
Short- and Midterm Comparison of Platelet-Rich Plasma with Hyaluronic Acid versus Leucocyte and Platelet-Rich Plasma on Pain and Function to Treat Hip Osteoarthritis. A Retrospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Results and Discussion
2.1. Descriptive Statistics
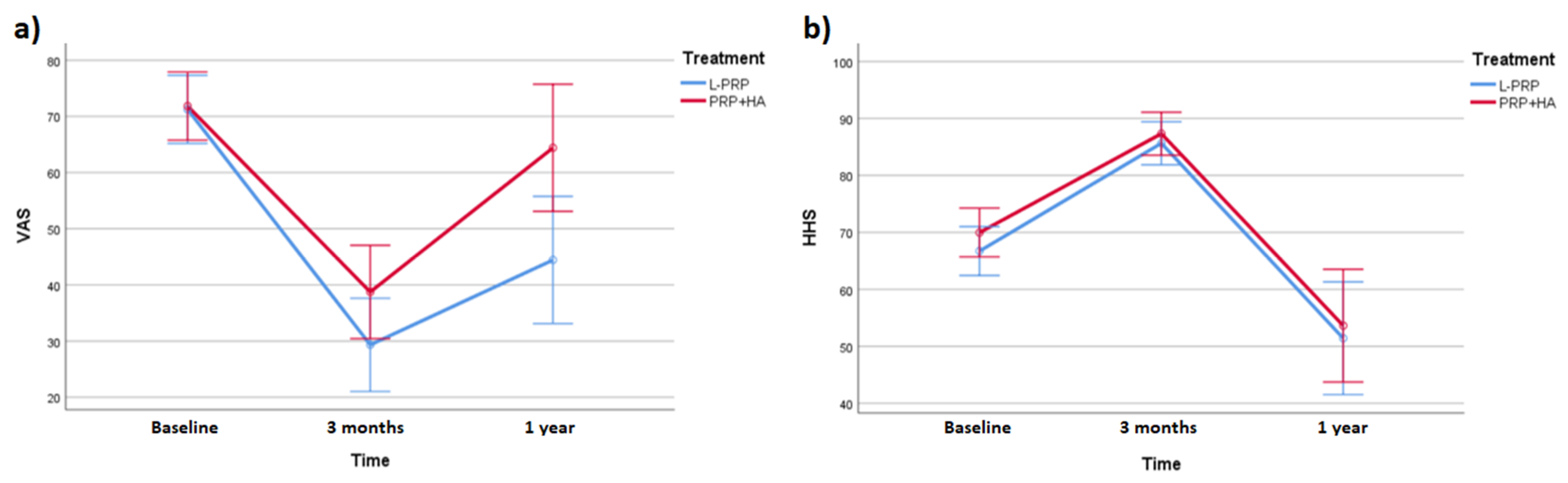
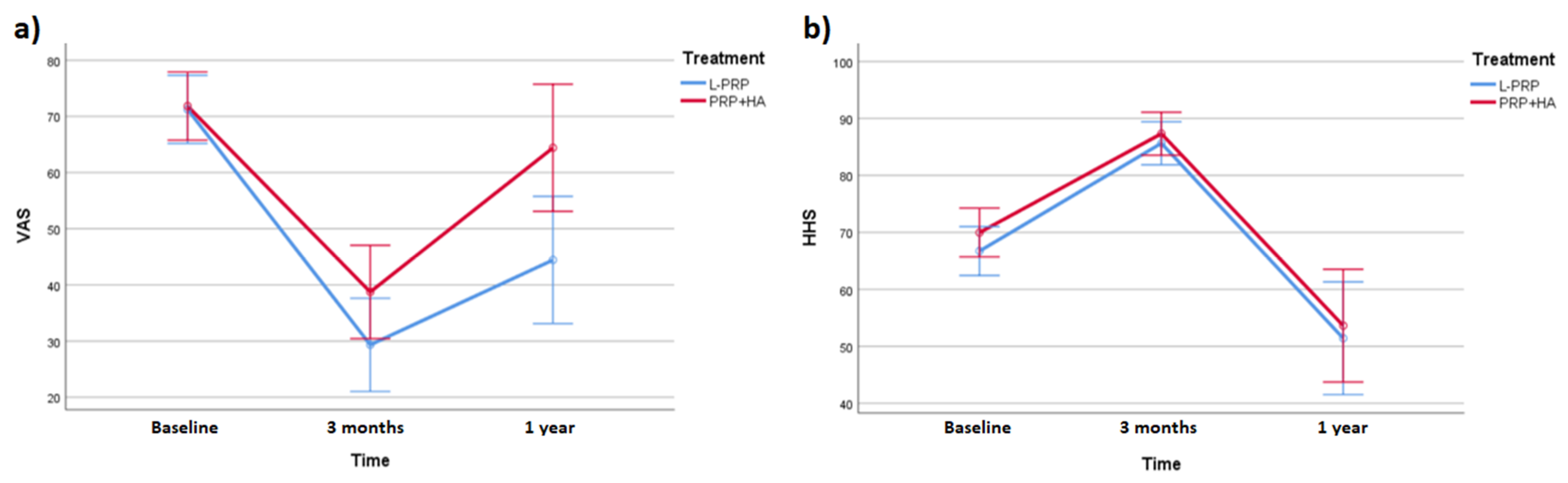
2.2. Efficacy of L-PRP and PRP+HA
2.3. Differences between Treatments
3. Conclusions
4. Materials and Methods
4.1. Study Design
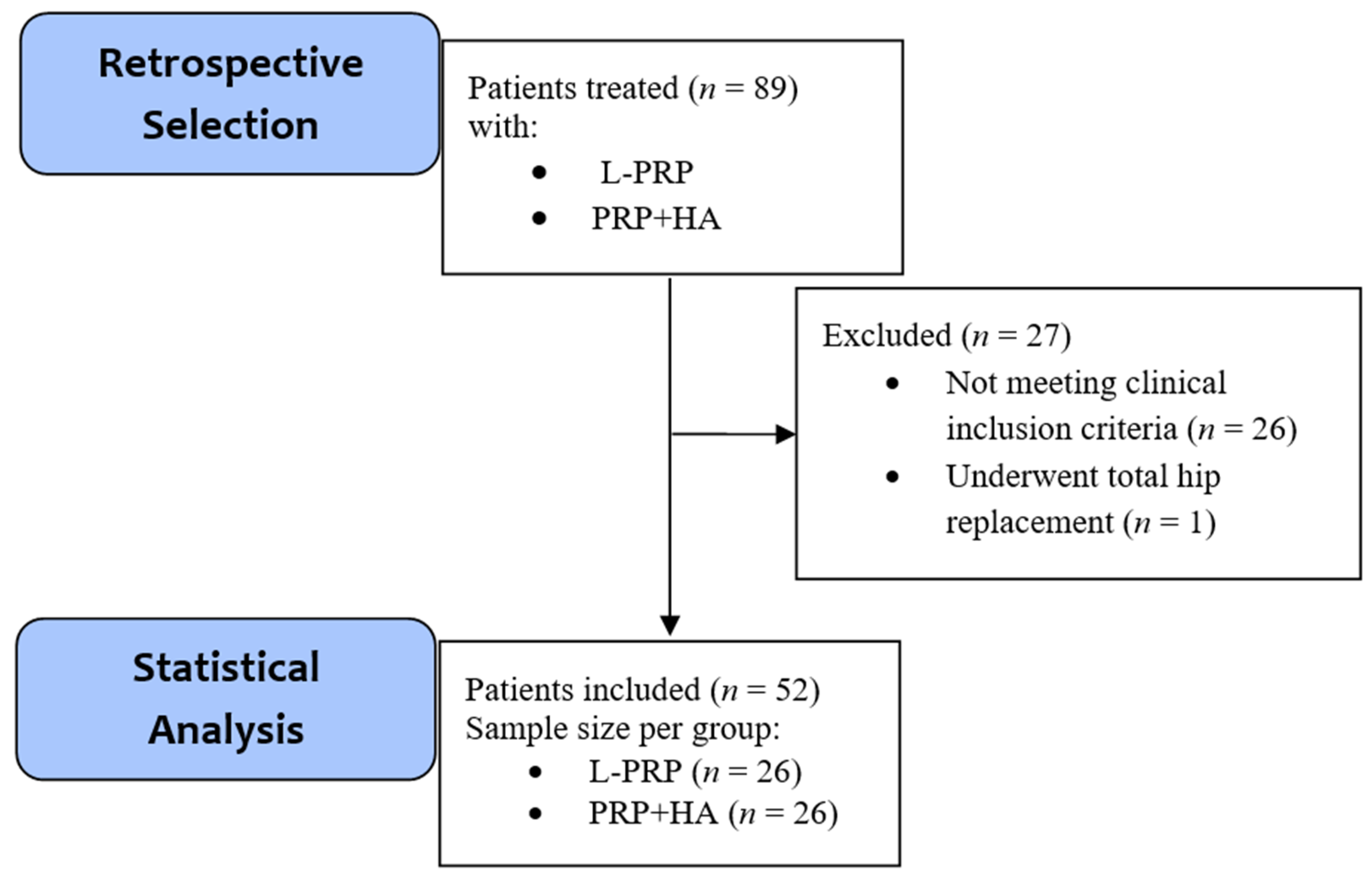
4.1.1. Patient Selection
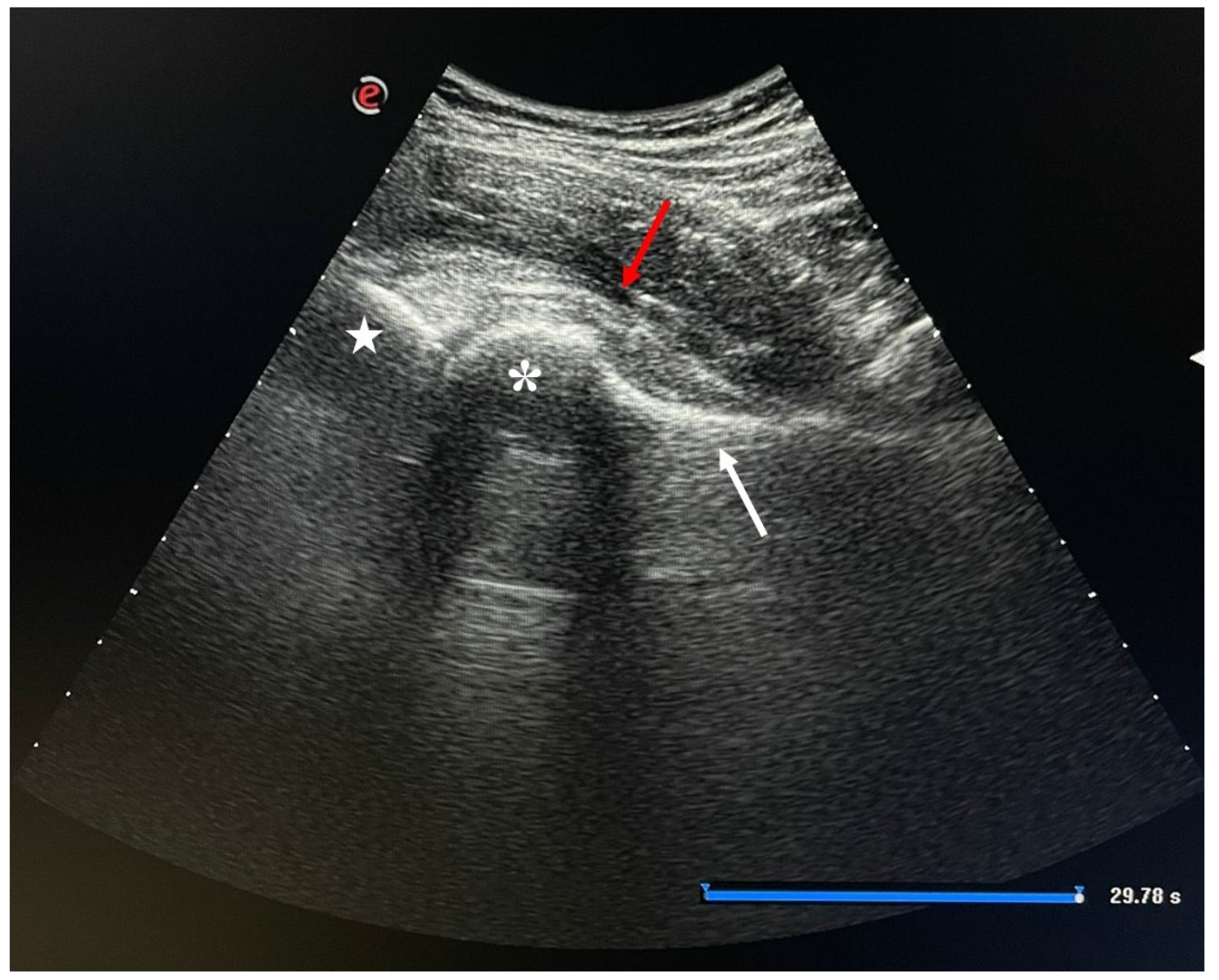
4.1.2. Injection Procedure
4.1.3. Treatment
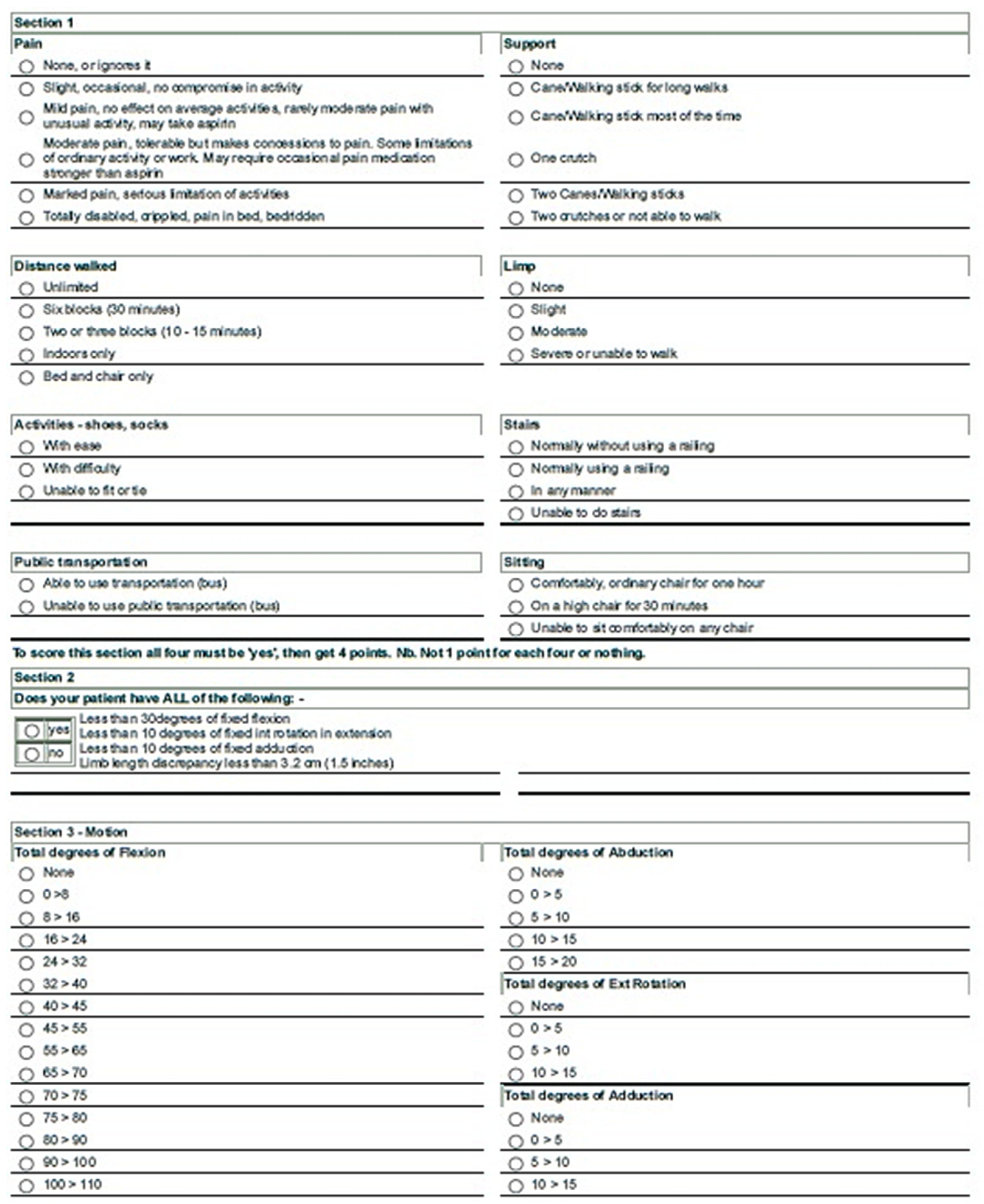
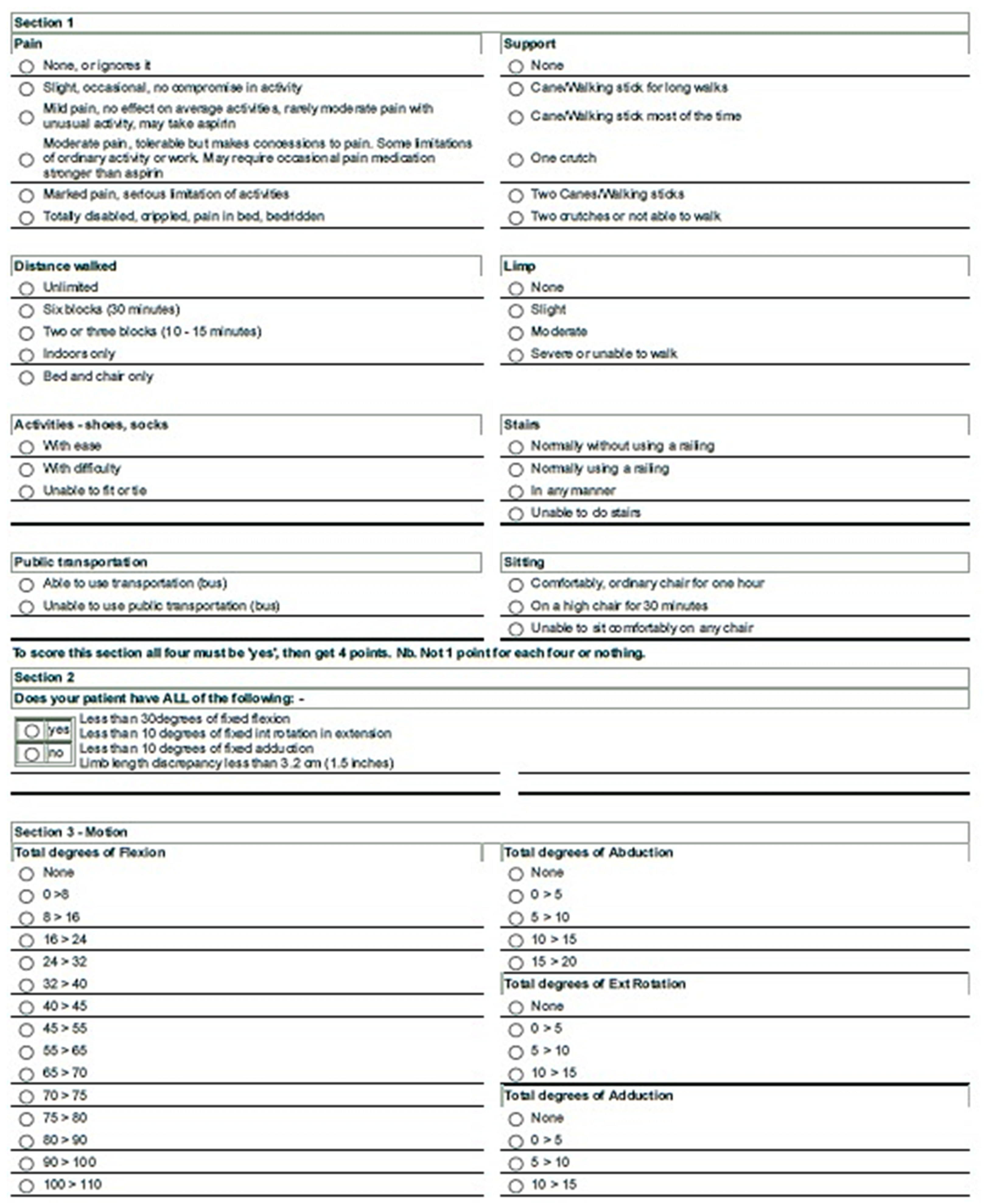
4.1.4. Outcomes
4.1.5. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef]
- Hussain, S.; Neilly, D.; Baliga, S.; Patil, S.; Meek, R. Knee osteoarthritis: A review of management options. Scott. Med. J. 2016, 61, 7–16. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Z.; Ma, J.; Ma, X. Different Intra-articular Injections as Therapy for Hip Osteoarthritis: A Systematic Review and Network Meta-analysis. Arthrosc. J. Arthrosc. Relat. Surg. 2020, 36, 1452–1464.e2. [Google Scholar] [CrossRef] [PubMed]
