
Tissue Engineering for Penile Reconstruction

 , ,
, ,  and
and
Abstract
1. Introduction
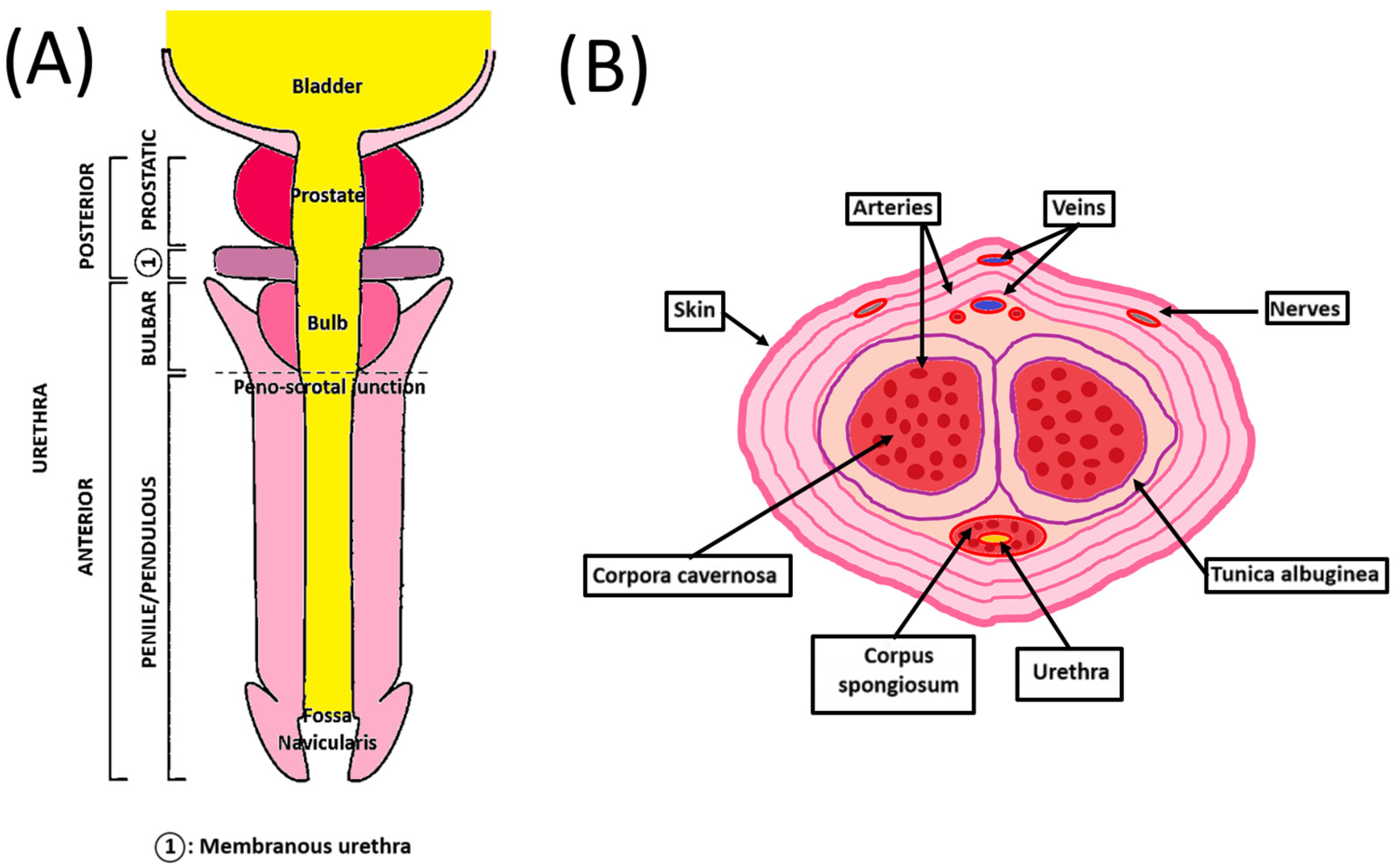
2. Penile Anatomy
3. Common Penile Pathologies, Anomalies, and Treatments
4. Tissue Engineering
4.1. Urethroplasty
4.1.1. Synthetic Biomaterials
4.1.2. Intelligent Biomaterials
4.1.3. Natural Biomaterials
4.2. Tissue Engineering for Peyronie’s Disease Correction
4.3. Corpus Cavernosum Replacement Strategies
4.4. Bioprinting
4.5. Acellularization of the Penis
5. Tissue Engineering: The Self-Assembly Approach
5.1. Urethral Substitutes
5.2. Tunic Albuginea Substitutes
6. Limitations and Perspectives

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Year | Animal | Outcome | Reference |
|---|---|---|---|---|
| Tissues | ||||
| Oral (buccal, lingual) mucosa | 1890 1992 1992 | Human Dog/Human Human | + | [172] [173] [174] |
| Genital skin | 1953 2008 | Human Human | − | [175] [176] |
| Dermal grafts | 1979 1995 | Human Human | − | [177] [178] |
| Vein graft | 1998 | Human | + | [179] |
| Tunica vaginalis | 1995 | Human | − | [180] |
| Fascia | 2022 | Human | + | [181] |
| Materials | ||||
| Synthetic * | 2012 2004 | In vitro In vitro/mouse | +/− | [97] [98] |
| Intelligent biomaterials: | 2013 2015 | In vitro In vitro | + | [102] [103] |
| Natural Acellular matrices -silk fibroin -collagen | 2007 2007 2013 2012 2015 2014 2018 | Human Human Human Rabbit Rabbit Rabbit | +/− | [120] [121] [122] [132] [133] [111] [115] |
| Penile Decellularization | 2019 | In vitro | + | [145] |
| Self-assembly technique | 2011 2013 | Mouse Mouse | + | [170] [164] |
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations List
| 3D | 3-Dimensional |
| ACCMs | Acellular corporal collagen matrix |
| ACM | Acellular matrix |
| BAM | Bladder acellular matrix |
| BMC | Bladder mesenchymal cell |
| DF | Dermal fibroblast |
| EC | Endothelial cell |
| ECM | Extracellular matrix |
| HIF-1α | Hypoxia-inducible factor-1α |
| IPSC | Induced pluripotent stem cell |
| K14 | Keratin 14 |
| LOEX | Laboratoire d’Organogenèse Expérimentale |
| MDSCs | Muscle-derived stem cell |
| PCL | Polycaprolactone |
| PET | Polyethylene terephthalate |
| PGA | Poly-glycolic acid |
| PLA | Poly-lactic acid |
| PLGA | Poly-lactic-co-glycolide |
| PNIPAM | Poly N-isopropylacrylamide |
| PTFE | Polytetrafluoroethylene |
| SIS | Small intestinal submucosa |
| SMC | Smooth muscle cell |
| UC | Urothelial cell |
| VEGF | Vascular endothelial growth factor |
| VF | Vesical fibroblast |
References
- Bouty, A.; Ayers, K.L.; Pask, A.; Heloury, Y.; Sinclair, A.H. The Genetic and Environmental Factors Underlying Hypospadias. Sex. Dev. 2015, 9, 239–259. [Google Scholar] [CrossRef]
- Loftus, C.J.; Wood, H.M. Congenital causes of neurogenic bladder and the transition to adult care. Transl. Androl. Urol. 2016, 5, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Keays, M.A.; Dave, S. Current hypospadias management: Diagnosis, surgical management, and long-term patient-centred outcomes. Can. Urol. Assoc. J. 2017, 11, S48–S53. [Google Scholar] [CrossRef] [PubMed]
- Abbas, T.O.; Mahdi, E.; Hasan, A.; AlAnsari, A.; Pennisi, C.P. Current Status of Tissue Engineering in the Management of Severe Hypospadias. Front. Pediatr. 2017, 5, 283. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.J.; DeSouza, R.A. Anterior urethral stricture review. Transl. Androl. Urol. 2013, 2, 32–38. [Google Scholar] [CrossRef]
- Mangera, A.; Osman, N.; Chapple, C. Evaluation and management of anterior urethral stricture disease. F1000Res 2016, 5, 153. [Google Scholar] [CrossRef]
- Davis, N.F.; Quinlan, M.R.; Bhatt, N.R.; Browne, C.; MacCraith, E.; Manecksha, R.; Walsh, M.T.; Thornhill, J.A.; Mulvin, D. Incidence, Cost, Complications and Clinical Outcomes of Iatrogenic Urethral Catheterization Injuries: A Prospective Multi-Institutional Study. J. Urol. 2016, 196, 1473–1477. [Google Scholar] [CrossRef]
- Santucci, R.A.; Joyce, G.F.; Wise, M. Male urethral stricture disease. J. Urol. 2007, 177, 1667–1674. [Google Scholar] [CrossRef]
- Pederzoli, F.; Joice, G.; Salonia, A.; Bivalacqua, T.J.; Sopko, N.A. Regenerative and engineered options for urethroplasty. Nat. Rev. Urol. 2019, 16, 453–464. [Google Scholar] [CrossRef]
- Andersson, K.E.; McCloskey, K.D. Lamina propria: The functional center of the bladder? Neurourol. Urodyn. 2014, 33, 9–16. [Google Scholar] [CrossRef]
- Baskin, L.S.; Erol, A.; Li, Y.W.; Liu, W.H. Anatomy of the neurovascular bundle: Is safe mobilization possible? J. Urol. 2000, 164, 977–980. [Google Scholar] [CrossRef]
- Chung, B.I.; Sommer, G.; Brooks, J.D. Anatomy of the Lower Urinary Tract and Male Genitalia. In Campbell-Walsh Urology; Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Perron, J. Abnormalities of the penis and abnormalities of the end of the urethra: Their surgical treatment. Soins 1969, 14, 347–353. [Google Scholar]
- Barbagli, G.; Palminteri, E.; Lazzeri, M.; Guazzoni, G. Anterior urethral strictures. BJU Int. 2003, 92, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Barbagli, G.; Sansalone, S.; Djinovic, R.; Romano, G.; Lazzeri, M. Current controversies in reconstructive surgery of the anterior urethra: A clinical overview. Int. Braz. J. Urol. 2012, 38, 307–316; discussion 316. [Google Scholar] [CrossRef] [PubMed]
- Caneparo, C.; Chabaud, S.; Bolduc, S. Reconstruction of Vascular and Urologic Tubular Grafts by Tissue Engineering. Processes 2021, 9, 513. [Google Scholar] [CrossRef]
