
The Accuracy of Algorithms Used by Artificial Intelligence in Cephalometric Points Detection: A Systematic Review



Abstract
1. Introduction
- Machine learning (ML) is a subset of AI and can be considered the central axis. Its functioning is based on the exposure to multiple sample data and their desired outcomes. This aims to “train” the algorithm, and through a set of probability and statistical tools, allows the machine to automatically detect new patterns and solve problems on its own [1,2,3].
- Deep learning (DL) is a part of machine learning. It seeks to mimic the human cognitive system by creating an artificial neural network with multiple layers, aiming to create a system that analyzes data and identifies more complex patterns than initially presented to improve its detection [2,4]. The learning method involves exposing the algorithm to pairs of data and their corresponding labels, such as relating a cephalometric point to its definition repetitively, so that it can predict the labeling of new data in the future [1]. While deep learning includes other types of models, such as recurrent neural networks (RNNs) for sequential data or transformers for language, CNNs are specifically designed to recognize spatial hierarchies in data, making them well-suited for tasks like image classification, object detection, and segmentation. Today, the most commonly used method for detection in radiological tests is CNN [1].
2. Materials and Methods
2.1. Focused Question
2.2. Eligibility Criteria
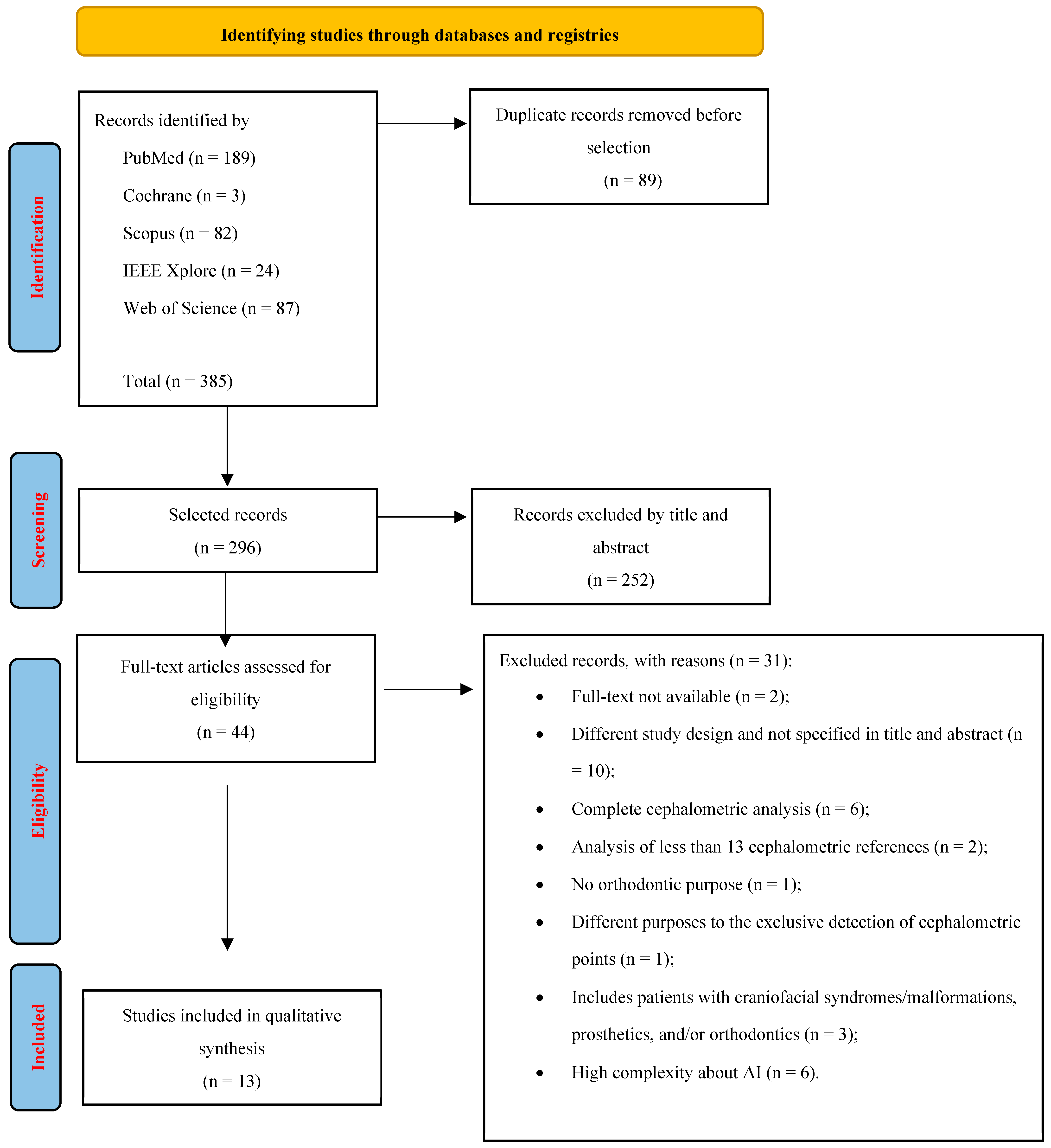
2.3. Search Strategy and Information Sources
2.4. Study Selection and Data Extraction
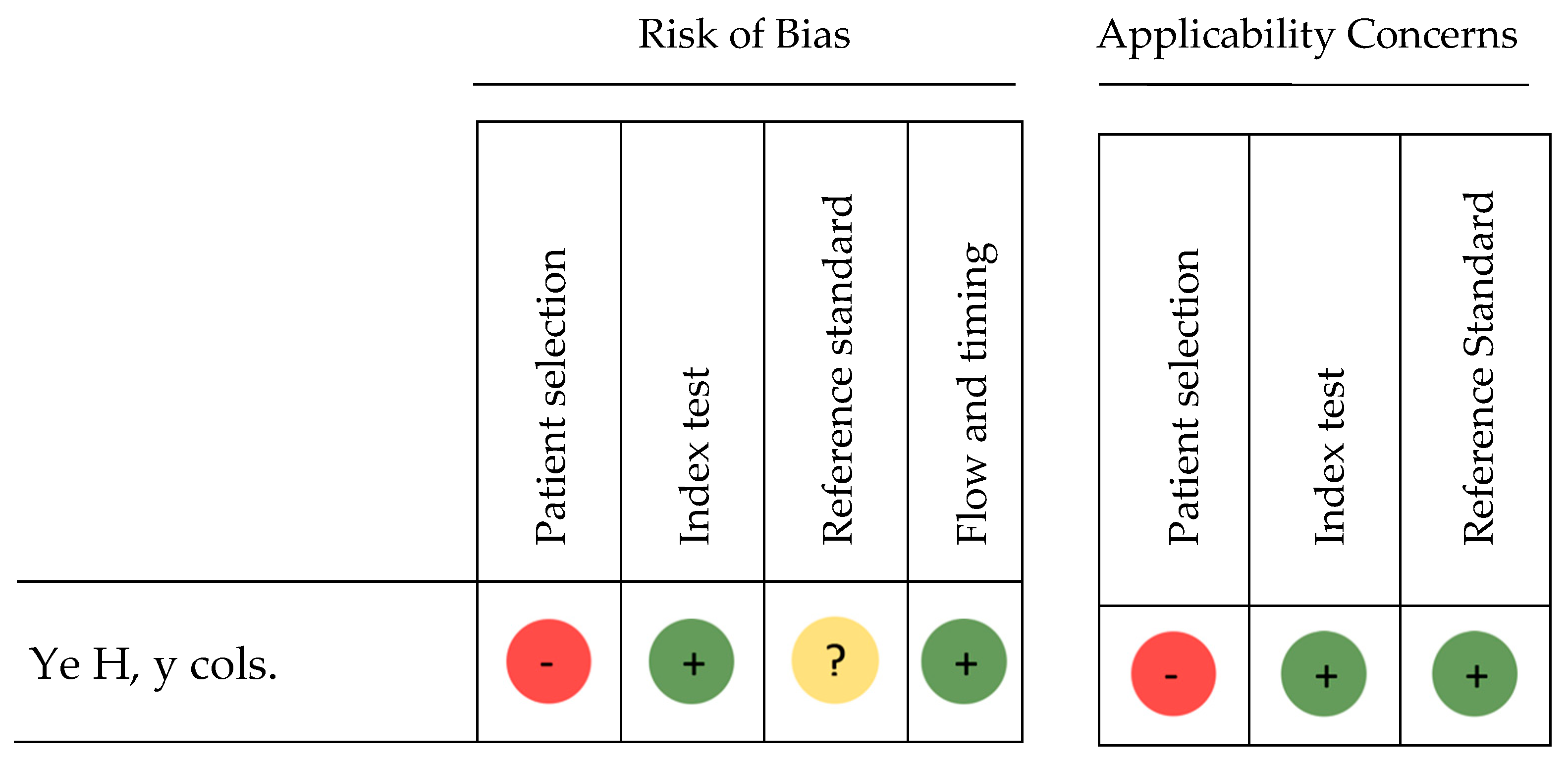
2.5. Risk of Bias
3. Results
3.1. Study Selection
3.2. Risk of Bias Assessment for Diagnostic Accuracy Studies
3.3. Risk of Bias Assessment for Cohort Observational Studies
3.4. Data Extraction: Qualitative Synthesis
4. Discussion
4.1. Limitations
4.2. Future Investigations
5. Conclusions
- Our findings suggest that CNNs represent the most promising AI form for detecting cephalometric landmarks in 2D lateral cranial teleradiography, offering lower error rates and higher reproducibility compared to other AI types reviewed.
- However, due to significant heterogeneity in study designs, data collection, and performance metrics, a definitive quantitative comparison was not feasible
- While AI demonstrates faster and more reproducible results than manual tracing, no algorithms currently match the precision of human professionals.
- Future research should aim to standardize evaluation criteria and datasets to enable a more robust comparison of AI methods.
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A. Data Collection Tables

{kind=link}
{kind=link}
| Author Origin Year | Study Design | Originating Institution | Objectives | Number of Participants Age Gender Other |
|---|---|---|---|---|
| Kim YH, et al. [58] Korea 2021 | RCC | Yonsei University Dental Hospital | Testing fully automatic point localization model based on CNN | 950 RX Age: - Gender: - |
| Kim J, et al. [51] Korea 2021 | RCC | 10 university hospitals in South Korea | Investigating the accuracy of automated identification of lateral cephalometric points using RetinaNet as CNN | 3.150 RX Age: - Gender: - |
| Bulatova G, et al. [52] USA 2021 | RCC | College of Dentistry, University of Illinois | Comparing the accuracy of CNN-based YOLOv3 algorithm with manual localization performed by experts | 110 RX Age: - Gender: - |
| Santos Menezes L, et al. [53] Brazil 2023 | RCC | Federal University of Bahia, Piracicaba Dental School, University of Campinas, University of São Paulo, Federal University of Sergipe, Brazil | Evaluation of CEFBOT AI software to identify cephalometric points in four brightness and contrast conditions | 30 RX Age: >18 years old Gender: - Others: without serious craniofacial deformities and asymmetries, unerupted incisors and teeth impacted on the apex of the incisors. |
| Lee J, et al. [10] Korea 2020 | RCC | Ewha Womans University Medical Center Seoul | Testing a BCNN-based model for cephalometric landmark localization with uncertainty-based confidence regions | 400 RX (ISBI public data IEEE 2015) Age: 6 to 60 years old Gender: - |
