
I-CARE-An Interaction System for the Individual Activation of People with Dementia

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. Research Questions
1.2. Ethical Guidelines and Key Objectives
2. Related Work: I-CARE in Comparison to Other System for People with Dementia
2.1. Technical Systems for People with Dementia
2.2. Technical Systems for Activation of People with Dementia
2.3. Studies of Activation Systems in the Field
2.4. Summary of the State-of-the-Art
3. Materials and Methods
3.1. I-CARE Activation Content
3.2. I-CARE System Architecture
3.3. I-CARE Intelligent Services
3.3.1. Annotation and Assessment of Interaction Events
3.3.2. Facial Analysis and Emotion Recognition
3.3.3. Biosignal Analysis based on Interactions, Psychophysiological Indicators and Voice
3.3.4. User Modeling and Recommendation System
3.3.5. Data-driven Analysis of User Interaction
3.4. I-CARE Evaluation & Study Participants
4. Results
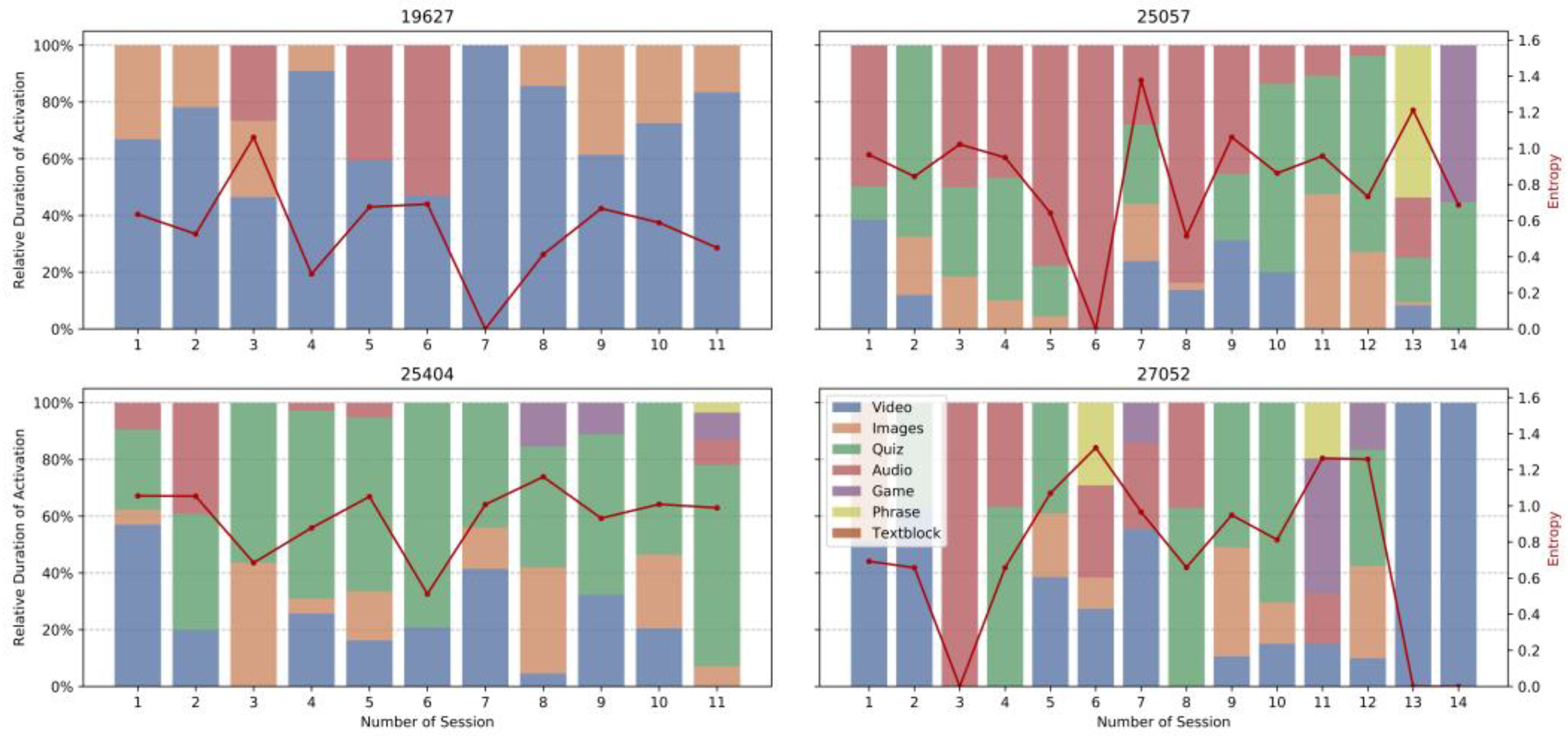
4.1. Usage Statistics
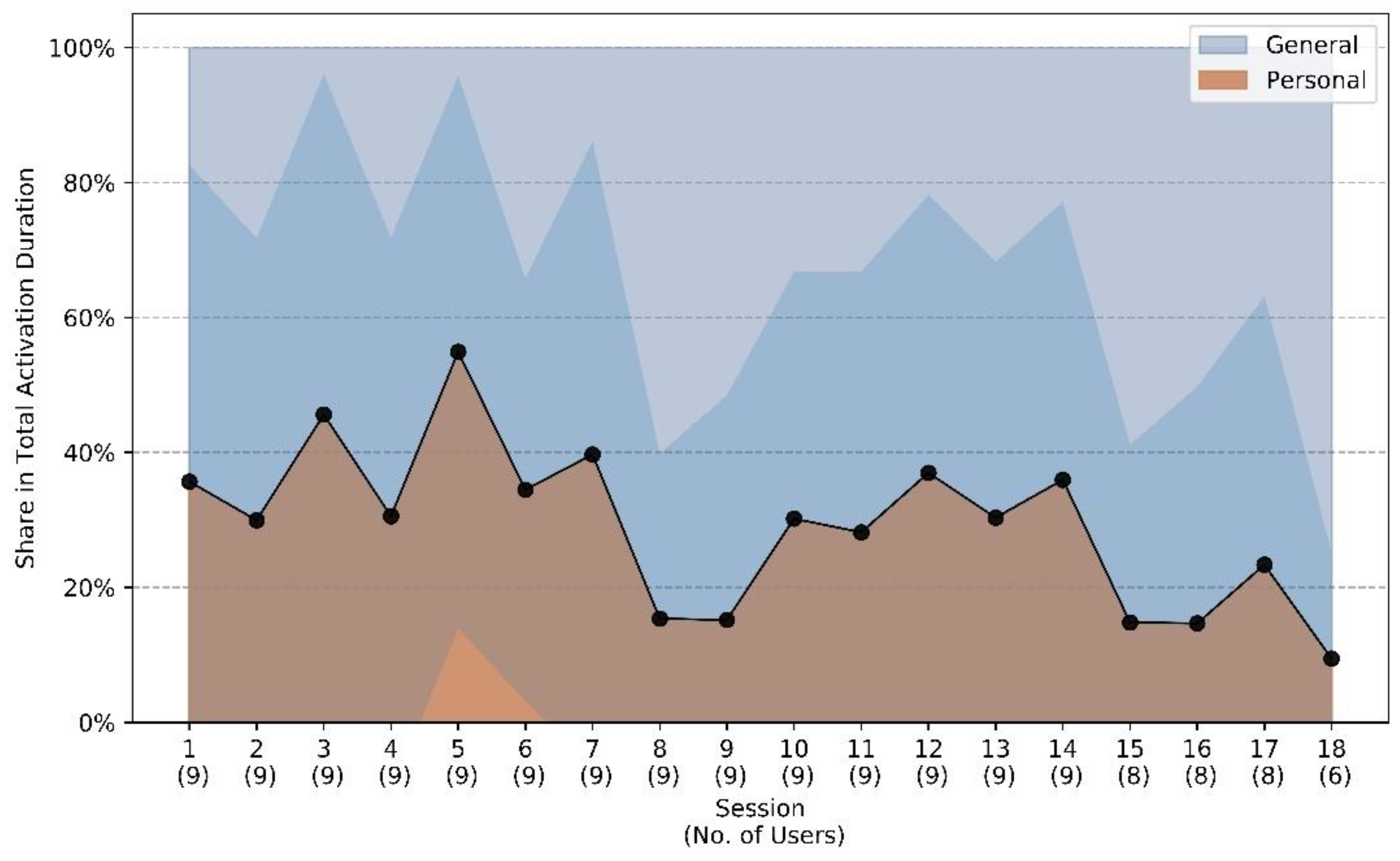
4.2. User Preferences
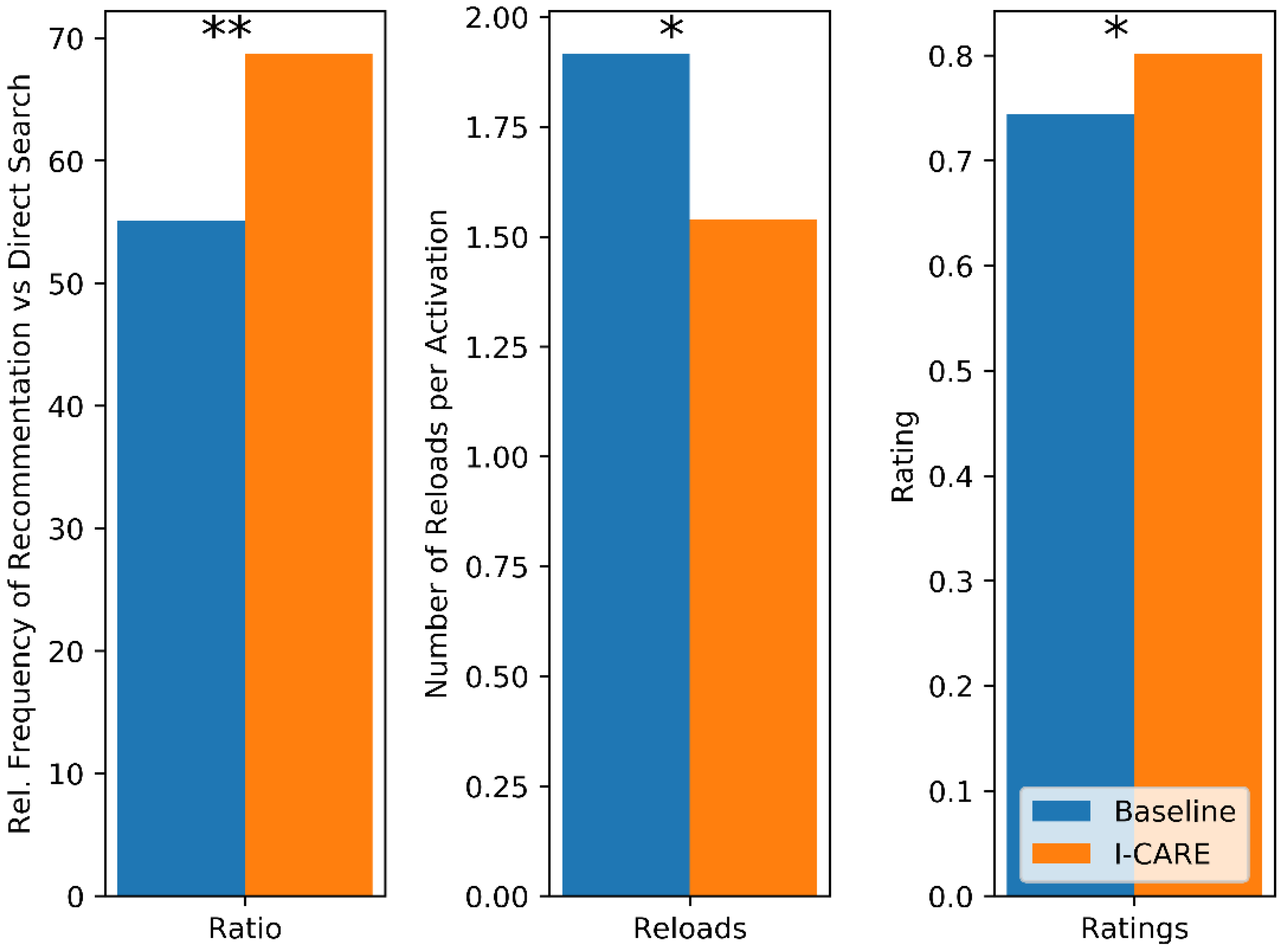