- Andrew, T.W.; Kanapathy, M.; Murugesan, L.; Muneer, A.; Kalaskar, D.; Atala, A. Towards clinical application of tissue engineering for erectile penile regeneration. Nat. Rev. Urol. 2019, 16, 734–744. [Google Scholar] [CrossRef] [PubMed]
- Yao, A.; Ingargiola, M.J.; Lopez, C.D.; Sanati-Mehrizy, P.; Burish, N.M.; Jablonka, E.M.; Taub, P.J. Total penile reconstruction: A systematic review. J. Plast. Reconstr. Aesthet. Surg. 2018, 71, 788–806. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.; Laforge, J.; Ross, M.M.; Vanlangendonck, R.; Hasoon, J.; Viswanath, O.; Kaye, A.D.; Urits, I. Male Sexual Dysfunction. Health Psychol. Res. 2022, 10, 37533. [Google Scholar] [CrossRef]
- Kraft, K.H.; Shukla, A.R.; Canning, D.A. Proximal hypospadias. Sci. World J. 2011, 11, 894–906. [Google Scholar] [CrossRef]
- Boillot, B.; Teklali, Y.; Moog, R.; Droupy, S. Penile congenital abnormalities. Prog. Urol. 2013, 23, 664–673. [Google Scholar] [CrossRef] [PubMed]
- Caione, P. Prevalence of hypospadias in European countries: Is it increasing? Eur. Urol. 2009, 55, 1027–1029; discussion 1029–1030. [Google Scholar] [CrossRef]
- Nelson, C.P.; Park, J.M.; Wan, J.; Bloom, D.A.; Dunn, R.L.; Wei, J.T. The increasing incidence of congenital penile anomalies in the United States. J. Urol. 2005, 174, 1573–1576. [Google Scholar] [CrossRef]
- Sagodi, L.; Kiss, A.; Kiss-Toth, E.; Barkai, L. Prevalence and possible causes of hypospadias. Orv. Hetil. 2014, 155, 978–985. [Google Scholar] [CrossRef]
- He, H.G.; Han, C.H.; Zhang, W. A Mouse Model of Hypospadias Induced by Estradiol Benzoate. Cell Biochem. Biophys. 2015, 73, 589–592. [Google Scholar] [CrossRef] [PubMed]
- Montag, S.; Palmer, L.S. Abnormalities of penile curvature: Chordee and penile torsion. Sci. World J. 2011, 11, 1470–1478. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, J.C.; Wiener, J.S.; Gargollo, P.C.; Inman, B.A.; Ross, S.S.; Routh, J.C. Contemporary epidemiological trends in complex congenital genitourinary anomalies. J. Urol. 2013, 190, 1590–1595. [Google Scholar] [CrossRef] [PubMed]
- Shankar, K.R.; Rickwood, A.M. The incidence of phimosis in boys. BJU Int. 1999, 84, 101–102. [Google Scholar] [CrossRef]
- Hayashi, Y.; Kojima, Y.; Mizuno, K.; Kohri, K. Prepuce: Phimosis, paraphimosis, and circumcision. Sci. World J. 2011, 11, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Chan, I.H.; Wong, K.K. Common urological problems in children: Prepuce, phimosis, and buried penis. Hong Kong Med. J. 2016, 22, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Bouvattier, C. Micropenis. Arch. Pediatr. 2014, 21, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Hatipoglu, N.; Kurtoglu, S. Micropenis: Etiology, diagnosis and treatment approaches. J. Clin. Res. Pediatr. Endocrinol. 2013, 5, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Sun, A.J.; Li, S.; Eisenberg, M.L. The Impact of Clostridium Histolyticum Collagenase on the Prevalence and Management of Peyronie’s Disease in the United States. World J. Mens. Health 2019, 37, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Pryor, J.; Akkus, E.; Alter, G.; Jordan, G.; Lebret, T.; Levine, L.; Mulhall, J.; Perovic, S.; Ralph, D.; Stackl, W. Peyronie’s disease. J. Sex. Med. 2004, 1, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Zhang, Y. Surgical Treatment of Primary Penile Scrotal Lymphedema: A Case Report. Urology 2021, 149, 225–226. [Google Scholar] [CrossRef] [PubMed]
- Shim, T.N.; Doiron, P.R.; Francis, N.; Minhas, S.; Muneer, A.; Hawkins, D.; Dinneen, M.; Bunker, C.B. Penile lymphoedema: Approach to investigation and management. Clin. Exp. Dermatol. 2019, 44, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Wood, D.; Woodhouse, C. Penile anomalies in adolescence. Sci. World J. 2011, 11, 614–623. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ericson, C.; Baird, B.; Broderick, G.A. Management of Priapism: 2021 Update. Urol. Clin. North. Am. 2021, 48, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Keskin, D.; Cal, C.; Delibas, M.; Ozyurt, C.; Gunaydin, G.; Nazli, O.; Cureklibatir, I. Intracavernosal adrenalin injection in priapism. Int. J. Impot. Res. 2000, 12, 312–314. [Google Scholar] [CrossRef][Green Version]
- Steinberg, M.H. Sickle cell anemia, the first molecular disease: Overview of molecular etiology, pathophysiology, and therapeutic approaches. Sci. World J. 2008, 8, 1295–1324. [Google Scholar] [CrossRef]
- Corradini, F.; Zattoni, M.; Barbagli, G.; Bianchi, G.; Giovanardi, M.; Serafini, C.; Genna, V.G.; Ribbene, A.; Balo, S.; Fidanza, F.; et al. Comparative Assessment of Cultures from Oral and Urethral Stem Cells for Urethral Regeneration. Curr. Stem Cell Res. Ther. 2016, 11, 643–651. [Google Scholar] [CrossRef]
- Rashidbenam, Z.; Jasman, M.H.; Hafez, P.; Tan, G.H.; Goh, E.H.; Fam, X.I.; Ho, C.C.K.; Zainuddin, Z.M.; Rajan, R.; Nor, F.M.; et al. Overview of Urethral Reconstruction by Tissue Engineering: Current Strategies, Clinical Status and Future Direction. Tissue Eng. Regen. Med. 2019, 16, 365–384. [Google Scholar] [CrossRef]
- Xuan, Z.; Zachar, V.; Pennisi, C.P. Sources, Selection, and Microenvironmental Preconditioning of Cells for Urethral Tissue Engineering. Int. J. Mol. Sci. 2022, 23, 14074. [Google Scholar] [CrossRef] [PubMed]
- Casarin, M.; Morlacco, A.; Dal Moro, F. Tissue Engineering and Regenerative Medicine in Pediatric Urology: Urethral and Urinary Bladder Reconstruction. Int. J. Mol. Sci. 2022, 23, 6360. [Google Scholar] [CrossRef] [PubMed]
- Culenova, M.; Ziaran, S.; Danisovic, L. Cells Involved in Urethral Tissue Engineering: Systematic Review. Cell Transplant. 2019, 28, 1106–1115. [Google Scholar] [CrossRef] [PubMed]