| Yao J, et al. [55] China 2021 | RCC | West China School of Stomatology, Sichuan University | Developing a new system for the automatic localization of cephalometric points, based on CNN | 512 RX Age: 9 to 40 years old Gender: 247 men, 265 women Others: No patients with absent, atypical or missing central incisors, molars, orthodontic wearers, cleft lip or palate, maxillofacial trauma or candidates for surgery or implants. |
| Zhao C, et al. [54] China 2023 | RCC | Jiading Central Hospital, Shanghai University of Medicine and Health Sciences | Evaluation of the MS-YOLOv3 algorithm for automatic landmark detection, and quantitative and qualitative comparison with YOLOV3 | 400 RX (ISBI public data IEEE 2014) Age: 6 to 60 years old Gender: - |
| Ristau B, et al. [50] USA 2022 | RCC | Louisiana State University School of Dentistry, New Orleans | Comparing the reliability of AudaxCeph for identifying cephalometric landmarks with human trackers | 60 RX Age: - Gender: - Others: Complete dentition, without craniofacial abnormalities, asymmetries or significant double borders of the mandible |
| Ramadan R, et al. [49] Saudi Arabia 2022 | RCC | Faculty of Engineering and Computer Science, Ha’il University Faculty of Computing and Artificial Intelligence, Benha University Department of Computer Engineering, Balkan International University, | Testing deep learning model based on centroid registration and ResNet50 | 400 RX (ISBI public data IEEE 2015) Age: 7 to 76 years old Gender: 235 women, 165 men |
| Hwang H, et al. [59] South Korea 2021 | RCC | Seoul National University Dental Hospital | To compare and evaluate fully automated cephalometric point localization based on a new form of YOLOv3 with manual tracing | 2.183 RX Age: - Gender: - |
| Ye H, et al. [48] China 2023 | RCT | Chongqing Medical University | Compare the accuracy of automatic or AI-assisted program layout; MyOrthoX, Angelalign and Digident with manual localization | 33 RX Age: - Gender: - Others: No patients with cleft lip and palate, systemic diseases or craniofacial syndromes |
| Uğurlu M [56] Türkiye 2022 | RCC | Faculty of Dentistry, Eskişehir Osmangazi University | Develop AI model (CranioCatch) for automatic detection of cephalometric points | 1.620 RX Age: 9 to 20 years old Gender: - |
| Davidovitch M, et al. [57] Israel 2022 | RCC | University Orthodontic Clinic Tel Aviv University | Evaluation of automatic recognition of cephalometric points by the Algoceph convolutional neural network (CNN) artificial intelligence system | 10 RX Age: - Gender: - Other: No congenital craniofacial/dental anomalies or facial trauma |
| INTERVENTION | OUTCOMES | ||||||
|---|---|---|---|---|---|---|---|
| Algorithm Learning Method | Cephalometric Landmarks: Number Location | Images: Training Validation Test | Gold Standard | SDR Clinical Range 2 mm | MRE +/- SD | Others | |
| Kim YH, et al. [58] | ROI machine; detecting areas of interest with points, and detection machine to predict coordinates CNN, DL | 13 points Hard tissue | 800 training 100 validation 50 test | ML performed by 2 orthodontists with 15 and 5 years of experience | Mean SDR: 64.3% Cephalometric point with the highest success rate: UIB y LIB 78.7% Cephalometric point with the lowest success rate: Ar 46.7% | Mean MRE: - Cephalometric point with the highest mean error: S 2.39 mm Cephalometric point with the lowest mean error: UIB 1.36 mm | - |
| Kim J, et al. [51] | Fully automated prediction algorithm based on 2 phases: Region of Interest (ROI) detection and landmark prediction CNN, DL | 20 points Hard tissue | 1.392 training 1218 additional training and development 440 validation 100 test | ML performed by 2 orthodontists with 30 and 10 years of experience | Mean SDR: 83.6% Cephalometric point with the highest success rate: S 100% Cephalometric point with the lowest success rate: Mx6 root 65% | Mean MRE: 1.36 mm +/- 0.98 Cephalometric point with the highest mean error: Md6 distal 2.09 mm +/- 1.91 Cephalometric point with the lowest mean error: Crown Mx1 0.46 mm +/- 0.37 | SDR clinical range 0–1 mm Mean SDR: 56.55% Cephalometric point with the highest success rate: S 98% Cephalometric point with the lowest success rate: B 26% |
| Bulatova G, et al. [52] | YOLO version 3 CNN, DL | 16 points Hard tissue | - No algorithm development | ML performed by 2 orthodontists | - | - | Absolute difference between AI and MT according to X, Y coordinate axes p > 0.05 (no significative diference): 75% points p < 0.05 (significative diference): 25% points Eje X: Point that differs the most: Go absolute value 8.7 +/- 9 Point that differs the least: Na absolute value 1.4 +/- 3.9 Eje Y: Point of greatest difference: L1apex absolute value 5.4 +/- 2.9 Point that differs the least: Na absolute value 1.3 +/- 2.7 |
