
Six-Month Patency of Long Carotid Bypass Grafts Constructed with In-Body Tissue Architecture-Induced Small-Diameter Biotubes in a Goat Model

 , , , ,
, , , ,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
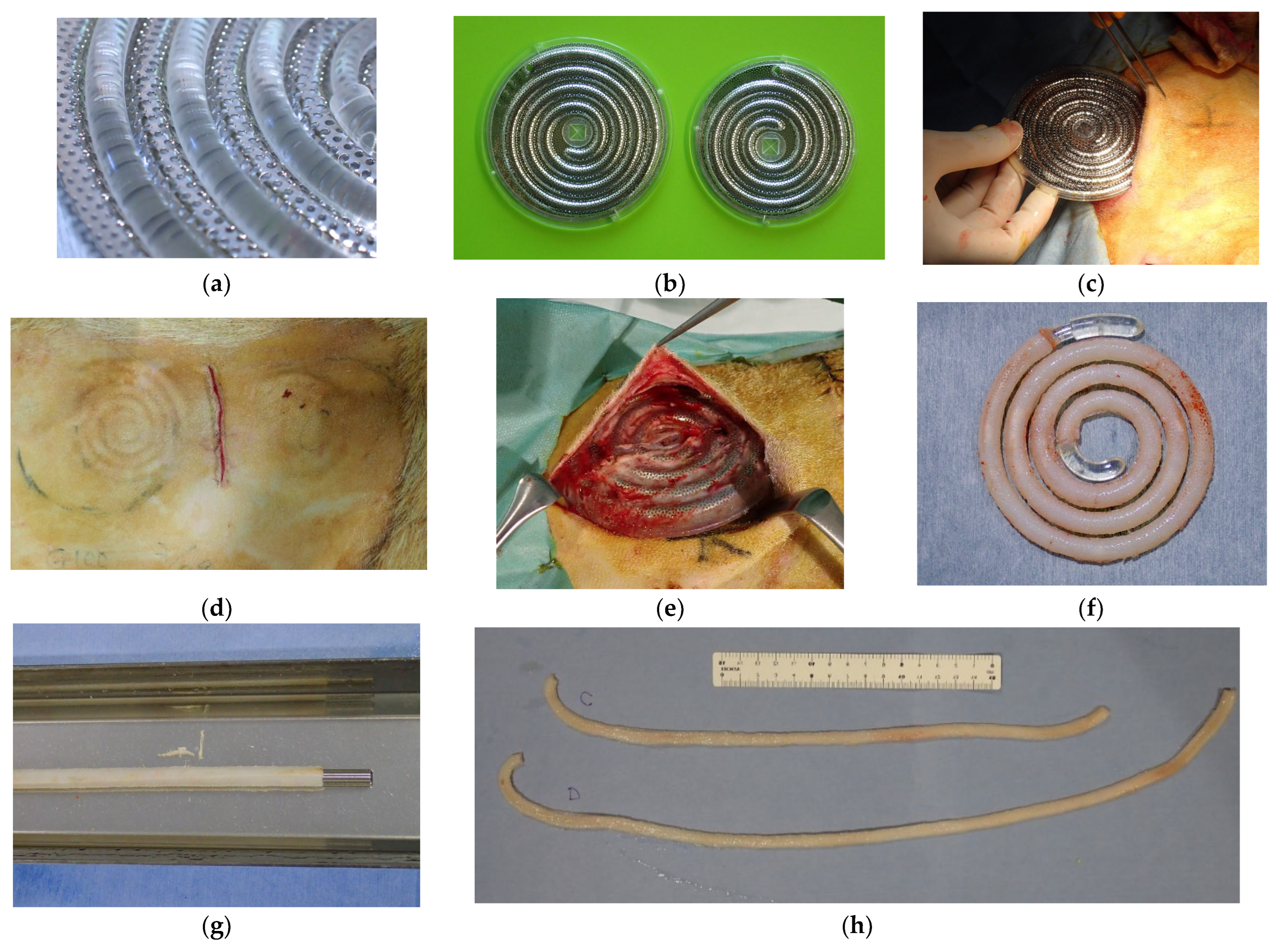
2.1. Preparation of Biotubes
2.2. Bypass Procedures
2.3. Histological Examination
2.4. Ethical Approval
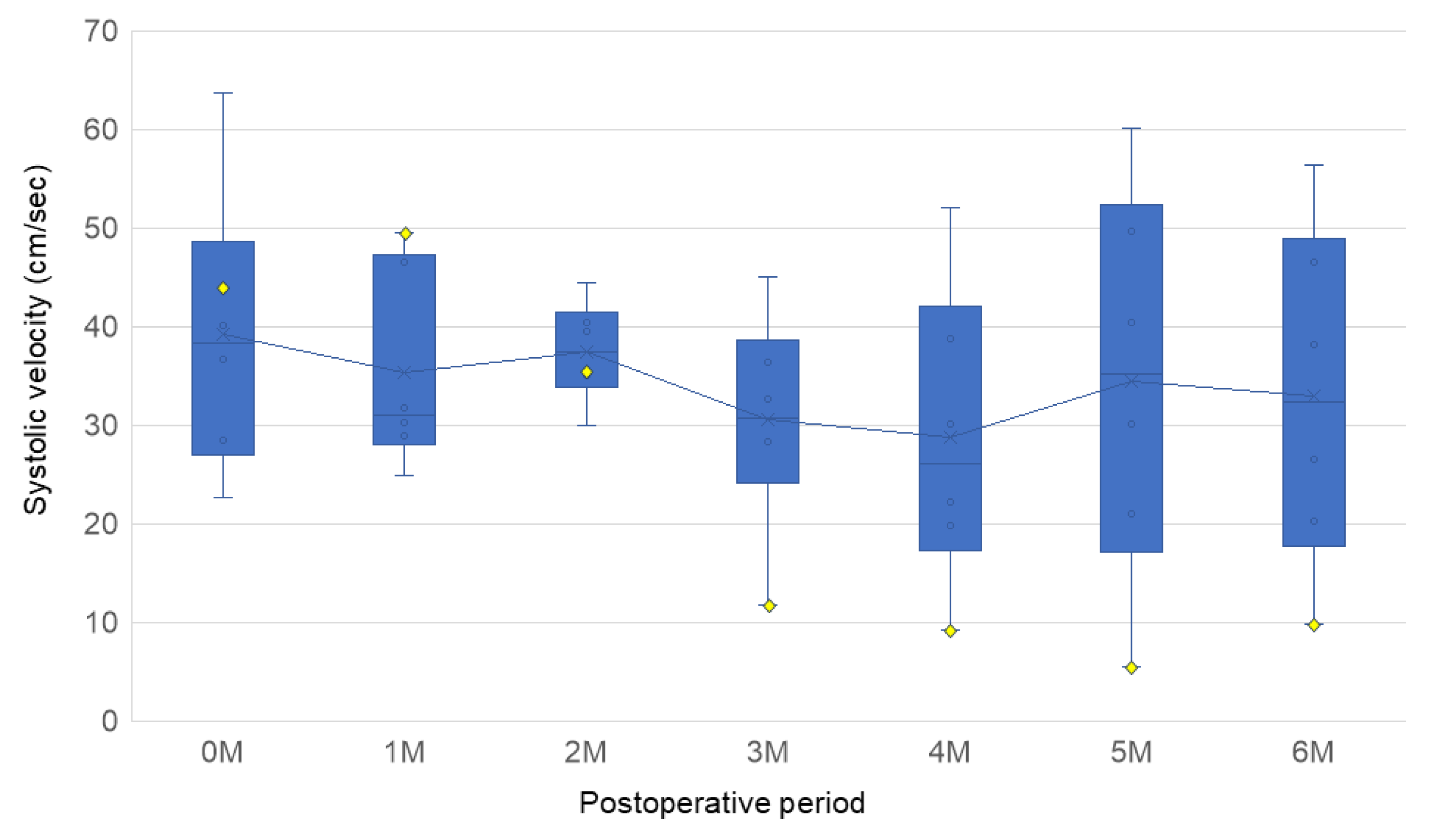
2.5. Statistical Analysis
3. Results
3.1. Biotube Production
3.2. Bypass Procedure
3.3. Histological Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PAD | Peripheral artery disease |
| CLI | Critical limb ischemia |
| TEVG | Tissue-engineered vascular graft |
| iBTA | In-body tissue architecture |
| ACT | Activated clotting time |
| CT | Computed tomography |
| α-SMA | α-smooth muscle actin |
References
- Majmundar, M.; Patel, K.N.; Doshi, R.; Mehta, H.; Vindhyal, M.R.; Hance, K.A.; Ali, A.; Gupta, K. Prognostic value of hospital frailty risk score and clinical outcomes in patients undergoing revascularization for critical limb-threatening ischemia. J. Am. Heart Assoc. 2023, 12, e030294. [Google Scholar] [CrossRef] [PubMed]
- Levin, S.R.; Arinze, N.; Siracuse, J.J. Lower extremity critical limb ischemia: A review of clinical features and management. Trends Cardiovasc. Med. 2020, 30, 125–130. [Google Scholar] [CrossRef]
- Kohler, C.; Gaizauskaite, K.; Kotopoulos, K.; Kotelis, D.; Schmidli, J.; Makaloski, V.; Weiss, S. Amputation-free survival, WiFi stage, and GLASS classifications in distal crural or pedal bypass for chronic limb-threatening ischemia. J. Clin. Med. 2024, 13, 6649. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, A.W.; Adam, D.J.; Bell, J.; Forbes, J.F.; Fowkes, F.G.; Gillespie, I.; Ruckley, C.V.; Raab, G.M. BASIL trial participants. bypass versus angioplasty in severe ischaemia of the leg (BASIL) trial: Analysis of amputation free and overall survival by treatment received. J. Vasc. Surg. 2010, 51, 18S–31S. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Sud, K.; Shishehbor, M.H. Nationwide trends of hospital admission and outcomes among critical limb ischemia patients: From 2003–2011. J Am Coll Cardiol 2016, 67, 1901–1913. [Google Scholar] [CrossRef]
- Almasri, J.; Adusumalli, J.; Asi, N.; Lakis, S.; Alsawas, M.; Prokop, L.J.; Bradbury, A.; Kolh, P.; Conte, M.S.; Murad, M.H. A systematic review and meta-analysis of revascularization outcomes of infrainguinal chronic limb-threatening ischemia. J. Vasc. Surg. 2019, 69, 126S–136S. [Google Scholar] [CrossRef]