- Browne, B.M.; Vanni, A.J. Use of Alternative Techniques and Grafts in Urethroplasty. Urol. Clin. North. Am. 2017, 44, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Milenkovic, U.; Albersen, M.; Castiglione, F. The mechanisms and potential of stem cell therapy for penile fibrosis. Nat. Rev. Urol. 2019, 16, 79–97. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Gupta, D.K. Tissue Engineering and Stem Cell Therapy in Pediatric Urology. J. Indian. Assoc. Pediatr. Surg. 2019, 24, 237–246. [Google Scholar] [CrossRef]
- Pozzi, E.; Muneer, A.; Sangster, P.; Alnajjar, H.M.; Salonia, A.; Bettocchi, C.; Castiglione, F.; Ralph, D.J. on behalf of the Trauma, Reconstructive Urology Working Party of the European Association of Urology (EAU) Young Academic Urologists (YAU). Stem-cell regenerative medicine as applied to the penis. Curr. Opin. Urol. 2019, 29, 443–449. [Google Scholar] [CrossRef]
- Johnson, M.J.; Kristinsson, S.; Ralph, O.; Chiriaco, G.; Ralph, D. The surgical management of ischaemic priapism. Int. J. Impot. Res. 2020, 32, 81–88. [Google Scholar] [CrossRef]
- Alnajjar, H.M.; Muneer, A. Recent advances in understanding and treating priapism. Fac. Rev. 2022, 11, 23. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Hsu, G.L.; Chang, S.J.; Yang, S.S.; Liu, S.P.; Hsieh, J.T. Surgical niche for the treatment of erectile dysfunction. Int. J. Urol. 2020, 27, 117–133. [Google Scholar] [CrossRef]
- Molodysky, E.; Liu, S.P.; Huang, S.J.; Hsu, G.L. Penile vascular surgery for treating erectile dysfunction: Current role and future direction. Arab. J. Urol. 2013, 11, 254–266. [Google Scholar] [CrossRef]
- Munarriz, R.; Thirumavalavan, N.; Gross, M.S. Is There a Role for Vascular Surgery in the Contemporary Management of Erectile Dysfunction? Urol. Clin. North. Am. 2021, 48, 543–555. [Google Scholar] [CrossRef]
- Kayes, O.; Shabbir, M.; Ralph, D.; Minhas, S. Therapeutic strategies for patients with micropenis or penile dysmorphic disorder. Nat. Rev. Urol. 2012, 9, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Kohn, T.P.; Pena, V.; Redett Iii, R.J., 3rd; Burnett, A.L. Penile allotransplantation: Early outcomes from reported cases and survivorship considerations. Minerva Urol. Nephrol. 2021, 73, 333–341. [Google Scholar] [CrossRef]
- Sopko, N.A.; Burnett, A.L. Penile transplantation is here. Lancet 2017, 390, 1008–1010. [Google Scholar] [CrossRef] [PubMed]
- Cetrulo, C.L., Jr.; Li, K.; Salinas, H.M.; Treiser, M.D.; Schol, I.; Barrisford, G.W.; McGovern, F.J.; Feldman, A.S.; Grant, M.T.; Tanrikut, C.; et al. Penis Transplantation: First US Experience. Ann. Surg. 2018, 267, 983–988. [Google Scholar] [CrossRef]
- Kueckelhaus, M.; Fischer, S.; Seyda, M.; Bueno, E.M.; Aycart, M.A.; Alhefzi, M.; ElKhal, A.; Pomahac, B.; Tullius, S.G. Vascularized composite allotransplantation: Current standards and novel approaches to prevent acute rejection and chronic allograft deterioration. Transpl. Int. 2016, 29, 655–662. [Google Scholar] [CrossRef]
- Markiewicz, M.R.; Lukose, M.A.; Margarone, J.E., 3rd; Barbagli, G.; Miller, K.S.; Chuang, S.K. The oral mucosa graft: A systematic review. J. Urol. 2007, 178, 387–394. [Google Scholar] [CrossRef]
- Aldaqadossi, H.A.; Shaker, H.; Youssof, H.; Kotb, Y.; Eladawy, M. Outcomes of staged lingual mucosal graft urethroplasty for redo hypospadias repair. J. Pediatr. Urol. 2019, 15, 519.e511–519.e517. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.P.; Bloom, D.A.; Kinast, R.; Wei, J.T.; Park, J.M. Patient-reported sexual function after oral mucosa graft urethroplasty for hypospadias. Urology 2005, 66, 1086–1089; discussion 1089–1090. [Google Scholar] [CrossRef]
- Markiewicz, M.R.; DeSantis, J.L.; Margarone, J.E., 3rd; Pogrel, M.A.; Chuang, S.K. Morbidity associated with oral mucosa harvest for urological reconstruction: An overview. J. Oral. Maxillofac. Surg. 2008, 66, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Dublin, N.; Stewart, L.H. Oral complications after buccal mucosal graft harvest for urethroplasty. BJU Int. 2004, 94, 867–869. [Google Scholar] [CrossRef] [PubMed]
- Djordjevic, M.L. Graft surgery in extensive urethral stricture disease. Curr. Urol. Rep. 2014, 15, 424. [Google Scholar] [CrossRef]
- Kim, S.J.; Lee, J.; Park, C.H.; Park, J.Y.; Song, S.H.; Kim, K.S.; Kim, H.G. Urethral defect due to periurethral abscess treated with a tunica vaginalis flap: A case report. Medicine 2018, 97, e13249. [Google Scholar] [CrossRef] [PubMed]
- Hmida, W.; Othmen, M.B.; Bako, A.; Jaidane, M.; Mosbah, F. Penile skin flap: A versatile substitute for anterior urethral stricture. Int. Braz. J. Urol. 2019, 45, 1057–1063. [Google Scholar] [CrossRef] [PubMed]
- Versteegden, L.R.; de Jonge, P.K.; IntHout, J.; van Kuppevelt, T.H.; Oosterwijk, E.; Feitz, W.F.; de Vries, R.B.; Daamen, W.F. Tissue Engineering of the Urethra: A Systematic Review and Meta-analysis of Preclinical and Clinical Studies. Eur. Urol. 2017, 72, 594–606. [Google Scholar] [CrossRef]
- Langer, R.; Vacanti, J.P. Tissue engineering. Science 1993, 260, 920–926. [Google Scholar] [CrossRef]
- Berthiaume, F.; Maguire, T.J.; Yarmush, M.L. Tissue engineering and regenerative medicine: History, progress, and challenges. Annu. Rev. Chem. Biomol. Eng. 2011, 2, 403–430. [Google Scholar] [CrossRef]
- Langer, R.; Vacanti, J. Advances in tissue engineering. J. Pediatr. Surg. 2016, 51, 8–12. [Google Scholar] [CrossRef]
- Zhang, J.; Xu, W.; Li, C.; Meng, F.; Guan, Y.; Liu, X.; Zhao, J.; Peng, J.; Wang, Y. Tissue Engineering Microtissue: Construction, Optimization, and Application. Tissue Eng. Part B Rev. 2022, 28, 393–404. [Google Scholar] [CrossRef]