| Santos Menezes L, et al. [53] | CEFBOT CNN, DL | 19 points 15 Hard tissue 4 Soft tissue | - No algorithm development | ML performed by 2 examiners, ECont (control) and ECal (calibration) | - | - | Reliability. Mean ICC between AI and MT for four brightness and contrast settings: X axis: ICC > 0.93 (very good). Best outcome AI with V3, worst with V4. Y axis: ICC > 0.89 (good). Best outcome AI with V3, worst with V4. Reproducibility. p < 0.05 between AI and MT for four brightness and contrast settings: X axis: Point with highest error: Po (p < 0.001) in V1, V2, V3, V4, V5. Point with lowest error: V1 Pog (p: 0.949); V2 Ll (p: 0.897); V3 Go (p: 0.978); V4 B (p: 0.991); V5 S (p: 0.994) Y axis: Point with highest error: Sn (p < 0.004) in V1. En V2, V3, V4, V5 all the point p > 0.05. Point with lowest error: V1 Lis (p: 0.974); V2 Ar (p: 0.949); V3 Pog (p: 0.952); V4 Ll (p: 0.985); V5 Po (p: 1.00) |
| Lee J, et al. [10] | BCNN-based model CNN, DL | 19 points 15 Hard tissue 4 Soft tissue | 150 training - validation 250 test | ML carried out by two expert specialists in orthodontics, junior and senior | Mean SDR: 82.11% Cephalometric point with the highest success rate: Ll 97.33% Cephalometric point with the lowest success rate: A point 52% | Mean MRE: 1.53 mm +/- 1.74 Cephalometric point with the highest mean error: Pog’ 2.62 mm +/- 2.07 Cephalometric point with the lowest mean error: S 0.86 mm +/- 1.92 | - |
| Yao J, et al. [55] | Algorithm based on a global detection module and a locally modified module CNN, DL | 37 points 26 Hard tissue 11 Soft tissue | 312 training 100 validation 100 test | ML performed by two expert orthodontic specialists | Mean SDR: 97.30% Cephalometric point with the highest success rate: Mes 100% Cephalometric point with the lowest success rate: Go and Pt 65% | Mean MRE: 1.04 mm+/- 0.89 Cephalometric point with the highest mean error: Pog’ 2.03 mm +/- 5.95 Cephalometric point with the lowest mean error: Prn 0.5 mm +/- 0.32 | SDR clinical range 1 mm Mean SDR: 54.05% Cephalometric point with the highest success rate: Prn 94% Cephalometric point with the lowest success rate: Pt 27% |
| Zhao C, et al. [54] | Multi-Scale YOLOV3 CNN, DL | 19 points 15 Hard tissue 4 Soft tissue | 1950 training ¿? - validation 150 test | Automatic localization performed by the classic YOLOv3 | Mean SDR MS-YOLOv3: 80% Cephalometric point with the highest success rate: S and PNS 95.33% Cephalometric point with the lowest success rate: Go 55.33% Mean SDR YOLOv3: 76.55% Cephalometric point with the highest success rate: S 91.33% Cephalometric point with the lowest success rate: Go 52% | Mean MRE MS-YOLOv3: - Cephalometric point with the highest mean error: Go 2.43 mm +/- 1.56 Cephalometric point with the lowest mean error: Pog’ 1.13 mm +/- 0.62 Mean MRE YOLOv3: - Cephalometric point with the highest mean error: Pog’ 3.25 mm +/- 1.79 Cephalometric point with the lowest mean error: ANS 1.46 mm +/- 0.97 | - |
| Ristau B, et al. [50] | AudaxCeph CNN, DL | 13 points Hard tissue | - No algorithm development | ML performed by 2 orthodontists with 31 and 34 years of experience | - | - | Mean difference Reviewer-AudaxCeph X, Y axis (mean + SD of error) (regarding p > 0.05) X axis: Deviation AI: Po 2.6 mm +/- 2.1. p = 0.88. Y axis: Deviation AI: L1 apex 2.0 mm +/- 1.3. p = 0.46. Or 1.8 +/- 1.2 p = 0.11, Po 2.3 mm +/- 2.2 p = 0.36 Difference Reviewer- AudaxCeph X, Y axis (%) X axis: Po 35.8% Y axis: L1 apex 40% |
| Ramadan R, et al. [49] | CNN-based model creating ROIs (regions of interest) and feature extraction with ResNet50 CNN, DL | 19 points 15 Hard tissue 4 Soft tissue | 150 training 250 test (150 testset, 100 testset2) | ML performed by two expert orthodontic specialists | Mean SDR Testset 1: 90.39% Cephalometric point with the highest success rate: S 98% Cephalometric point with the lowest success rate: A point 70.1% Mean SDR Testset 2: 82.66% Cephalometric point with the highest success rate: S and upper incisal edge 97.2% Cephalometric point with the lowest success rate: Ll 25.4% | Mean MRE Testset 1: 1.23 mm +/- 0.73 Cephalometric point with the highest mean error: A point 2.1 mm +/- 1.43 Cephalometric point with the lowest mean error: S 0.33 mm +/- 0.12 Mean MRE Testset 2: 1.37 +/- 0.88 mm Cephalometric point with the highest mean error: Ll 3.51 mm +/- 2.01 Cephalometric point with the lowest mean error: Upper incisor edge 0.32 mm +/- 0.22 | |
