
Multimodal Machine Learning for Predicting Post-Surgery Quality of Life in Colorectal Cancer Patients

 , , , and
, , , and
Abstract
1. Introduction
2. Motivation and Quality of Life Indicators in Colorectal Cancer
- Imitations of Current QoL Assessments: Traditional methods, typically involving post-surgical questionnaires, often provide delayed insights that fail to inform real-time clinical decision-making, limiting the ability to preemptively address potential QoL issues.
- Gap in Predictive Care Models: There is a lack of robust predictive models to anticipate QoL outcomes before surgical interventions, which could significantly improve treatment planning and patient preparation.
- Untapped Potential of Healthcare Data: The vast amount of healthcare data in CRC management remains largely underutilized for predictive and personalized care approaches.
- Need for Personalized Treatment Strategies: Each CRC patient’s journey is unique, yet current treatment protocols lack the granularity to address individual QoL concerns effectively.
- Improving Informed Consent and Patient Expectations: More accurate predictions of post-treatment QoL could significantly enhance the informed consent process, helping to set realistic expectations and improve patient satisfaction.
- Enhancing Surgical Decision-Making: Predictive tools for QoL outcomes would enable surgeons and oncologists to make more informed decisions about surgical approaches and post-operative care strategies.
- GQOLI2: A broad measure of a patient’s subjective well-being across multiple life domains, offering insights into psychosocial adaptation post-treatment.
- Wexner Score: Assesses the severity of fecal incontinence, a common issue following colorectal cancer treatment, crucial for understanding its social and psychological impact.
- LARS Score: Quantifies bowel dysfunction symptoms experienced by patients after anterior resection, providing insights into functional recovery and needed interventions.
- AUR Score: Evaluates structural outcomes post-treatment using anorectal ultrasonography, linking physical changes to their impact on quality of life.
3. Related Works
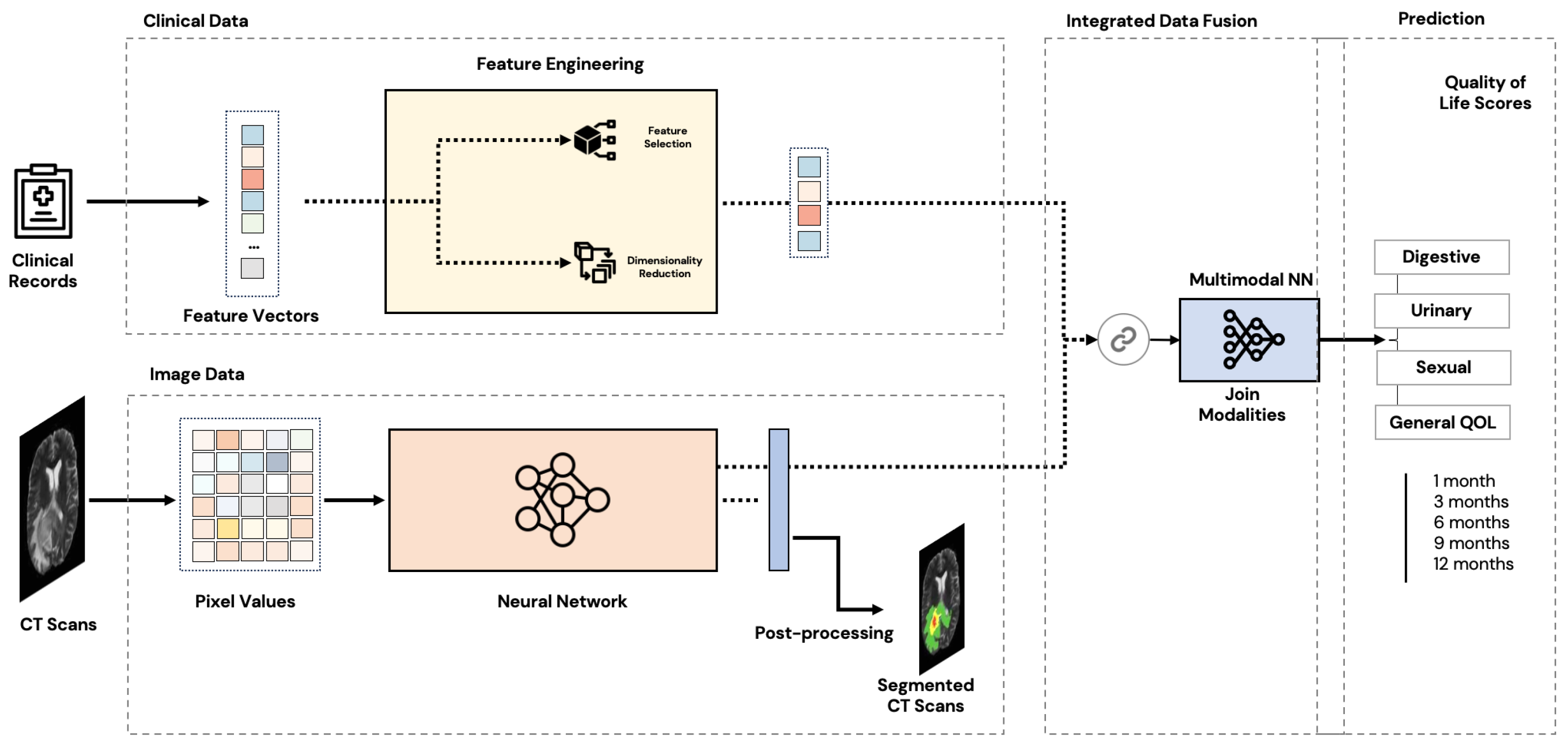
4. Methodology
4.1. Data Collection and Pre-Processing
4.1.1. Data Collection
- Clinical Data: Collected from electronic health records, the clinical dataset contains 49 features, including patient demographic information (age, gender), medical history (e.g., hypertension, diabetes, smoking status), treatment details (surgery type, chemotherapy, radiotherapy), and post-surgical outcomes (complications, recurrence rates). The longitudinal follow-up allowed us to track changes in the quality of life indicators such as the Wexner Score, LARS Score, and AUR Score over time.