- Bedard, P.; Gauvin, S.; Ferland, K.; Caneparo, C.; Pellerin, E.; Chabaud, S.; Bolduc, S. Innovative Human Three-Dimensional Tissue-Engineered Models as an Alternative to Animal Testing. Bioengineering 2020, 7, 115. [Google Scholar] [CrossRef]
- Roy, V.; Magne, B.; Vaillancourt-Audet, M.; Blais, M.; Chabaud, S.; Grammond, E.; Piquet, L.; Fradette, J.; Laverdiere, I.; Moulin, V.J.; et al. Human Organ-Specific 3D Cancer Models Produced by the Stromal Self-Assembly Method of Tissue Engineering for the Study of Solid Tumors. Biomed. Res. Int. 2020, 2020, 6051210. [Google Scholar] [CrossRef] [PubMed]
- Caneparo, C.; Sorroza-Martinez, L.; Chabaud, S.; Fradette, J.; Bolduc, S. Considerations for the clinical use of stem cells in genitourinary regenerative medicine. World J. Stem Cells 2021, 13, 1480–1512. [Google Scholar] [CrossRef]
- Reiss, J.; Robertson, S.; Suzuki, M. Cell Sources for Cultivated Meat: Applications and Considerations throughout the Production Workflow. Int. J. Mol. Sci. 2021, 22, 7513. [Google Scholar] [CrossRef]
- Vargas, A.; Peltier, A.; Dube, J.; Lefebvre-Lavoie, J.; Moulin, V.; Goulet, F.; Lavoie, J.P. Evaluation of contractile phenotype in airway smooth muscle cells isolated from endobronchial biopsy and tissue specimens from horses. Am. J. Vet. Res. 2017, 78, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Ringuette Goulet, C.; Bernard, G.; Chabaud, S.; Couture, A.; Langlois, A.; Neveu, B.; Pouliot, F.; Bolduc, S. Tissue-engineered human 3D model of bladder cancer for invasion study and drug discovery. Biomaterials 2017, 145, 233–241. [Google Scholar] [CrossRef]
- Chaudhari, A.A.; Vig, K.; Baganizi, D.R.; Sahu, R.; Dixit, S.; Dennis, V.; Singh, S.R.; Pillai, S.R. Future Prospects for Scaffolding Methods and Biomaterials in Skin Tissue Engineering: A Review. Int. J. Mol. Sci. 2016, 17, 1974. [Google Scholar] [CrossRef]
- Baudequin, T.; Tabrizian, M. Multilineage Constructs for Scaffold-Based Tissue Engineering: A Review of Tissue-Specific Challenges. Adv. Healthc. Mater. 2018, 7, 1700734. [Google Scholar] [CrossRef]
- Loh, Q.L.; Choong, C. Three-dimensional scaffolds for tissue engineering applications: Role of porosity and pore size. Tissue Eng. Part B Rev. 2013, 19, 485–502. [Google Scholar] [CrossRef] [PubMed]
- Almeida, H.A.; Bartolo, P.J. Biomimetic Boundary-Based Scaffold Design for Tissue Engineering Applications. Methods Mol. Biol. 2021, 2147, 3–18. [Google Scholar] [CrossRef]
- Lam, J.; Lee, E.J.; Clark, E.C.; Mikos, A.G. Honing Cell and Tissue Culture Conditions for Bone and Cartilage Tissue Engineering. Cold Spring Harb. Perspect. Med. 2017, 7, a025734. [Google Scholar] [CrossRef][Green Version]
- Caneparo, C.; Baratange, C.; Chabaud, S.; Bolduc, S. Conditioned medium produced by fibroblasts cultured in low oxygen pressure allows the formation of highly structured capillary-like networks in fibrin gels. Sci. Rep. 2020, 10, 9291. [Google Scholar] [CrossRef]
- Pellerin, F.A.; Caneparo, C.; Pellerin, E.; Chabaud, S.; Pelletier, M.; Bolduc, S. Heat-Inactivation of Fetal and Newborn Sera Did Not Impair the Expansion and Scaffold Engineering Potentials of Fibroblasts. Bioengineering 2021, 8, 184. [Google Scholar] [CrossRef]
- Caneparo, C.; Chabaud, S.; Fradette, J.; Bolduc, S. Evaluation of a Serum-Free Medium for Human Epithelial and Stromal Cell Culture. Int. J. Mol. Sci. 2022, 23, 10035. [Google Scholar] [CrossRef] [PubMed]
- Pisciolaro, R.L.; Duailibi, M.T.; Novo, N.F.; Juliano, Y.; Pallos, D.; Yelick, P.C.; Vacanti, J.P.; Ferreira, L.M.; Duailibi, S.E. Tooth Tissue Engineering: The Importance of Blood Products as a Supplement in Tissue Culture Medium for Human Pulp Dental Stem Cells. Tissue Eng. Part A 2015, 21, 2639–2648. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.G.; Fu, W.J.; Wang, X.X.; Xu, Y.D.; Li, G.; Hong, B.F.; Hu, K.; Cui, F.Z.; Wang, Y.; Zhang, X. Transdifferentiation of human adipose-derived stem cells into urothelial cells: Potential for urinary tract tissue engineering. Cell Tissue Res. 2012, 347, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Yu, H.; Fan, C.; Kong, Q.; Liu, D.; Meng, L. Differentiate into urothelium and smooth muscle cells from adipose tissue-derived stem cells for ureter reconstruction in a rabbit model. Am. J. Transl. Res. 2016, 8, 3757–3768. [Google Scholar]
- Zupancic, D.; Mrak Poljsak, K.; Kreft, M.E. Co-culturing porcine normal urothelial cells, urinary bladder fibroblasts and smooth muscle cells for tissue engineering research. Cell Biol. Int. 2018, 42, 411–424. [Google Scholar] [CrossRef]
- Wu, R.; Liu, G.; Bharadwaj, S.; Zhang, Y. Isolation and myogenic differentiation of mesenchymal stem cells for urologic tissue engineering. Methods Mol. Biol. 2013, 1001, 65–80. [Google Scholar] [CrossRef]
- Li, H.; Xu, Y.; Xie, H.; Li, C.; Song, L.; Feng, C.; Zhang, Q.; Xie, M.; Wang, Y.; Lv, X. Epithelial-differentiated adipose-derived stem cells seeded bladder acellular matrix grafts for urethral reconstruction: An animal model. Tissue Eng. Part A 2014, 20, 774–784. [Google Scholar] [CrossRef]
- Ribeiro-Filho, L.A.; Sievert, K.D. Acellular matrix in urethral reconstruction. Adv. Drug Deliv. Rev. 2015, 82–83, 38–46. [Google Scholar] [CrossRef]
- Abbas, T.O.; Yalcin, H.C.; Pennisi, C.P. From Acellular Matrices to Smart Polymers: Degradable Scaffolds that are Transforming the Shape of Urethral Tissue Engineering. Int. J. Mol. Sci. 2019, 20, 1763. [Google Scholar] [CrossRef] [PubMed]