4.3. Recommendation System Evaluation
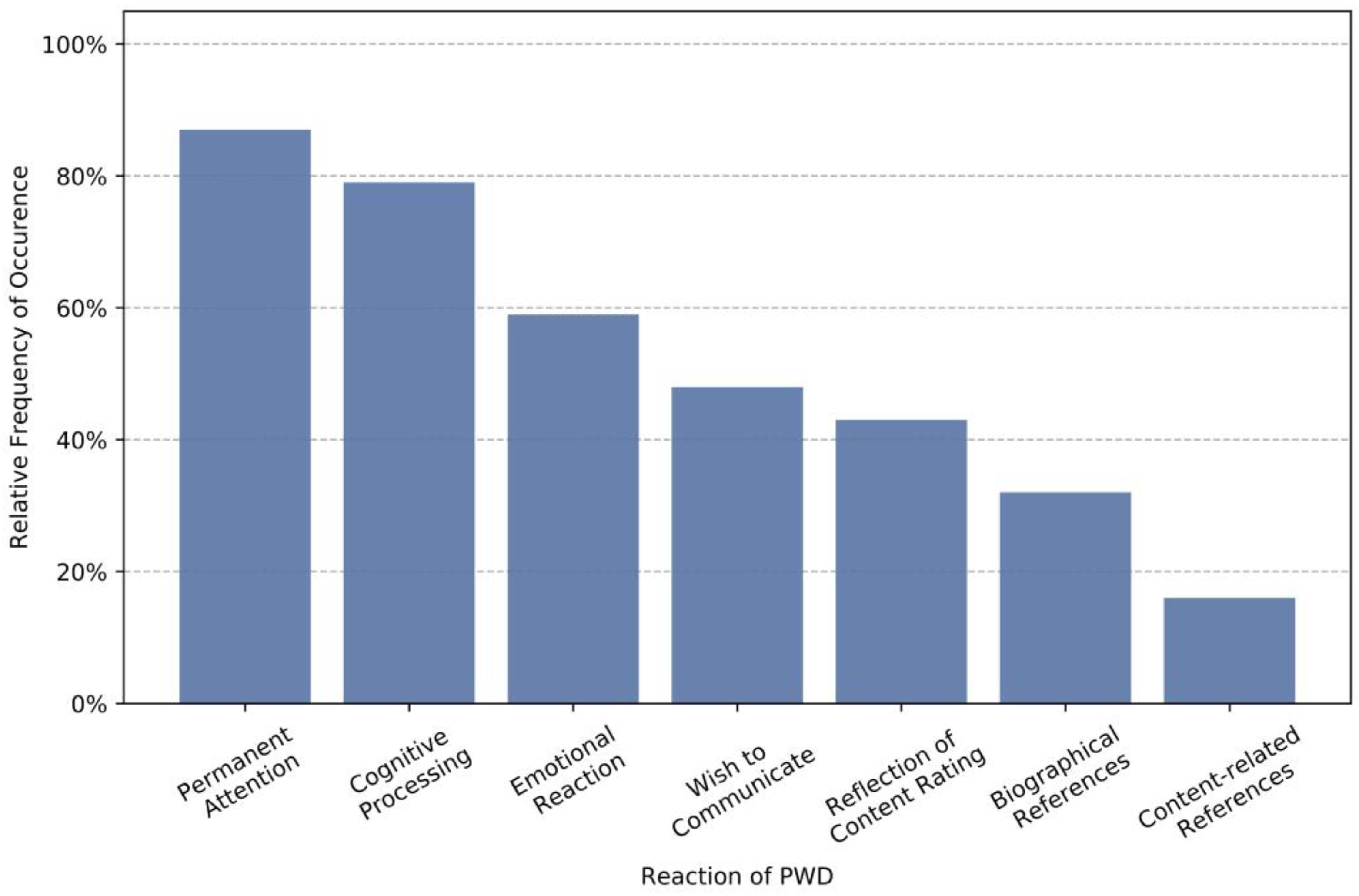
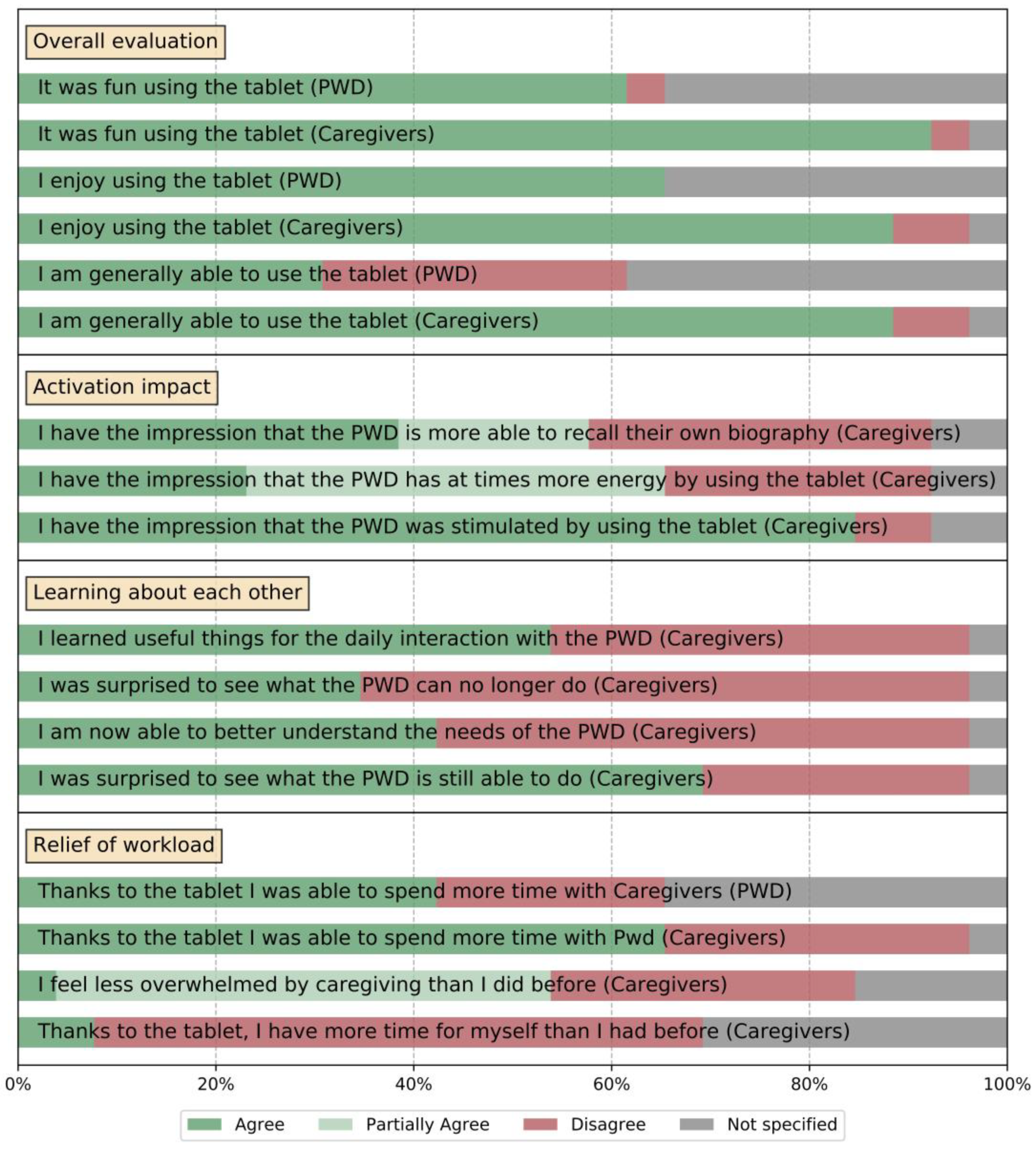
4.4. Questionnaire
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forsa-Umfrage ‘Angst vor Krankheiten’ im Auftrag der DAK. 2017. Available online: https://www.dak.de/dak/download/forsa-umfrage-1949432.pdf (accessed on 21 October 2018).
