
Assessment of Drivers with Alzheimer’s Disease in High Demand Driving Situations: Coping with Intersections in a Driving Simulator

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
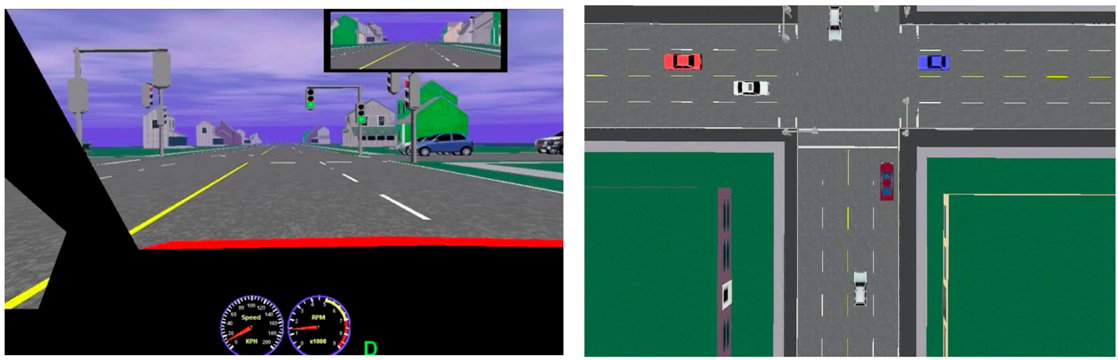
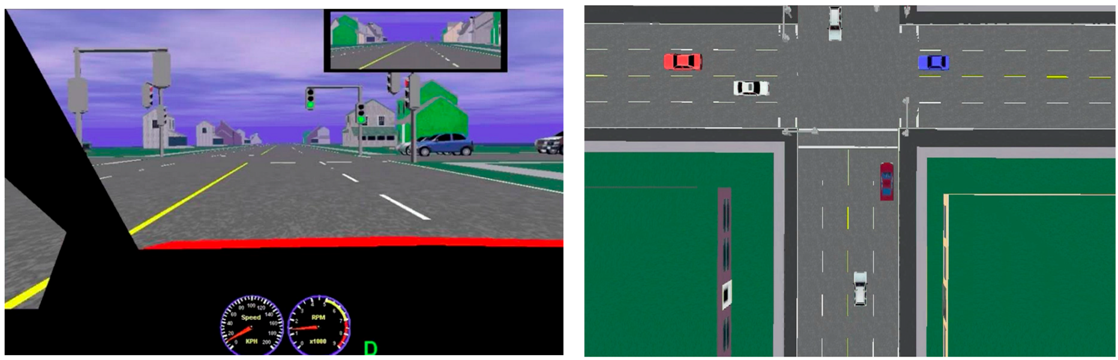
2.2. Driving Simulator
2.3. Driving Errors Evaluation Scheme
2.4. Procedure
2.5. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Preparation Errors
3.3. Execution Errors
3.4. Recovery Errors
3.5. Initiation Errors and Crashes
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix

{kind=link}
| Errors | Definition | Nature |
|---|---|---|
| Initiation errors | All errors prevent adequate analysis of the intersection. | |
| Omission | Does not respect the verbal command. | |
| Requested turn not executed | The participant continues straight, omitting the requested turn | Judgement |
| Unrequested turn executed | The participant turns to the right or left, although they were requested to continue going straight. | Judgement |
| Opposite turn executed | The participant executes a turn in the opposite direction of what was requested. | Judgement |
| Vehicle control | The position of the vehicle before the intersection makes it impossible for the participant to complete the request. | |
| Driving in the opposite direction | The participant drives in the left lane into oncoming traffic | Judgement |
| Driving on the shoulder | The participant follows the road, but driving on the shoulder of the road, preventing the participant from accomplishing the turn. | Judgement |
| Driving off the road | The participant drifts from the road and continues on the grass in another direction. | Judgement |
| Crash | Simulator displays noise and image of crash. | |
| Frequency of crash | Note the frequency of crash and at which intersection they occur | |
| Before the Intersection | All errors made before the stop line of the intersection | |
| Brakes and speed | ||
| No use of brakes | The participant attempts to execute the command to turn without the use of the brakes, or does not slow down at all before the turn, or a yellow light. | Attention |
| Braking | Participant uses brakes too late to execute a turn or avoid an obstacle (results in a sound on the simulator). | Judgement |
| Exceeding speed limit by 5 km/h to 15 km/h | Exceeding the speed limit by 5 to 15 km/h. Worth one error point on the evaluation scheme. | Judgement |
| Exceeding speed limit by more than 15 km/h | Exceeding the speed limit by more than 15 km/h. Worth two error points on the evaluation scheme. | Judgement |
| Inappropriate stops | All stops which are not due to a signal, mark on the ground, or obstacle are inappropriate | |
| Excessive preparation | Slowing down right after the command, where the driving speed is less than half the speed limit for a significant distance, but without locking the wheels. | Judgement |
| Frequency of inappropriate stops after the verbal command | Note the number of inappropriate stops after the verbal command. | Judgement |
| Exceeding the stop line | In the case where a signal demands a stop, the participant stops the vehicle after already passing the stop line. | Coordination |
| Choice of lane | ||
| Lane deviation | A deviation occurs when at least one of the front wheels is in the neighbouring lane (left or right). | Coordination |
| Wrong lane | After a command to turn, the participant does not change lanes or stay in the correct lane to be in an adequate position to complete the correct turn (right lane for a right turn, left lane for a left turn). | Judgement |