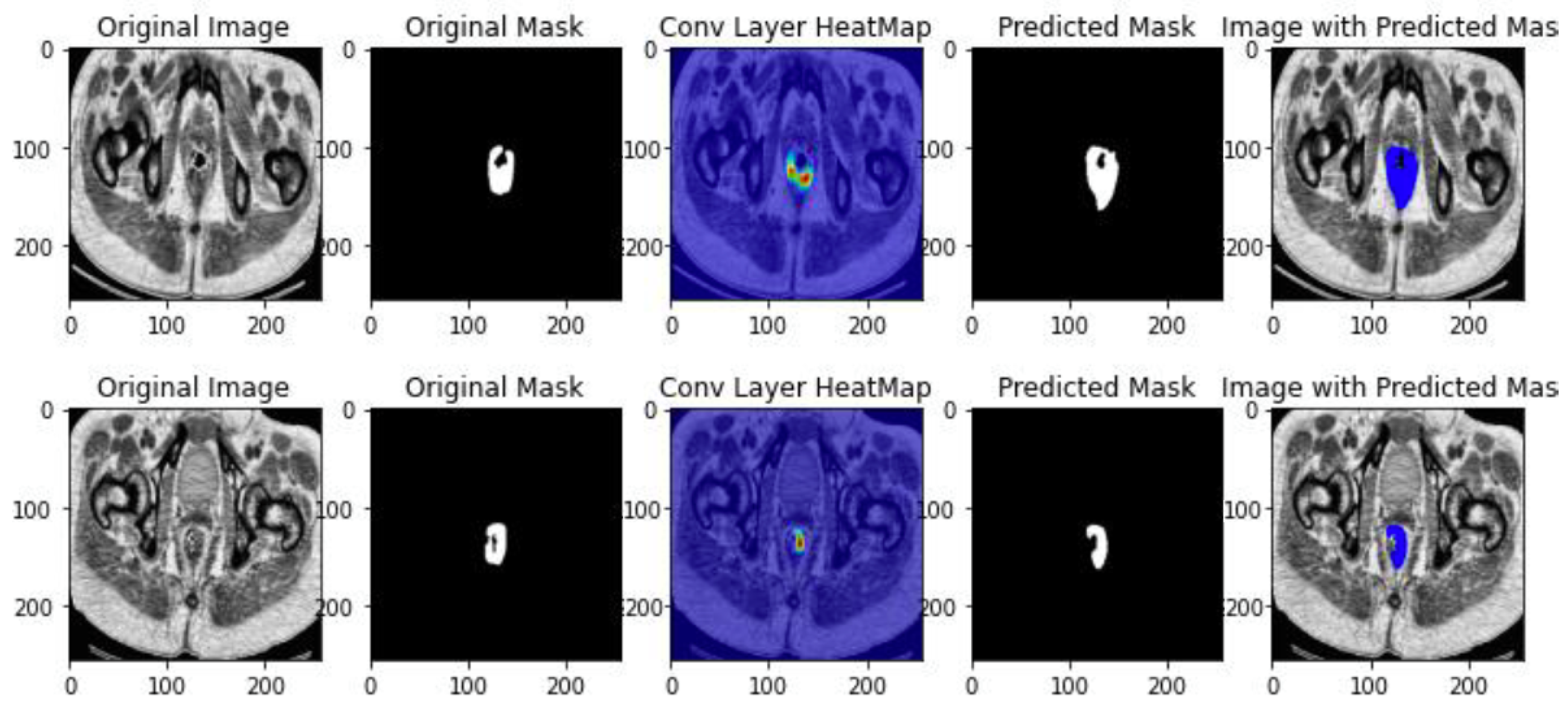
- Imaging Data: The CT scan images, collected at each follow-up point, provide detailed views of the patients’ anatomy. These images focus on tumor morphology and location. Tumor segmentation masks were manually annotated by medical professionals, highlighting the regions of interest for our analysis.
- Pre-surgical baseline measurements;
- Immediate post-surgical evaluations;
- Regular follow-up assessments at 3, 6, and 12 months post-surgery.
4.1.2. Clinical Data Acquisition
4.1.3. Pre-Processing
- Handling missing data by dropping columns with high missing values and imputing others using K-Nearest Neighbor algorithm [32].
- Handling outliers by correcting erroneous records with the help of experts.
- Discretizing continuous variables based on established thresholds to evaluate QoL.
- Balancing data by using Synthetic Minority Oversampling Technique (SMOTE) to generate synthetic samples and Random Oversampling for targets with insufficient samples.
- Scaling data to unify ranges and prevent confusion for the model.
- Encoding labels to handle numeric data and start from 0 rather than 1 for some algorithms.
4.1.4. Feature Engineering
4.1.5. Imaging Data Acquisition
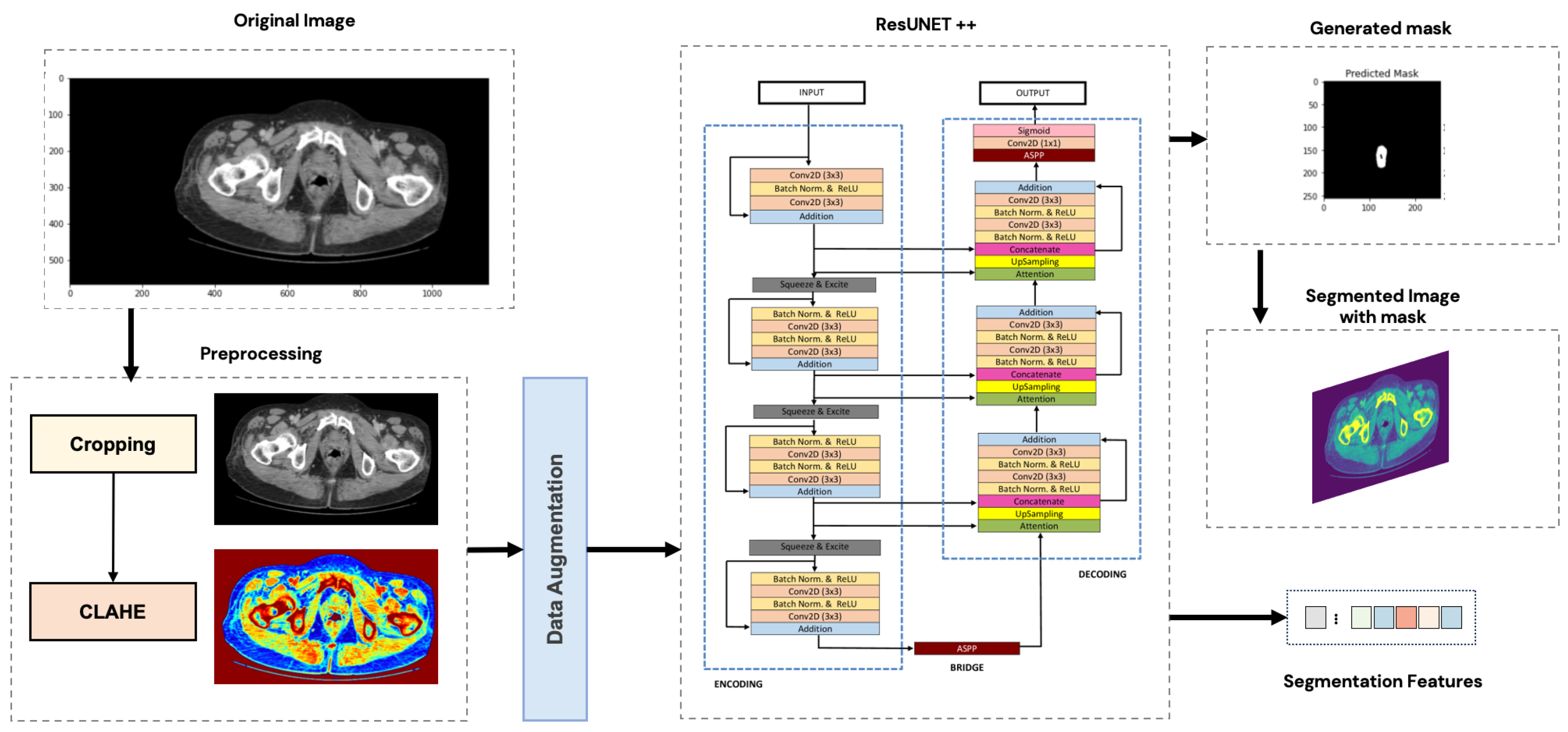
4.1.6. Pre-Processing
4.2. Clinical Data Analysis
4.2.1. Digestive Troubles Analysis
4.2.2. Urinary Troubles Analysis
4.2.3. Sexual Troubles Analysis
4.2.4. General Quality of Life Analysis
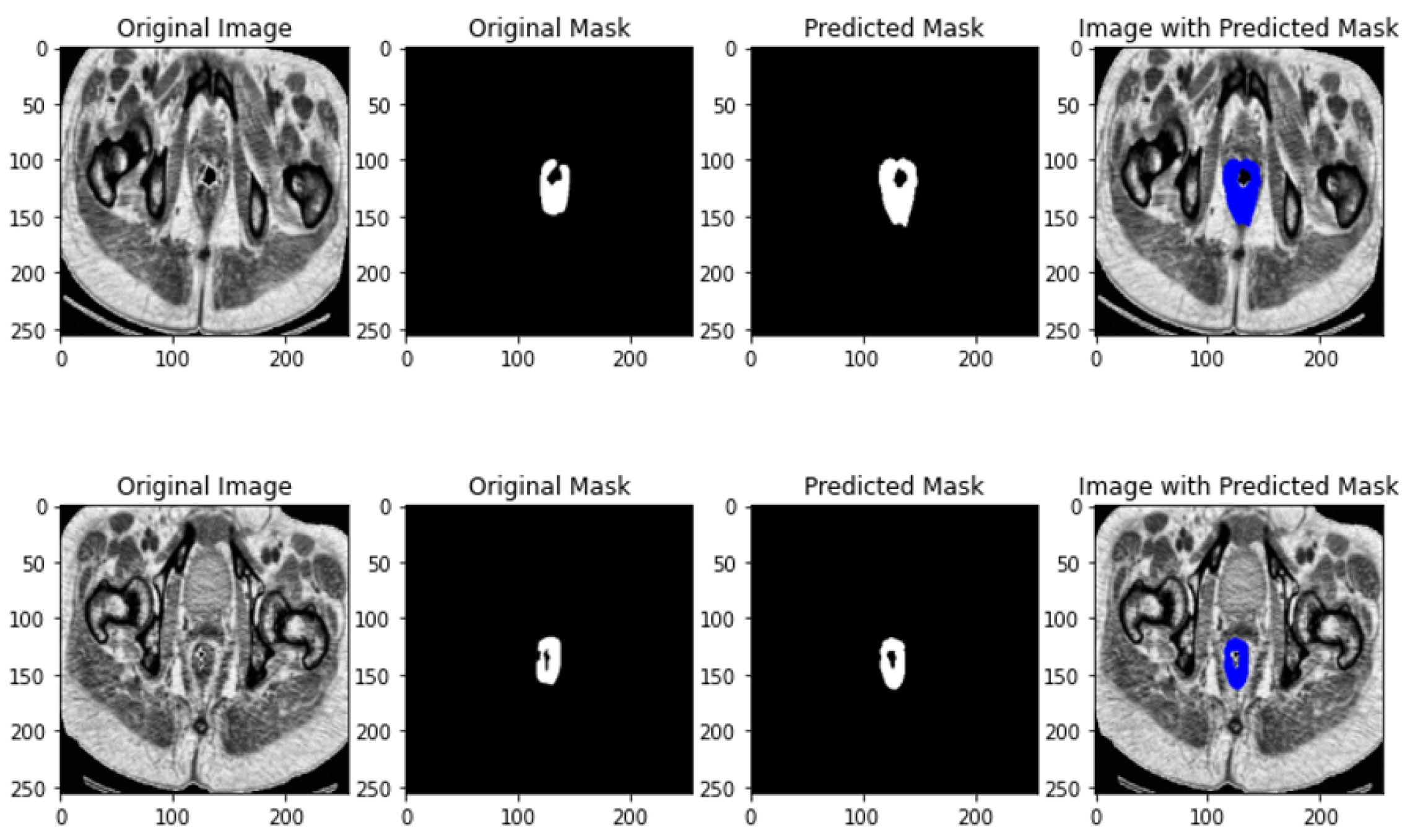
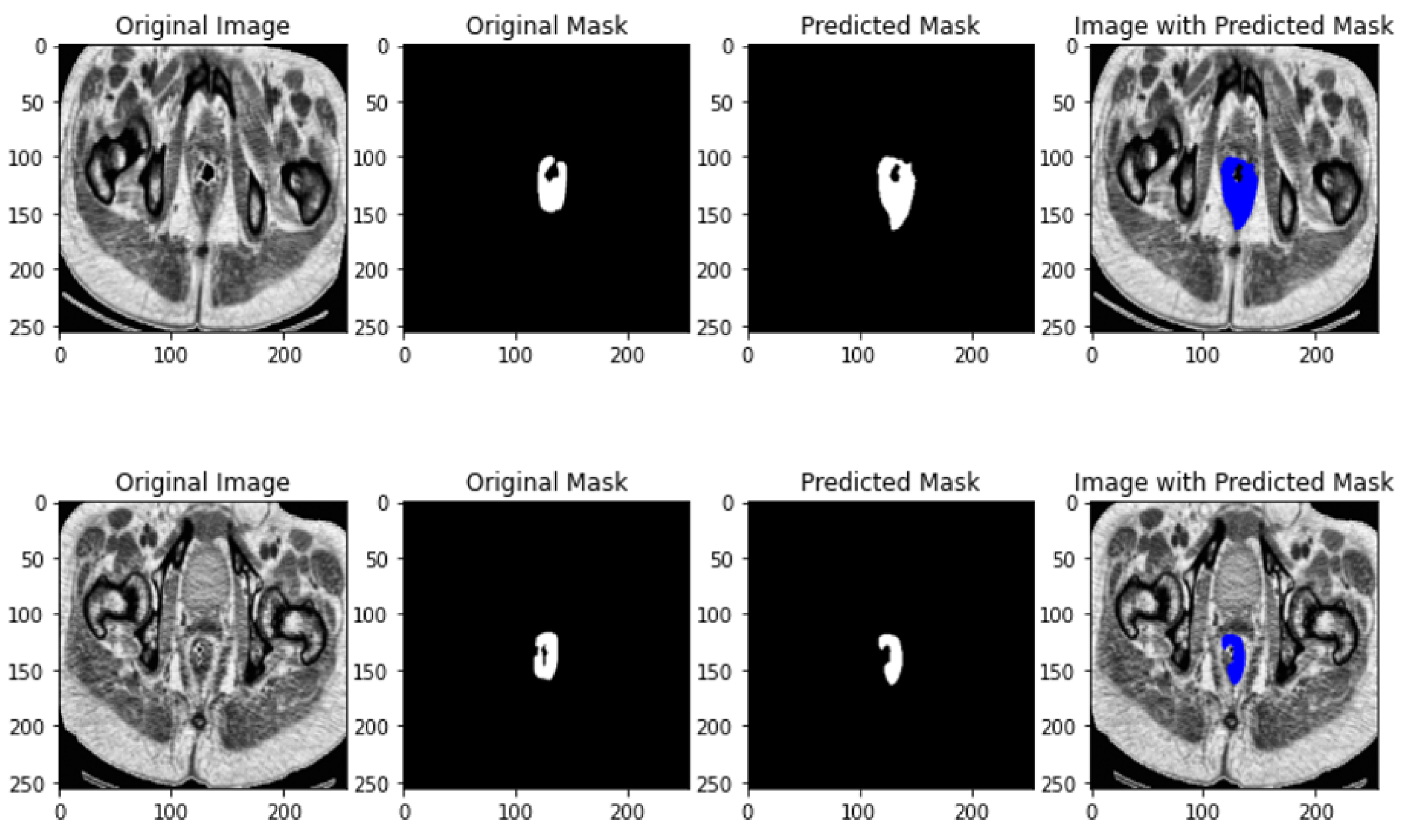
4.3. Imaging Data Segmentation
4.3.1. Segmentation Models
U-NET [6]
U-NET++ [40]
ResUNET [41]
ResUNET++ [42]
4.3.2. Segmentation Quality and Validation
- DICE Coefficient (Sørensen-Dice Index)
- A is the set of predicted labels (e.g., the predicted segmentation);
- B is the set of ground truth labels (e.g., the actual segmentation);
- is the intersection of the predicted and ground truth labels (i.e., the common area);
- and are the cardinalities (sizes) of sets A and B, respectively.
- A DICE coefficient of 1 indicates perfect overlap;
- A DICE coefficient of 0 indicates no overlap.
- Intersection over Union (IOU)
- A is the predicted segmentation;
- B is the ground truth segmentation;
- is the intersection of sets A and B;
- is the union of sets A and B, which can be calculated as .
- An IoU of 1 means perfect overlap;
- An IoU of 0 means no overlap.
4.4. Multimodal Data Integration
4.5. Results and Discussion
4.5.1. Implications
4.5.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Jansen, L.; Koch, L.; Brenner, H.; Arndt, V. Quality of life among long-term (⩾5 years) colorectal cancer survivors–systematic review. Eur. J. Cancer 2010, 46, 2879–2888. [Google Scholar] [CrossRef] [PubMed]
- Saraswat, D.; Bhattacharya, P.; Verma, A.; Prasad, V.K.; Tanwar, S.; Sharma, G.; Bokoro, P.N.; Sharma, R. Explainable AI for healthcare 5.0: Opportunities and challenges. IEEE Access 2022, 10, 84486–84517. [Google Scholar] [CrossRef]
- Chtouki, K.; Rhanoui, M.; Mikram, M.; Yousfi, S.; Amazian, K. Supervised Machine Learning for Breast Cancer Risk Factors Analysis and Survival Prediction. In Proceedings of the International Conference On Big Data and Internet of Things, Tangier, Morocco, 25–27 October 2023; Springer: Berlin/Heidelberg, Germany; pp. 59–71. [Google Scholar]
- Mikram, M.; Moujahdi, C.; Rhanoui, M.; Meddad, M.; Khallout, A. Hybrid deep learning models for diabetic retinopathy classification. In Proceedings of the International Conference On Big Data and Internet of Things, Rabat, Morocco, 17–18 March 2022; Springer: Berlin/Heidelberg, Germany; pp. 167–178. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; Springer: Berlin/Heidelberg, Germany; pp. 234–241. [Google Scholar]