- Maust, D.T.; Solway, E.; Langa, K.M.; Kullgren, J.T.; Kirch, M.; Singer, D.C.; Malani, P. Perception of dementia risk and preventive actions among US adults aged 50 to 64 years. JAMA Neurol. 2020, 77, 259–262. [Google Scholar] [CrossRef] [PubMed]
- World Alzheimer Report. 2016. Available online: https://www.alz.co.uk/research/world-report-2016 (accessed on 30 April 2018).
- Ferri, C.P.; Prince, M.; Brayne, C.; Brodaty, H.; Fratiglioni, L.; Ganguli, M.; Hall, K.; Hasegawa, K.; Hendrie, H.; Huang, Y.; et al. Global prevalence of dementia: A Delphi consensus study. Lancet 2005, 366, 2112–2117. [Google Scholar] [CrossRef]
- Wimo, A.; Guerchet, M.; Ali, G.-C.; Wu, Y.-T.; Prina, A.M.; Winblad, B.; Jönsson, L.; Liu, Z.; Prince, M. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimers’ Dement. 2017, 13, 1–7. [Google Scholar] [CrossRef]
- Schultz, T.; Putze, F.; Kruse, A. (Eds.) Technische Unterstützung für Menschen mit Demenz: Symposium 30.09.-01.10.2013; KIT Scientific Publishing: Karlsruhe, Germany, 2014. [Google Scholar]
- Depner, A. Wie kann man das machen? Methodische und ethische Dimensionen partizipativer Ansätze zur Einbindung verschiedener Akteure in die Entwicklung technischer Aktivierungssysteme für Menschen mit Demenz. In Proceedings of the AAL Congress, Karlsruhe, Germany, 19–21 September 2018. [Google Scholar]
- Lohse, J.; Simon, C. Individuelle Aktivierung von Menschen mit Demenz—Tablet soll Freude und Neugier an neuer Technologie wecken. Alzheimeraktuell 2017, 3, 25. [Google Scholar]
- Kruse, A. Lebensphase hohes Alter: Verletzlichkeit und Reife; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Vernooij-Dassen, M.; Vasse, E.; Zuidema, S.; Cohen-Mansfield, J.; Moyle, W. Psychosocial interventions for dementia patients in long-term care. Int. Psychogeriatr. 2010, 22, 1121–1128. [Google Scholar] [CrossRef]
- Van Mierlo, L.; van der Roest, H.; Meiland, F.; Dröes, R. Personalized dementia care: Proven effectiveness of psychosocial interventions in subgroups. Ageing Res. Rev. 2010, 9, 163–183. [Google Scholar] [CrossRef]
- O’Connor, D.W.; Ames, D.; Gardner, B.; King, M. Psychosocial treatments of behavior symptoms in dementia: A systematic review of reports meeting quality standards. Int. Psychogeriatr. 2009, 21, 225–240. [Google Scholar] [CrossRef] [PubMed]
- García-Casal, J.A.; Loizeau, A.; Csipke, E.; Franco-Martín, M.; Perea-Bartolomé, M.V.; Orrell, M. Computer-based cognitive interventions for people living with dementia: A systematic literature review and meta-analysis. Aging Ment. Health 2017, 21, 454–467. [Google Scholar] [CrossRef] [PubMed]
- Bickel, C.; Pantel, J.; Eysenbach, K.; Schröder, J. Syntactic comprehension deficits in Alzheimer’s disease. Brain Lang. 2000, 71, 432–448. [Google Scholar] [CrossRef] [PubMed]
- Bucks, R.S.; Singh, S.; Cuerden, J.M.; Wilcock, G.K. Analysis of spontaneous, conversational speech in dementia of Alzheimer type: Evaluation of an objective technique for analysing lexical performance. Aphasiology 2000, 14, 71–91. [Google Scholar] [CrossRef]
- Weiner, J.; Schultz, T. Automatic screening for transition into dementia using speech. In Proceedings of the Speech Communication; 13th ITG-Symposium, Oldenburg, Germany, 10–12 October 2018; pp. 1–5. [Google Scholar]