- Palco, M.; Fenga, D.; Basile, G.C.; Rizzo, P.; Cavalieri, B.; Leonetti, D.; Alito, A.; Bruschetta, A.; Traina, F. Platelet-Rich Plasma Combined with Hyaluronic Acid versus Leucocyte and Platelet-Rich Plasma in the Conservative Treatment of Knee Osteoarthritis. A Retrospective Study. Med. Kaunas Lith. 2021, 57, 232. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, M.D.O.; Barbieri, C.H.; Barbieri Neto, J. Platelet-rich plasma gel promotes regeneration of articular cartilage in knees of sheeps. Acta Ortop. Bras. 2013, 21, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Filardo, G.; Madry, H.; Jelic, M.; Roffi, A.; Cucchiarini, M.; Kon, E. Mesenchymal stem cells for the treatment of cartilage lesions: From preclinical findings to clinical application in orthopaedics. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 1717–1729. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Yuan, T.; Chen, S.; Xie, X.; Zhang, C. The temporal effect of platelet-rich plasma on pain and physical function in the treatment of knee osteoarthritis: Systematic review and meta-analysis of randomized controlled trials. J. Orthop. Surg. 2017, 12, 16. [Google Scholar] [CrossRef] [Green Version]
- Anitua, E.; Sánchez, M.; Nurden, A.T.; Zalduendo, M.M.; de la Fuente, M.; Azofra, J.; Andía, I. Platelet-released growth factors enhance the secretion of hyaluronic acid and induce hepatocyte growth factor production by synovial fibroblasts from arthritic patients. Rheumatol. Oxf. Engl. 2007, 46, 1769–1772. [Google Scholar] [CrossRef] [Green Version]
- Battaglia, M.; Guaraldi, F.; Vannini, F.; Buscio, T.; Buda, R.; Galletti, S. Platelet-rich plasma (PRP) intra-articular ultrasound-guided injections as a possible treatment for hip osteoarthritis: A pilot study. Clin. Exp. Rheumatol. 2011, 29, 754. [Google Scholar]
- Reid, M.C. Viscosupplementation for osteoarthritis: A primer for primary care physicians. Adv. Ther. 2013, 30, 967–986. [Google Scholar] [CrossRef] [Green Version]
- Gobbi, A.; Bathan, L. Biological approaches for cartilage repair. J. Knee Surg. 2009, 22, 36–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavallo, C.; Filardo, G.; Mariani, E.; Kon, E.; Marcacci, M.; Pereira