A Narrative Review of Suicide: Aiming at a More Encompassing Understanding

{kind=link}
Abstract
:1. Introduction
The Phenomenology of Suicide
2. The Different Philosophical Perspectives—Patient, Family, and Healthcare Professionals
2.1. The Patient
2.2. The Healthcare Professional
2.3. The Family
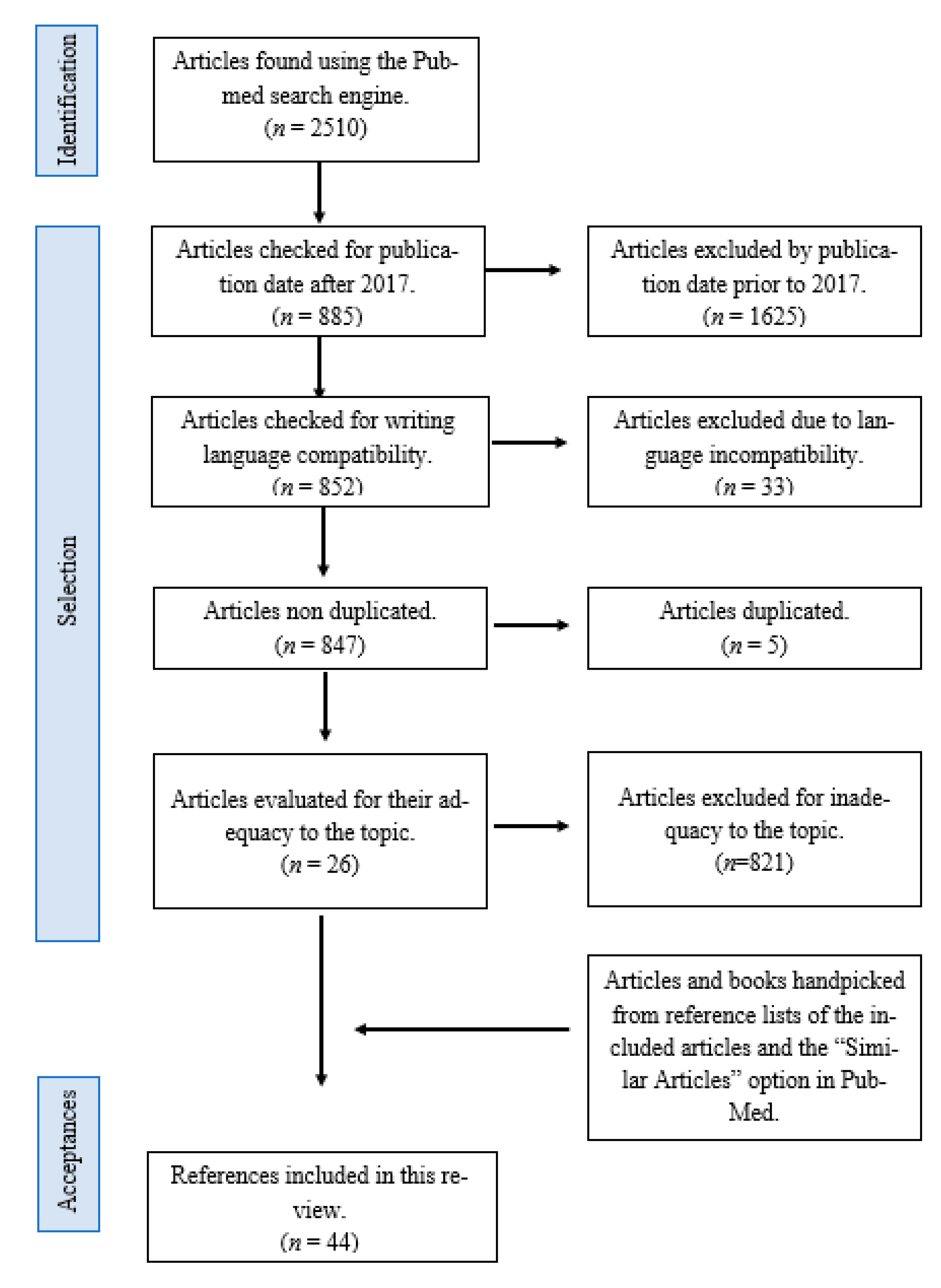
3. Materials and Methods
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pompili, M. Phenomenology of Suicide. Unlocking the Suicidal Mind, 1st ed.; Springer International Publishing: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Durkheim, E. Suicide, a Study in Sociology, 1951 ed.; Spaulding, J.A.; Simpson, G., Translators; Routledge: Abingdon, UK, 1897; ISBN 0710033117. [Google Scholar]
- Erlich, M.D.; Rolin, S.A.; Dixon, L.B.; Adler, D.A.; Oslin, D.W.; Levine, B.; Berlant, J.L.; Goldman, B.; Koh, S.; First, M.B.; et al. Why we need to enhance suicide postvention. Evaluating a survey of psychiatrists’ behaviors after the suicide of a patient. J. Nerv. Ment. Dis. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, K.; Murphy, G.; Jackson, D. Events prior to completed suicide: Perspectives of family survivors. Issues Ment. Health Nurs. 2013, 34, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Baumeister, R.F. Suicide as escape from self. Psychol. Rev. 1990, 90–113. [Google Scholar] [CrossRef] [PubMed]
- Berlim, M.T.; Mattevi, B.S.; Pavanello, D.P.; Caldieraro, M.A.; Fleck, M.P.A.; Wingate, L.R.; Joiner, T.E. Psychache and suicidality in adult mood disordered outpatients in brazil. Suicide Life-Threat. Behav. 2003, 33. [Google Scholar] [CrossRef]
- Schneidman, E. Suicide as psychache: A clinical approach to self-destructive behavior. J. Nerv. Ment. Dis. 1993, 181, 145–147. [Google Scholar] [CrossRef]
- Schneidman, E. The psychological pain assessment scale. Suicide Life-Threat. Behav. 1999, 29, 287–294. [Google Scholar] [PubMed]
- Schlimme, J.E. Sense of self-determination and the suicidal experience. A phenomenological approach. Med. Health Care Philos. 2013, 16, 211–223. [Google Scholar] [CrossRef] [Green Version]
- Naherniak, B.; Bhaskaran, J.; Sareen, J.; Wang, Y.; Bolton, J.M. Ambivalence about Living and the Risk for Future Suicide Attempts: A Longitudinal Analysis. Prim. Care Companion CNS Disord. 2019, 21, 18m02361. [Google Scholar] [CrossRef]
- Pompili, M. Exploring the phenomenology of suicide. Suicide Life Threat Behav. 2010, 40, 234–244. [Google Scholar] [CrossRef]