| Hwang H, et al. [59] | YOLO version 3 CNN, DL | 19 points 15 Hard tissue 4 Soft tissue | 1.983 training 200 test | ML performed by 1 examiner with 30 years of experience | Mean SDR: 75.45% Cephalometric point with the highest success rate: S 96% Cephalometric point with the lowest success rate: Go 38% | Mean MRE: 1.76 mm +/- 2.16 Cephalometric point with the highest mean error: Or 2.84 mm +/- 5.91 Cephalometric point with the lowest mean error: Ll 1.04 mm +/- 0.60 | |
| Ye H, et al. [48] | MyOrthoX Angelalign Digident CNN, DL | 32 points 21 Hard tissue 11 Soft tissue | - No algorithm development | ML performed by an orthodontist, and verified by 2 more orthodontists | Mean SDR Angelalign: 93.09% Cephalometric point with the highest success rate: Sn, Ul, Ll, Si, Pog’, Me’, Gn’, S, Ptm, U1, Pog, Gn, Me 98% Cephalometric point with the lowest success rate: Po and Pt 79% Mean SDR MyOrthoX: 89.99% Cephalometric point with the highest success rate: Gn, Sn, Pog’, Gn’, S, PNS, Pog 100% Cephalometric point with the lowest success rate: UIA 35% Mean SDR Digident: 87.53% Cephalometric point with the highest success rate: Ul, Ll, Pog’, S, PNS, Pog, Gn, Me, Pcd 100% Cephalometric point with the lowest success rate: ANS 35% | Mean MRE Angelalign: 0.80 mm +/- 0.26 Cephalometric point with the highest mean error: Pt 1.49 mm +/- 1.24 Cephalometric point with the lowest mean error: Go 0.46 mm +/- 0.54 Mean MRE MyOrthoX: 0.97 mm +/- 0.51 Cephalometric point with the highest mean error: UIA 2.39 mm +/- 1.05 Cephalometric point with the lowest mean error: Sn 0.55 mm +/- 0.32 Mean MRE Digident: 1.11 mm +/- 0.48 Cephalometric point with the highest mean error: Prn 2.34 mm +/- 1.57 Cephalometric point with the lowest mean error: Gn 0.43 mm +/- 0.29 | SDR clinical range <1 mm: Mean SDR Angelalign: 78.08% Cephalometric point with the highest success rate: Go 98% Cephalometric point with the lowest success rate: Pt 40% Mean SDR MyOrthoX: 67.02% Cephalometric point with the highest success rate: Sn 91% Cephalometric point with the lowest success rate:UIA 5% Mean SDR Digident: 59.13% Cephalometric point with the highest success rate: Pog, Me 95% Cephalometric point with the lowest success rate: Prn 19% Mean time Manual group: 153.47 s +/- 14.83 AI group: Angelalign: 5.18 s +/- 0.19. MyOrthoX: 1.08 s +/- 0.12. Digident: 5.60 s +/- 0.20 |
| Uğurlu M [56] | CranioCatch CNN, DL | 21 points 17 Hard tissue 4 Soft tissue | 1.360 training 140 validation 180 test | ML performed by 1 examiner with 9 years of experience | Mean SDR: 76.2% Cephalometric point with the highest success rate: S 98.3% Cephalometric point with the lowest success rate: Go 48.3% | Mean MRE: 3.40 mm +/- 1.57 Cephalometric point with the highest mean error: Go 8.30 mm +/- 2.98 Cephalometric point with the lowest mean error: S 0.62 mm +/- 0.43 | |
| Davidovitch M, et al. [57] | Algoceph CNN, DL | 21 points 15 Hard tissue 6 Soft tissue | - No algorithm development | ML performed by 7 orthodontic teachers, 9 3rd year residents and 10 1st year residents, and 4 technicians from the imaging center | Mean SDR: 85.72% | Mean MRE: - Cephalometric point with the highest mean error: Pog’ in Y axis 2.67 +/- 2.55 mm Cephalometric point with the lowest mean error: Soft nose 0.01 mm +/- 0.75 and B point 0.01 +/- 0.65 mm in Y axis. | Significant difference in points between AI and MT according to X, Y coordinate axes X axis: Or 1.07 mm +/- 1.29, Ptm 0.99 mm +/- 0.98, Ba 1.03 mm +/- 0.90 Y axis: Pog’ 2.67 mm +/- 2.55, Ul 1.11 mm +/- 1.16, Po 1.14 mm +/- 1.41 |
References
- Kiełczykowski, M.; Kamiński, K.; Perkowski, K.; Zadurska, M.; Czochrowska, E. Application of Artificial Intelligence (AI) in a Cephalometric Analysis: A Narrative Review. Diagnostics 2023, 13, 2640. [Google Scholar] [CrossRef]
- Monill-González, A.; Rovira-Calatayud, L.; d’Oliveira, N.G.; Ustrell-Torrent, J.M. Artificial intelligence in orthodontics: Where are we now? A scoping review. Orthod. Craniofacial Res. 2021, 24, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.G.; Jun, S.; Cho, Y.W.; Lee, H.; Kim, G.B.; Seo, J.B.; Beom, J.; Kim, N. Deep Learning in Medical Imaging: General Overview. Korean J. Radiol. 2017, 18, 570. [Google Scholar] [CrossRef]