- Conte, M.S.; Azene, E.; Doros, G.; Gasper, W.J.; Hamza, T.; Kashyap, V.S.; Guzman, R.; Mena-Hurtado, C.; Menard, M.T.; Rosenfield, K.; et al. Secondary interventions following open vs endovascular revascularization for chronic limb threatening ischemia in the BEST-CLI trial. J. Vasc. Surg. 2024, 79, 1428–1437.e4. [Google Scholar] [CrossRef]
- Lin, A.; King, E.G. Alternative conduits for lower extremity bypass. Ann. Vasc. Surg. 2024, 107, 122–126. [Google Scholar] [CrossRef]
- Hamouda, M.; Zarrintan, S.; Vootukuru, N.; Thandra, S.; Quatromoni, J.G.; Malas, M.B.; Gaffey, A.C. Outcomes of prosthetic and biological grafts compared to arm vein grafts in patients with chronic limb-threatening ischemia. J. Vasc. Surg. 2024, 81, 682–692. [Google Scholar] [CrossRef]
- Pereira, C.E.; Albers, M.; Romiti, M.; Brochado-Neto, F.C.; Pereira, C.A. Meta-analysis of femoropopliteal bypass grafts for lower extremity arterial insufficiency. J. Vasc. Surg. 2006, 44, 510–517. [Google Scholar] [CrossRef]
- Rychlik, I.J.; Davey, P.; Murphy, J.; O’Donnell, M.E. A meta-analysis to compare Dacron versus polytetrafluroethylene grafts for above-knee femoropopliteal artery bypass. J. Vasc. Surg. 2014, 60, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Kitsuka, T.; Hama, R.; Ulziibayar, A.; Matsuzaki, Y.; Kelly, J.; Shinoka, T. Clinical application for tissue engineering focused on materials. Biomedicines 2022, 10, 1439. [Google Scholar] [CrossRef]
- Durán-Rey, D.; Crisóstomo, V.; Sánchez-Margallo, J.A.; Sánchez-Margallo, F.M. Systematic review of tissue-engineered vascular grafts. Front. Bioeng. Biotechnol. 2021, 9, 771400. [Google Scholar] [CrossRef] [PubMed]
- Fang, S.; Ellman, D.G.; Andersen, D.C. Review: Tissue engineering of small-diameter vascular grafts and their in vivo evaluation in large animals and humans. Cells 2021, 10, 713. [Google Scholar] [CrossRef]
- Gutowski, P.; Gage, S.M.; Guziewicz, M.; Ilzecki, M.; Kazimierczak, A.; Kirkton, R.D.; Niklason, L.E.; Pilgrim, A.; Prichard, H.L.; Przywara, S.; et al. Arterial reconstruction with human bioengineered acellular blood vessels in patients with peripheral arterial disease. J. Vasc. Surg. 2020, 72, 1247–1258. [Google Scholar] [CrossRef] [PubMed]