- Fu, Y.; Lei, Y.; Wang, T.; Curran, W.J.; Liu, T.; Yang, X. A review of deep learning based methods for medical image multi-organ segmentation. Phys. Medica 2021, 85, 107–122. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.S.; Choi, B.S.; Chung, S.Y.; Kim, N.; Chun, J.; Kim, Y.B.; Chang, J.S.; Kim, J.S. Clinical evaluation of atlas-and deep learning-based automatic segmentation of multiple organs and clinical target volumes for breast cancer. Radiother. Oncol. 2020, 153, 139–145. [Google Scholar] [CrossRef]
- Xie, Y.; Xing, F.; Shi, X.; Kong, X.; Su, H.; Yang, L. Efficient and robust cell detection: A structured regression approach. Med Image Anal. 2018, 44, 245–254. [Google Scholar] [CrossRef]
- Mahmood, F.; Borders, D.; Chen, R.J.; McKay, G.N.; Salimian, K.J.; Baras, A.; Durr, N.J. Deep adversarial training for multi-organ nuclei segmentation in histopathology images. IEEE Trans. Med Imaging 2019, 39, 3257–3267. [Google Scholar] [CrossRef]
- Takamatsu, M.; Yamamoto, N.; Kawachi, H.; Chino, A.; Saito, S.; Ueno, M.; Ishikawa, Y.; Takazawa, Y.; Takeuchi, K. Prediction of early colorectal cancer metastasis by machine learning using digital slide images. Comput. Methods Programs Biomed. 2019, 178, 155–161. [Google Scholar] [CrossRef]
- Bychkov, D.; Linder, N.; Turkki, R.; Nordling, S.; Kovanen, P.E.; Verrill, C.; Walliander, M.; Lundin, M.; Haglund, C.; Lundin, J. Deep learning based tissue analysis predicts outcome in colorectal cancer. Sci. Rep. 2018, 8, 3395. [Google Scholar] [CrossRef]
- Baltrušaitis, T.; Ahuja, C.; Morency, L.P. Multimodal machine learning: A survey and taxonomy. IEEE Trans. Pattern Anal. Mach. Intell. 2018, 41, 423–443. [Google Scholar] [CrossRef]
- Lee, S.I.; Yoo, S.J. Multimodal deep learning for finance: Integrating and forecasting international stock markets. J. Supercomput. 2020, 76, 8294–8312. [Google Scholar] [CrossRef]
- Bousnina, N.; Ghouzali, S.; Mikram, M.; Abdul, W. DTCWT-DCT watermarking method for multimodal biometric authentication. In Proceedings of the 2nd International Conference on Networking, Information Systems & Security, Riyadh, Saudi Arabia, 1–3 May 2019; pp. 1–7. [Google Scholar]
- Acosta, J.N.; Falcone, G.J.; Rajpurkar, P.; Topol, E.J. Multimodal biomedical AI. Nat. Med. 2022, 28, 1773–1784. [Google Scholar] [CrossRef] [PubMed]
- Borgaonkar, M.; Irvine, E. Quality of life measurement in gastrointestinal and liver disorders. Gut 2000, 47, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Lewandowska, A.; Rudzki, G.; Lewandowski, T.; Próchnicki, M.; Rudzki, S.; Laskowska, B.; Brudniak, J. Quality of life of cancer patients treated with chemotherapy. Int. J. Environ. Res. Public Health 2020, 17, 6938. [Google Scholar] [CrossRef]
- Velikova, G.; Booth, L.; Smith, A.B.; Brown, P.M.; Lynch, P.; Brown, J.M.; Selby, P.J. Measuring quality of life in routine oncology practice improves communication and patient well-being: A randomized controlled trial. J. Clin. Oncol. 2004, 22, 714–724. [Google Scholar] [CrossRef]
- Breukink, S.; Van der Zaag-Loonen, H.; Bouma, E.; Pierie, J.; Hoff, C.; Wiggers, T.; Meijerink, W. Prospective evaluation of quality of life and sexual functioning after laparoscopic total mesorectal excision. Dis. Colon Rectum 2007, 50, 147–155. [Google Scholar] [CrossRef]
- Gray, N.M.; Hall, S.J.; Browne, S.; Macleod, U.; Mitchell, E.; Lee, A.J.; Johnston, M.; Wyke, S.; Samuel, L.; Weller, D.; et al. Modifiable and fixed factors predicting quality of life in people with colorectal cancer. Br. J. Cancer 2011, 104, 1697–1703. [Google Scholar] [CrossRef]
