Abstract
Background: Buccal bone dehiscence is a frequent finding during implant placement and often requires horizontal bone augmentation. When combined with immediate loading protocols, concerns remain regarding early implant stability and failure risk. This retrospective case series aimed to describe the early clinical outcomes of immediately loaded implants placed in sites with buccal dehiscence treated by horizontal bone augmentation and restored with full-arch screw-retained prostheses. Methods: Fifty-nine consecutive edentulous patients were rehabilitated with immediately loaded cross-arch implant-supported prostheses. A total of 253 implants were placed, including 148 implants presenting buccal dehiscence and treated with horizontal bone augmentation using particulate grafting materials with or without autogenous bone and a resorbable collagen membrane. Clinical outcomes were assessed over a 1-year follow-up period. Implant survival and biological complications were recorded. Descriptive statistics were applied. An exploratory event-based comparison between augmented and non-augmented implants was performed using Fisher’s exact test, and risk ratios (RRs) with 95% confidence intervals (CIs) were calculated. Results: At 1 year, no patients were lost to follow-up. Two implant failures occurred, both in augmented sites (2/148; 1.35%), while no failures were observed among non-augmented implants (0/105). The exploratory comparison did not show a statistically significant difference in failure rates between groups (p = 0.51). The estimated RR for implant failure associated with horizontal augmentation was 3.56 (95% CI: 0.17–73.34). Two biological complications (one peri-implantitis and one peri-implant mucositis) were recorded, both involving augmented implants. Conclusions: Within the limitations of this retrospective case series, immediately loaded implants placed in sites with buccal dehiscence and treated with horizontal bone augmentation demonstrated high early survival rates and a low incidence of biological complications. These findings are descriptive and exploratory and should be interpreted as hypothesis-generating. Further prospective controlled studies with longer follow-up are needed to confirm these observations.
1. Introduction
Despite continuous advances in preventive and restorative dentistry, edentulism remains a prevalent clinical condition that significantly affects oral function, facial aesthetics, and patients’ quality of life [1,2]. Fixed implant-supported rehabilitations are widely accepted as a treatment modality for fully edentulous patients, offering predictable functional and esthetic outcomes [3]. In particular, full-arch screw-retained prostheses supported by four to six implants have demonstrated high survival rates and favorable long-term results in both the maxilla and mandible [4,5,6].
A common approach for full-arch rehabilitation involves implant placement within the interforaminal region of the mandible or the intersinus area of the maxilla [7,8]. However, anatomical constraints such as progressive alveolar bone resorption, superficial positioning of the mental foramen, and maxillary sinus pneumatization may limit optimal implant positioning [9,10]. To overcome these limitations, distal implants are often placed with intentional angulation in order to increase the anteroposterior spread, improve load distribution, and reduce prosthetic cantilever length [11,12]. While tilted implant configurations offer biomechanical advantages, they may also introduce additional prosthetic and biological challenges that require careful surgical and restorative planning [13,14]. A cross-sectional study by Gibello et al. evaluating full-arch implant-supported prostheses showed that the prosthetic complication rate increased over the follow-up period, despite a 100% implant survival rate. These findings suggested that prosthetic complication rates tend to increase with longer durations of prosthesis function [15].
A comprehensive preoperative assessment is therefore essential, particularly with regard to the evaluation of available hard tissue volume and the potential presence of buccal bone defects [16].
Buccal bone dehiscences and fenestrations are frequently encountered during implant placement and are defined as partial or complete absence of the buccal cortical plate, resulting in exposure of the implant surface [17]. These defects may arise from pre-existing alveolar ridge resorption, post-extraction remodeling, or individual anatomical variations [18,19]. When present, such defects represent a significant surgical challenge and may compromise implant stability, peri-implant tissue health, and long-term outcomes if left untreated [20]. Consequently, horizontal bone augmentation procedures are commonly indicated to restore the buccal bone contour and promote favorable conditions for osseointegration [21,22].
Horizontal guided bone regeneration typically involves the use of particulate grafting materials, either alone or in combination with autogenous bone, often covered by a resorbable collagen membrane [23]. This approach aims to re-establish adequate hard tissue support, protect the implant surface, and enhance both functional and esthetic outcomes. However, these regenerative procedures are technique-sensitive, and their application in conjunction with immediate loading protocols raises additional clinical concerns [24].
Immediate loading has gained increasing popularity due to reduced treatment time, improved patient comfort, and faster functional rehabilitation [25,26]. Nevertheless, its success is closely associated with achieving adequate primary implant stability, which is commonly assessed through insertion torque values or implant stability quotient measurements [27,28]. When implants are placed in sites requiring simultaneous bone augmentation, particularly in the presence of buccal dehiscence, the mechanical engagement with native bone may be reduced. This condition could potentially compromise primary stability and increase the risk of early implant failure or biological complications [29].
Despite the widespread clinical use of immediate loading protocols and horizontal augmentation techniques, limited data are available regarding their combined application in implants placed in sites with buccal dehiscence. Most available evidence derives from heterogeneous clinical reports, and the early outcomes of such combined approaches remain insufficiently documented.
Therefore, the aim of this retrospective case series was to describe the early clinical outcomes of immediately loaded implants placed in sites with buccal dehiscence treated by horizontal bone augmentation and restored with full-arch screw-retained prostheses. By reporting implant survival and early biological complications over a one-year follow-up period, this study seeks to provide descriptive, hypothesis-generating data to support clinical decision making and to inform future prospective investigations.
2. Materials and Methods
2.1. Study Design and Ethical Considerations
This investigation was designed as a retrospective observational case series. Consecutive edentulous patients rehabilitated with immediately loaded full-arch implant-supported prostheses, in whom at least one implant exhibited a buccal bone dehiscence at the time of placement, were included. Clinical data were collected from patients treated in a private dental practice in Sala Consilina (Salerno, Italy) by a single experienced clinician (F.G.) between January 2014 and November 2019.
