
An Underrecognized Histologic Clue to the Diagnosis of Mucous Membrane Pemphigoid: A Case Report and Review of Diagnostic Guidelines

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
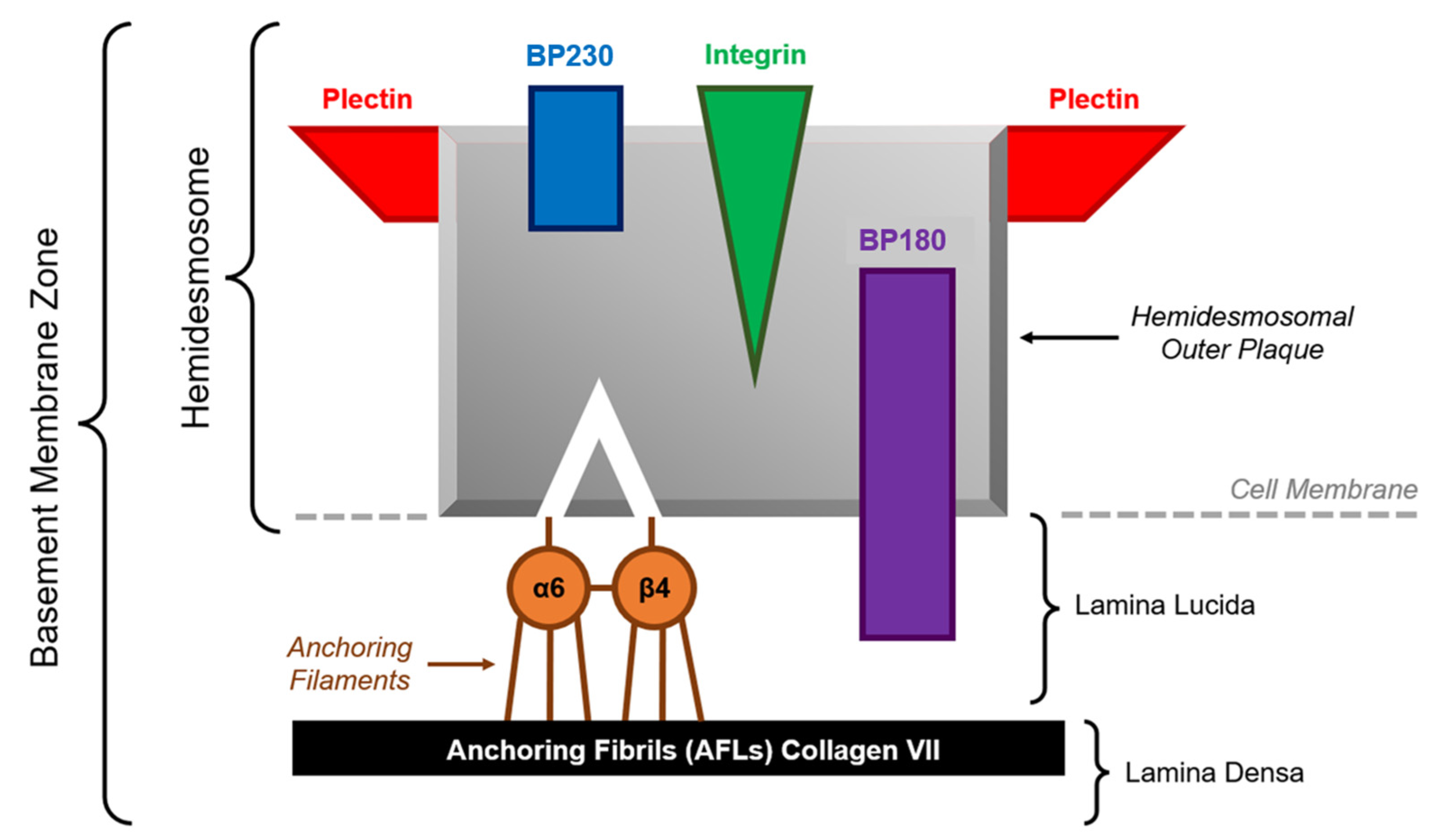