| Shoulder lane | The participant drives on the shoulder lane but is still able to complete the correct turn | Perceptual |
| Signaling | ||
| Disobeying signal | Action does not correspond to the signal. | Attention |
| Safety | ||
| Follows too closely | The participant follows the preceding vehicle too closely, putting the driver at a high risk of crash. If the participant’s view did not show the wheels of the vehicle in front of them, the following distance was considered too close. | Judgement |
| Right of way not given to pedestrian | The participant does not give right of way to the pedestrian. | Attention |
| During the intersection | Between the stop line of the participant, and that of the drivers going in the opposite direction. | |
| Vehicle control | ||
| Excessive stopping and anticipation for a turn to the right | Very long stop at the stop line without any apparent reason, even though the light is green. A stop was considered too long when there was no apparent reason why the participant should be waiting any longer to engage in the turn. | Judgement |
| Very slow execution | Unnecessary braking during the execution of the intersection. A slow execution occurred when there was no apparent reason for participants to use brakes during a turn. | Attention and coordination |
| Incapable of controlling the vehicle | Loss of control of the vehicle, including inappropriate use of the steering wheel (i.e., participant did not orient the car directly towards the destined road), accelerator (i.e., unnecessary variation of speed during execution), and lane deviations. | Coordination |
| Left turn | ||
| Vehicle is an obstruction in the intersection. | When waiting in the middle of the intersection for space to turn left, the vehicle obstructs the lane going in the other direction. | Judgement |
| Insufficient time to complete turn | The participant does not have enough space to complete the turn, resulting in a crash. | Attention, perceptual and judgement |
| Missed turn | Space is available to carry out the left turn, but is not chosen. | Judgement |
| Traffic light | ||
| Disobeying traffic light | Enters the intersection at an inadequate moment and disobeys traffic light. | Attention |
| After the intersection | The vehicle leaves the intersection marked by a white line on the ground, and up to 30 m afterwards | |
| Speed | ||
| Speed remains constant | Does not increase speed after a successful turn. | Judgement |
| Excessive braking | Does not increase speed after a successful turn, and is using the brakes unnecessarily. | Judgement |
| Stopping | ||
| Unnecessary stop after the intersection. | Unnecessary stop once the intersection is completed. | Judgement |
| Vehicle orientation | ||
| Wrong orientation | Unable to return the vehicle to a correct position, even though the initiation was not problematic. | Coordination |
| Loss of control | The participant orients the vehicle on the shoulder, or in the opposite lane (left), without immediate correction of the situation. | Coordination |
References
- Dickerson, A.E. Driving and Community Mobility as an Instrumental Activity of Daily Living. In Stroke Rehabilitation, 4th ed.; Gillen, G., Ed.; Elsevier Publishing: St. Louis, MO, USA, 2015; pp. 237–264. [Google Scholar]
- Carr, D.B.; O’Neill, D. Mobility and safety issues in drivers with dementia. Int. Psychogeriatr. 2015, 27, 1613–1622. [Google Scholar] [CrossRef] [PubMed]