- Skovrind, I.; Harvald, E.B.; Juul Belling, H.; Jørgensen, C.D.; Lindholt, J.S.; Andersen, D.C. Concise Review: Patency of small-diameter tissue-engineered vascular grafts: A meta-analysis of preclinical trials. Stem Cells Transl. Med. 2019, 8, 671–680. [Google Scholar] [CrossRef]
- Nakayama, Y.; Iwai, R.; Terazawa, T.; Tajikawa, T.; Umeno, T.; Kawashima, T.; Nakashima, Y.; Shiraishi, Y.; Yamada, A.; Higashita, R.; et al. Pre-implantation evaluation of a small-diameter.; long vascular graft (Biotube®) for below-knee bypass surgery in goats. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 2387–2398. [Google Scholar] [CrossRef]
- Umeno, T.; Mori, K.; Iwai, R.; Kawashima, T.; Shuto, T.; Nakashima, Y.; Tajikawa, T.; Nakayama, Y.; Miyamoto, S. Carotid artery bypass surgery of in-body tissue architecture-induced small-diameter biotube in a goat model: A pilot study. Bioengineering 2024, 11, 203. [Google Scholar] [CrossRef]
- Mori, K.; Umeno, T.; Kawashima, T.; Wada, T.; Genda, T.; Arakura, M.; Oda, Y.; Mizoguchi, T.; Iwai, R.; Tajikawa, T.; et al. Breaking the limit of cardiovascular regenerative medicine: Successful 6-Month goat implant in world’s first ascending aortic replacement using biotube blood vessels. Bioengineering 2024, 11, 405. [Google Scholar] [CrossRef]
- ISO 7198:2016; Cardiovascular Implants And Extracorporeal Systems—Vascular Prostheses—Tubular Vascular Grafts and Vascular Patches. International Organization for Standardization: Geneva, Switzerland, 2016.
- Kawashima, T.; Umeno, T.; Terazawa, T.; Wada, T.; Shuto, T.; Nishida, H.; Anai, H.; Nakayama, Y.; Miyamoto, S. Aortic valve neocuspidization with in-body tissue-engineered autologous membranes: Preliminary results in a long-term goat model. Interact. Cardiovasc. Thorac. Surg. 2021, 32, 969–977. [Google Scholar] [CrossRef]
- Tajikawa, T.; Sekido, Y.; Mori, K.; Kawashima, T.; Nakashima, Y.; Miyamoto, S.; Nakayama, Y. Diverse shape design and physical property evaluation of in-body tissue architecture-induced tissues. Bioengineering 2024, 11, 598. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, Z.; Dong, Y. Collagen-based biomaterials for tissue engineering. ACS Biomater. Sci. Eng. 2023, 9, 1132–1150. [Google Scholar] [CrossRef]
- Boccafoschi, F.; Habermehl, J.; Vesentini, S.; Mantovani, D. Biological performances of collagen-based scaffolds for vascular tissue engineering. Biomaterials 2005, 26, 7410–7417. [Google Scholar] [CrossRef]