All procedures were conducted in accordance with the principles of the Declaration of Helsinki. All patients provided written informed consent for treatment and for the use of their anonymized clinical data for scientific purposes. This study was reported following the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for observational studies.
According to local regulations governing retrospective observational studies based on anonymized clinical records, formal ethics committee approval was not required.
2.2. Patient Selection Criteria
Patients were eligible if they met the following inclusion criteria, summarized in Table 1.

Table 1.
Inclusion criteria.
Four to six implants with a minimum length of 11 mm and a minimum diameter of 4.5 mm were placed in the presence of adequate bone volume. Immediate implants were included. Exclusion criteria were as follows in Table 2.
Table 2.
Exclusion criteria.
Patients were classified as non-smokers or smokers (≤10 cigarettes/day) and according to opposing dentition (natural/fixed prostheses or complete dentures).
2.3. Pre-Operative Planning and Surgical Protocol
Initial diagnostic assessment was performed using panoramic radiographs, employing radiopaque markers as reference points to assist in anatomical orientation. To obtain the requisite detail for definitive treatment planning, Cone-Beam Computed Tomography (CBCT) scans (Carestream Dental LLC, Atlanta, GA, USA) were acquired with the radiographic guide in situ, aiding in both virtual planning and surgical navigation. These same guides were subsequently employed intraoperatively to guarantee precise implant placement, thereby strictly adhering to the established preoperative digital planning. Prior to surgery, all patients underwent professional oral prophylaxis and received 2 g of amoxicillin combined with clavulanic acid administered orally one hour prior to the procedure. Penicillin-allergic individuals were prescribed a single dose of 500 mg clarithromycin one hour before the procedure. Immediately before surgery, patients rinsed for one minute with a 0.2% chlorhexidine gluconate solution. Conscious sedation was administered intravenously using a combination of sedatives, followed by local anesthesia using mepivacaine with epinephrine at concentrations of 1:100,000 or 1:50,000. The design of the mucoperiosteal flap was executed utilizing full-thickness crestal incisions. In cases of adequate hard tissue volume, limited mucoperiosteal elevation was performed. Conversely, when bone availability was compromised, extended full-thickness flaps were raised to expose critical anatomical structures, such as the mental foramen or the anterior maxillary sinus wall. Any residual teeth or root fragments were removed using atraumatic techniques, and surgical sites were thoroughly degranulated.
Implant placement involved the use of conical-cylindrical SPI-Contact implants (Thommen Medical; Grenchen, Switzerland), featuring a 1.5 mm polished collar. Implants were predominantly 11 mm in length and 4.5 mm in diameter. All implants were placed according to the manufacturer’s guidelines, except for site preparation: a 4.0 mm profile drill was used in place of the recommended size to intentionally underprepare the osteotomy and thereby enhance primary stability through increased insertion torque. In the premolar regions, distal implants were positioned with a distal angulation to optimize load distribution.
Buccal dehiscence was defined intraoperatively as a partial or complete absence of the buccal cortical plate resulting in exposure of the implant surface after implant placement and flap elevation. Due to the retrospective nature of this study, defect morphology (e.g., standardized measurements of defect width and depth) was not systematically recorded in a reproducible manner and therefore could not be included in the analyses.
Implants were placed with the polished collar supracrestally positioned, even in post-extraction scenarios. A motor-driven insertion torque of 70 Ncm was applied, after which primary stability was verified manually using the SPI-MONO torque ratchet (Thommen Medical; Grenchen, Switzerland). If any of the initially planned four implants failed to reach a minimum insertion torque of 35 Ncm, an additional implant (fifth or sixth) was placed adjacent to the low-stability unit. The 35 Ncm threshold was adopted as a pragmatic criterion commonly used to support immediate loading protocols, as suggested in the literature [30]. In cases where two or more implants failed to achieve sufficient torque, the surgical protocol dictated submerging all implants and deferring prosthetic loading for a three-month osseointegration period [25].
In cases of buccal bone dehiscence (Figure 1), an autogenous granular bone layer was harvested using a bone scraper (14620.10 Stoma; Emmingen-Liptingen, Germany) and applied to cover the exposed implant surface. This graft was subsequently overlaid with an inorganic bovine bone substitute (Bio-Oss, Geistlich, Wolhusen, Switzerland). A double layer of resorbable collagen membrane (Bio-Gide, Geistlich, Switzerland) was then placed over the graft and stabilized with titanium pins, initially using Kalos pins (Orbetello, Italy) and later Smartact pins (Meta, Reggio Emilia, Italy). This regenerative protocol was implemented in 23 implants, whereas in 125 implants only the inorganic bovine bone graft was utilized without the autogenous one. Following graft placement, healing abutments were installed, and wound closure was achieved using single resorbable sutures (Vicryl 4-0 SH1, 22 mm 1/2 c; Ethicon, New Brunswick, NJ, USA).
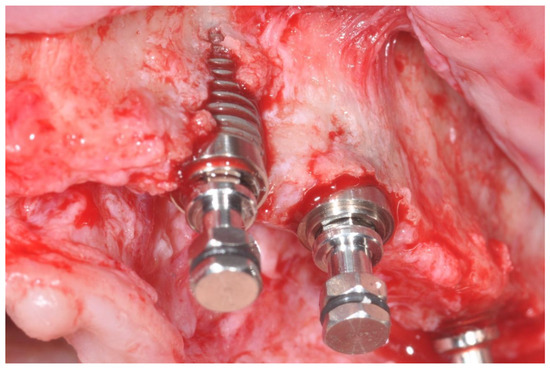
Figure 1.
Bone dehiscence of the buccal alveolar bone.