Ruiz, M.T.; Facchini, A.; Grigolo, B. Comparison of platelet-rich plasma formulations for cartilage healing: An in vitro study. J. Bone Joint Surg. Am. 2014, 96, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Iio, K.; Furukawa, K.-I.; Tsuda, E.; Yamamoto, Y.; Maeda, S.; Naraoka, T.; Kimura, Y.; Ishibashi, Y. Hyaluronic acid induces the release of growth factors from platelet-rich plasma. Asia-Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2016, 4, 27–32. [Google Scholar] [CrossRef]
- Garcia, F.L.; Williams, B.T.; Polce, E.M.; Heller, D.B.; Aman, Z.S.; Nwachukwu, B.U.; Nho, S.J.; Chahla, J. Preparation Methods and Clinical Outcomes of Platelet-Rich Plasma for Intra-articular Hip Disorders: A Systematic Review and Meta-analysis of Randomized Clinical Trials. Orthop. J. Sports Med. 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Gazendam, A.; Ekhtiari, S.; Bozzo, A.; Phillips, M.; Bhandari, M. Intra-articular saline injection is as effective as corticosteroids, platelet-rich plasma and hyaluronic acid for hip osteoarthritis pain: A systematic review and network meta-analysis of randomised controlled trials. Br. J. Sports Med. 2021, 55, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.D.; Devji, T.; Bhandari, M.; Fierlinger, A.; Niazi, F.; Christensen, R. Clinical benefit of intra-articular saline as a comparator in clinical trials of knee osteoarthritis treatments: A systematic review and meta-analysis of randomized trials. Semin. Arthritis Rheum. 2016, 46, 151–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandak, E.; Overgaard, A.F.; Kristensen, L.E.; Ellegaard, K.; Guldberg-Møller, J.; Bartholdy, C.; Hunter, D.J.; Altman, R.D.; Christensen, R.; Bliddal, H.; et al. Exercise therapy and patient education versus intra-articular saline injections in the treatment of knee osteoarthritis: An evidence-based protocol for an open-label randomised controlled trial (the DISCO trial). Trials 2021, 22, 18. [Google Scholar] [CrossRef] [PubMed]
- Sante, L.D.; Villani, C.; Santilli, V.; Valeo, M.; Bologna, E.; Imparato, L.; Paoloni, M.; Iagnocco, A. Intra-articular hyaluronic acid vs platelet-rich plasma in the treatment of hip osteoarthritis. Med. Ultrason. 2016, 18, 463. [Google Scholar] [CrossRef] [Green Version]