- Bédard, M.; Leonard, E.; McAuliffe, J.; Weaver, B.; Gibbons, C.; Dubois, S. Visual attention and older drivers: The contribution of inhibition of return to safe driving. Exp. Aging Res. 2006, 32, 119–135. [Google Scholar] [CrossRef] [PubMed]
- Trick, L.M.; Enns, J.T.; Mills, J.; Vavrik, J. Paying attention behind the wheel: A framework for studying the role of attention in driving. Theor. Issues Ergon. Sci. 2004, 5, 385–424. [Google Scholar] [CrossRef]
- Freund, B.; Szinovacz, M. Effects of cognition on driving involvement among the oldest old: Variations by gender and alternative transportation opportunities. Gerontologist 2002, 42, 621–633. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.C. The role of reduced fitness to drive due to medical impairments in explaining crashes involving older drivers. Traffic Inj. Prev. 2008, 9, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Spannhorst, S.; Toepper, M.; Schulz, P.; Wenzel, G.; Driessen, M.; Kreisel, S. Advice for Elderly Drivers in a German Memory Clinic: A Case Report on Medical, Ethical and Legal Consequences. Geriatrics 2016, 1, 9. [Google Scholar] [CrossRef]
- Jang, R.W.; Man-Son-Hing, M.; Molnar, F.J.; Hogan, D.B.; Marshall, S.C.; Auger, J.; Graham, I.D.; Korner-Bitensky, N.; Tomlinson, G.; Kowgier, M.E.; et al. Family physicians’ attitudes and practices regarding assessments of medical fitness to drive in older persons. J. Gen. Intern. Med. 2007, 22, 531–543. [Google Scholar] [CrossRef] [PubMed]
- Crizzle, A.M.; Classen, S.; Bédard, M.; Lanford, D.; Winter, S. MMSE as a predictor of on-road driving performance in community dwelling older drivers. Accid. Anal. Prev. 2012, 49, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Esser, P.; Dent, S.; Jones, C.; Sheridan, B.J.; Bradley, A.; Wade, D.T.; Dawes, H. Utility of the MOCA as a cognitive predictor for fitness to drive. J. Neurol. Neurosurg. Psychiatry 2016, 87, 567–568. [Google Scholar] [CrossRef] [PubMed]
- Lovas, J.; Fereshtehnejad, S.M.; Cermakova, P.; Lundberg, C.; Johansson, B.; Johansson, K.; Winblad, B.; Eriksdotter, M.; Religa, D. Assessment and Reporting of Driving Fitness in Patients with Dementia in Clinical Practice: Data from SveDem, the Swedish Dementia Registry. J. Alzheimer’s Dis. 2016, 53, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Stinchcombe, A.; Odenheimer, G.L.; Bédard, M. Managing Safety and Mobility Needs of Older Drivers. In Psychology and Geriatrics: Integrated Care for an Aging Nation; Academic Press: Cambridge, MA, USA, 2015; pp. 135–152. [Google Scholar]
- Bédard, M.; Marshall, S.; Man-Son-Hing, M.; Weaver, B.; Gélinas, I.; Korner-Bitensky, N.; Mazer, B.; Naglie, G.; Porter, M.M.; Rapoport, M.J.; et al. It is premature to test older drivers with the SIMARD-MD. Accid. Anal. Prev. 2013, 61, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Bédard, M.; Weaver, B.; Darzins, P.; Porter, M.M. Predicting driving performance in older adults: We are not there yet! Traffic Inj. Prev. 2008, 9, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Yamin, S.; Stinchcombe, A.; Gagnon, S. Deficits in Attention and Visual Processing but not Global Cognition Predict Simulated Driving Errors in Drivers Diagnosed with Mild Alzheimer’s Disease. Am. J. Alzheimer’s Dis. Other Dement. 2016, 31, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Perry, R.J.; Watson, P.; Hodges, J.R. The nature and staging of attention dysfunction in early (minimal and mild) Alzheimer’s disease: Relationship to episodic and semantic memory impairment. Neuropsychologia 2000, 38, 252–271. [Google Scholar] [CrossRef]