- Benson, O.; Gibson, S.; Brand, S.L. The experience of agency in feeling of being suicidal. J. Conscious. Stud. 2013, 20, 56–79. [Google Scholar]
- Cannon, K.E.; Hudzik, T.J. Suicide: Phenomenology and Neurobiology, 1st ed.; Springer International Publishing: New York, NY, USA, 2014; Volume 1. [Google Scholar] [CrossRef]
- Orbach, I.; Mikulincer, M.; Gilboa-Schechtman, E.; Sirota, P. Mental pain and its relationship to suicidality and life meaning. Suicide Life-Threat. Behav. 2003, 33. [Google Scholar] [CrossRef] [PubMed]
- Nugent, A.C.; Ballard, E.D.; Park, L.T.; Zarate, C.A. Research on the pathophysiology, treatment, and prevention of suicide: Practical and ethical issues. BMC Psychiatry 2019, 19, 332. [Google Scholar] [CrossRef] [Green Version]
- Pompili, M. The increase of suicide rates: The need for a paradigm shift. Lancet 2018, 474–475. [Google Scholar] [CrossRef] [Green Version]
- Al-Mateen, C.S.; Jones, K.; Linker, J.; O’Keefe, D.; Cimolai, V. Clinician response to a child who completes suicide. Child Adolesc. Psychiatric. Clin. N. Am. 2018, 27, 621–635. [Google Scholar] [CrossRef]
- Feigelman, W.; Cerel, J. Feelings of Blameworthiness and Their Associations With the Grieving Process in Suicide Mourning. Front Psychol. 2020, 11, 610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, I.T.; Iglewicz, A.; Glorioso, D.; Lanouette, N.; Seay, K.; Manjusha, I.; Zisook, S. Suicide bereavement and complicated grief. Dialogues Clin. Neurosci. 2012, 14, 177–186. [Google Scholar] [CrossRef]
- Andriessen, K.; Krysinska, K.; Rickwood, D.; Pirkis, J. “It Changes Your Orbit”: The Impact of Suicide and Traumatic Death on Adolescents as Experienced by Adolescents and Parents. Int. J. Environ. Res. Public Health 2020, 17, 9356. [Google Scholar] [CrossRef]
- Dutra, K.; Preis, L.; Caetano, J.; Santos, J.; Lessa, G. Experiencing suicide in the family: From mourning to the quest for overcoming. Rev. Bras. Enferm. 2018, 71 (Suppl. 5), 2146–2153. [Google Scholar] [CrossRef] [PubMed]
- Eisma, M.; Riele, B.; Overgaauw, M.; Doering, B. Does prolonged grief or suicide bereavement cause public stigma? A vignette-based experiment. Psychiatry Res. 2019, 272, 784–789. [Google Scholar] [CrossRef]
- Scocco, P.; Idotta, C.; Totaro, S.; Preti, A. Addressing psychological distress in people bereaved through suicide: From care to cure. Psychiatry Res. 2021, 300, 113869. [Google Scholar] [CrossRef]