2.4. Post-Operative Management and Prosthetic Protocol
Postoperatively, patients were advised to take analgesics (Ibuprofen 600 mg) twice daily with meals. A soft diet was recommended for 45 days. Professional oral hygiene inspection was conducted over the three days following surgery to facilitate prosthesis preparation. Patients were instructed to refrain from brushing the surgical area and from rinsing until suture removal, which occurred approximately 10 days after the procedure. Cleaning of the prostheses was recommended using gauze soaked with 0.2% chlorhexidine solution, followed by progressive use of a soft toothbrush, then a medium-bristled toothbrush, and ultimately a water jet device. The definitive prosthetic rehabilitation was initiated immediately following implant insertion.
Individual perforated trays were used to take impressions with precision material. Impregum F (Espe Dental AG, Seefeld, Germany). Definitive screw-retained prostheses were made by placing titanium abutments (VARIOtemp for fixed prostheses, Thommen) on the model, which were connected using titanium rods of 2 mm diameter soldered with an argon syncrystallization device (WELDER INTRAORAL MIDI, Implamed, Cremona, Italy), an intraoral welder, to create a rigid framework. Despite the disparallelism between the implants, it was not necessary to use angulated abutments on the tilted implants. On the second post-operative day, the framework was intraorally evaluated to meticulously assess its adaptation, verify the aesthetic and functional parameters, and confirm phonetic integration.
It was then finalized with a lining in acrylic resin, and the inter-arch relationship was recorded based on the pre-operative digitally designed surgical-prosthetic template. A cantilever length of no more than 1.5 cm per side was permitted. On the third day after surgery, prostheses were screwed onto the implants using a standard torque of 25 Ncm, and the screw access holes were sealed with gutta-percha. A panoramic radiograph was obtained to check the precise seating and secure adaptation of the definitive abutments onto the implants.
Prostheses were designed to have a group function occlusal scheme and were adjusted to have homogeneous occlusal contacts also on cantilevers, when present. Suture removal was performed approximately ten days post-operatively by cutting the knot and leaving the remaining portion of the absorbable suture inside the soft tissues to be spontaneously resorbed. Detailed post-operative oral hygiene protocols were comprehensively communicated to the patient.
2.5. Follow-Up
Patients were seen again every month for the first six months. After a three-month follow-up period, the prostheses were rebased. Patients were recalled for maintenance visits (Figure 2), and the occlusion was evaluated every six months, during which the screw-retained prostheses were removed to assess implant stability and allow for professional cleaning. Patient compliance with home oral hygiene guided the follow-up period.

Figure 2.
Definitive screw-retained prosthesis.
2.6. Outcome Evaluation
The outcomes evaluated in this study were as follows:
- -
- Implant failure: Any mobility and/or infection requiring implant removal and/or biomechanical complications such as implant fracture or deformations of the connections. Implant stability was checked at baseline, 1 month, 3 months after implant placement and thereafter every 6 months by removing the screw-retained prosthesis and checking implant mobility by rocking test through handling of two instruments;
- -
- Any complications, including bleeding, numbness of the lower lip and chin, peri-implant mucositis or peri-implantitis, fistulas formation, screw loosening, phonetic problems, etc.
This study was structured as a retrospective single-cohort study. The inclusion criteria were defined to encompass patients exhibiting alveolar bone dehiscence, who subsequently underwent horizontal guided bone regeneration and rehabilitation with a fixed, screw-retained cross-arch prosthesis planned for immediate functional loading.
No sample size calculation was performed. Patients were considered the statistical unit for descriptive analyses, whereas implant-level analyses were adopted for event-based outcomes.
2.7. Statistical Analysis
Due to the retrospective nature of the study design, neither an a priori sample size determination nor a statistical power analysis was performed. Inferential statistical testing was not planned a priori, given the absence of a formal control group and the primary descriptive aim of this study. Therefore, results should be interpreted as exploratory and hypothesis-generating rather than confirmatory.
Nevertheless, an exploratory post hoc comparison was subsequently performed, as described below.
Descriptive statistics were used to summarize patient- and implant-level characteristics, including frequencies and percentages for categorical variables. Patient-level variables were used to describe the study population, whereas implant-level analyses were adopted for event-based outcomes, including implant failure and biological complications.
In order to explore potential differences in early implant failure occurrence, an event-based comparison was performed between augmented and non-augmented implants. Given the low number of events and the presence of zero-event cells, Fisher’s exact test was selected as the most appropriate method for comparing failure rates between groups.
To quantify the magnitude of association between horizontal augmentation and implant failure, risk ratios (RRs) with 95% confidence intervals (CIs) were calculated. A continuity correction (Haldane–Anscombe method) was applied to allow estimation in the presence of zero failures in one group.
All statistical analyses were conducted at the implant level and were considered exploratory in nature. No adjustment for multiple comparisons was performed, and statistical significance was not the primary objective of the analysis. Because multiple implants were placed in the same patient, implant-level outcomes may not be statistically independent; no adjustment for within-patient clustering (e.g., mixed-effects models or robust standard errors) was performed due to the very low number of events. Therefore, implant-level comparative results should be interpreted as hypothesis-generating. A two-sided p-value < 0.05 was considered indicative of statistical significance. Analyses were performed using standard statistical software.
3. Results
3.1. Patient- and Implant-Level Characteristics
A total of 59 consecutive edentulous patients (32 females and 27 males) with a mean age of 58 years (range: 40–80 years) were included. No patients were lost to follow-up during the 1-year observation period.
Overall, 59 immediately loaded full-arch screw-retained prostheses (45 maxillary and 14 mandibular) were delivered on 253 implants. Among these, 148 implants (58.5%) presented a buccal bone dehiscence at the time of placement and were treated with horizontal bone augmentation, while 105 implants (41.5%) were placed in sites without dehiscence and did not require augmentation. Baseline patient characteristics and treatment-related variables are summarized in Table 3.
Table 3.
Patients’ and intervention characteristics.
Among the augmented implants, 112 were located in the maxilla and 36 in the mandible. A total of 114 implants were placed in post-extractive sites, of which 77 exhibited buccal dehiscence. Overall, 42 implants with dehiscence were placed with an insertion torque ≤ 35 Ncm.