- Dallari, D.; Stagni, C.; Rani, N.; Sabbioni, G.; Pelotti, P.; Torricelli, P.; Tschon, M.; Giavaresi, G. Ultrasound-Guided Injection of Platelet-Rich Plasma and Hyaluronic Acid, Separately and in Combination, for Hip Osteoarthritis: A Randomized Controlled Study. Am. J. Sports Med. 2016, 44, 664–671. [Google Scholar] [CrossRef]
- Medina-Porqueres, I.; Ortega-Castillo, M.; Muriel-Garcia, A. Effectiveness of platelet-rich plasma in the management of hip osteoarthritis: A systematic review and meta-analysis. Clin. Rheumatol. 2021, 40, 53–64. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological Assessment of Osteo-Arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Harris, W.H. Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J. Bone Joint Surg. Am. 1969, 51, 737–755. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, P.; Binazzi, R.; Vaccari, V.; Girolami, M.; Morici, F.; Impallomeni, C.; Commessatti, M.; Silvello, L. Long-term results with cementless Fitek (or Fitmore) cups. J. Arthroplast. 2005, 20, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Dettoni, F.; Pellegrino, P.; La Russa, M.R.; Bonasia, D.E.; Blonna, D.; Bruzzone, M.; Castoldi, F.; Rossi, R. Validation and cross cultural adaptation of the Italian version of the Harris Hip Score. Hip. Int. J. Clin. Exp. Res. Hip. Pathol. Ther. 2015, 25, 91–97. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Group | L-PRP | PRP+HA | Total | |
|---|---|---|---|---|
| Age | 50.62 ± 16.14 | 64.81 ± 10.81 | 57.47 ± 15.20 | |
| Sex | M/F | 16/10 | 12/14 | 28/24 |
| KL grade | II/III | 14/12 | 10/16 | 24/28 |
| Baseline | 3 Months FU | 1 Year FU | |
|---|---|---|---|
| VAS (L-PRP) | 72.69 ± 13.65 | 30.00 ± 16.37 | 49.62 ± 14.53 |
| VAS (PRP+HA) | 70.38 ± 15.55 | 38.08 ± 19.90 | 59.23 ± 26.74 |
| HHS (L-PRP) | 66.86 ± 9.96 | 86.09 ± 8.88 | 53.08 ± 24.31 |
| HHS (PRP+HA) | 69.93 ± 10.31 | 86.88 ± 8.88 | 51.97 ± 22.91 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palco, M.; Rizzo, P.; Basile, G.C.; Alito, A.; Bruschetta, D.; Accorinti, M.; Restuccia, R.; Leonetti, D. Short- and Midterm Comparison of Platelet-Rich Plasma with Hyaluronic Acid versus Leucocyte and Platelet-Rich Plasma on Pain and Function to Treat Hip Osteoarthritis. A Retrospective Study. Gels 2021, 7, 222. https://doi.org/10.3390/gels7040222