- Bichu, Y.M.; Hansa, I.; Bichu, A.Y.; Premjani, P.; Flores-Mir, C.; Vaid, N.R. Applications of artificial intelligence and machine learning in orthodontics: A scoping review. Prog. Orthod. 2021, 22, 18. [Google Scholar] [CrossRef] [PubMed]
- Kaul, V.; Enslin, S.; Gross, S.A. History of artificial intelligence in medicine. Gastrointest. Endosc. 2020, 92, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Malik, P.A.; Pathania, M.; Rathaur, V.K. Overview of artificial intelligence in medicine. J. Fam. Med. Prim. Care 2019, 8, 2328–2331. [Google Scholar]
- Wong, K.F.; Lam, X.Y.; Jiang, Y.; Yeung, A.W.K.; Lin, Y. Artificial intelligence in orthodontics and orthognathic surgery: A bibliometric analysis of the 100 most-cited articles. Head Face Med. 2023, 19, 38. [Google Scholar] [CrossRef]
- Yamashiro, T.; Ko, C.C. Artificial intelligence and machine learning in orthodontics. Orthod. Craniofacial Res. 2021, 24, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Le, V.N.T.; Kang, J.; Oh, I.S.; Kim, J.G.; Yang, Y.M.; Lee, D.W. Effectiveness of Human-Artificial Intelligence Collaboration in Cephalometric Landmark Detection. J. Pers. Med. 2022, 12, 387. [Google Scholar] [CrossRef]
- Lee, J.H.; Yu, H.J.; Kim, M.J.; Kim, J.W.; Choi, J. Automated cephalometric landmark detection with confidence regions using Bayesian convolutional neural networks. BMC Oral Health 2020, 20, 270. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Shim, E.; Park, J.; Kim, Y.J.; Lee, U.; Kim, Y. Web-based fully automated cephalometric analysis by deep learning. Comput. Methods Programs Biomed. 2020, 194, 105513. [Google Scholar] [CrossRef]
- Leonardi, R.; Giordano, D.; Maiorana, F.; Spampinato, C. Automatic Cephalometric Analysis a Systematic Review. Angle Orthod. 2008, 78, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.; Suhail, Y.; Nelson, J.; Upadhyay, M. Artificial Intelligence for radiographic image analysis. Semin. Orthod. 2021, 27, 109–120. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, C.; Shan, Z.; Liu, J.; Zhang, C.; Shan, Z. Application of Artificial Intelligence in Orthodontics, Current State and Future Perspectives. Healthcare 2023, 11, 2760. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses, the PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2014. [Google Scholar]
- Wang, C.W.; Huang, C.T.; Hsieh, M.C.; Li, C.H.; Chang, S.W.; Li, W.C.; Remy, V.; Raphael, M.; Sebastien, J.; Pierre, G.; et al. Evaluation and Comparison of Anatomical Landmark Detection Methods for Cephalometric X-Ray Images: A Grand Challenge. IEEE Trans. Med. Imaging 2015, 34, 1890–1900. [Google Scholar] [CrossRef]
- Hwang, H.W.; Park, J.H.; Moon, J.H.; Yu, Y.; Kim, H.; Her, S.B.; Srinivasan, G.; Aljanabi, M.N.; Donatelli, R.E.; Lee, S.J. Automated identification of cephalometric landmarks, Part 2-Might it be better than human? Angle Orthod. 2020, 90, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Gong, B.W.; Chang, S.; Zuo, F.F.; Xie, X.J.; Wang, S.F.; Wang, Y.J.; Sun, Y.Y.; Guan, X.C.; Bai, Y.X. Automated cephalometric landmark identification and location based on convolutional neural network. Zhonghua Kou Qiang Yi Xue Za Zhi 2023, 58, 1249–1256. [Google Scholar] [PubMed]
- Moreno, M.; Gebeile-Chauty, S. Comparative study of two software for the detection of cephalometric landmarks by artificial intelligence. L’Orthodontie Française 2022, 93, 41–61. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Che, H.; Sun, J.; Rao, Y.; Wu, J. An automatic cephalometric landmark detection method based on heatmap regression and Monte Carlo dropout. In Proceedings of the 2023 45th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Sydney, Australia, 24–27 July 2023; pp. 1–4. [Google Scholar]
- King, C.H.; Wang, Y.L.; Lin, W.Y.; Tsai, C.L. Automatic Cephalometric Landmark Detection on X-Ray Images Using Object Detection. In Proceedings of the 2022 IEEE 19th International Symposium on Biomedical Imaging (ISBI), Kolkata, India, 28–31 March 2022; pp. 1–4. [Google Scholar]
- Du, D.; Ren, T.; Chen, C.; Jiang, Y.; Song, G.; Li, Q.; Niu, J. Anatomical Landmarks Annotation on 2D Lateral Cephalograms with Channel Attention. In Proceedings of the 2022 22nd IEEE International Symposium on Cluster, Cloud and Internet Computing (CCGrid), Taormina, Italy, 16–19 May 2022; pp. 279–288. [Google Scholar]