- Xu, Y.; Ju, L.; Tong, J.; Zhou, C.M.; Yang, J.J. Machine learning algorithms for predicting the recurrence of stage IV colorectal cancer after tumor resection. Sci. Rep. 2020, 10, 2519. [Google Scholar] [CrossRef]
- Valeikaite-Tauginiene, G.; Kraujelyte, A.; Poskus, E.; Jotautas, V.; Saladzinskas, Z.; Tamelis, A.; Lizdenis, P.; Dulskas, A.; Samalavicius, N.E.; Strupas, K.; et al. Predictors of quality of life six years after curative colorectal cancer surgery: Results of the prospective multicenter study. Medicina 2022, 58, 482. [Google Scholar] [CrossRef]
- Lu, S.C.; Xu, C.; Nguyen, C.H.; Geng, Y.; Pfob, A.; Sidey-Gibbons, C. Machine Learning–Based Short-Term Mortality Prediction Models for Patients With Cancer Using Electronic Health Record Data: Systematic Review and Critical Appraisal. JMIR Med. Inform. 2022, 10, e33182. [Google Scholar] [CrossRef]
- Sim, J.A.; Kim, Y.; Kim, J.H.; Lee, J.M.; Kim, M.S.; Shim, Y.M.; Zo, J.I.; Yun, Y.H. The major effects of health-related quality of life on 5-year survival prediction among lung cancer survivors: Applications of machine learning. Sci. Rep. 2020, 10, 10693. [Google Scholar] [CrossRef] [PubMed]
- Savić, M.; Kurbalija, V.; Ilić, M.; Ivanović, M.; Jakovetić, D.; Valachis, A.; Autexier, S.; Rust, J.; Kosmidis, T. Analysis of Machine Learning Models Predicting Quality of Life for Cancer Patients. In Proceedings of the 13th International Conference on Management of Digital EcoSystems, Virtual Event, 1–3 November 2021; pp. 35–42. [Google Scholar]
- Nuutinen, M.; Korhonen, S.; Hiltunen, A.M.; Haavisto, I.; Poikonen-Saksela, P.; Mattson, J.; Kondylakis, H.; Mazzocco, K.; Pat-Horenczyk, R.; Sousa, B.; et al. Impact of machine learning assistance on the quality of life prediction for breast cancer patients. In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies, Virtual Event, 9–11 February 2022; pp. 344–352. [Google Scholar]
- Zhou, C.; Hu, J.; Wang, Y.; Ji, M.H.; Tong, J.; Yang, J.J.; Xia, H. A machine learning-based predictor for the identification of the recurrence of patients with gastric cancer after operation. Sci. Rep. 2021, 11, 1571. [Google Scholar] [CrossRef] [PubMed]
- Ting, W.C.; Chang, H.R.; Chang, C.C.; Lu, C.J. Developing a novel machine learning-based classification scheme for predicting SPCs in colorectal cancer survivors. Appl. Sci. 2020, 10, 1355. [Google Scholar] [CrossRef]
- Karri, R.; Chen, Y.P.P.; Drummond, K.J. Using machine learning to predict health-related quality of life outcomes in patients with low grade glioma, meningioma, and acoustic neuroma. PLoS ONE 2022, 17, e0267931. [Google Scholar] [CrossRef] [PubMed]
- Trebeschi, S.; van Griethuysen, J.J.; Lambregts, D.M.; Lahaye, M.J.; Parmar, C.; Bakers, F.C.; Peters, N.H.; Beets-Tan, R.G.; Aerts, H.J. Deep learning for fully-automated localization and segmentation of rectal cancer on multiparametric MR. Sci. Rep. 2017, 7, 5301. [Google Scholar] [CrossRef]
- Peterson, L.E. K-nearest neighbor. Scholarpedia 2009, 4, 1883. [Google Scholar] [CrossRef]
- Whitley, D. A genetic algorithm tutorial. Stat. Comput. 1994, 4, 65–85. [Google Scholar] [CrossRef]
- Yang, X.S. Flower pollination algorithm for global optimization. In Proceedings of the International Conference on Unconventional Computing and Natural Computation, Orlean, France, 3–7 September 2012; Springer: Berlin/Heidelberg, Germany; pp. 240–249. [Google Scholar]
- Mirjalili, S. SCA: A sine cosine algorithm for solving optimization problems. Knowl.-Based Syst. 2016, 96, 120–133. [Google Scholar] [CrossRef]