- Werneke, J.; Vollrath, M. What does the driver look at? The influence of intersection characteristics on attention allocation and driving behavior. Accid. Anal. Prev. 2012, 45, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Aksan, N.; Anderson, S.W.; Dawson, J.; Uc, E.; Rizzo, M. Cognitive functioning differentially predicts different dimensions of older drivers’ on-road safety. Accid. Anal. Prev. 2015, 75, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Stinchcombe, A.; Gagnon, S.; Zhang, J.J.; Montembeault, P.; Bédard, M. Fluctuating attentional demand in a simulated driving assessment: The roles of age and driving complexity. Traffic Inj. Prev. 2011, 2, 576–587. [Google Scholar] [CrossRef] [PubMed]
- Stanton, N.A.; Salmon, P.M. Human error taxonomies applied to driving: A generic driver error taxonomy and its implications for intelligent transport systems. Saf. Sci. 2009, 47, 227–237. [Google Scholar] [CrossRef]
- Vlahodimitrakou, Z.; Charlton, J.L.; Langford, J.; Koppel, S.; Di Stefano, M.; Macdonald, W.; Mazer, B.; Gélinas, I.; Vrkljan, B.; Porter, M.M.; et al. Development and evaluation of a Driving Observation Schedule (DOS) to study everyday driving performance of older drivers. Accid. Anal. Prev. 2013, 61, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Reisberg, B.; Ferris, S.H.; De Leon, M.J.; Crook, T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am. J. Psychiatry 1982, 139, 1136–1138. [Google Scholar] [PubMed]
- Folstein, M.; Folstein, S.; McHugh, P. Mini-Mental State: A practical method for grading the cognitive state of patients for the clinicians. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Crum, R.M.; Anthony, J.C.; Bassett, S.S.; Folstein, M.F. Population-based norms for the Mini-Mental State Examination by age and educational level. JAMA 1993, 269, 2386–2391. [Google Scholar] [CrossRef] [PubMed]
- Bédard, M.; Parkkari, M.; Weaver, B.; Riendeau, J.; Dahlquist, M. Assessment of driving performance using a simulator protocol: Validity and reproducibility. Am. J. Occup. Ther. 2010, 64, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, M.; McGehee, D.V.; Dawson, J.D.; Anderson, S.N. Simulated car crashes at intersections with drivers with Alzheimer Disease. Alzheimer Dis. Assoc. Disord. 2001, 15, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Casutt, G.; Theill, N.; Martin, M.; Keller, M.; Jancke, L. The drive-wise project: Driving simulator training increases real driving performance in healthy older drivers. Front. Aging Neurosci. 2014, 6, 85. [Google Scholar] [CrossRef] [PubMed]
| Errors | Mean AD | SD AD | Mean Control | SD Control | t | df | p |
|---|---|---|---|---|---|---|---|
| Brakes and speed | |||||||
| No use of brakes | 1.500 | 1.146 | 0.262 | 0.490 | 4.482 | 36 | <0.001 |
| Braking | 8.824 | 7.462 | 3.000 | 3.021 | 3.269 | 36 | 0.002 |
| Exceeding speed limit by 5 km/h to 15 km /h | 10.529 | 4.605 | 5.143 | 3.870 | 3.919 | 36 | <0.001 |
| Exceeding speed limit by more than 15 km/h | 7.500 | 4.822 | 2.000 | 2.225 | 4.661 | 36 | <0.001 |
| Inappropriate stop | |||||||
| Excessive preparation | 6.912 | 6.129 | 5.714 | 5.083 | 0.659 | 36 | 0.514 |
| Frequency of inappropriate stops after the verbal command | 11.176 | 8.107 | 6.548 | 4.022 | 2.296 | 36 | 0.028 |
| Exceeding the stop line | 0.500 | 0.685 | 0.429 | 0.482 | 0.377 | 36 | 0.708 |
| Choice of lane | |||||||
| Lane deviation | 14.059 | 8.624 | 7.405 | 7.144 | 2.603 | 36 | 0.013 |
| Wrong lane | 1.735 | 1.786 | 0.524 | 1.054 | 2.602 | 36 | 0.013 |