- Fajar, A.; Pangestu, G.; Sarno, R.; Ardani, I.G.A.W. Cephalometric Landmark Detection on Cephalograms using Regression CNN. In Proceedings of the 2022 5th International Conference on Information and Communications Technology (ICOIACT), Yogyakarta, Indonesia, 24–25 August 2022; pp. 150–154. [Google Scholar]
- Rashmi, S.; Srinath, S.; Rakshitha, R.; Poornima, B.V. Extended Template Matching method for Region of Interest Extraction in Cephalometric Landmarks Annotation. In Proceedings of the 2022 IEEE 9th Uttar Pradesh Section International Conference on Electrical, Electronics and Computer Engineering (UPCON), Allahabad, India, 2–4 December 2022; pp. 1–6. [Google Scholar]
- Song, Y.; Qiao, X.; Iwamoto, Y.; Chen, Y.W. A Teacher-Student Learning Based On Composed Ground-Truth Images For Accurate Cephalometric Landmark Detection. In Proceedings of the 2021 IEEE International Conference on Image Processing (ICIP), Anchorage, AK, USA, 19–22 September 2021; pp. 3777–3781. [Google Scholar]
- Reddy, P.K.; Kanakatte, A.; Gubbi, J.; Poduval, M.; Ghose, A.; Purushothaman, B. Anatomical Landmark Detection using Deep Appearance-Context Network. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; pp. 3569–3572. [Google Scholar]
- Zhang, Q.; Guo, J.; He, T.; Yao, J.; Tang, W.; Yi, Z. A Novel Landmark Detection Method for Cephalometric Measurement. In Proceedings of the 2021 IEEE International Conference on Medical Imaging Physics and Engineering (ICMIPE), Hefei, China, 12–14 November 2021; pp. 1–10. [Google Scholar]
- Goutham, E.N.D.; Vasamsetti, S.; Kishore, P.V.V.; Sardana, H.K. Automatic Localization of Landmarks in Cephalometric Images Via Modified U-Net. In Proceedings of the 2019 10th International Conference on Computing, Communication and Networking Technologies (ICCCNT), Kanpur, India, 6–8 July 2019; pp. 1–6. [Google Scholar]
- Tabata, L.C.; Nyirenda, C.N.; Faster, R.-C.N.N. Based Cephalometric Landmarks Detection. In Proceedings of the 2021 IEEE AFRICON, Arusha, Tanzania, 13–15 September 2021; pp. 1–6. [Google Scholar]
- El-Dawlatly, M.; Attia, K.H.; Abdelghaffar, A.Y.; Mostafa, Y.A.; Abd El-Ghafour, M. Preciseness of artificial intelligence for lateral cephalometric measurements. J. Orofac. Orthop. 2024, 85, 27–33. [Google Scholar] [CrossRef]
- Lee, J.; Bae, S.R.; Noh, H.K. Commercial artificial intelligence lateral cephalometric analysis: Part 1—The possibility of replacing manual landmarking with artificial intelligence service. J. Clin. Pediatr. Dent. 2023, 47, 106–118. [Google Scholar]
- Lee, J.; Bae, S.R.; Noh, H.K. Commercial artificial intelligence lateral cephalometric analysis: Part 2—Effects of human examiners on artificial intelligence performance, a pilot study. J. Clin. Pediatr. Dent. 2023, 47, 130–141. [Google Scholar] [PubMed]
- Jeon, S.; Lee, K.C. Comparison of cephalometric measurements between conventional and automatic cephalometric analysis using convolutional neural network. Prog. Orthod. 2021, 22, 14. [Google Scholar] [CrossRef] [PubMed]
- Vithanaarachchi, N.; Chandrasiri, A.; Nawarathna, L. A comparison of cephalometric measurements obtained using conventional and digital methods. Ceylon Med. J. 2020, 65, 39–45. [Google Scholar] [CrossRef]
- Kang, S.; Kim, I.; Kim, Y.J.; Kim, N.; Baek, S.H.; Sung, S.J. Accuracy and clinical validity of automated cephalometric analysis using convolutional neural networks. Orthod. Craniofacial Res. 2024, 27, 64–77. [Google Scholar] [CrossRef]
- Kumar, M.; Kumari, S.; Chandna, A.; Singh, A.; Kumar, K.; Punita, H. Comparative Evaluation of CephNinja for Android and NemoCeph for Computer for Cephalometric Analysis: A Study to Evaluate the Diagnostic Performance of CephNinja for Cephalometric Analysis. J. Int. Soc. Prev. Community Dent. 2020, 10, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Nishimoto, S.; Sotsuka, Y.; Kawai, K.; Ishise, H.; Kakibuchi, M. Personal computer-based cephalometric landmark detection with deep learning, using cephalograms on the internet. J. Craniofacial Surg. 2019, 30, 91–95. [Google Scholar] [CrossRef]
- Gomez-Trenado, G.; Mesejo, P.; Cordon, O. Cascade of convolutional models for few-shot automatic cephalometric landmarks localization. Eng. Appl. Artif. Intell. 2023, 123, 106391. [Google Scholar] [CrossRef]