- Mirjalili, S.; Gandomi, A.H.; Mirjalili, S.Z.; Saremi, S.; Faris, H.; Mirjalili, S.M. Salp Swarm Algorithm: A bio-inspired optimizer for engineering design problems. Adv. Eng. Softw. 2017, 114, 163–191. [Google Scholar] [CrossRef]
- Schapire, R.E. Explaining adaboost. In Empirical Inference: Festschrift in Honor of Vladimir N. Vapnik; Springer: Berlin/Heidelberg, Germany, 2013; pp. 37–52. [Google Scholar]
- Chen, T. Xgboost: Extreme gradient boosting. R Package Version 0.4-2 2015, 1. [Google Scholar]
- Friedman, J.H. Greedy function approximation: A gradient boosting machine. Ann. Stat. 2001, 1189–1232. [Google Scholar] [CrossRef]
- Zhou, Z.; Rahman Siddiquee, M.M.; Tajbakhsh, N.; Liang, J. Unet++: A nested u-net architecture for medical image segmentation. In Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support; Springer: Berlin/Heidelberg, Germany, 2018; pp. 3–11. [Google Scholar]
- Diakogiannis, F.I.; Waldner, F.; Caccetta, P.; Wu, C. ResUNet-a: A deep learning framework for semantic segmentation of remotely sensed data. ISPRS J. Photogramm. Remote Sens. 2020, 162, 94–114. [Google Scholar] [CrossRef]
- Jha, D.; Smedsrud, P.H.; Riegler, M.A.; Johansen, D.; De Lange, T.; Halvorsen, P.; Johansen, H.D. Resunet++: An advanced architecture for medical image segmentation. In Proceedings of the 2019 IEEE International Symposium on Multimedia (ISM), San Diego, CA, USA, 9–11 December 2019; pp. 225–2255. [Google Scholar]
- Bardak, B.; Tan, M. Improving clinical outcome predictions using convolution over medical entities with multimodal learning. Artif. Intell. Med. 2021, 117, 102112. [Google Scholar] [CrossRef] [PubMed]
- Zekaoui, N.E.; Yousfi, S.; Mikram, M.; Rhanoui, M. Enhancing Large Language Models’ Utility for Medical Question-Answering: A Patient Health Question Summarization Approach. In Proceedings of the 2023 14th International Conference on Intelligent Systems: Theories and Applications (SITA), Casablanca, Morocco, 22–23 November 2023; pp. 1–8. [Google Scholar]
- Tjoa, E.; Guan, C. A survey on explainable artificial intelligence (xai): Toward medical xai. IEEE Trans. Neural Netw. Learn. Syst. 2020, 32, 4793–4813. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article | Country | Objective | Data Types | Data Size | Pre-Processing | Feature Selection | Models | Main Metrics | Best Performance | Feature Importance |
|---|---|---|---|---|---|---|---|---|---|---|
| [20] | Netherlands | Descriptive Study Changes in QoL after tumor resection | Clinical | 56 | X | X | X | X | X | X |
| [21] | Scotland | Predictive Study Best Predictive Factors associated with QoL | Clinical | 496 | X | X | Linear Regression | R-Squared | 0.574 | Metastatic Gender Social functioning Fatigue Dyspnea Depression |
| [22] | Taiwan | Predictive Study postoperative recurrence risk among stage IV colorectal cancer patients | Clinical Demographical | 999 | Missing Data: Multiple Interpolation | X | Logistic Regression Decision Tree Gradient Boosting lightGBM | Main: AUC Secondary: Accuracy, F1-Score | LightGBM: AUC: 0.767 F1-Score: 0.974 Accuracy: 0.825 | Chemotherapy Age Operation time Carcinoembryonic antigen radiotherapy |
| [23] | Lithuania | Descriptive Study long-term results of the QoL after surgical treatment of CRC | Clinical Demographical | 88 | X | X | Linear Regression | X | X | Age Tumor location |
| [24] | Brazil USA Japan Iran Spain Turkey Taiwan China | Systematic Review Short-Term Mortality Prediction for QoL Improvement | Clinical Demographical | 173 to 26,946 | Numerical: Normalization, Discretization, Standardization Categorical: One-hot encoding Missing Data: constant value, complete case only, Probalistic imputation, missForest | Zero Variance Correlation LASSO Recursive FS Forward FS | Decision Tree Neural Networks Naïve Bayes Gradient Boosting Linear Regressions Random Forest Support Vector Machine | Main: AUROC Secondary: Accuracy | Neural Networks: AUROC: 0.92 Accuracy: X | X |