3.2. Implant Survival and Clinical Outcomes
After 1 year of functional loading, two implant failures were recorded, resulting in an overall implant survival rate of 99.2%. Both failures occurred in augmented sites, corresponding to a failure rate of 1.35% among augmented implants (2/148). No implant failures were observed among non-augmented implants (0/105).
Both failed implants were located in the maxilla and occurred in two different patients. One failure involved an implant placed with an insertion torque ≤ 35 Ncm, whereas the second failure occurred in an implant placed with an insertion torque > 35 Ncm. A detailed description of the failed implants, including patient-related characteristics, implant position, insertion torque, and timing of failure, is provided in Table 4. No mechanical complications, such as implant fracture or prosthetic failure, were recorded during the follow-up period.
Table 4.
Description of the implant failures occurred up to the first year of loading.
3.3. Biological Complications
Two biological complications were observed during the 1-year follow-up period, both affecting augmented implants. Specifically, one case of peri-implantitis and one case of peri-implant mucositis were recorded, corresponding to a complication rate of 1.35% among augmented implants. No biological complications were observed in non-augmented sites.
Details regarding the type of complication and implant location are reported in Table 5.
Table 5.
Description of the complications that occurred up to the first year of function.
3.4. Results of Statistical Analysis
An exploratory event-based comparison of implant failure rates between augmented and non-augmented implants was performed. Given the low number of failures and the presence of zero-event cells, Fisher’s exact test was used.
The analysis did not demonstrate a statistically significant difference in early implant failure rates between augmented and non-augmented implants (p = 0.51). The estimated risk ratio for implant failure associated with horizontal bone augmentation was 3.56, with a wide 95% confidence interval (0.17–73.34), reflecting the limited number of events and reduced statistical precision. In addition, exact binomial 95% confidence intervals were calculated for overall implant survival and group-specific failure proportions to provide an estimate of uncertainty around descriptive rates.
No additional implant- or patient-level variables were formally tested for association with implant failure due to the small number of observed events.
4. Discussion
This retrospective case series evaluated the 1-year clinical outcomes of immediately loaded implants placed in sites presenting buccal bone dehiscence and treated with horizontal bone augmentation. The primary finding of the present study was a high overall implant survival rate (99.2%), with only two implant failures and two biological complications observed during the follow-up period. These outcomes are consistent with previously published reports on immediate loading protocols in full-arch rehabilitations [25,31,32].
The management of buccal bone dehiscence represents a frequent and clinically relevant challenge in implant dentistry, particularly in post-extractive sites and in the anterior maxilla, where buccal plate resorption is common [33,34,35]. Immediate implant placement in such conditions has been associated with an increased risk of soft tissue recession and esthetic complications if dehiscence defects are not adequately managed [36,37,38]. Horizontal bone augmentation using particulate grafts and resorbable collagen membranes is widely considered a predictable technique to restore buccal bone volume and to support peri-implant tissues [39,40,41]. Long-term retrospective and longitudinal studies have demonstrated favorable outcomes for horizontal ridge augmentation procedures, including satisfactory bone regeneration and stability over time [42,43,44].
From a contemporary implantology perspective, insertion torque provides only an indirect estimate of primary stability at the time of implant placement. Resonance Frequency Analysis (RFA), expressed as Implant Stability Quotient (ISQ), represents a non-invasive method to objectively monitor implant stability over time and to support clinical decision making regarding loading protocols [45]. ISQ values range from 0 to 100, and values approximately between 60 and 70 are often considered clinically meaningful for assessing primary and secondary stability in many clinical settings. Although RFA was not available in the present retrospective series, future prospective studies combining insertion torque measurements with serial ISQ assessments could provide a more comprehensive evaluation of stability dynamics in augmented dehiscence sites undergoing immediate loading.
Despite the favorable overall outcomes observed in the present study, it is noteworthy that all implant failures occurred in sites treated with horizontal augmentation. One failed implant exhibited low insertion torque (<35 Ncm), reinforcing the importance of primary stability in immediate loading protocols [46]. Nevertheless, the occurrence of a failure in an implant placed with adequate insertion torque suggests that additional factors may influence early implant failure in augmented sites. The biological and biomechanical characteristics of regenerated bone, which often consists of a combination of autogenous and xenogeneic graft materials, may differ from those of pristine bone and potentially affect early osseointegration [47,48].
Defect morphology and graft composition may represent additional factors influencing early outcomes in augmented dehiscence sites. Wider or deeper buccal defects may reduce native bone–implant contact, potentially affecting primary stability and biomechanical behavior during immediate loading. Moreover, in the present series, some implants were treated using a thin autogenous bone layer combined with an anorganic bovine bone substitute, whereas others received the xenograft alone. Such differences in graft composition may have influenced early healing dynamics and the biological environment surrounding the implants. However, the retrospective design, the absence of standardized defect measurements, and the low number of adverse events did not allow meaningful subgroup or comparative analyses.
The exploratory statistical analysis performed did not reveal a statistically significant difference in early implant failure rates between augmented and non-augmented implants. However, the wide confidence interval associated with the estimated risk ratio reflects the limited number of events and the consequent lack of statistical precision. Therefore, the absence of statistical significance should not be interpreted as evidence of equivalence between the two groups but rather as a limitation inherent to the exploratory nature of the analysis.
Biological complications were also limited to augmented implants, with one case of peri-implantitis and one case of peri-implant mucositis recorded during the follow-up period. These findings may be related to the increased complexity of maintaining peri-implant tissue health in regenerated sites, where altered soft tissue contours and grafted bone may complicate plaque control [49,50]. In this context, increasing attention has been directed toward biological adjuvants capable of enhancing soft tissue healing and early wound stabilization in oral surgery [51]. Autologous platelet concentrates have been extensively investigated for their potential to improve clinical and radiographic healing following tooth extractions and impacted third molar removal, demonstrating favorable effects on postoperative recovery and soft tissue outcomes [52,53]. Although these approaches were not applied in the present study, their biological rationale may be of interest for future investigations aiming to optimize peri-implant tissue healing, particularly in surgically complex scenarios involving bone augmentation.