- Knecht, S.; Erggelet, C.; Endres, M.; Sittinger, M.; Kaps, C.; Stussi, E. Mechanical testing of fixation techniques for scaffold-based tissue-engineered grafts. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 83, 50–57. [Google Scholar] [CrossRef]
- Nooeaid, P.; Salih, V.; Beier, J.P.; Boccaccini, A.R. Osteochondral tissue engineering: Scaffolds, stem cells and applications. J. Cell Mol. Med. 2012, 16, 2247–2270. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.I.; Kim, B.S.; Lee, Y.M.; Ihn, K.J.; Kim, S.H.; Kim, Y.H. Morphology of elastic poly(L-lactide-co-epsilon-caprolactone) copolymers and in vitro and in vivo degradation behavior of their scaffolds. Biomacromolecules 2004, 5, 1303–1309. [Google Scholar] [CrossRef]
- Ceonzo, K.; Gaynor, A.; Shaffer, L.; Kojima, K.; Vacanti, C.A.; Stahl, G.L. Polyglycolic acid-induced inflammation: Role of hydrolysis and resulting complement activation. Tissue Eng. 2006, 12, 301–308. [Google Scholar] [CrossRef]
- Ribeiro, C.; Sencadas, V.; Correia, D.M.; Lanceros-Mendez, S. Piezoelectric polymers as biomaterials for tissue engineering applications. Colloids Surf. B Biointerfaces 2015, 136, 46–55. [Google Scholar] [CrossRef]
- Lv, X.; Feng, C.; Liu, Y.; Peng, X.; Chen, S.; Xiao, D.; Wang, H.; Li, Z.; Xu, Y.; Lu, M. A smart bilayered scaffold supporting keratinocytes and muscle cells in micro/nano-scale for urethral reconstruction. Theranostics 2018, 8, 3153–3163. [Google Scholar] [CrossRef]
- Knipe, J.M.; Peppas, N.A. Multi-responsive hydrogels for drug delivery and tissue engineering applications. Regen. Biomater. 2014, 1, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Jochum, F.D.; Theato, P. Temperature- and light-responsive smart polymer materials. Chem. Soc. Rev. 2013, 42, 7468–7483. [Google Scholar] [CrossRef]
- Correia, C.O.; Leite, A.J.; Mano, J.F. Chitosan/bioactive glass nanoparticles scaffolds with shape memory properties. Carbohydr. Polym. 2015, 123, 39–45. [Google Scholar] [CrossRef]
- Tzoneva, R.; Seifert, B.; Behl, M.; Lendlein, A. Elastic multiblock copolymers for vascular regeneration: Protein adsorption and hemocompatibility. Clin. Hemorheol. Microcirc. 2012, 52, 337–348. [Google Scholar] [CrossRef]
- Hardy, J.G.; Palma, M.; Wind, S.J.; Biggs, M.J. Responsive Biomaterials: Advances in Materials Based on Shape-Memory Polymers. Adv. Mater. 2016, 28, 5717–5724. [Google Scholar] [CrossRef]
- Roelofs, L.A.; Oosterwijk, E.; Kortmann, B.B.; Daamen, W.F.; Tiemessen, D.M.; Brouwer, K.M.; Eggink, A.J.; Crevels, A.J.; Wijnen, R.M.; van Kuppevelt, T.H.; et al. Bladder Regeneration Using a Smart Acellular Collagen Scaffold with Growth Factors VEGF, FGF2 and HB-EGF. Tissue Eng. Part A 2016, 22, 83–92. [Google Scholar] [CrossRef]
- Yuan, B.; Jin, Y.; Sun, Y.; Wang, D.; Sun, J.; Wang, Z.; Zhang, W.; Jiang, X. A strategy for depositing different types of cells in three dimensions to mimic tubular structures in tissues. Adv. Mater. 2012, 24, 890–896. [Google Scholar] [CrossRef]
- Xie, M.; Song, L.; Wang, J.; Fan, S.; Zhang, Y.; Xu, Y. Evaluation of stretched electrospun silk fibroin matrices seeded with urothelial cells for urethra reconstruction. J. Surg. Res. 2013, 184, 774–781. [Google Scholar] [CrossRef]
- Sack, B.S.; Mauney, J.R.; Estrada, C.R., Jr. Silk Fibroin Scaffolds for Urologic Tissue Engineering. Curr. Urol. Rep. 2016, 17, 16. [Google Scholar] [CrossRef] [PubMed]
- Panilaitis, B.; Altman, G.H.; Chen, J.; Jin, H.J.; Karageorgiou, V.; Kaplan, D.L. Macrophage responses to silk. Biomaterials 2003, 24, 3079–3085. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.G.; Tu, D.; Franck, D.; Gil, E.S.; Algarrahi, K.; Adam, R.M.; Kaplan, D.L.; Estrada, C.R., Jr.; Mauney, J.R. Acellular bi-layer silk fibroin scaffolds support tissue regeneration in a rabbit model of onlay urethroplasty. PLoS ONE 2014, 9, e91592. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.; Li, Z.; Chen, S.; Xie, M.; Huang, J.; Peng, X.; Yang, R.; Wang, H.; Xu, Y.; Feng, C. Structural and functional evaluation of oxygenating keratin/silk fibroin scaffold and initial assessment of their potential for urethral tissue engineering. Biomaterials 2016, 84, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Gundogdu, G.; Okhunov, Z.; Cristofaro, V.; Starek, S.; Veneri, F.; Orabi, H.; Jiang, P.; Sullivan, M.P.; Mauney, J.R. Evaluation of Bi-Layer Silk Fibroin Grafts for Tubular Ureteroplasty in a Porcine Defect Model. Front. Bioeng. Biotechnol. 2021, 9, 723559. [Google Scholar] [CrossRef] [PubMed]
- Pinnagoda, K.; Larsson, H.M.; Vythilingam, G.; Vardar, E.; Engelhardt, E.M.; Thambidorai, R.C.; Hubbell, J.A.; Frey, P. Engineered acellular collagen scaffold for endogenous cell guidance, a novel approach in urethral regeneration. Acta Biomater. 2016, 43, 208–217. [Google Scholar] [CrossRef]
- Larsson, H.M.; Vythilingam, G.; Pinnagoda, K.; Vardar, E.; Engelhardt, E.M.; Sothilingam, S.; Thambidorai, R.C.; Kamarul, T.; Hubbell, J.A.; Frey, P. Fiber density of collagen grafts impacts rabbit urethral regeneration. Sci. Rep. 2018, 8, 10057. [Google Scholar] [CrossRef]
- Vardar, E.; Engelhardt, E.M.; Larsson, H.M.; Mouloungui, E.; Pinnagoda, K.; Hubbell, J.A.; Frey, P. Tubular Compressed Collagen Scaffolds for Ureteral Tissue Engineering in a Flow Bioreactor System. Tissue Eng. Part A 2015, 21, 2334–2345. [Google Scholar] [CrossRef] [PubMed]
- Davis, N.F.; Cunnane, E.M.; O’Brien, F.J.; Mulvihill, J.J.; Walsh, M.T. Tissue engineered extracellular matrices (ECMs) in urology: Evolution and future directions. Surgeon 2018, 16, 55–65. [Google Scholar] [CrossRef]
- Badylak, S.F.; Lantz, G.C.; Coffey, A.; Geddes, L.A. Small intestinal submucosa as a large diameter vascular graft in the dog. J. Surg. Res. 1989, 47, 74–80. [Google Scholar] [CrossRef]