Palco M, Rizzo P, Basile GC, Alito A, Bruschetta D, Accorinti M, Restuccia R, Leonetti D. Short- and Midterm Comparison of Platelet-Rich Plasma with Hyaluronic Acid versus Leucocyte and Platelet-Rich Plasma on Pain and Function to Treat Hip Osteoarthritis. A Retrospective Study. Gels. 2021; 7(4):222. https://doi.org/10.3390/gels7040222
Chicago/Turabian StylePalco, Michelangelo, Paolo Rizzo, Giorgio Carmelo Basile, Angelo Alito, Daniele Bruschetta, Maria Accorinti, Roberto Restuccia, and Danilo Leonetti. 2021. "Short- and Midterm Comparison of Platelet-Rich Plasma with Hyaluronic Acid versus Leucocyte and Platelet-Rich Plasma on Pain and Function to Treat Hip Osteoarthritis. A Retrospective Study" Gels 7, no. 4: 222. https://doi.org/10.3390/gels7040222
APA StylePalco, M., Rizzo, P., Basile, G. C., Alito, A., Bruschetta, D., Accorinti, M., Restuccia, R., & Leonetti, D. (2021). Short- and Midterm Comparison of Platelet-Rich Plasma with Hyaluronic Acid versus Leucocyte and Platelet-Rich Plasma on Pain and Function to Treat Hip Osteoarthritis. A Retrospective Study. Gels, 7(4), 222. https://doi.org/10.3390/gels7040222