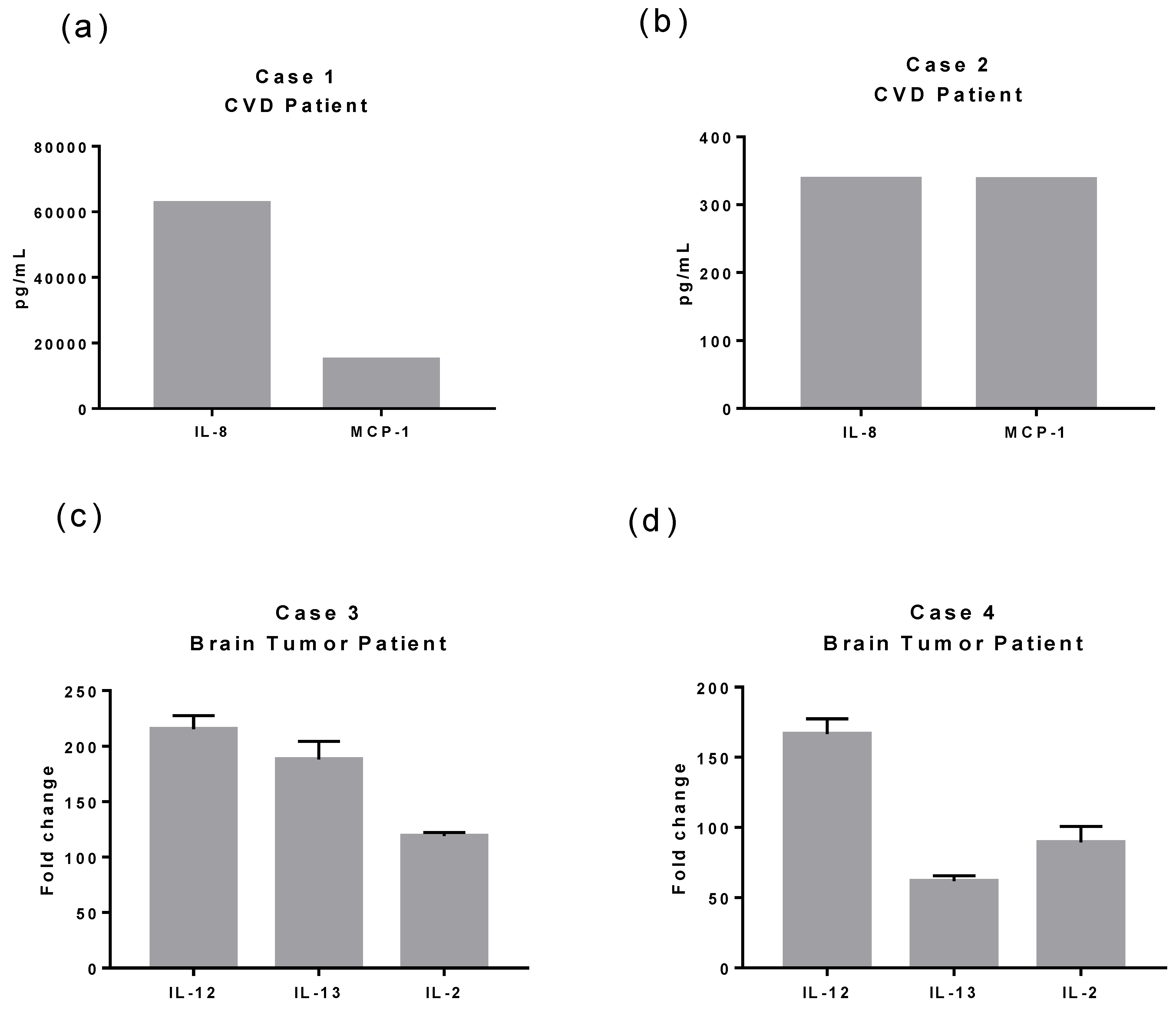
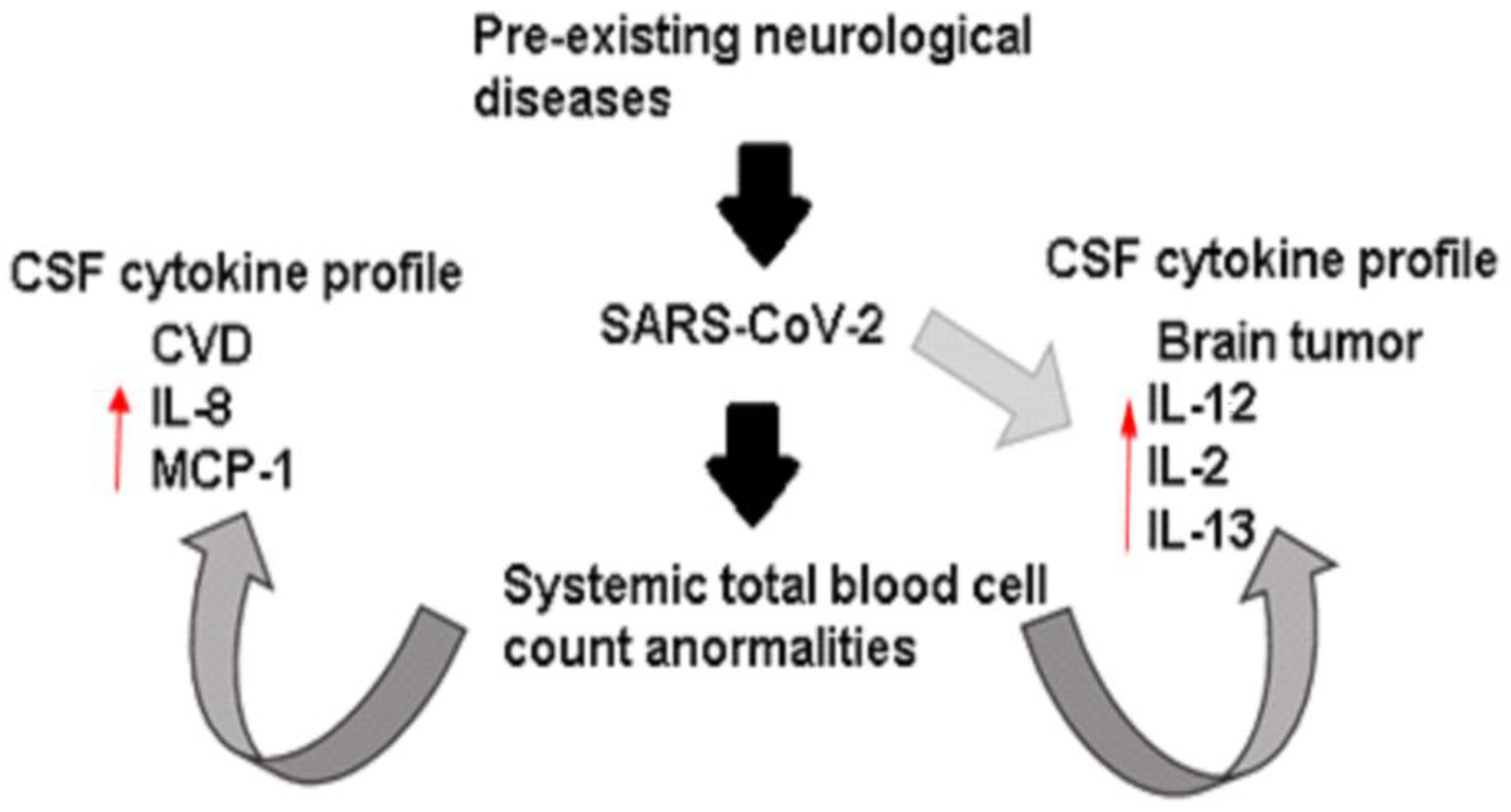
| Case 1 | Female | 54 | CVD (acute intra-axial hemorrhage) | Without symptoms | -Moderate headache -Balance impairment -Weakness -Loss of consciousness | Positive/Negative | Dimer-D (14,760 Ug/L) Glucose (161 mg/dL) Total cholesterol (236 mg/dL) | Leukocytosis (12.10 × 103/mm3) Lymphopenia (0.70 × 103/ mm3) Neutrophilia (11.30 × 103/ mm3) Monocytopenia (0.1 × 103/ mm3) |  | IL-8 MCP-1 IFN-α |
| Case 2 | Male | 45 | CVD (diffuse subarachnoid hemorrhage) | Without symptoms | -Seizure -Psychomotor agitation -Disorientation | Positive/Negative | Dimer-D (4304 Ug/L) Fibrinogen (562 mg/dL) | Leukocytosis (15.70 × 103/ mm3) Lymphopenia (0.90 × 103/ mm3) Neutrophilia (14.20 × 103/ mm3) |  | IL-8 MCP-1 IFN-α |
| Case 3 | Female | 43 | Brain tumor (petroclival meningioma) | Pneumonia | -Severe headache -Drowsiness | Positive/Positive | Triglycerides (372 mg/dL) Glucose (110 mg/dL) ALT (70 