| [25] | South Korea | Predictive Study HRQOL features in a 5-year lung cancer survival prediction | Clinical Sociodemographic | 809 | Data Balancing: Oversampling Missing Data Imputation | Forward Feature Selection | Decision Tree Bagging Random Forest AdaBoost Logistic Regression | Main: AUC Secondary: Accuracy | Bagging AUC: 0.981 Accuracy: 0.93 | Cancer Stage Body Mass Index Depression Age |
| [26] | Sweden | Predictive Study prediction of QoL scores based on clinical data | Clinical | 18,988 and 2466 | Missing Data: Mean, Iterative MVI | X | Random Forest Support Vector Machine Naïve Bayes K Nearest Neighbor Decision Tree Neural Networks | F1-Score | Decision Tree and Random Forest F1-Score: 0.515–9.532 | X |
| [27] | Finland Israel Portugal Italy | Predictive Study performance to predict patients’ QoL during treatment process | Sociodemographic Clinical and psychosocial | 608 | Target column discretization | X | Random Forest | Main: AUROC Secondary: Recall, Precision, Accuracy | AUROC: 0.832 Recall: 0.727 Precision:0.727 Accuracy: 0.785 | Mental Health Age Distress Level Body Mass Index |
| [28] | Korea | Predictive Study gastric cancer recurrence after surgery | Clinical Demographical | 2012 | Missing Data Imputation Numerical Data: Normalization | X | lightGBM Random Forest Gradient Boosting Decision Tree Logistic Regression | Main: AUC Secondary: Accuracy, Precision, Recall | Random Forest AUC: 0.795 Recall: 0.148 Precision: 0.48 Accuracy: 0.797 | Body Mass Index Weight Operation Time Age Height Tumor Size Chemotherapy Tumor Location |
| [29] | Taiwan | Predictive Study Risk factors associated with second cancer in CRC patients | Clinical | 4287 | X | Not Mentioned | Random Forest MARS XGBoost Support Vector Machine Extreme Learning Machine | Main: AUC Secondary: Accuracy | XGBoost: AUC: 0.723 Accuracy: 0.695 | Sex Age Primary site Tumor Size Stage Drinking Behavior |
| [30] | Australia | Predictive Study Reduced HRQoL after tumor resection | Clinical | 262 | Missing Data: KNN Imputation Data Imbalance: SMOTE | X | Support Vector Machine Random Forest | AUC | SVM and Random Forest AUC: 0.69 to 0.98 | X |
| [31] | Netherlands Germany | Segmentation Study Localization and Segmentation of rectal cancer | Magnetic Resonance Imaging | 140 | Standardization of intensities Data Augmentation | X | Neural Networks | Dice Coefficient | 0.7 | X |
| Feature Column | Description |
|---|---|
| Age | Patient’s age |
| Gender | Patient’s gender |
| AHT | Patient has arterial hypertension or not |
| Diabetes | Patient has diabetes or not |
| Cardiopathy | Patient has a heart disease or not |
| Operated | Patient was previously operated or not |
| Tobacco | Patient smokes or not |
| Alcohol | Patient drinks alcohol or not |
| S Case | Patient had a similar case in his family or not |
| Dig Tumor | Patient has a digestive tumor or not |
| Extradig Tumor | Patient has a tumor out of the digestive system or not |
| Hematochezia | Patient has hematochezia or not |
| Rectal Syd | Patient has rectal syndromes or not |
| Occlusion | Patient has intestinal obstruction or not |
| Diarrhea | Patient has diarrhea or not |
| Constipation | Patient has constipation or not |
| Other | Patient has clinical signs other than the mentioned ones or not |
| TR | Patient had rectal examination or not |
| TRaspect | The aspect of the rectal examination: ulcerative budding, stenosing, sphincter impairment |