- Zhang, Y.; Kropp, B.P.; Moore, P.; Cowan, R.; Furness, P.D., 3rd; Kolligian, M.E.; Frey, P.; Cheng, E.Y. Coculture of bladder urothelial and smooth muscle cells on small intestinal submucosa: Potential applications for tissue engineering technology. J. Urol. 2000, 164, 928–934; discussion 925–934. [Google Scholar] [CrossRef]
- Fiala, R.; Vidlar, A.; Vrtal, R.; Belej, K.; Student, V. Porcine small intestinal submucosa graft for repair of anterior urethral strictures. Eur. Urol. 2007, 51, 1702–1708; discussion 1708. [Google Scholar] [CrossRef]
- Palminteri, E.; Berdondini, E.; Colombo, F.; Austoni, E. Small intestinal submucosa (SIS) graft urethroplasty: Short-term results. Eur. Urol. 2007, 51, 1695–1701; discussion 1701. [Google Scholar] [CrossRef]
- Orabi, H.; Safwat, A.S.; Shahat, A.; Hammouda, H.M. The use of small intestinal submucosa graft for hypospadias repair: Pilot study. Arab. J. Urol. 2013, 11, 415–420. [Google Scholar] [CrossRef]
- Kubricht, W.S., 3rd; Williams, B.J.; Eastham, J.A.; Venable, D.D. Tensile strength of cadaveric fascia lata compared to small intestinal submucosa using suture pull through analysis. J. Urol. 2001, 165, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Kuniakova, M.; Klein, M.; Galfiova, P.; Csobonyeiova, M.; Feitscherova, C.; Polak, S.; Novakova, Z.V.; Topoliova, K.; Trebaticky, B.; Varga, I.; et al. Decellularization of the human urethra for tissue engineering applications. Exp. Biol. Med. 2023, 248, 1034–1042. [Google Scholar] [CrossRef] [PubMed]
- Kasravi, M.; Ahmadi, A.; Babajani, A.; Mazloomnejad, R.; Hatamnejad, M.R.; Shariatzadeh, S.; Bahrami, S.; Niknejad, H. Immunogenicity of decellularized extracellular matrix scaffolds: A bottleneck in tissue engineering and regenerative medicine. Biomater. Res. 2023, 27, 10. [Google Scholar] [CrossRef] [PubMed]
- Feil, G.; Christ-Adler, M.; Maurer, S.; Corvin, S.; Rennekampff, H.O.; Krug, J.; Hennenlotter, J.; Kuehs, U.; Stenzl, A.; Sievert, K.D. Investigations of urothelial cells seeded on commercially available small intestine submucosa. Eur. Urol. 2006, 50, 1330–1337. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Qinglai, T.; Yang, Q.; Li, M.; Zeng, S.; Yang, X.; Xiao, Z.; Tong, X.; Lei, L.; Li, S. Functional acellular matrix for tissue repair. Mater. Today Bio 2023, 18, 100530. [Google Scholar] [CrossRef]
- Dorin, R.P.; Pohl, H.G.; De Filippo, R.E.; Yoo, J.J.; Atala, A. Tubularized urethral replacement with unseeded matrices: What is the maximum distance for normal tissue regeneration? World J. Urol. 2008, 26, 323–326. [Google Scholar] [CrossRef]
- Yoo, J.J.; Meng, J.; Oberpenning, F.; Atala, A. Bladder augmentation using allogenic bladder submucosa seeded with cells. Urology 1998, 51, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Hauser, S.; Bastian, P.J.; Fechner, G.; Muller, S.C. Small intestine submucosa in urethral stricture repair in a consecutive series. Urology 2006, 68, 263–266. [Google Scholar] [CrossRef]
- Nuininga, J.E.; van Moerkerk, H.; Hanssen, A.; Hulsbergen, C.A.; Oosterwijk-Wakka, J.; Oosterwijk, E.; de Gier, R.P.; Schalken, J.A.; van Kuppevelt, T.; Feitz, W.F. Rabbit urethra replacement with a defined biomatrix or small intestinal submucosa. Eur. Urol. 2003, 44, 266–271. [Google Scholar] [CrossRef]
- Gu, G.L.; Xia, S.J.; Zhang, J.; Liu, G.H.; Yan, L.; Xu, Z.H.; Zhu, Y.J. Tubularized urethral replacement using tissue-engineered peritoneum-like tissue in a rabbit model. Urol. Int. 2012, 89, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Chun, S.Y.; Kim, B.S.; Kwon, S.Y.; Park, S.I.; Song, P.H.; Yoo, E.S.; Kim, B.W.; Kwon, T.G.; Kim, H.T. Urethroplasty using autologous urethral tissue-embedded acellular porcine bladder submucosa matrix grafts for the management of long-segment urethral stricture in a rabbit model. J. Korean Med. Sci. 2015, 30, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Roth, C.C.; Kropp, B.P. Recent advances in urologic tissue engineering. Curr. Urol. Rep. 2009, 10, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Lentz, A.C.; Carson, C.C., 3rd. Peyronie’s surgery: Graft choices and outcomes. Curr. Urol. Rep. 2009, 10, 460–467. [Google Scholar] [CrossRef]
- Ferretti, L.; Giuliani, M.; Bessede, T.; Qiu, X.; Zhang, H.; Alsaid, B.; Durrbach, A.; Giuliano, F.; Benoit, G.; Droupy, S. Tissue engineering for penile surgery: Comparative study of noncellular and cell-seeded synthetic grafts for tunica albuginea replacement. J. Sex. Med. 2012, 9, 625–631. [Google Scholar] [CrossRef]
- Eberli, D.; Susaeta, R.; Yoo, J.J.; Atala, A. A method to improve cellular content for corporal tissue engineering. Tissue Eng. Part A 2008, 14, 1581–1589. [Google Scholar] [CrossRef]
- Gundogdu, G.; Okhunov, Z.; Starek, S.; Veneri, F.; Orabi, H.; Holzman, S.A.; Sullivan, M.P.; Khoury, A.E.; Mauney, J.R. Evaluation of Bi-Layer Silk Fibroin Grafts for Penile Tunica Albuginea Repair in a Rabbit Corporoplasty Model. Front. Bioeng. Biotechnol. 2021, 9, 791119. [Google Scholar] [CrossRef]
- Knoll, L.D. Use of small intestinal submucosa graft for the surgical management of Peyronie’s disease. J. Urol. 2007, 178, 2474–2478; discussion 2478. [Google Scholar] [CrossRef]
- Breyer, B.N.; Brant, W.O.; Garcia, M.M.; Bella, A.J.; Lue, T.F. Complications of porcine small intestine submucosa graft for Peyronie’s disease. J. Urol. 2007, 177, 589–591. [Google Scholar] [CrossRef]
- Leungwattanakij, S.; Bivalacqua, T.J.; Reddy, S.; Hellstrom, W.J. Long-term follow-up on use of pericardial graft in the surgical management of Peyronie’s disease. Int. J. Impot. Res. 2001, 13, 183–186. [Google Scholar] [CrossRef]