- Oh, K.; Oh, I.S.; Le, V.N.T.; Lee, D.W. Deep Anatomical Context Feature Learning for Cephalometric Landmark Detection. IEEE J. Biomed. Health Inform. 2021, 25, 806–817. [Google Scholar] [CrossRef]
- Park, J.H.; Hwang, H.W.; Moon, J.H.; Yu, Y.; Kim, H.; Her, S.B.; Girish, S.; Noori, A.A.M.; Richard, E.D.; Lee, S.-J. Automated identification of cephalometric landmarks: Part 1—Comparisons between the latest deep-learning methods YOLOV3 and SSD. Angle Orthod. 2019, 89, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Guo, Y.; Yang, C.; Zhou, Y.; Lin, Y.; Cheng, F.; Shuqi, Q.; Qingchen, F.; Li, J. Artificial intelligence system for automated landmark localization and analysis of cephalometry. Dentomaxillofacial Radiol. 2023, 52, 20220081. [Google Scholar] [CrossRef]
- Wang, X.; Rigall, E.; Chen, Q.; Zhang, S.; Dong, J. Efficient and Stable Cephalometric Landmark Localization Using Two-Stage Heatmaps’ Regression. IEEE Trans. Instrum. Meas. 2022, 71, 1–16. [Google Scholar] [CrossRef]
- Lu, G.; Zhang, Y.; Kong, Y.; Zhang, C.; Coatrieux, J.L.; Shu, H. Landmark Localization for Cephalometric Analysis Using Multiscale Image Patch-Based Graph Convolutional Networks. IEEE J. Biomed. Health Inform. 2022, 26, 3015–3024. [Google Scholar] [CrossRef]
- Qian, J.; Luo, W.; Cheng, M.; Tao, Y.; Lin, J.; Lin, H. CephaNN: A Multi-Head Attention Network for Cephalometric Landmark Detection. IEEE Access 2020, 8, 112633–112641. [Google Scholar] [CrossRef]
- Neeraja, R.; Anbarasi, L.J. CephXNet: A Deep Convolutional Squeeze-and-Excitation Model for Landmark Prediction on Lateral Cephalograms. IEEE Access 2023, 11, 90780–90800. [Google Scholar] [CrossRef]
- Ye, H.; Cheng, Z.; Ungvijanpunya, N.; Chen, W.; Cao, L.; Gou, Y. Is automatic cephalometric software using artificial intelligence better than orthodontist experts in landmark identification? BMC Oral Health 2023, 23, 467. [Google Scholar] [CrossRef]
- Ramadan, R.A.; Khedr, A.Y.; Yadav, K.; Alreshidi, E.J.; Sharif, M.H.; Azar, A.T.; Kamberaj, H. Convolution neural network based automatic localization of landmarks on lateral x-ray images. Multimed. Tools Appl. 2022, 81, 37403–37415. [Google Scholar] [CrossRef]
- Ristau, B.; Coreil, M.; Chapple, A.; Armbruster, P.; Ballard, R. Comparison of AudaxCeph®’s fully automated cephalometric tracing technology to a semi-automated approach by human examiners. Int. Orthod. 2022, 20, 100691. [Google Scholar] [CrossRef]
- Kim, J.; Kim, I.; Kim, Y.J.; Kim, M.; Cho, J.H.; Hong, M.; Kyung-Hwa, K.; Sung-Hoon, L.; Su-Jung, K.; Ho, K.Y.; et al. Accuracy of automated identification of lateral cephalometric landmarks using cascade convolutional neural networks on lateral cephalograms from nationwide multi-centres. Orthod. Craniofacial Res. 2021, 24, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Bulatova, G.; Kusnoto, B.; Grace, V.; Tsay, T.P.; Avenetti, D.M.; Sanchez, F.J.C. Assessment of automatic cephalometric landmark identification using artificial intelligence. Orthod. Craniofacial Res. 2021, 24, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Santos Menezes, L.D.; Silva, T.P.; Lima dos Santos, M.A.; Hughes, M.M.; Reis Mariano Souza, S.D.; Leite Ribeiro, P.M.; Luiz, F.P.H.; Takeshita, W.M. Assessment of landmark detection in cephalometric radiographs with different conditions of brightness and contrast using the an artificial intelligence software. Dentomaxillofacial Radiol. 2023, 52, 20230065. [Google Scholar] [CrossRef]
- Zhao, C.Y.; Yuan, Z.B.; Luo, S.C.; Wang, W.J.; Ren, Z.; Yao, X.F.; Wu, T. Automatic recognition of cephalometric landmarks via multi-scale sampling strategy. Heliyon 2023, 9, 17459. [Google Scholar] [CrossRef]
- Yao, J.; Zeng, W.; He, T.; Zhou, S.; Zhang, Y.; Guo, J.; Tang, W. Automatic localization of cephalometric landmarks based on convolutional neural network. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Uğurlu, M. Performance of a Convolutional Neural Network—Based Artificial Intelligence Algorithm for Automatic Cephalometric Landmark Detection. Turk. J. Orthod. 2022, 35, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Davidovitch, M.; Sella-Tunis, T.; Abramovicz, L.; Reiter, S.; Matalon, S.; Shpack, N. Verification of convolutional Neural Network Cephalometric Landmark Identification. Appl. Sci. 2022, 12, 12784. [Google Scholar] [CrossRef]