| Distance | Anal margin |
| TR:contraction | Patient has contraction or not |
| TR:circumference | Rectal circumference: ½, ¾, circumferential |
| Fixity | Whether the tumor is fixed on an anterior or posterior organ |
| rectoig/colo | Whether the examination made is a recto sigmoidoscopy or colonoscopy |
| endo:pos | Tumor position from endoscopy examination |
| Stenosis | Stenosing tumor or not |
| Type his | The histological type corresponds to the normal cell from which derives the tumor |
| pos(TDM/TAP) | Tumor position from CT Scan |
| Extent | Tumor size estimation from CT Scan |
| envah | Whether the tumor is invasive or not |
| Resectability | Whether it is possible to resect the tumor or not |
| ADPs | Whether there is an adenopathy or not |
| META | Whether there is metastasis or not |
| CMT | Whether the patient has undergone chemotherapy or not |
| CCR | Whether the patient has concurrent chemo-radiotherapy or not |
| Protocol | The CCR protocol: short, intermediate, long |
| Delay | Delay between Post-CCR and surgery |
| Surgery Type | Surgery type: Colectomy, anterior rectal resection, abdominoperineal amputation with definitive or protective colostomy |
| Path | Laser surgery: Laparotomy, laparoscopy, laparo conversion |
| Anastomosis type | A surgical procedure in which the colon is attached to another organ after resection of the rectum. |
| Reservoir | Whether the patient has a reservoir or not (is infected by pathogens or not) |
| Ileostomy/colostomy | Whether the patient has an opening to divert toward the tummy or not. |
| Temporary colostomy | Whether the patient has temp colostomy or not |
| Definitive colostomy | Whether the patient has definitive colostomy or not |
| CMTadjuvant | Whether the patient has additional chemotherapy treatment to lower recurrence risk or not |
| ANAPATH | Whether there was an anatomical pathology or not |
| yTNM | The cancer classification |
| Complications | Whether the patient had postoperative complications or not |
| Fistula | Whether the patient has fistula or not |
| Target | Model | F1-Score | Acc | Selected Features |
|---|---|---|---|---|
| LARS score (1 month) | Random Forest | 0.57 | 77% | Gender, Delay CMTadjuvante |
| LARS score (3 months) | LightGBM | 0.51 | 73% | S Case, Extradig Tumor Constipation, pos(TDM/TAP) envah, Surgery Type Anastomosis type, Stade |
| LARS score (6 months) | Logistic Regression | 0.34 | 63% | syd r, endo:pos ADPs, Surgery Type |
| LARS score (9 months) | Decision Tree | 0.35 | 70% | TR:contracture, endo:pos pos(TDM/TAP), envah |
| Wexner Score (1 month) | K-Nearest Neighbors | 0 | 67% | Age, Other endo:pos; Anastomosis type |
| Wexner Score (3 months) | K-Nearest Neighbors | 0.40 | 67% | Operated, distance Delay, Anastomosis type |
| Wexner Score (6 months) | Decision Tree | 0.30 | 77% | Occlusion, endo:pos Delay |
| Wexner Score (9 months) | Gradient Boosting | 0.34 | 77% | TR:contracture, pos(TDM/TAP) Colostomy |
| Target | Model | F1-Score | Acc | Selected Features |
|---|---|---|---|---|
| UI Score (3 months) | XGB | 0.21 | 70% | approach |
| UI Score (9 months) | XGB | 0.33 | 77% | Gender, rectoig/colo CCR |
| AUR Score (3 months) | Random Forest | 0.85 | 97% | Distance, Surgery Type approach |
| AUR Score (6 months) | Decision Tree | 0.79 | 97% | syd r, Other endo:pos, Surgery Type approach |
| AUR Score (9 months) | Decision Tree | 0.79 | 97% | pos(TDM/TAP), Protocol Anastomosis type, CMTadjuvante |
| AUR Score (12 months) | Gradient Boosting | 0.91 | 93% | Extradig Tumor, approach colotomie IGD |
| Target | Model | F1-Score | Acc | Selected Features |
|---|---|---|---|---|