- Seelye, A.M.; Schmitter-Edgecombe, M.; Cook, D.J.; Crandall, A. Naturalistic assessment of everyday activities and prompting technologies in mild cognitive impairment. J. Int. Neuropsychol. Soc. 2013, 19, 442–452. [Google Scholar] [CrossRef]
- Kuhlmann, A.; Reuter, V.; Schramek, R.; Dimitrov, T.; Görnig, M.; Matip, E.v.; Matthies, O.; Naroska, E. OurPuppet–Pflegeunterstützung mit einer interaktiven Puppe für pflegende Angehörige. Zeitschrift für Gerontologie und Geriatrie 2018, 51, 3–8. [Google Scholar] [CrossRef]
- Chang, Y.-J.; Tsai, S.-K.; Wang, T.-Y. A context aware handheld wayfinding system for individuals with cognitive impairments. In Proceedings of the 10th international ACM SIGACCESS conference on Computers and accessibility, Halifax, NS, Canada, 13–15 October 2008; pp. 27–34. [Google Scholar]
- Rehrl, T.; Troncy, R.; Bley, A.; Ihsen, S.; Scheibl, K.; Schneider, W.; Glende, S.; Goetze, S.; Kessler, J.; Hintermueller, C.; et al. The ambient adaptable living assistant is meeting its users. In Proceedings of the AAL Forum 2012-Eindhoven, Eindhoven, The Netherlands, 24–27 September 2012. [Google Scholar]
- Fasola, J.; Mataric, M.J. Using socially assistive human–robot interaction to motivate physical exercise for older adults. Proc. IEEE 2012, 100, 2512–2526. [Google Scholar] [CrossRef]
- Lin, J.J.; Mamykina, L.; Lindtner, S.; Delajoux, G.; Strub, H.B. Fish’n’Steps: Encouraging Physical Activity with an Interactive Computer Game. In Proceedings of the International Conference on Ubiquitous Computing, Orange County, CA, USA, 17–21 September 2006; pp. 261–278. [Google Scholar]
- Guhl, T.; Heuer, S.; Rosales, B.; Walther, S.; Schneider, J. Entwicklung eines Mobilitätsassistenten für Eingeschränkte Personen–Hintergrund, Status und Möglichkeiten der Kooperation; Schultz, T., Putze, F., Kruse, A., Hg., Eds.; Technische Unterstützung für Menschen mit Demenz; KIT Scientific Publishing: Karlsruhe, Germany, 2014; pp. 145–166. [Google Scholar]
- Dimitrov, T.; Kramps, O.; Ressel, C.; Könen, S.; Matthies, O.; Habibi, A.; Matip, E.M.; Polzehl, T.; Voigt-Antons, J.N.; Heutelbeck, D.; et al. “OurPuppet”–Entwicklung einer Mensch-Technik-Interaktion für die Unterstützung informell Pflegender. Zukunft der Pflege Tagungsband der 1. Clusterkonferenz 2018, 1, 78. [Google Scholar]
- Graf, B.; Reiser, U.; Hägele, M.; Mauz, K.; Klein, P. Robotic home assistant Care-O-bot® 3—product vision and innovation platform. In Proceedings of the 2009 IEEE Workshop on Advanced Robotics and its Social Impacts, Tokyo, Japan, 23–25 November 2009; pp. 139–144. [Google Scholar] [CrossRef]
- Gillespie, A.; Best, C.; O’Neill, B. Cognitive function and assistive technology for cognition: A systematic review. J. Int. Neuropsychol. Soc. 2012, 18, 1–19. [Google Scholar] [CrossRef]
- Crete-Nishihata, M.; Baecker, R.M.; Massimi, M.; Ptak, D.; Campigotto, R.; Kaufman, L.D.; Brickman, A.M.; Turner, G.R.; Steinerman, J.R.; Black, S.E. Reconstructing the past: Personal memory technologies are not just personal and not just for memory. Hum. Comput. Interact. 2012, 27, 92–123. [Google Scholar]
- Wada, K.; Shibata, T.; Musha, T.; Kimura, S. Robot therapy for elders affected by dementia. IEEE Eng. Med. Biol. Mag. 2008, 27, 53–60. [Google Scholar] [CrossRef]
- Media4Care: Das Tablet für Senioren, Menschen mit Demenz und ihre Betreuer. 2016. Available online: https://www.media4care.de (accessed on 28 April 2018).