- Pitman, A.; Osborn, D.; King, M.; Erlangsen, A. Effects of suicide bereavement on mental health and suicide risk. Lancet Psychiatry 2014, 1, 86–94. [Google Scholar] [CrossRef]
- Levi-Belz, Y.; Lev-Ari, L. Is There Anybody Out There? Attachment Style and Interpersonal Facilitators as Protective Factors Against Complicated Grief Among Suicide-Loss Survivors. J. Nerv. Ment. Dis. 2019, 207, 131–136. [Google Scholar] [CrossRef]
- Stone, S. Supporting Families and Providers When Suicide Occurs. Am. J. Hosp. Palliat. Care 2019, 36, 264–265. [Google Scholar] [CrossRef] [PubMed]
- Orford, N. Grief after Suicide. JAMA 2020, 323, 1720–1721. [Google Scholar] [CrossRef] [PubMed]
- Frumkin, M.; Robinaugh, D.; LeBlanc, N.; Ahmad, Z.; Bui, E.; Nock, M.; Simon, N.; McNally, R. The pain of grief: Exploring the concept of psychological pain and its relation to complicated grief, depression, and risk for suicide in bereaved adults. J. Clin. Psychol. 2021, 77, 254–267. [Google Scholar] [CrossRef]
- Shields, C.; Russo, K.; Kavanagh, M. Angels of Courage: The Experiences of Mothers Who Have Been Bereaved by Suicide. Omega 2019, 80, 175–201. [Google Scholar] [CrossRef] [PubMed]
- Hagstrom, A.S. Research-Based Theater and “Stigmatized Trauma”: The Case of Suicide Bereavement. Front. Psychol. 2020, 11, 1129. [Google Scholar] [CrossRef]
- Creighton, G.; Oliffe, J.L.; Bottorff, J.; Johnson, J. “I should have…”: A photovoice study with women who have lost a man to suicide. Am. J. Men’s Health 2018, 12, 1262–1274. [Google Scholar] [CrossRef] [PubMed]
- Ross, V.; Kõlves, K.; Leo, D. Exploring the Support Needs of People Bereaved by Suicide: A Qualitative Study. Omega 2021, 82, 632–645. [Google Scholar] [CrossRef]
- Hagstrom, A.S. “Why did he choose to die?”: A meaning-searching approach to parental suicide bereavement in youth. Death Stud. 2019, 43, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Frey, L.; Fulginiti, A. Talking about suicide may not be enough: Family reaction as a mediator between disclosure and interpersonal needs. J. Ment. Health 2017, 26, 366–372. [Google Scholar] [CrossRef]
- Mento, C.; Silvestri, M.; Muscatello, M.; Rizzo, A.; Celebre, L.; Bruno, A.; Zoccali, A. Psychological pain and risk of suicide in adolescence. Int. J. Adolesc. Med. Health 2020. [Google Scholar] [CrossRef]
- Hamdan, S.; Berkman, N.; Lavi, N.; Levy, S.; Brent, D. The Effect of Sudden Death Bereavement on the Risk for Suicide. Crisis 2020, 41, 214–224. [Google Scholar] [CrossRef]
