
Petrified Ears: A Clue for Adrenal Insufficiency



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
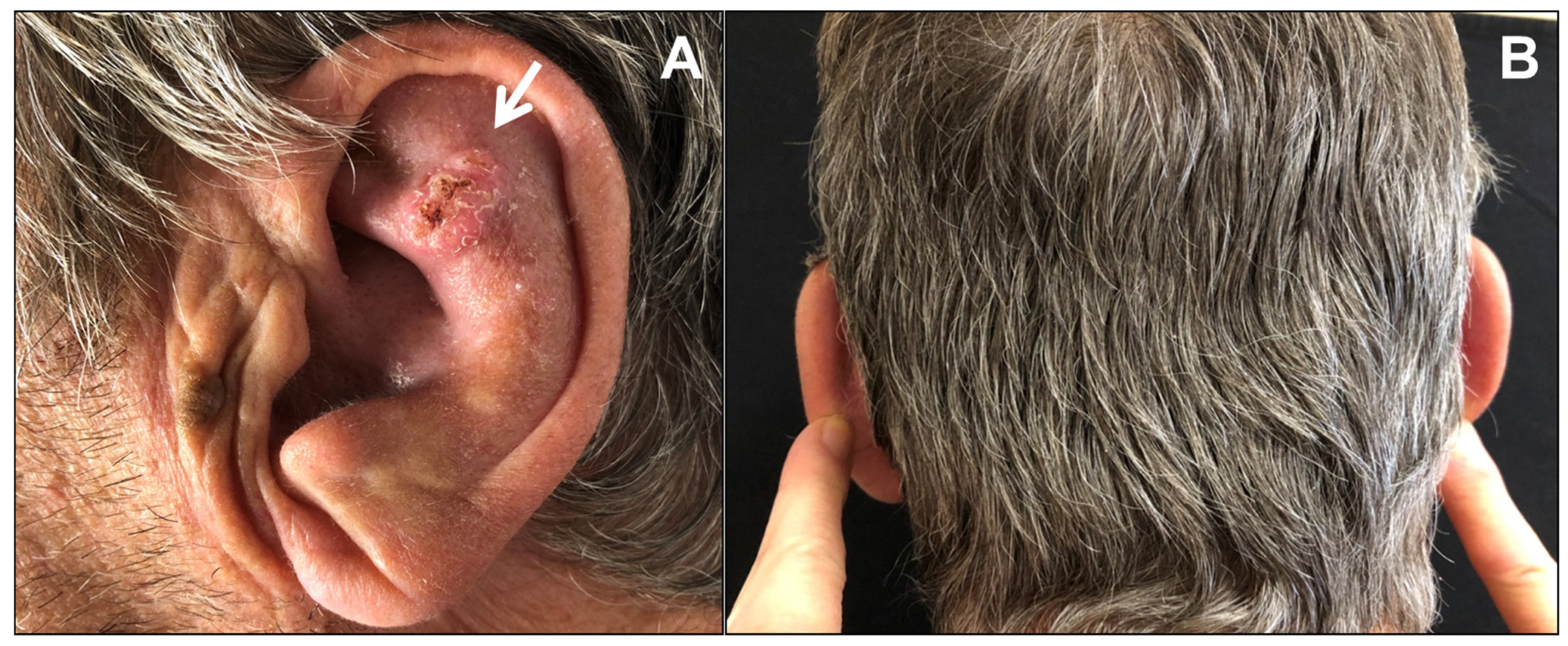
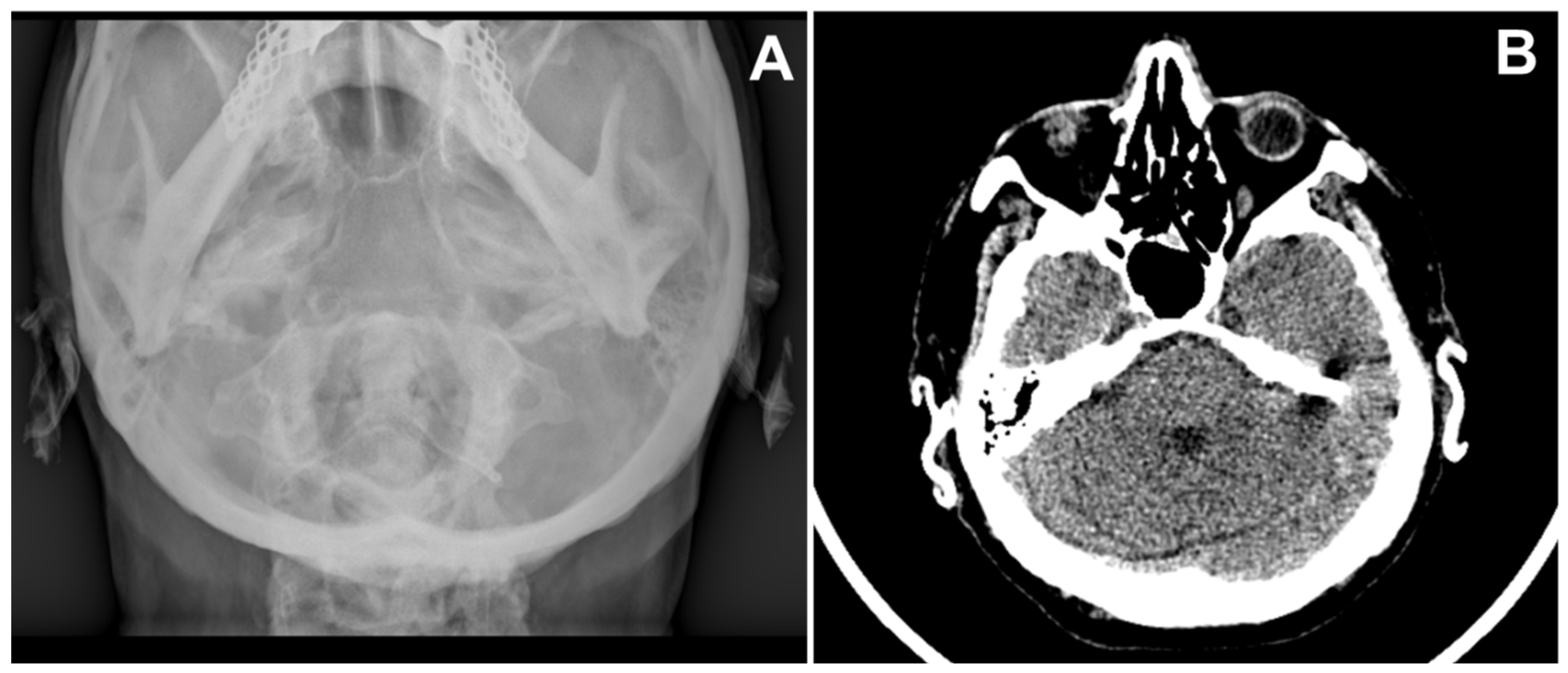
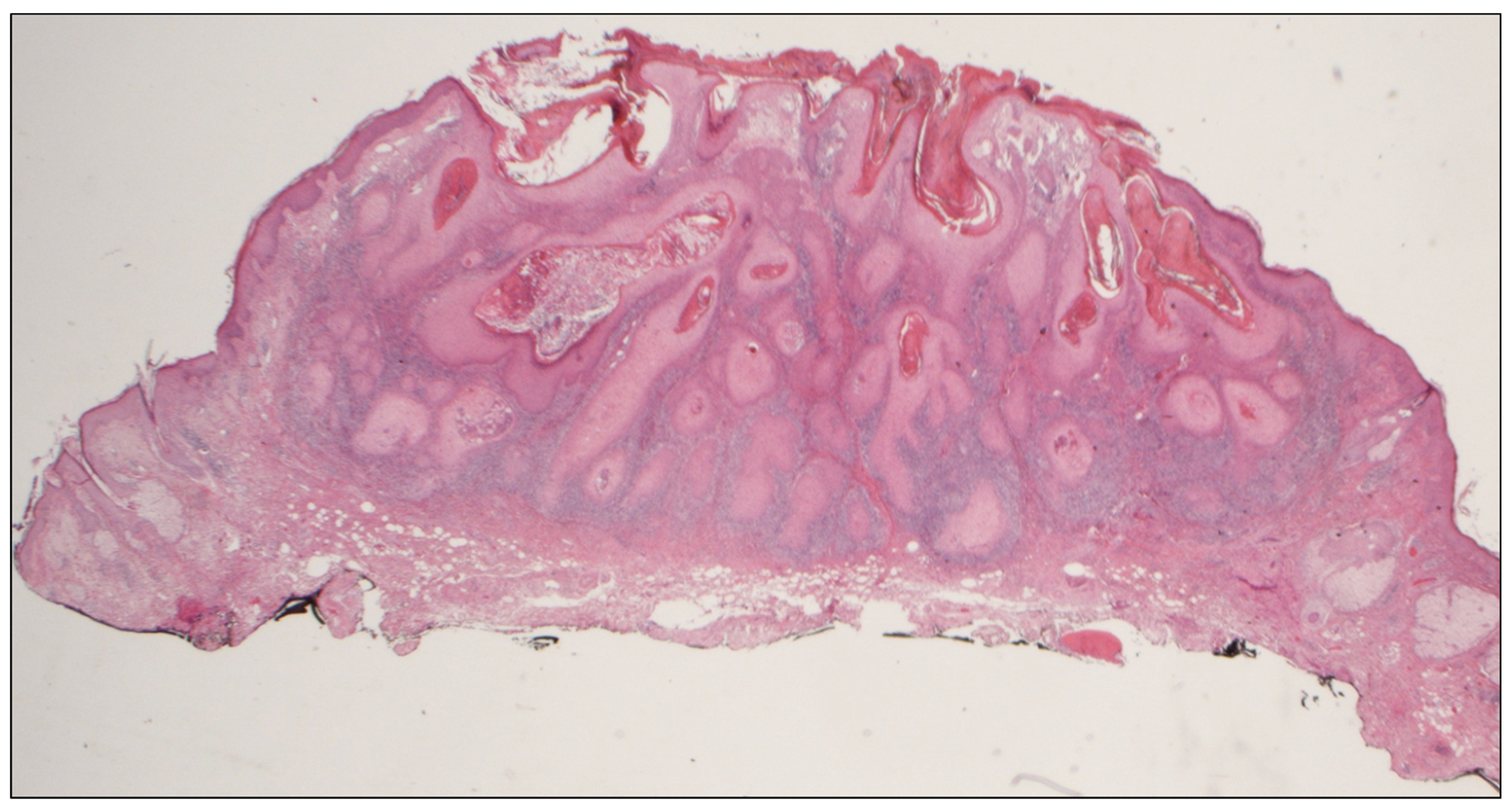
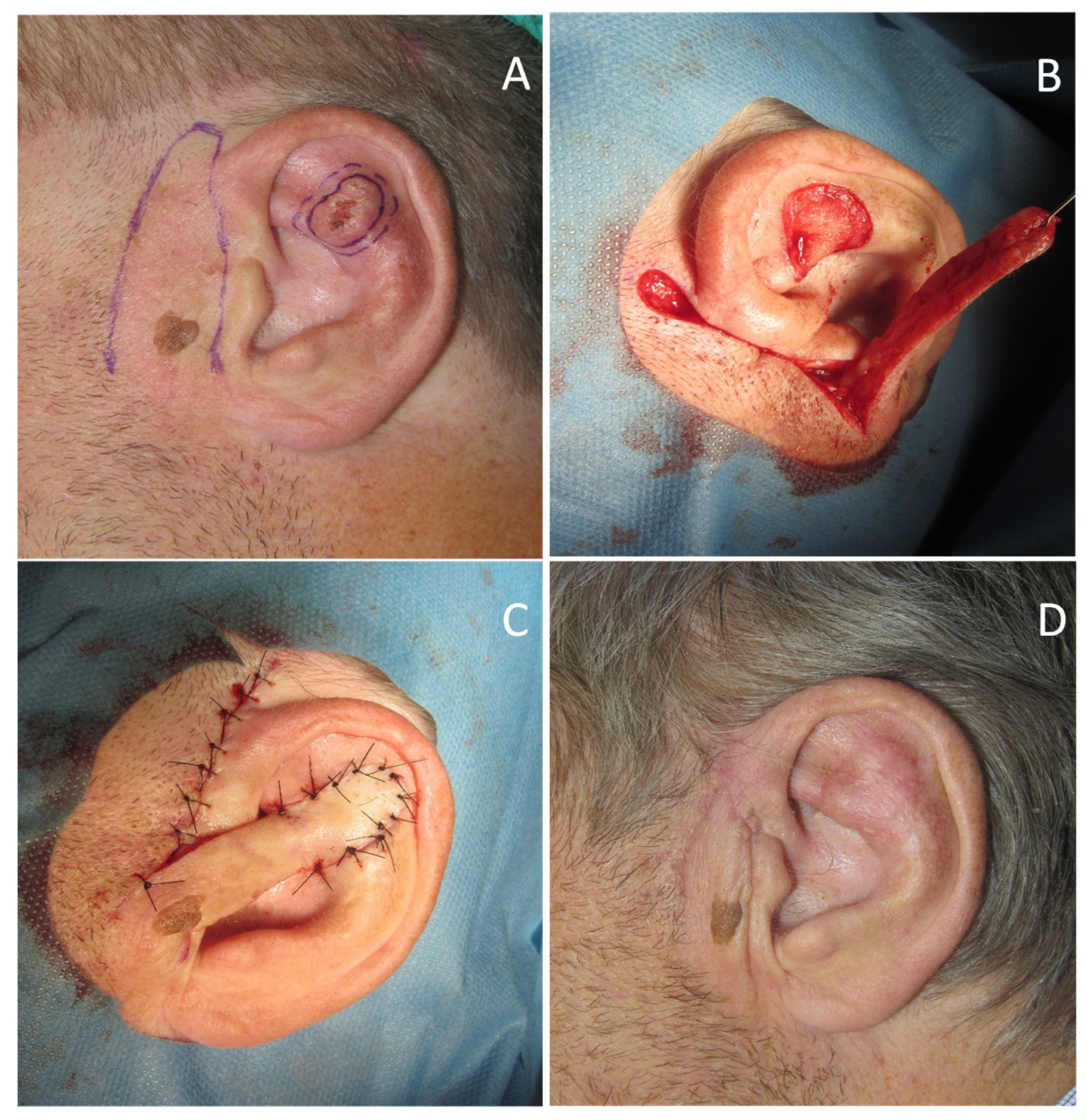
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bochdalek, G. Psysiologische Verknöcherung der Aurecula. Prag. Vierteljahrschr. 1866, 89, 33–46. [Google Scholar]
- Shah, A.; Khorshid, S.M.; Suchak, R.; Law Pak Chong, S. Unilateral petrified ear. Clin. Exp. Dermatol. 2019, 44, 310–312. [Google Scholar] [CrossRef] [PubMed]