- Tyack, C.; Camic, P.M.; Heron, M.J.; Hulbert, S. Viewing art on a tablet computer: A well-being intervention for people with dementia and their caregivers. J. Appl. Gerontol. 2017, 36, 864–894. [Google Scholar] [CrossRef]
- Bejan, A.; Gündogdu, R.; Butz, K.; Müller, N.; Kunze, C.; König, P. Using multimedia information and communication technology (ICT) to provide added value to reminiscence therapy for people with dementia. Zeitschrift für Gerontologie und Geriatrie 2018, 51, 9–15. [Google Scholar] [CrossRef]
- Ryan, A.A.; McCauley, C.O.; Laird, E.A.; Gibson, A.; Mulvenna, M.D.; Bond, R.; Bunting, B.; Curran, K.; Ferry, F. There is still so much inside’: The impact of personalised reminiscence, facilitated by a tablet device, on people living with mild to moderate dementia and their family carers. Dementia 2020, 19, 1131–1150. [Google Scholar] [CrossRef] [PubMed]
- Naini, K.D.; Kawase, R.; Kanhabua, N.; Niederée, C.; Altingovde, I.S. Those were the days: Learning to rank social media posts for reminiscence. Inf. Retr. J. 2019, 22, 159–187. [Google Scholar] [CrossRef]
- Foong, P.S.; Zhao, S.; Carlson, K.; Liu, Z. Vita: Towards supporting volunteer interactions with long-term care residents with dementia. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems 2017, Denver, CO, USA, 6–11 May 2017; pp. 6195–6207. [Google Scholar]
- Gilson, A.; Dodds, D.; Kaur, A.; Potteiger, M.; Ford, J., II. Using computer tablets to improve moods for older adults with dementia and interactions with their caregivers: Pilot intervention study. JMIR Form. Res. 2019, 3, e14530. [Google Scholar] [CrossRef] [PubMed]
- Westphal, B.J.; Lee, H.; Cheung, N.M.; Teo, C.G.; Leong, W.K. Experience of Designing and Deploying a Tablet Game for People with Dementia. In Proceedings of the 29th Australian Conference on Computer-Human Interaction, Brisbane, Australia, 1—28 December 2017; pp. 31–40. [Google Scholar]
- Nikitina, S.; Callaioli, S.; Baez, M. Smart conversational agents for reminiscence. In Proceedings of the 2018 IEEE/ACM 1st International Workshop on Software Engineering for Cognitive Services (SE4COG), Gothenburg, Sweden, 28–29 May 2018; pp. 52–57. [Google Scholar]
- Sas, C.; Davies, N.; Clinch, S.; Shaw, P.; Mikusz, M.; Steeds, M.; Nohrer, L. Supporting stimulation needs in dementia care through wall-sized displays. In Proceedings of the 2020 CHI Conference on Human Factors in Computing Systems, Honolulu, HI, USA, 25–30 April 2020; pp. 1–16. [Google Scholar]
- Huber, S.; Berner, R.; Uhlig, M.; Klein, P.; Hurtienne, J. Tangible objects for reminiscing in dementia care. In Proceedings of the Thirteenth International Conference on Tangible, Embedded, and Embodied Interaction, Stockholm, Sweden, 18–21 March 2019; pp. 15–24. [Google Scholar]
- Thoolen, M.; Brankaert, R.; Lu, Y. AmbientEcho: Exploring Interactive Media Experiences in the Context of Residential Dementia Care. In Proceedings of the 2020 ACM Designing Interactive Systems Conference 2020, Eindhoven, The Netherlands, 6–20 July 2020; pp. 1495–1508. [Google Scholar]
- Zafeiridi, P.; Paulson, K.; Dunn, R.; Wolverson, E.; White, C.; Thorpe, J.A. A web-based platform for people with memory problems and their caregivers (CAREGIVERSPRO-MMD): Mixed-methods evaluation of usability. JMIR Form. Res. 2018, 2, e4. [Google Scholar] [CrossRef]
- Hattink, B.; Droes, R.-M.; Sikkes, S.; Oostra, E.; Lemstra, A.W. Evaluation of the Digital Alzheimer Center: Testing usability and usefulness of an online portal for patients with dementia and their carers. JMIR Res. Protoc. 2016, 5, e144. [Google Scholar] [CrossRef]
- Torkamani, M.; McDonald, L.; Aguayo, I.S.; Kanios, C.; Katsanou, M.-N.; Madeley, L.; Limousin, P.D.; Lees, A.J.; Haritou, M.; Jahanshahi, M.; et al. A randomized controlled pilot study to evaluate a technology platform for the assisted living of people with dementia and their carers. J. Alzheimers’ Dis. 2014, 41, 515–523. [Google Scholar] [CrossRef]
- Astell, A.; Alm, N.; Gowans, G.; Ellis, M.; Dye, R.; Vaughan, P. Involving older people with dementia and their carers in designing computer based support systems: Some methodological considerations. Univers. Access Inf. Soc. 2009, 8, 49. [Google Scholar] [CrossRef]
- Löfqvist, C.; Nygren, C.; Széman, Z.; Iwarsson, S. Assistive devices among very old people in five European countries. Scand. J. Occup. Ther. 2005, 12, 181–192. [Google Scholar] [CrossRef]