- Levi-Belz, Y.; Aisenberg, D. Interpersonal predictors of suicide ideation and complicated-grief trajectories among suicide bereaved individuals: A four-year longitudinal study. J. Affect. Disord. 2021, 282, 1030–1035. [Google Scholar] [CrossRef]
- Naguy, A.; Elbadry, H.; Salem, H. Suicide: A Précis! J. Family Med. Prim. Care 2020, 9, 4009–4015. [Google Scholar] [CrossRef]
- Linde, K.; Treml, J.; Steinig, J.; Nagl, M.; Kersting, A. Grief interventions for people bereaved by suicide: A systematic review. PLoS ONE 2017, 12, e0179496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kucukalic, S.; Kucukalic, A. Stigma and Suicide. Psychiatr. Danub. 2017, 29 (Suppl. 5), 895–899. [Google Scholar] [PubMed]
- Cipolletta, S.; Entilli, L.; Bettio, F.; Leo, D. Live-Chat Support for People Bereaved by Suicide. Crisis 2021. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Hong, S.; Hong, H. The Impact of Referral to Mental Health Services on Suicide Death Risk in Adolescent Suicide Survivors. Soa Chongsonyon Chongsin Uihak 2020, 31, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Ivbijaro, G.; Kolkiewicz, L.; Goldberg, D.; Riba, M.B.; N’jie, I.N.; Geller, J.; Kallivayalil, R.; Javed, A.; Švab, I.; Summergrad, P.; et al. Preventing suicide, promoting resilience: Is this achievable from a global perspective? Asia Pac. Psychiatry 2019, 11, e12371. [Google Scholar] [CrossRef]
- Wainwright, V.; Cordingley, L.; Chew-Graham, C.; Kapur, N.; Shaw, J.; Smith, S.; McGale, B.; McDonnell, S. Experiences of support from primary care and perceived needs of parents bereaved by suicide: A qualitative study. Br. J. Gen. Pract. 2020, 70, e102–e110. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madeira, L.; Miranda, A.T. A Narrative Review of Suicide: Aiming at a More Encompassing Understanding. Philosophies 2021, 6, 74. https://doi.org/10.3390/philosophies6030074
Madeira L, Miranda AT. A Narrative Review of Suicide: Aiming at a More Encompassing Understanding. Philosophies. 2021; 6(3):74. https://doi.org/10.3390/philosophies6030074
Chicago/Turabian StyleMadeira, Luís, and Ana Teresa Miranda. 2021. "A Narrative Review of Suicide: Aiming at a More Encompassing Understanding" Philosophies 6, no. 3: 74. https://doi.org/10.3390/philosophies6030074
APA StyleMadeira, L., & Miranda, A. T. (2021). A Narrative Review of Suicide: Aiming at a More Encompassing Understanding. Philosophies, 6(3), 74. https://doi.org/10.3390/philosophies6030074