- Thomson, M.A.; Biggs, P.; Berth-Jones, J. Familial petrified ears associated with endocrinopathy. J. Am. Acad. Dermatol. 2007, 57, S121–S122. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, T.; Yoshida, M.; Terada, Y. Petrified Ear Auricles with Isolated Adrenocorticotropic Hormone Deficiency. Intern. Med. 2017, 56, 3263–3264. [Google Scholar] [CrossRef] [PubMed][Green Version]
- James, H.A.; Wermers, R.A. “Petrified Ears”: Auricular Ossification in Adrenal Insufficiency. Mayo Clin. Proc. 2016, 91, 1487–1488. [Google Scholar] [CrossRef] [PubMed]
- Gogate, Y.; Gangadhar, P.; Walia, R.R.; Bhansali, A. “Petrified ears” with idiopathic adult-onset pituitary insufficiency. Indian J. Endocrinol. Metab. 2012, 16, 830–832. [Google Scholar] [PubMed]
- Gossner, J. Prevalence of the petrified ear: A computed tomographic study. Eur. Arch. Otorhinolaryngol. 2014, 271, 195–197. [Google Scholar] [CrossRef]
- Buikema, K.E.; Adams, E.G. A rare case of petrified ear. Case Rep. Dermatol. Med. 2012, 2012, 410601. [Google Scholar] [CrossRef] [PubMed]
- Thomas, L.; Naidoo, K.; Woolfall, P.; Carmichael, A.J. A unique presentation of ‘petrified ears’ with pain due to fracture. J. Eur. Acad. Dermatol. Venereol. 2019, 33, e51–e52. [Google Scholar] [CrossRef]
- Lister, G.D. Ossification in the elastic cartilage of the ear. Br. J. Surg 1969, 56, 399–400. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Recalcati, S.; Fantini, F. Petrified Ears: A Clue for Adrenal Insufficiency. Dermatopathology 2021, 8, 45-48. https://doi.org/10.3390/dermatopathology8010009
Recalcati S, Fantini F. Petrified Ears: A Clue for Adrenal Insufficiency. Dermatopathology. 2021; 8(1):45-48. https://doi.org/10.3390/dermatopathology8010009
Chicago/Turabian StyleRecalcati, Sebastiano, and Fabrizio Fantini. 2021. "Petrified Ears: A Clue for Adrenal Insufficiency" Dermatopathology 8, no. 1: 45-48. https://doi.org/10.3390/dermatopathology8010009
APA StyleRecalcati, S., & Fantini, F. (2021). Petrified Ears: A Clue for Adrenal Insufficiency. Dermatopathology, 8(1), 45-48. https://doi.org/10.3390/dermatopathology8010009