- Salminen, A.-L.; Brandt, Å.; Samuelsson, K.; Töytäri, O.; Malmivaara, A. Mobility devices to promote activity and participation: A systematic review. J. Rehabil. Med. 2009, 41, 697–706. [Google Scholar] [CrossRef]
- Lauriks, S.; Reinersmann, A.; Van Der Roest, H.; Meiland, F.; Davies, R.; Moelaert, F.; Mulvenna, M.; Nugent, C.; Dröes, R. Review of ICT-based services for identified unmet needs in people with dementia. Ageing Res. Rev. 2007, 6, 223–246. [Google Scholar] [CrossRef] [PubMed]
- Schultz, T. I-CARE: Individual activation of people with dementia. In Proceedings of the 13th biannual conference of the German cognitive science society (KogWis 2016), Bremen, Germany, 26–30 September 2016; Proceedings (Hrsg: Barkowsky T). pp. 26–30. [Google Scholar]
- Gehrig, T.; Al-Halah, Z.; Ekenel, H.K.; Stiefelhagen, R. Action Unit Intensity Estimation Using Hierarchical Partial Least Squares. In Proceedings of the 2015 11th IEEE International Conference and Workshops on Automatic Face and Gesture Recognition (FG), Ljubljana, Slovenia, 4–8 May 2015; Volume 1, pp. 1–6. [Google Scholar]
- Fischer, M.; Ekenel, H.K.; Stiefelhagen, R. Person re-identification in tv series using robust face recognition and user feedback. Multimed. Tools Appl. 2011, 55, 83–104. [Google Scholar] [CrossRef]
- Richter, M.; Gehrig, T.; Ekenel, H.K. Facial Expression Classification on Web Images. In Proceedings of the 21st International Conference on Pattern Recognition (ICPR2012), Tsukuba, Japan, 11–15 November 2012; pp. 3517–3520. [Google Scholar]
- Ekman, P.; Friesen, W.V. Manual for the Facial Action Coding System; Consulting Psychologists Press: Palo Alto, CA, USA, 1978. [Google Scholar]
- Steinert, L.; Putze, F.; Küster, D.; Schultz, T. Towards Engagement Recognition of People with Dementia in Care Settings. In Proceedings of the 2020 International Conference on Multimodal Interaction, Utrecht, The Netherlands, 25–29 October 2020; pp. 558–565. [Google Scholar]
- Empatica Inc.—ISO 13485 Cert. No. 9124.EPTC. 2018. Available online: https://www.empatica.com/ (accessed on 25 October 2018).
- Jannach, D.; Zanker, M.; Felfernig, A.; Friedrich, G. Recommender Systems: An Introduction; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar]
- Liu, H.; Singh, P. ConceptNet—A practical commonsense reasoning tool-kit. Bt Technol. J. 2004, 22, 211–226. [Google Scholar] [CrossRef]
- Pröpper, R.; Putze, F.; Schultz, T. Jam: Java-Based Associative Memory. In Proceedings of the Paralinguistic Information and its Integration in Spoken Dialogue Systems Workshop, Granada, Spain; Springer: New York, NY, USA, 2011; pp. 143–155. [Google Scholar]
- Doneit, W.; Lohse, J.; Glesing, K.; Simon, C.; Fischer, M.; Depner, A.; Kruse, A.; Franz, I.; Schultz, T.; Putze, F.; et al. Data-driven analysis of interactions between people with dementia and a tablet device. Curr. Dir. Biomed. Eng. 2017, 3, 735–738. [Google Scholar] [CrossRef][Green Version]
- Mikut, R.; Bartschat, A.; Doneit, W.; Ordiano, J.Á.; Schott, B.; Stegmaier, J.; Waczowicz, S.; Reischl, M. The MATLAB toolbox SciXMiner: User’s manual and programmer’s guide. arXiv 2017, arXiv:1704.03298. [Google Scholar]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schultz, T.; Putze, F.; Steinert, L.; Mikut, R.; Depner, A.; Kruse, A.; Franz, I.; Gaerte, P.; Dimitrov, T.; Gehrig, T.; et al. I-CARE-An Interaction System for the Individual Activation of People with Dementia. Geriatrics 2021, 6, 51. https://doi.org/10.3390/geriatrics6020051
Schultz T, Putze F, Steinert L, Mikut R, Depner A, Kruse A, Franz I, Gaerte P, Dimitrov T, Gehrig T, et al. I-CARE-An Interaction System for the Individual Activation of People with Dementia. Geriatrics. 2021; 6(2):51. https://doi.org/10.3390/geriatrics6020051
Chicago/Turabian StyleSchultz, Tanja, Felix Putze, Lars Steinert, Ralf Mikut, Anamaria Depner, Andreas Kruse, Ingo Franz, Philipp Gaerte, Todor Dimitrov, Tobias Gehrig, and et al. 2021. "I-CARE-An Interaction System for the Individual Activation of People with Dementia" Geriatrics 6, no. 2: 51. https://doi.org/10.3390/geriatrics6020051
APA StyleSchultz, T., Putze, F., Steinert, L., Mikut, R., Depner, A., Kruse, A., Franz, I., Gaerte, P., Dimitrov, T., Gehrig, T., Lohse, J., & Simon, C. (2021). I-CARE-An Interaction System for the Individual Activation of People with Dementia. Geriatrics, 6(2), 51. https://doi.org/10.3390/geriatrics6020051