- Taylor, F.L.; Levine, L.A. Surgical correction of Peyronie’s disease via tunica albuginea plication or partial plaque excision with pericardial graft: Long-term follow up. J. Sex. Med. 2008, 5, 2221–2228; discussion 2229–2230. [Google Scholar] [CrossRef] [PubMed]
- Fallon, B. Cadaveric dura mater graft for correction of penile curvature in Peyronie disease. Urology 1990, 35, 127–129. [Google Scholar] [CrossRef]
- Leungwattanakij, S.; Bivalacqua, T.J.; Yang, D.Y.; Hyun, J.S.; Hellstrom, W.J. Comparison of cadaveric pericardial, dermal, vein, and synthetic grafts for tunica albuginea substitution using a rat model. BJU Int. 2003, 92, 119–124. [Google Scholar] [CrossRef] [PubMed]
- van der Merwe, A.; Graewe, F.; Zuhlke, A.; Barsdorf, N.W.; Zarrabi, A.D.; Viljoen, J.T.; Ackermann, H.; Spies, P.V.; Opondo, D.; Al-Qaoud, T.; et al. Penile allotransplantation for penis amputation following ritual circumcision: A case report with 24 months of follow-up. Lancet 2017, 390, 1038–1047. [Google Scholar] [CrossRef]
- Henry, G.D.; Donatucci, C.F.; Conners, W.; Greenfield, J.M.; Carson, C.C.; Wilson, S.K.; Delk, J.; Lentz, A.C.; Cleves, M.A.; Jennermann, C.J.; et al. An outcomes analysis of over 200 revision surgeries for penile prosthesis implantation: A multicenter study. J. Sex. Med. 2012, 9, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Micol, L.A.; Arenas da Silva, L.F.; Geutjes, P.J.; Oosterwijk, E.; Hubbell, J.A.; Feitz, W.F.; Frey, P. In-vivo performance of high-density collagen gel tubes for urethral regeneration in a rabbit model. Biomaterials 2012, 33, 7447–7455. [Google Scholar] [CrossRef] [PubMed]
- Chouhan, J.D.; Thakker, P.U.; Terlecki, R.P. Engineering of erectile tissue: The state and future of corporal restoration. World J. Urol. 2020, 38, 2109–2113. [Google Scholar] [CrossRef]
- An, G.; Ji, C.; Wei, Z.; Chen, H.; Zhang, J. Engineering of corpus cavernosum using vascular endothelial growth factor-expressing muscle-derived stem cells seeded on acellular corporal collagen matrices. Urology 2013, 81, 424–431. [Google Scholar] [CrossRef]
- An, G.; Guo, F.; Liu, X.; Wang, Z.; Zhu, Y.; Fan, Y.; Xuan, C.; Li, Y.; Wu, H.; Shi, X.; et al. Functional reconstruction of injured corpus cavernosa using 3D-printed hydrogel scaffolds seeded with HIF-1alpha-expressing stem cells. Nat. Commun. 2020, 11, 2687. [Google Scholar] [CrossRef]
- Sekar, M.P.; Budharaju, H.; Zennifer, A.; Sethuraman, S.; Vermeulen, N.; Sundaramurthi, D.; Kalaskar, D.M. Current standards and ethical landscape of engineered tissues-3D bioprinting perspective. J. Tissue Eng. 2021, 12, 20417314211027677. [Google Scholar] [CrossRef]
- Murphy, S.V.; Atala, A. 3D bioprinting of tissues and organs. Nat. Biotechnol. 2014, 32, 773–785. [Google Scholar] [CrossRef]
- Tan, Y.; Landford, W.N.; Garza, M.; Suarez, A.; Zhou, Z.; Coon, D. Complete Human Penile Scaffold for Composite Tissue Engineering: Organ Decellularization and Characterization. Sci. Rep. 2019, 9, 16368. [Google Scholar] [CrossRef] [PubMed]
- Saba, I.; Jakubowska, W.; Bolduc, S.; Chabaud, S. Engineering Tissues without the Use of a Synthetic Scaffold: A Twenty-Year History of the Self-Assembly Method. Biomed. Res. Int. 2018, 2018, 5684679. [Google Scholar] [CrossRef] [PubMed]
- Switzer, B.R.; Summer, G.K. Collagen synthesis in human skin fibroblasts: Effects of ascorbate, -ketoglutarate and ferrous ion on proline hydroxylation. J. Nutr. 1972, 102, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Hata, R.; Senoo, H. L-ascorbic acid 2-phosphate stimulates collagen accumulation, cell proliferation, and formation of a three-dimensional tissuelike substance by skin fibroblasts. J. Cell Physiol. 1989, 138, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Germain, L.; Larouche, D.; Nedelec, B.; Perreault, I.; Duranceau, L.; Bortoluzzi, P.; Beaudoin Cloutier, C.; Genest, H.; Caouette-Laberge, L.; Dumas, A.; et al. Autologous bilayered self-assembled skin substitutes (SASSs) as permanent grafts: A case series of 14 severely burned patients indicating clinical effectiveness. Eur. Cell Mater. 2018, 36, 128–141. [Google Scholar] [CrossRef] [PubMed]
- Le-Bel, G.; Guerin, L.P.; Carrier, P.; Mouriaux, F.; Germain, L.; Guerin, S.L.; Bazin, R. Grafting of an autologous tissue-engineered human corneal epithelium to a patient with limbal stem cell deficiency (LSCD). Am. J. Ophthalmol. Case Rep. 2019, 15, 100532. [Google Scholar] [CrossRef]
- Orabi, H.; Saba, I.; Rousseau, A.; Bolduc, S. Novel three-dimensional autologous tissue-engineered vaginal tissues using the self-assembly technique. Transl. Res. 2017, 180, 22–36. [Google Scholar] [CrossRef]
- Ringuette-Goulet, C.; Bolduc, S.; Pouliot, F. Modeling human bladder cancer. World J. Urol. 2018, 36, 1759–1766. [Google Scholar] [CrossRef]
- Bouhout, S.; Perron, E.; Gauvin, R.; Bernard, G.; Ouellet, G.; Cattan, V.; Bolduc, S. In vitro reconstruction of an autologous, watertight, and resistant vesical equivalent. Tissue Eng. Part A 2010, 16, 1539–1548. [Google Scholar] [CrossRef]
- Cattan, V.; Bernard, G.; Rousseau, A.; Bouhout, S.; Chabaud, S.; Auger, F.A.; Bolduc, S. Mechanical stimuli-induced urothelial differentiation in a human tissue-engineered tubular genitourinary graft. Eur. Urol. 2011, 60, 1291–1298. [Google Scholar] [CrossRef]