| Shoulder lane | 0.441 | 0.704 | 0.000 | 0.000 | 2.879 | 36 | 0.007 |
| Signaling | |||||||
| Disobeying signal | 4.147 | 2.720 | 2.357 | 2.393 | 2.157 | 36 | 0.038 |
| Safety | |||||||
| Follows too closely | 0.353 | 0.702 | 0.190 | 0.512 | 0.825 | 36 | 0.415 |
| Right of way not given to pedestrian | 0.000 | 0.000 | 0.024 | 0.109 | −0.897 | 36 | 0.375 |
| Errors | Mean AD | SD AD | Mean Control | SD Control | t | df | p |
|---|---|---|---|---|---|---|---|
| Vehicle control | |||||||
| Excessive stopping and anticipation for a right turn | 0.324 | 0.611 | 0.857 | 1.415 | 0.019 | 36 | 0.157 |
| Very slow execution | 1.706 | 2.100 | 2.310 | 2.052 | −0.892 | 36 | 0.378 |
| Incapable of controlling the vehicle | 3.324 | 2.639 | 0.643 | 1.002 | 4.298 | 36 | <0.001 |
| Left turn | |||||||
| Vehicle is an obstruction in the intersection. | 0.471 | 0.624 | 0.238 | 0.407 | 1.384 | 36 | 0.175 |
| Insufficient time to complete turn | 0.059 | 0.166 | 0.000 | 0.000 | 1.629 | 36 | 0.112 |
| Missed turn | 0.118 | 0.281 | 0.238 | 0.375 | −1.097 | 36 | 0.280 |
| Traffic light | |||||||
| Disobeying signal | 2.412 | 1.593 | 1.333 | 1.099 | 2.464 | 36 | 0.019 |
| Errors | Mean AD | SD AD | Mean Control | SD Control | t | df | p |
|---|---|---|---|---|---|---|---|
| Speed | |||||||
| Speed remains constant | 1.118 | 0.781 | 0.810 | 0.661 | 1.317 | 36 | 0.196 |
| Stopping | |||||||
| Unnecessary stop after the intersection | 0.206 | 0.532 | 0.143 | 0.359 | 0.435 | 36 | 0.666 |
| Vehicle orientation | |||||||
| Wrong orientation | 4.353 | 2.377 | 3.262 | 1.758 | 1.626 | 36 | 0.113 |
| Loss of control | 2.147 | 2.269 | 0.786 | 1.168 | 2.391 | 36 | 0.022 |
| Errors | Mean AD | SD AD | Mean Control | SD Control | t | df | p |
|---|---|---|---|---|---|---|---|
| Initiation errors | |||||||
| Omission | 1.588 | 1.121 | 0.357 | 0.761 | 4.022 | 36 | <0.001 |
| Requested turn not executed | 1.529 | 1.125 | 0.286 | 0.644 | 4.283 | 36 | <0.001 |
| Opposite turn executed | 0.059 | 0.243 | 0.071 | 0.239 | −0.161 | 36 | 0.873 |
| Vehicle control | 1.735 | 2.768 | 0.095 | 0.201 | 2.716 | 36 | 0.010 |
| Driving in the opposite direction | 0.765 | 1.276 | 0.048 | 0.150 | 2.561 | 36 | 0.015 |
| Driving on the shoulder | 0.147 | 0.386 | 0.048 | 0.150 | 1.086 | 36 | 0.285 |
| Driving off the road | 0.824 | 1.600 | 0.000 | 0.000 | 2.366 | 36 | 0.023 |
| Crash | |||||||
| Frequency of crash | 3.265 | 2.641 | 0.952 | 1.036 | 3.687 | 36 | 0.001 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stinchcombe, A.; Paquet, S.; Yamin, S.; Gagnon, S. Assessment of Drivers with Alzheimer’s Disease in High Demand Driving Situations: Coping with Intersections in a Driving Simulator. Geriatrics 2016, 1, 21. https://doi.org/10.3390/geriatrics1030021
Stinchcombe A, Paquet S, Yamin S, Gagnon S. Assessment of Drivers with Alzheimer’s Disease in High Demand Driving Situations: Coping with Intersections in a Driving Simulator. Geriatrics. 2016; 1(3):21. https://doi.org/10.3390/geriatrics1030021
Chicago/Turabian StyleStinchcombe, Arne, Stephanie Paquet, Stephanie Yamin, and Sylvain Gagnon. 2016. "Assessment of Drivers with Alzheimer’s Disease in High Demand Driving Situations: Coping with Intersections in a Driving Simulator" Geriatrics 1, no. 3: 21. https://doi.org/10.3390/geriatrics1030021
APA StyleStinchcombe, A., Paquet, S., Yamin, S., & Gagnon, S. (2016). Assessment of Drivers with Alzheimer’s Disease in High Demand Driving Situations: Coping with Intersections in a Driving Simulator. Geriatrics, 1(3), 21. https://doi.org/10.3390/geriatrics1030021