Previous studies have highlighted the importance of supportive care and patient compliance in preventing peri-implant diseases, particularly in complex rehabilitations involving immediate loading and bone augmentation procedures [54,55].
Immediate implant placement and loading in the presence of buccal bone dehiscence can be considered a viable treatment option in selected cases; however, wider or deeper defects have been associated with an increased risk of gingival recession and biological complications [56,57]. This underscores the importance of careful case selection, accurate intraoperative assessment of defect morphology, and the use of appropriate hard- and soft-tissue augmentation techniques.
The clinical decision-making process during surgery plays a crucial role in the management of dehiscence defects. Early identification of buccal bone defects requires surgical experience and the ability to adapt the treatment plan accordingly. Proceeding with simultaneous horizontal augmentation and immediate loading should be based on a comprehensive evaluation of implant primary stability, bone quality, defect extension, and patient-related risk factors such as smoking or systemic conditions.
Compared with other clinical reports, the present study benefits from a relatively large number of implants placed according to a standardized surgical and prosthetic protocol and treated by a single experienced clinician. In addition, no patients were lost to follow-up, strengthening the internal consistency of the data.
Limitations of This Study
Several limitations of the present study must be acknowledged. First, the retrospective observational design inherently limits the ability to control for confounding variables and precludes causal inference. No formal control group was included, and the analysis was primarily descriptive in nature. Although an exploratory statistical comparison was performed, the very low number of implant failures limited the possibility of identifying statistically meaningful associations or predictive factors. Additionally, implant-level analyses may be affected by within-patient clustering because multiple implants were placed in the same individual; no clustering adjustment was applied, which may limit inferential interpretation of implant-level comparisons.
Second, no a priori sample size calculation or statistical power analysis was performed, and the patient was considered the statistical unit for descriptive purposes. This limits the generalizability of the findings and the interpretation of subgroup analyses.
Third, implant stability was assessed clinically using a manual rocking test rather than quantitative methods such as resonance frequency analysis. While this assessment was consistently performed by the same experienced clinician, it may introduce a degree of subjectivity.
In addition, standardized radiographic evaluation of marginal bone levels was not available, preventing quantitative assessment of peri-implant bone changes over time. This was due to the retrospective nature of this study and the lack of standardized longitudinal radiographic imaging protocols.
Finally, the 1-year follow-up period allows evaluation of early implant survival and short-term biological outcomes but does not permit conclusions regarding long-term implant performance, peri-implant bone stability, or prosthetic maintenance.
5. Conclusions
Within the limitations of this retrospective case series, implants placed in sites presenting buccal bone dehiscence and treated with horizontal bone augmentation demonstrated high early survival rates and a low incidence of biological complications when immediately loaded under full-arch screw-retained prostheses.
Although all implant failures and biological complications occurred in augmented sites, the overall frequency of adverse events was low during the 1-year follow-up period. These findings suggest that, under stringent clinical conditions and careful case selection, the combination of horizontal augmentation and immediate loading may represent a feasible therapeutic approach in selected edentulous patients.
Nevertheless, given the retrospective design, the short follow-up period, and the exploratory nature of the statistical analysis, the results should be interpreted with caution. Further prospective controlled studies with larger sample sizes, objective outcome measures, and longer follow-up are required to confirm the clinical predictability and long-term performance of this treatment protocol.
Author Contributions