| Dyspareunia (3 months) | Bagging | 0.18 | 63% | Constipation Fistula |
| Dyspareunia (6 months) | Decision Tree | 0.31 | 77% | Gender, HTA Diabetes, Cardiopathy Operated, Tobacco Alcohol, S Case Extradig Tumor, rectorragies Occlusion |
| Dyspareunia (9 months) | Random Forest | 0.70 | 90% | Gender, Alcohol Extradig Tumor, rectorragies syd r, Occlusion Other, Distance |
| Dyspareunia (12 months) | XGB | 0.88 | 97% | Age Gender |
| Target | Model | F1-Score | Acc | Selected Features |
|---|---|---|---|---|
| Ejaculation Troubles | SVC | 0.74 | 87% | Gender, Distance TR: circumference |
| Erection troubles (3 months) | K-Nearest Neighbor | 0.91 | 97% | Gender, Diabetes Tobacco, syd r Constipation, envah |
| Erection troubles (6 months) | Random Forest | 0.93 | 97% | Cardiopathy, Occlusion Distance, TR:circumference envah, resecability CCR, reservoir CMTadjuvante, ANAPATH |
| Erection troubles (9 months) | Decision Tree | 0.82 | 93% | Gender, S Case Dig Tumor, rectorragies Constipation, Other Distance |
| Erection troubles (12 months) | Decision Tree | 0.88 | 93% | Gender, syd r Diarrhea, Other Distance, TR:circumference |
| Variable | Model | F1-1 Score | Acc | Selected Features |
|---|---|---|---|---|
| GQOL (1 month) | AdaBoost | 0.85 | 87% | Age, Gender Cardiopathy, Operated Extradig Tumor, Diarrhea Other, stenose Protocol, approach ileotsomie, Temp Colostomy |
| GQOL (3 months) | XGB | 0.84 | 83% | Gender, Extradig Tumor distance, Delay Colostomy |
| GQOL (6 months) | Gradient Boosting | 0.8 | 80% | Extradig Tumor, pos(TDM/TAP) Anastomosis type, ileotsomie CMTadjuvante |
| GQOL (9 months) | XGB | 0.87 | 87% | syd r, Occlusion Constipation, TRaspect rectoig/colo, endo:pos CCR, approach reservoir, Temp Colostomy Colostomy, Stade |
| GQOL (12 months) | Gradient Boosting | 0.96 | 93% | HTA, Cardiopathy Operated, Tobacco Extradig Tumor, syd r Occlusion, Other endo:pos, type his envah, Protocol Delay, suite Fistula, Stade |
| Model | DICE | IOU |
|---|---|---|
| UNET | 74% | 58% |
| UNET++ | 67% | 51% |
| ResUNET | 72% | 56% |
| ResUNET++ | 76% | 61% |
| Target Variable | Approach | Fusion Type | Test Accuracy |
|---|---|---|---|
| GQOL12 | Mono-Modal | No Fusion | 64% |
| Multi-Modal | Joint Fusion | 64% | |
| Wexner Score 3 | Mono-Modal | No Fusion | 24% |
| Multi-Modal | Joint Fusion | 48% | |
| LARS Score 9 | Mono-Modal | No Fusion | 60% |
| Multi-Modal | Joint Fusion | 60% | |
| AUR Score 9 | Mono-Modal | No Fusion | 88% |
| Multi-Modal | Joint Fusion | 96% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rhanoui, M.; Mikram, M.; Amazian, K.; Ait-Abderrahim, A.; Yousfi, S.; Toughrai, I. Multimodal Machine Learning for Predicting Post-Surgery Quality of Life in Colorectal Cancer Patients. J. Imaging 2024, 10, 297. https://doi.org/10.3390/jimaging10120297
Rhanoui M, Mikram M, Amazian K, Ait-Abderrahim A, Yousfi S, Toughrai I. Multimodal Machine Learning for Predicting Post-Surgery Quality of Life in Colorectal Cancer Patients. Journal of Imaging. 2024; 10(12):297. https://doi.org/10.3390/jimaging10120297
Chicago/Turabian StyleRhanoui, Maryem, Mounia Mikram, Kamelia Amazian, Abderrahim Ait-Abderrahim, Siham Yousfi, and Imane Toughrai. 2024. "Multimodal Machine Learning for Predicting Post-Surgery Quality of Life in Colorectal Cancer Patients" Journal of Imaging 10, no. 12: 297. https://doi.org/10.3390/jimaging10120297
APA StyleRhanoui, M., Mikram, M., Amazian, K., Ait-Abderrahim, A., Yousfi, S., & Toughrai, I. (2024). Multimodal Machine Learning for Predicting Post-Surgery Quality of Life in Colorectal Cancer Patients. Journal of Imaging, 10(12), 297. https://doi.org/10.3390/jimaging10120297