- Kim, Y.H.; Lee, C.; Ha, E.G.; Choi, Y.J.; Han, S.S. A fully deep learning model for the automatic identification of cephalometric landmarks. Imaging Sci. Dent. 2021, 51, 299. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.W.W.; Moon, J.H.H.; Kim, M.G.G.; Donatelli, R.E.E.; Lee, S.J.J. Evaluation of automated cephalometric analysis based on the latest deep learning method. Angle Orthod. 2021, 91, 329–335. [Google Scholar] [CrossRef]
- Hwang, J.J.; Jung, Y.H.; Cho, B.H.; Heo, M.S. An overview of deep learning in the field of dentistry. Imaging Sci. Dent. 2019, 49, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Durão, A.P.R.; Morosolli, A.; Pittayapat, P.; Bolstad, N.; Ferreira, A.P.; Jacobs, R. Cephalometric landmark variability among orthodontists and dentomaxillofacial radiologists: A comparative study. Imaging Sci. Dent. 2015, 45, 213–220. [Google Scholar] [CrossRef]
- Miloro, M.; Borba, A.M.; Ribeiro-Junior, O.; Naclério-Homem, M.G.; Jungner, M. Is there consistency in cephalometric landmark identification amongst oral and maxillofacial surgeons? Int. J. Oral Maxillofac. Surg. 2014, 43, 445–453. [Google Scholar] [CrossRef]
| PICO Question for Inclusion Criteria | |
|---|---|
| P (Population) | Orthodontic patients with lateral cranial radiographs (2D) |
| I (Intervention) | Automatic detection of cephalometric landmarks by artificial intelligence (AI) models |
| C (Comparison) | Reference standards established by professionals and the existing literature |
| O (Outcomes) | Measurable or predictive outcomes, such as accuracy, sensitivity, and reproducibility |
| Databases | Search Strategy |
|---|---|
| Pubmed | ((artificial intelligence [Title/Abstract] AND anatomic landmarks [Title/Abstract]) OR cephalometry [Title/Abstract] OR cephalometry landmarks [Title/Abstract]) AND orthodontics [Title/Abstract] AND (“2013” [Date—Publication]: “2023” [Date—Publication]) |
| Scopus | artificial AND intelligence AND cephalometric AND landmarks |
| Cochrane | artificial intelligence AND orthodontic appliance |
| IEEE Xplore | artificial intelligence AND cephalometric landmarks |
| Web of Science | ((TS = (artificial intelligence)) AND TS = (cephalometric landmarks)) and 2023 or 2022 or 2021 or 2020 or 2019 or 2016 (Publication Years) |
| Selection | Comparison | Outcomes | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Articles | Representa-Tiveness of the Exposed Cohort | Unexpo-sed Cohort Selection | Exposure Determination | Demonstration of an Aspect of Interest not Present at the Start of the Study | Study Controls | Study Controls for Any Additional Factors | Evaluation of the Result | Sufficiently Long Follow-Up Time | Adequacy of Cohort Monito-ring | Conclusions |
| Kim Y, et al. [58] |  | | | | | | (6) HIGH | |||
| Kim J, et al. [51] | | | | | | | | (7) LOW | ||
| Bulatova G, et al. [52] | | | | | | | | | (8) LOW | |
| Santos Menezes L, et al. [53] | | | | | | | | | (8) LOW | |
| Lee J, et al. [10] | | | | | | | | (7) LOW | ||
| Yao J, et al. [55] | | | | | | | (6) HIGH | |||
| Zhao C, et al. [54] | | | | | | | | (7) LOW | ||
| Ristau B, et al. [50] | | | | | | | | (7) LOW | ||
| Ramadan R, et al. [49] | | | | | | | | (7) LOW | ||
| Hwang H, et al. [59] | | | | | | | (6) HIGH | |||
| Uğurlu M [56] | | | | | | | (6) HIGH | |||
| Davidovitch M, et al. [57] | | | | | | | (6) HIGH | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribas-Sabartés, J.; Sánchez-Molins, M.; d’Oliveira, N.G. The Accuracy of Algorithms Used by Artificial Intelligence in Cephalometric Points Detection: A Systematic Review. Bioengineering 2024, 11, 1286. https://doi.org/10.3390/bioengineering11121286
Ribas-Sabartés J, Sánchez-Molins M, d’Oliveira NG. The Accuracy of Algorithms Used by Artificial Intelligence in Cephalometric Points Detection: A Systematic Review. Bioengineering. 2024; 11(12):1286. https://doi.org/10.3390/bioengineering11121286
Chicago/Turabian StyleRibas-Sabartés, Júlia, Meritxell Sánchez-Molins, and Nuno Gustavo d’Oliveira. 2024. "The Accuracy of Algorithms Used by Artificial Intelligence in Cephalometric Points Detection: A Systematic Review" Bioengineering 11, no. 12: 1286. https://doi.org/10.3390/bioengineering11121286
APA StyleRibas-Sabartés, J., Sánchez-Molins, M., & d’Oliveira, N. G. (2024). The Accuracy of Algorithms Used by Artificial Intelligence in Cephalometric Points Detection: A Systematic Review. Bioengineering, 11(12), 1286. https://doi.org/10.3390/bioengineering11121286