Conceptualization, F.G. and A.A. (Alfonso Acerra).; methodology, A.A. (Alfonso Acerra); validation, F.G., M.C.; formal analysis, A.A. (Angelo Aliberti); investigation, M.L.; data curation, M.L.; writing—original draft preparation, A.A. (Alfonso Acerra); writing—review and editing, A.A. (Angelo Aliberti); visualization, M.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki. Ethics Committee or Institutional Review Board (IRB) approval has been deemed unnecessary for the reasons listed in the national “Provisions relating to the processing of personal data for scientific research purposes” (Italian Data Protection Authority-General Authorization No. 9/2016). The processing of the data reported in this paper has been conducted by appropriate safeguards for scientific research under Article 89(1) of the General Data Protection Regulation (GDPR EU/2016/679) [58] . All the possible pertinent technical and organizational measures have been adopted in order to protect the rights and freedoms of the data subjects involved while conducting scientific research. The published data do not entail any significant personalized impact on data subjects, and all the possible measures aimed at ensuring respect for the principle of data minimization (anonymization/pseudonymization) have been adopted.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gerritsen, A.E.; Creugers, N.H.J. Quality of life associated with tooth loss and tooth replacement. Ned. Tijdschr. Tandheelkd. 2011, 118, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Emami, E.; de Souza, R.F.; Kabawat, M.; Feine, J.S. The Impact of Edentulism on Oral and General Health. Int. J. Dent. 2013, 2013, 498305. [Google Scholar] [CrossRef] [PubMed]
- Agliardi, E.L.; Pozzi, A.; Romeo, D.; Del Fabbro, M. Clinical Outcomes of Full-Arch Immediate Fixed Prostheses Supported by Two Axial and Two Tilted Implants: A Retrospective Cohort Study with 12–15 Years of Follow-Up. Clin. Oral Implant. Res. 2023, 34, 351–366. [Google Scholar] [CrossRef] [PubMed]
- Brånemark, P.I.; Svensson, B.; van Steenberghe, D. Ten-Year Survival Rates of Fixed Prostheses on Four or Six Implants Ad Modum Brånemark in Full Edentulism. Clin. Oral Implant. Res. 1995, 6, 227–231. [Google Scholar] [CrossRef]
- Pantaleo, G.; Acerra, A.; Giordano, F.; D’Ambrosio, F.; Langone, M.; Caggiano, M. Immediate Loading of Fixed Prostheses in Fully Edentulous Jaws: A 7-Year Follow-Up from a Single-Cohort Retrospective Study. Appl. Sci. 2022, 12, 12427. [Google Scholar] [CrossRef]
- Maló, P.; Rangert, B.; Nobre, M. All-on-4 Immediate-Function Concept with Brånemark System Implants for Completely Edentulous Maxillae: A 1-Year Retrospective Clinical Study. Clin. Implant. Dent. Relat. Res. 2005, 7, S88–S94. [Google Scholar] [CrossRef]
- Lin, G.; Ye, S.; Liu, F.; He, F. A Retrospective Study of 30,959 Implants: Risk Factors Associated with Early and Late Implant Loss. J. Clin. Periodontol. 2018, 45, 733–743. [Google Scholar] [CrossRef]
- Soto-Penaloza, D.; Zaragozí-Alonso, R.; Penarrocha-Diago, M.; Penarrocha-Diago, M. The All-on-Four Treatment Concept: Systematic Review. J. Clin. Exp. Dent. 2017, 9, e474–e488. [Google Scholar] [CrossRef]
- Vera, C.; De Kok, I.J.; Chen, W.; Reside, G.; Tyndall, D.; Cooper, L.F. Evaluation of Post-Implant Buccal Bone Resorption Using Cone Beam Computed Tomography: A Clinical Pilot Study. Int. J. Oral Maxillofac. Implant. 2012, 27, 1249–1257. [Google Scholar]
- Gershenson, A.; Nathan, H.; Luchansky, E. Mental Foramen and Mental Nerve: Changes with Age. Acta Anat. 1986, 126, 21–28. [Google Scholar] [CrossRef]
- Gherlone, E.F.; D’Orto, B.; Nagni, M.; Capparè, P.; Vinci, R. Tilted Implants and Sinus Floor Elevation Techniques Compared in Posterior Edentulous Maxilla: A Retrospective Clinical Study over Four Years of Follow-Up. Appl. Sci. 2022, 12, 6729. [Google Scholar] [CrossRef]
- Mehta, S.P.; Sutariya, P.V.; Pathan, M.R.; Upadhyay, H.H.; Patel, S.R.; Kantharia, N.D.G. Clinical Success between Tilted and Axial Implants in Edentulous Maxilla: A Systematic Review and Meta-Analysis. J. Indian Prosthodont. Soc. 2021, 21, 217–228. [Google Scholar] [CrossRef]
- Agliardi, E.; Panigatti, S.; Clericò, M.; Villa, C.; Malò, P. Immediate Rehabilitation of the Edentulous Jaws with Full Fixed Prostheses Supported by Four Implants: Interim Results of a Single Cohort Prospective Study. Clin. Oral Implant. Res. 2010, 21, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Caggiano, M.; D’Ambrosio, F.; Acerra, A.; Giudice, D.; Giordano, F. Biomechanical Implications of Mandibular Flexion on Implant-Supported Full-Arch Rehabilitations: A Systematic Literature Review. J. Clin. Med. 2023, 12, 5302. [Google Scholar] [CrossRef] [PubMed]
- Gibello, U.; Lanzetti, J.; Crupi, A.; Longhi, B.; Molinero-Mourelle, P.; Roccuzzo, A.; Pera, F. Clinical Outcomes of Full-Arch Fixed Implant-Supported Prostheses in Patients Lacking Supportive Peri-Implant Care: A Cross-Sectional Study. Int. J. Oral Implant. 2025, 18, 147–157. [Google Scholar]
- Monje, A.; Roccuzzo, A.; Buser, D.; Wang, H.-L. Influence of Buccal Bone Wall Thickness on the Peri-Implant Hard and Soft Tissue Dimensional Changes: A Systematic Review. Clin. Oral Implant. Res. 2023, 34, 157–176. [Google Scholar] [CrossRef]
- Chen, S.T.; Buser, D. Esthetic Outcomes Following Immediate and Early Implant Placement in the Anterior Maxilla–a Systematic Review. Int. J. Oral Maxillofac. Implant. 2014, 29, 186–215. [Google Scholar] [CrossRef]
- Tan, W.L.; Wong, T.L.T.; Wong, M.C.M.; Lang, N.P. A Systematic Review of Post-Extractional Alveolar Hard and Soft Tissue Dimensional Changes in Humans. Clin. Oral Implant. Res. 2012, 23, 1–21. [Google Scholar] [CrossRef]
- Sangiovanni, G.; Giordano, F.; Acerra, A.; Chiacchio, A.; Valletta, A. Surgical Extrusion: State of the Art and Literature Review. J. Osseointegration 2023, 15, 83–90. [Google Scholar] [CrossRef]