U/L) Q-albumin (7.3 × 10−3 g/dL) | Leukocytosis (12.40 × 103/ mm3) Neutrophilia (9.10 × 103/ mm3) Monocytopenia (0.2 × 103/ mm3) |  | IL-12 IL-2 IL-13 |
| Case 4 | Male | 43 | Brain tumor (in the fourth ventricle) | Anosmia Peripheral oxygen saturation of 89% Neurological impairment Pneumonia | -Intense headache -Syncope -Gait abnormalities -Decreased alertness | Positive/Negative | ALT (79 U/L) | Leukocytosis (12.40 × 103/ mm3) Neutrophilia (14.20 × 103/ mm3) Lymphopenia (0.90 × 103/ mm3) Monocytopenia (0.1 × 103/ mm3) |  | IL-12 IL-2 IL-13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Méndez-García, L.A.; Solleiro-Villavicencio, H.; Guartazaca-Guerrero, S.; Rodríguez-Morales, J.; Carrillo-Ruiz, J.D. Neurological Diseases Define the Cytokine Profile in CFS during SARS-CoV-2 Infection in Highly Ill Patients. Trop. Med. Infect. Dis. 2023, 8, 290. https://doi.org/10.3390/tropicalmed8060290
Méndez-García LA, Solleiro-Villavicencio H, Guartazaca-Guerrero S, Rodríguez-Morales J, Carrillo-Ruiz JD. Neurological Diseases Define the Cytokine Profile in CFS during SARS-CoV-2 Infection in Highly Ill Patients. Tropical Medicine and Infectious Disease. 2023; 8(6):290. https://doi.org/10.3390/tropicalmed8060290
Chicago/Turabian StyleMéndez-García, Lucía Angélica, Helena Solleiro-Villavicencio, Sebastián Guartazaca-Guerrero, Jahir Rodríguez-Morales, and José Damián Carrillo-Ruiz. 2023. "Neurological Diseases Define the Cytokine Profile in CFS during SARS-CoV-2 Infection in Highly Ill Patients" Tropical Medicine and Infectious Disease 8, no. 6: 290. https://doi.org/10.3390/tropicalmed8060290
APA StyleMéndez-García, L. A., Solleiro-Villavicencio, H., Guartazaca-Guerrero, S., Rodríguez-Morales, J., & Carrillo-Ruiz, J. D. (2023). Neurological Diseases Define the Cytokine Profile in CFS during SARS-CoV-2 Infection in Highly Ill Patients. Tropical Medicine and Infectious Disease, 8(6), 290. https://doi.org/10.3390/tropicalmed8060290