- Copes, F.; Pien, N.; Van Vlierberghe, S.; Boccafoschi, F.; Mantovani, D. Collagen-based tissue engineering strategies for vascular medicine. Front. Bioeng. Biotechnol. 2019, 7, 166. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Su, C.; Zou, J.; Zhong, B.; Wang, L.; Chen, B.; Li, J.; Wei, M. Investigating the efficacy of uncrosslinked porcine collagen coated vascular grafts for neointima formation and endothelialization. Front. Bioeng. Biotechnol. 2024, 12, 1418259. [Google Scholar] [CrossRef]
- Fan, Y.; Pei, J.; Qin, Y.; Du, H.; Qu, X.; Li, W.; Huang, B.; Tan, J.; Liu, Y.; Li, G.; et al. Construction of tissue-engineered vascular grafts with enhanced patency by integrating heparin.; cell-adhesive peptide.; and carbon monoxide nanogenerators into acellular blood vessels. Bioact. Mater. 2023, 34, 221–236. [Google Scholar] [CrossRef] [PubMed]
- Radke, D.; Jia, W.; Sharma, D.; Fena, K.; Wang, G.; Goldman, J.; Zhao, F. Tissue engineering at the blood-contacting surface: A review of challenges and strategies in vascular graft development. Adv. Healthc. Mater. 2018, 7, e1701461. [Google Scholar] [CrossRef]
- Smith, R.J., Jr.; Yi, T.; Nasiri, B.; Breuer, C.K.; Andreadis, S.T. Implantation of VEGF-functionalized cell-free vascular grafts: Regenerative and immunological response. FASEB J. 2019, 33, 5089–5100. [Google Scholar] [CrossRef]
- Rodriguez-Soto, M.A.; Riveros, A.; Suarez Vargas, N.; Garcia-Brand, A.J.; Camargo, C.M.; Cruz, J.C.; Sandoval, N.; Briceño, J.C. Failure analysis of TEVG’s II: Late failure and entering the regeneration pathway. Cells 2022, 11, 939. [Google Scholar] [CrossRef]
- Hao, D.; Fan, Y.; Xiao, W.; Liu, R.; Pivetti, C.; Walimbe, T.; Guo, F.; Zhang, X.; Farmer, D.L.; Wang, F.; et al. Rapid endothelialization of small diameter vascular grafts by a bioactive integrin-binding ligand specifically targeting endothelial progenitor cells and endothelial. Cells Acta Biomater. 2020, 108, 178–193. [Google Scholar] [CrossRef]
- Zizhou, R.; Wang, X.; Houshyar, S. Review of polymeric biomimetic small-diameter vascular grafts to tackle intimal hyperplasia. ACS Omega 2022, 7, 22125–22148. [Google Scholar] [CrossRef] [PubMed]