- Qian, S.-J.; Pu, Y.-P.; Zhang, X.-M.; Wu, X.-Y.; Liu, B.-L.; Lai, H.-C.; Shi, J.-Y. Clinical, Radiographic, and Esthetic Evaluation of Immediate Implant Placement with Buccal Bone Dehiscence in the Anterior Maxilla: A 1-Year Prospective Case Series. Clin. Implant. Dent. Relat. Res. 2023, 25, 3–10. [Google Scholar] [CrossRef]
- Tay, J.R.H.; Lu, X.J.; Lai, W.M.C.; Fu, J.-H. Clinical and Histological Sequelae of Surgical Complications in Horizontal Guided Bone Regeneration: A Systematic Review and Proposal for Management. Int. J. Implant. Dent. 2020, 6, 76. [Google Scholar] [CrossRef] [PubMed]
- Caggiano, M.; D’Ambrosio, F.; Giordano, F.; Acerra, A.; Sammartino, P.; Iandolo, A. The “Sling” Technique for Horizontal Guided Bone Regeneration: A Retrospective Case Series. Appl. Sci. 2022, 12, 5889. [Google Scholar] [CrossRef]
- Lorenz, J.; Ghanaati, S.; Aleksic, Z.; Milinkovic, I.; Lazic, Z.; Magić, M.; Wessing, B.; Grotenclos, R.S.; Merli, M.; Mariotti, G.; et al. Horizontal Guided Bone Regeneration of the Posterior Mandible to Allow Implant Placement: 1-Year Prospective Study Results. Clin. Oral Implant. Res. 2025, 36, 100–116. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Liang, Q.; Lu, H.; Chu, H.; Gan, Z.; Rong, M. Clinical Outcomes of Alveolar Ridge Augmentation with In Situ Autogenous Block Bone: A Retrospective Review. Int. J. Oral Maxillofac. Implant. 2021, 36, 1008–1015. [Google Scholar] [CrossRef]
- Jiang, X.; Zhou, W.; Wu, Y.; Wang, F. Clinical Outcomes of Immediate Implant Loading with Fixed Prostheses in Edentulous Maxillae: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2021, 36, 503–519. [Google Scholar] [CrossRef]
- Liu, X.Q.; Liu, J.Z.; Feng, H.L.; Heng, M.D.; Wang, B.; Pan, S.X. Time Efficiency of Immediate Loading of Full-Arch Implant Reconstructions Using Prefabricated Prostheses Located by an Anchor Pin: A Pilot Study. Chin. J. Dent. Res. 2021, 24, 257–265. [Google Scholar] [CrossRef]
- Degidi, M.; Nardi, D.; Piattelli, A. A Six-Year Follow-up of Full-Arch Immediate Restorations Fabricated with an Intraoral Welding Technique. Implant. Dent. 2013, 22, 224–231. [Google Scholar] [CrossRef]
- D’Albis, G.; Forte, M.; Alrashadah, A.O.; Marini, L.; Corsalini, M.; Pilloni, A.; Capodiferro, S. Immediate Loading of Implants-Supported Fixed Partial Prostheses in Posterior Regions: A Systematic Review. Dent. J. 2025, 13, 213. [Google Scholar] [CrossRef]
- Anitua, E. Immediate Loading of Short Implants in Posterior Maxillae: Case Series. Acta Stomatol. Croat. 2017, 51, 157–162. [Google Scholar] [CrossRef]
- Del Giudice, R.; Piattelli, A.; Grande, N.-M.; Cataneo, E.; Crispino, A.; Petrini, M. Implant Insertion Torque Value in Immediate Loading: A Retrospective Study. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e398–e403. [Google Scholar] [CrossRef]
- Simonpieri, A.; Gasparro, R.; Pantaleo, G.; Mignogna, J.; Riccitiello, F.; Sammartino, G. Four-Year Post-Loading Results of Full-Arch Rehabilitation with Immediate Placement and Immediate Loading Implants: A Retrospective Controlled Study. Quintessence Int. 2017, 48, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Pun, L.; Lau, K.Y.; Li, K.Y.; Wong, M.C.M. A Systematic Review on Survival and Success Rates of Implants Placed Immediately into Fresh Extraction Sockets after at Least 1 Year. Clin. Oral Implant. Res. 2012, 23, 39–66. [Google Scholar] [CrossRef] [PubMed]
- Weigl, P.; Strangio, A. The Impact of Immediately Placed and Restored Single-Tooth Implants on Hard and Soft Tissues in the Anterior Maxilla. Eur. J. Oral Implantol. 2016, 9, S89–S106. [Google Scholar] [PubMed]
- Chappuis, V.; Araújo, M.G.; Buser, D. Clinical Relevance of Dimensional Bone and Soft Tissue Alterations Post-Extraction in Esthetic Sites. Periodontol. 2000 2017, 73, 73–83. [Google Scholar] [CrossRef]
- Januário, A.L.; Duarte, W.R.; Barriviera, M.; Mesti, J.C.; Araújo, M.G.; Lindhe, J. Dimension of the Facial Bone Wall in the Anterior Maxilla: A Cone-Beam Computed Tomography Study. Clin. Oral Implant. Res. 2011, 22, 1168–1171. [Google Scholar] [CrossRef]
- Wittneben, J.-G.; Molinero-Mourelle, P.; Hamilton, A.; Alnasser, M.; Obermaier, B.; Morton, D.; Gallucci, G.O.; Wismeijer, D. Clinical Performance of Immediately Placed and Immediately Loaded Single Implants in the Esthetic Zone: A Systematic Review and Meta-Analysis. Clin. Oral Implant. Res. 2023, 34, 266–303. [Google Scholar] [CrossRef]
- Slagter, K.W.; den Hartog, L.; Bakker, N.A.; Vissink, A.; Meijer, H.J.A.; Raghoebar, G.M. Immediate Placement of Dental Implants in the Esthetic Zone: A Systematic Review and Pooled Analysis. J. Periodontol. 2014, 85, e241–e250. [Google Scholar] [CrossRef]
- Dominiak, M.; Hnitecka, S.; Olchowy, C.; Dominiak, S.; Gedrange, T. Possible Treatment of Severe Bone Dehiscences Based on 3D Bone Reconstruction—A Description of Treatment Methodology. Appl. Sci. 2021, 11, 10299. [Google Scholar] [CrossRef]
- Keddar, M.; Evrard, L.; Shall, F. Horizontal Ridge Augmentation Using Guided Bone Regeneration with an Association of Particulate Allografts Mixed with Platelet-Rich Fibrin, Collagen Membrane and Tent-Screws: A Prospective Study. J. Stomatol. Oral Maxillofac. Surg. 2024, 125, 101872. [Google Scholar] [CrossRef]