- Bouhout, S.; Gauvin, R.; Gibot, L.; Aube, D.; Bolduc, S. Bladder substitute reconstructed in a physiological pressure environment. J. Pediatr. Urol. 2011, 7, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Imbeault, A.; Bernard, G.; Rousseau, A.; Morissette, A.; Chabaud, S.; Bouhout, S.; Bolduc, S. An endothelialized urothelial cell-seeded tubular graft for urethral replacement. Can. Urol. Assoc. J. 2013, 7, E4–E9. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bouhout, S.; Chabaud, S.; Bolduc, S. Organ-specific matrix self-assembled by mesenchymal cells improves the normal urothelial differentiation in vitro. World J. Urol. 2016, 34, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Versteegden, L.R.; van Kampen, K.A.; Janke, H.P.; Tiemessen, D.M.; Hoogenkamp, H.R.; Hafmans, T.G.; Roozen, E.A.; Lomme, R.M.; van Goor, H.; Oosterwijk, E.; et al. Tubular collagen scaffolds with radial elasticity for hollow organ regeneration. Acta Biomater. 2017, 52, 1–8. [Google Scholar] [CrossRef]
- Caneparo, C.; Chabaud, S.; Fradette, J.; Bolduc, S. Engineered human organ-specific urethra as a functional substitute. Sci. Rep. 2022, 12, 21346. [Google Scholar] [CrossRef]
- Carrier, P.; Deschambeault, A.; Audet, C.; Talbot, M.; Gauvin, R.; Giasson, C.J.; Auger, F.A.; Guerin, S.L.; Germain, L. Impact of cell source on human cornea reconstructed by tissue engineering. Investig. Ophthalmol. Vis. Sci. 2009, 50, 2645–2652. [Google Scholar] [CrossRef]
- Jean, J.; Lapointe, M.; Soucy, J.; Pouliot, R. Development of an in vitro psoriatic skin model by tissue engineering. J. Dermatol. Sci. 2009, 53, 19–25. [Google Scholar] [CrossRef]
- Imbeault, A.; Bernard, G.; Ouellet, G.; Bouhout, S.; Carrier, S.; Bolduc, S. Surgical option for the correction of Peyronie’s disease: An autologous tissue-engineered endothelialized graft. J. Sex. Med. 2011, 8, 3227–3235. [Google Scholar] [CrossRef]
- Kumar, D.; Anand, T.; Kues, W.A. Clinical potential of human-induced pluripotent stem cells: Perspectives of induced pluripotent stem cells. Cell Biol. Toxicol. 2017, 33, 99–112. [Google Scholar] [CrossRef]
- Korneyev, I.; Ilyin, D.; Schultheiss, D.; Chapple, C. The first oral mucosal graft urethroplasty was carried out in the 19th century: The pioneering experience of Kirill Sapezhko (1857–1928). Eur. Urol. 2012, 62, 624–627. [Google Scholar] [CrossRef]
- Burger, R.A.; Muller, S.C.; el-Damanhoury, H.; Tschakaloff, A.; Riedmiller, H.; Hohenfellner, R. The buccal mucosal graft for urethral reconstruction: A preliminary report. J. Urol. 1992, 147, 662–664. [Google Scholar] [CrossRef]
- Dessanti, A.; Rigamonti, W.; Merulla, V.; Falchetti, D.; Caccia, G. Autologous buccal mucosa graft for hypospadias repair: An initial report. J. Urol. 1992, 147, 1081–1083; discussion 1083–1084. [Google Scholar] [CrossRef]
- Presman, D.; Greenfield, D.L. Reconstruction of the perineal urethra with a free full-thickness skin graft from the prepuce. J. Urol. 1953, 69, 677–680. [Google Scholar] [CrossRef]
- Barbagli, G.; Guazzoni, G.; Lazzeri, M. One-stage bulbar urethroplasty: Retrospective analysis of the results in 375 patients. Eur. Urol. 2008, 53, 828–833. [Google Scholar] [CrossRef]
- Wild, R.M.; Devine, C.J., Jr.; Horton, C.E. Dermal graft repair of Peyronie’s disease: Survey of 50 patients. J. Urol. 1979, 121, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Austoni, E.; Colombo, F.; Mantovani, F.; Patelli, E.; Fenice, O. Radical surgery and conservation of erection in Peyronie’s disease. Arch. Ital. Urol. Androl. 1995, 67, 359–364. [Google Scholar] [PubMed]
- Lue, T.F.; El-Sakka, A.I. Venous patch graft for Peyronie’s disease. Part I: Technique. J. Urol. 1998, 160, 2047–2049. [Google Scholar] [CrossRef] [PubMed]
- Helal, M.A.; Lockhart, J.L.; Sanford, E.; Persky, L. Tunica vaginalis flap for the management of disabling Peyronie’s disease: Surgical technique, results, and complications. Urology 1995, 46, 390–392. [Google Scholar] [CrossRef]
- Ulubay, M.; Akdeniz, E. The Effect of Autologous Temporal Fascia Graft on Erectile Function and Psychometric Properties in Peyronie’s Disease Patients. Urol. J. 2022, 20, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Saad, S.; Osman, N.I.; Chapple, C.R. Tissue engineering: Recent advances and review of clinical outcome for urethral strictures. Curr. Opin. Urol. 2021, 31, 498–503. [Google Scholar] [CrossRef] [PubMed]







| Perfusion | − − − | + | + | Native porcine urethra | ||
| Urothelial cells | − − − | − | + | |||
| Weeks | 2 | 3 | 4 | 3 + 1 | 3 + 1 | |
| Burst pressure (mmHg) | 803 | 1133 | 1801 | 1761 | 1703 | 418 |
| Native Urothelial Tissue | Reconstructed Urothelial Tissue (VF-Matrix) | Reconstructed Urothelial Tissue (VF:DF-Matrix) | Reconstructed Urothelial Tissue (DF-Matrix) | |
|---|---|---|---|---|
| Presence of cells | +++ | +++ | +++ | + |
| Differentiation of cells | +++ | +++ | +(+) | − |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elia, E.; Caneparo, C.; McMartin, C.; Chabaud, S.; Bolduc, S. Tissue Engineering for Penile Reconstruction. Bioengineering 2024, 11, 230. https://doi.org/10.3390/bioengineering11030230
Elia E, Caneparo C, McMartin C, Chabaud S, Bolduc S. Tissue Engineering for Penile Reconstruction. Bioengineering. 2024; 11(3):230. https://doi.org/10.3390/bioengineering11030230
Chicago/Turabian StyleElia, Elissa, Christophe Caneparo, Catherine McMartin, Stéphane Chabaud, and Stéphane Bolduc. 2024. "Tissue Engineering for Penile Reconstruction" Bioengineering 11, no. 3: 230. https://doi.org/10.3390/bioengineering11030230
APA StyleElia, E., Caneparo, C., McMartin, C., Chabaud, S., & Bolduc, S. (2024). Tissue Engineering for Penile Reconstruction. Bioengineering, 11(3), 230. https://doi.org/10.3390/bioengineering11030230