- Etzerodt, A.; Moestrup, S.K. CD163 and inflammation: Biological, diagnostic, and therapeutic aspects. Antioxid. Redox Signal 2013, 18, 2352–2363. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.; Sakamoto, A.; Kawakami, R.; Guo, L.; Slenders, L.; Mosquera, J.V.; Ghosh, S.K.B.; Wesseling, M.; Shiraki, T.; Bellissard, A.; et al. CD163+ macrophages induce endothelial-to-mesenchymal transition in atheroma. Circ. Res. 2024, 135, e4–e23. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Akahori, H.; Harari, E.; Smith, S.L.; Polavarapu, R.; Karmali, V.; Otsuka, F.; Gannon, R.L.; Braumann, R.E.; Dickinson, M.H.; et al. CD163+ macrophages promote angiogenesis and vascular permeability accompanied by inflammation in atherosclerosis. J. Clin. Investig. 2018, 128, 1106–1124. [Google Scholar] [CrossRef]
- Sakamoto, A.; Kawakami, R.; Mori, M.; Guo, L.; Paek, K.H.; Mosquera, J.V.; Cornelissen, A.; Ghosh, S.K.B.; Kawai, K.; Konishi, T.; et al. CD163+ macrophages restrain vascular calcification.; promoting the development of high-risk plaque. JCI Insight 2023, 8, e154922. [Google Scholar] [CrossRef]
- Dhange, M.; Sankad, G.; Safdar, R.; Jamshed, W.; Eid, M.R.; Bhujakkanavar, U.; Gouadria, S.; Chouikh, R. A mathematical model of blood flow in a stenosed artery with post-stenotic dilatation and a forced field. PLoS ONE 2022, 17, e0266727. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, K.; Umeno, T.; Kawashima, T.; Shuto, T.; Iwai, R.; Teng, L.; Tajikawa, T.; Nakayama, Y.; Miyamoto, S. Six-Month Patency of Long Carotid Bypass Grafts Constructed with In-Body Tissue Architecture-Induced Small-Diameter Biotubes in a Goat Model. Bioengineering 2025, 12, 260. https://doi.org/10.3390/bioengineering12030260
Mori K, Umeno T, Kawashima T, Shuto T, Iwai R, Teng L, Tajikawa T, Nakayama Y, Miyamoto S. Six-Month Patency of Long Carotid Bypass Grafts Constructed with In-Body Tissue Architecture-Induced Small-Diameter Biotubes in a Goat Model. Bioengineering. 2025; 12(3):260. https://doi.org/10.3390/bioengineering12030260
Chicago/Turabian StyleMori, Kazuki, Tadashi Umeno, Takayuki Kawashima, Takashi Shuto, Ryosuke Iwai, Lupeng Teng, Tsutomu Tajikawa, Yasuhide Nakayama, and Shinji Miyamoto. 2025. "Six-Month Patency of Long Carotid Bypass Grafts Constructed with In-Body Tissue Architecture-Induced Small-Diameter Biotubes in a Goat Model" Bioengineering 12, no. 3: 260. https://doi.org/10.3390/bioengineering12030260
APA StyleMori, K., Umeno, T., Kawashima, T., Shuto, T., Iwai, R., Teng, L., Tajikawa, T., Nakayama, Y., & Miyamoto, S. (2025). Six-Month Patency of Long Carotid Bypass Grafts Constructed with In-Body Tissue Architecture-Induced Small-Diameter Biotubes in a Goat Model. Bioengineering, 12(3), 260. https://doi.org/10.3390/bioengineering12030260