- Sanz, M.; Dahlin, C.; Apatzidou, D.; Artzi, Z.; Bozic, D.; Calciolari, E.; De Bruyn, H.; Dommisch, H.; Donos, N.; Eickholz, P.; et al. Biomaterials and Regenerative Technologies Used in Bone Regeneration in the Craniomaxillofacial Region: Consensus Report of Group 2 of the 15th European Workshop on Periodontology on Bone Regeneration. J. Clin. Periodontol. 2019, 46, 82–91. [Google Scholar] [CrossRef]
- Tony, J.B.; Parthasarathy, H.; Tadepalli, A.; Ponnaiyan, D.; Alamoudi, A.; Kamil, M.A.; Alzahrani, K.J.; Alsharif, K.F.; Halawani, I.F.; Alnfiai, M.M.; et al. CBCT Evaluation of Sticky Bone in Horizontal Ridge Augmentation with and without Collagen Membrane-A Randomized Parallel Arm Clinical Trial. J. Funct. Biomater. 2022, 13, 194. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.-W.; Hwang, S.-S.; Yun, P.-Y.; Kim, Y.-K. Horizontal Ridge Augmentation with Porcine Bone-Derived Grafting Material: A Long-Term Retrospective Clinical Study with More than 5 Years of Follow-Up. J. Korean Assoc. Oral Maxillofac. Surg. 2023, 49, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Luo, Y.; Qu, Y.; Man, Y. Horizontal Ridge Augmentation in the Anterior Maxilla with in Situ Onlay Bone Grafting: A Retrospective Cohort Study. Clin. Oral Investig. 2022, 26, 5893–5908. [Google Scholar] [CrossRef] [PubMed]
- Farias, D.; Caceres, F.; Sanz, A.; Olate, S. Horizontal Bone Augmentation in the Posterior Atrophic Mandible and Dental Implant Stability Using the Tenting Screw Technique. Int. J. Periodontics Restor. Dent. 2021, 41, e147–e155. [Google Scholar] [CrossRef]
- Veljkovic, L.; Nedeljkovic, M.; Rosic, G.; Selakovic, D.; Jovicic, N.; Stevanovic, M.; Milanovic, J.; Arnaut, A.; Vasiljevic, M.; Milanovic, P. Clinical and Histological Assessment of Knife-Edge Thread Implant Stability After Ridge Preservation Using Hydroxyapatite and Sugar Cross-Linked Collagen: Preliminary Report. Dent. J. 2025, 13, 585. [Google Scholar] [CrossRef]
- Manfredini, M.; Ghizzoni, M.; Cusaro, B.; Beretta, M.; Maiorana, C.; Souza, F.Á.; Poli, P.P. High Insertion Torque-Clinical Implications and Drawbacks: A Scoping Review. Medicina 2025, 61, 1187. [Google Scholar] [CrossRef]
- Schrott, A.; Riggi-Heiniger, M.; Maruo, K.; Gallucci, G.O. Implant Loading Protocols for Partially Edentulous Patients with Extended Edentulous Sites–a Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2014, 29, 239–255. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Savoini, M.; Dalmasso, P.; Ramieri, G. Long-Term Outcomes of Implants Placed after Vertical Alveolar Ridge Augmentation in Partially Edentulous Patients: A 10-Year Prospective Clinical Study. Clin. Oral Implant. Res. 2017, 28, 1204–1210. [Google Scholar] [CrossRef]
- Esposito, M.; Siormpas, K.; Mitsias, M.; Bechara, S.; Trullenque-Eriksson, A.; Pistilli, R. Immediate, Early (6 Weeks) and Delayed Loading (3 Months) of Single Implants: 4-Month Post-Loading from a Multicenter Pragmatic Randomised Controlled Trial. Eur. J. Oral Implantol. 2016, 9, 249–260. [Google Scholar]
- Renvert, S.; Quirynen, M. Risk Indicators for Peri-Implantitis. A Narrative Review. Clin. Oral Implant. Res. 2015, 26, 15–44. [Google Scholar] [CrossRef]
- Acerra, A.; Caggiano, M.; Chiacchio, A.; Scognamiglio, B.; D’Ambrosio, F. PRF and PRP in Dentistry: An Umbrella Review. J. Clin. Med. 2025, 14, 3224. [Google Scholar] [CrossRef]
- Campana, M.D.; Aliberti, A.; Acerra, A.; Sammartino, P.; Dolce, P.; Sammartino, G.; Gasparro, R. The Effectiveness and Safety of Autologous Platelet Concentrates as Hemostatic Agents after Tooth Extraction in Patients on Anticoagulant Therapy: A Systematic Review of Randomized, Controlled Trials. J. Clin. Med. 2023, 12, 5342. [Google Scholar] [CrossRef]
- Aliberti, A.; Mariniello, M.; Bergaminelli, M.; Dolce, P.; Gargiulo, D.; Sammartino, G.; Spagnuolo, G.; Gasparro, R. Using Injectable Platelet-Rich Fibrin to Improve Recovery after Impacted Lower Third Molar Extraction: A Randomized Controlled Clinical Trial. Clin. Oral Investig. 2025, 29, 467. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.-L. Peri-Implantitis. J. Periodontol. 2018, 89, S267–S290. [Google Scholar] [CrossRef]
- Bertolini, M.M.; Del Bel Cury, A.A.; Pizzoloto, L.; Acapa, I.R.H.; Shibli, J.A.; Bordin, D. Does Traumatic Occlusal Forces Lead to Peri-Implant Bone Loss? A Systematic Review. Braz. Oral Res. 2019, 33, e069. [Google Scholar] [CrossRef]
- Buser, D.; Martin, W.; Belser, U.C. Optimizing Esthetics for Implant Restorations in the Anterior Maxilla: Anatomic and Surgical Considerations. Int. J. Oral Maxillofac. Implant. 2004, 19, 43–61. [Google Scholar]
- Ickroth, A.; Seyssens, L.; Christiaens, V.; Pitman, J.; Cosyn, J. Immediate versus Early Implant Placement for Single Tooth Replacement in the Aesthetic Area: A Systematic Review and Meta-Analysis. Clin. Oral Implant. Res. 2024, 35, 585–597. [Google Scholar] [CrossRef] [PubMed]
- General Authorization No. 9/2016; Authorization for the Processing of Personal Data for Scientific Research Purposes. Italian Data Protection Authority (Garante per la Protezione dei Dati Personali): Rome, Italy, 2016.


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.