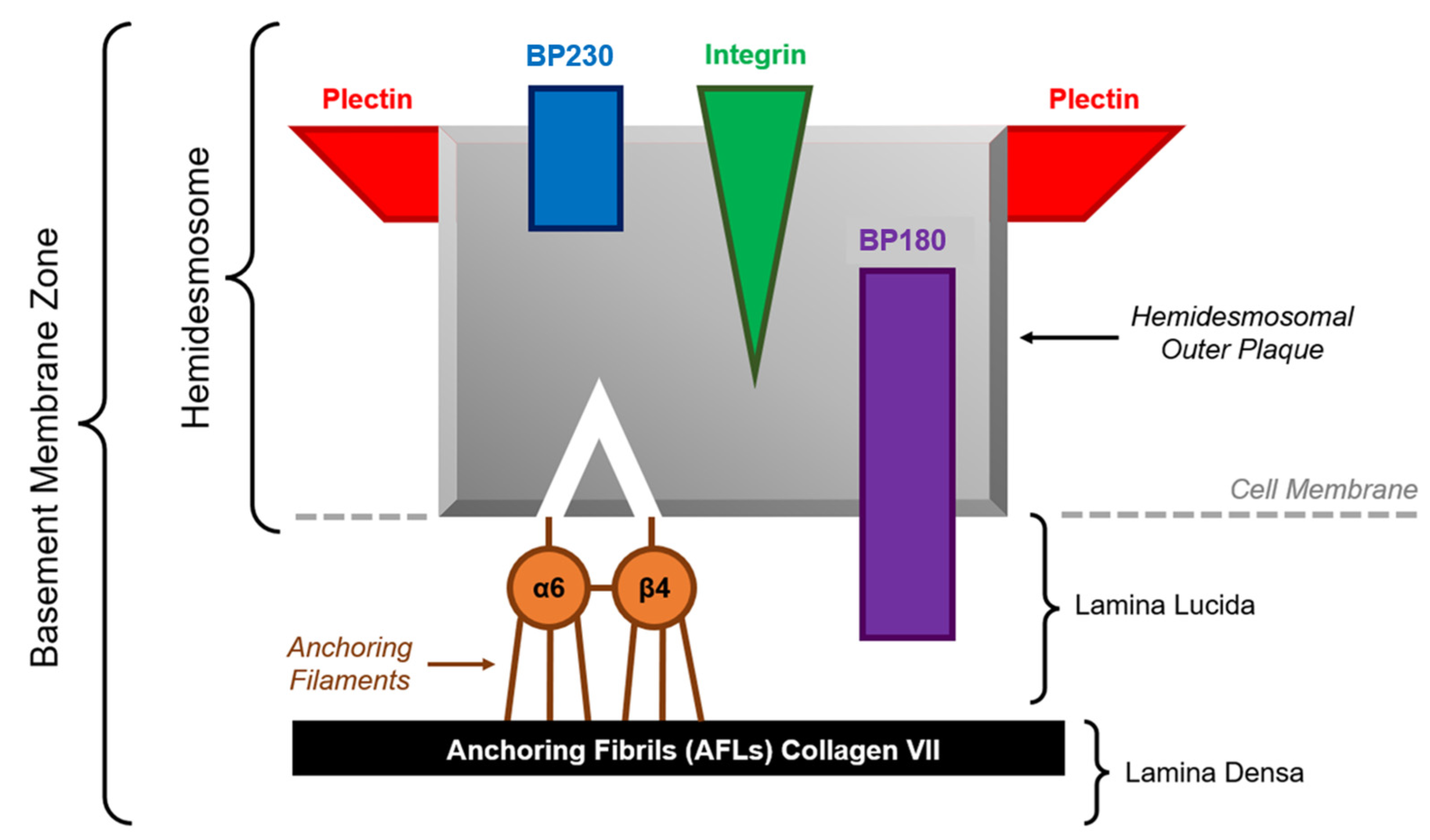
:1. Introduction
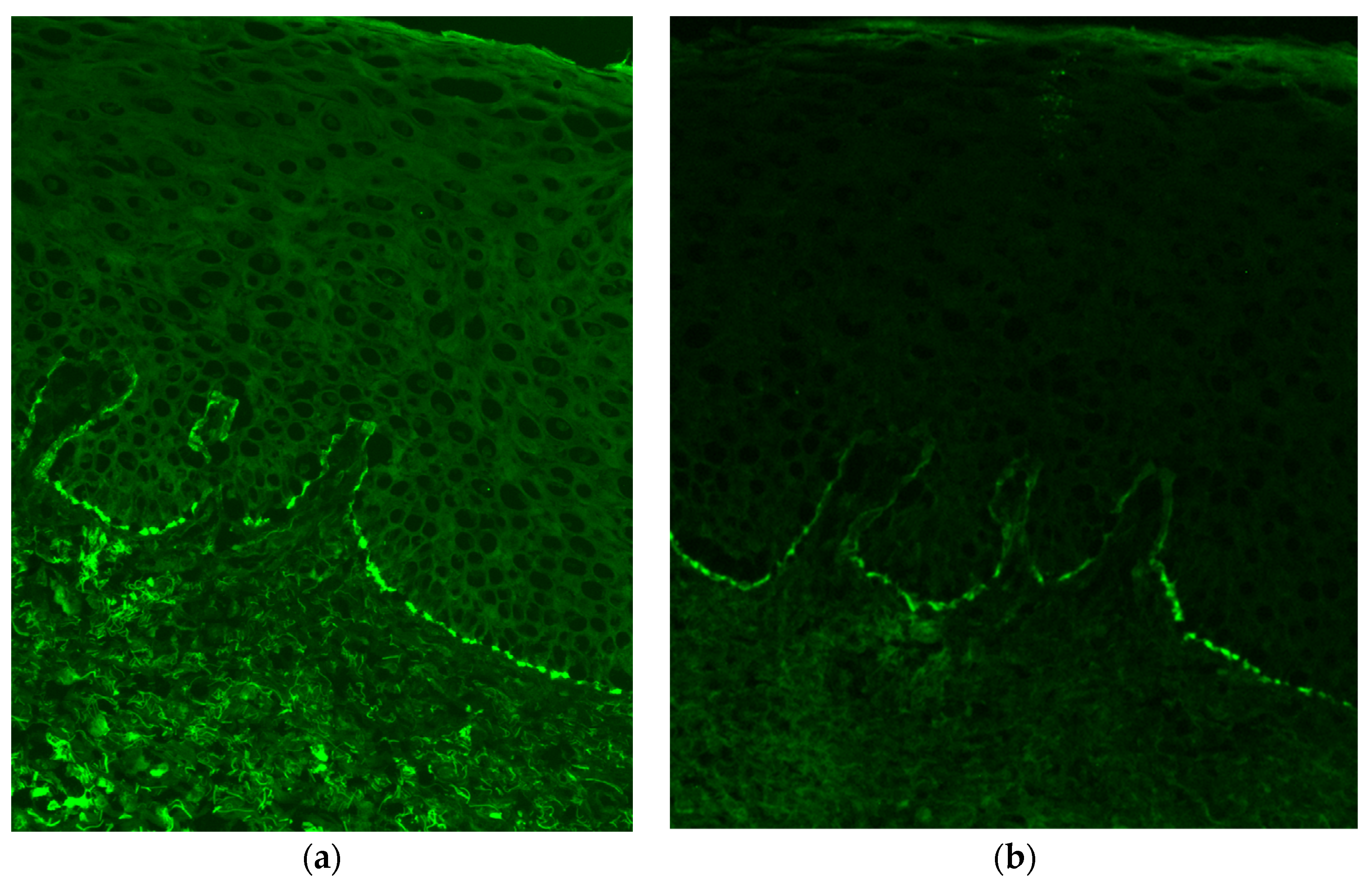
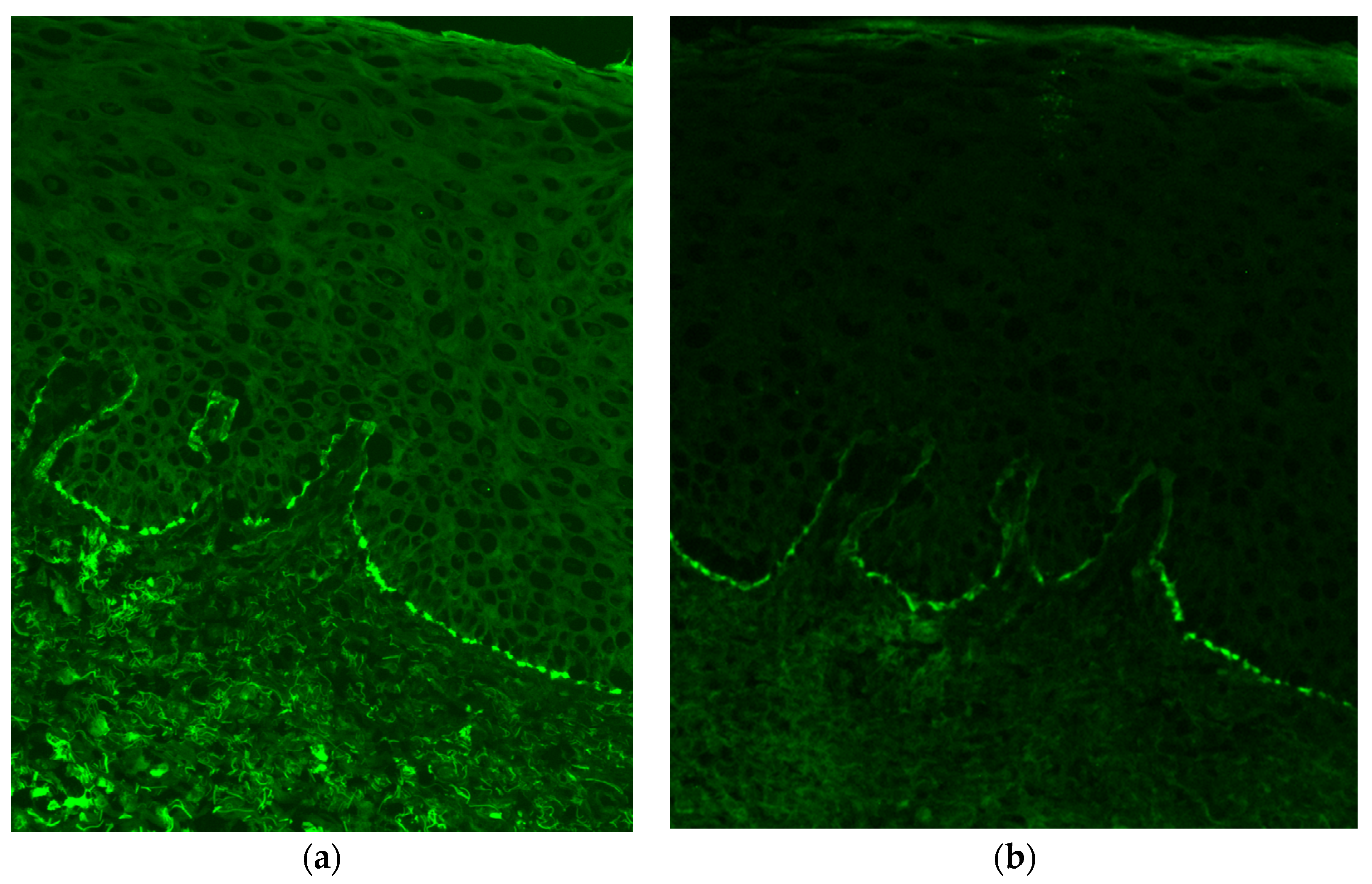
1.1. Immunofluorescence Studies
1.2. Diagnostic Guidelines
- For single mucous membrane involvement without skin involvement: Perilesional biopsy (i.e., obtain specimen from a location adjacent to the inflamed site).
- For multiple mucous membrane involvements without skin involvement: Obtain specimen from “tissue adjacent to an inflamed nonocular mucosal site”.
- For mucous membrane involvement and skin involvement: Perilesional biopsy (i.e., obtain specimen from a location adjacent to the inflamed site).
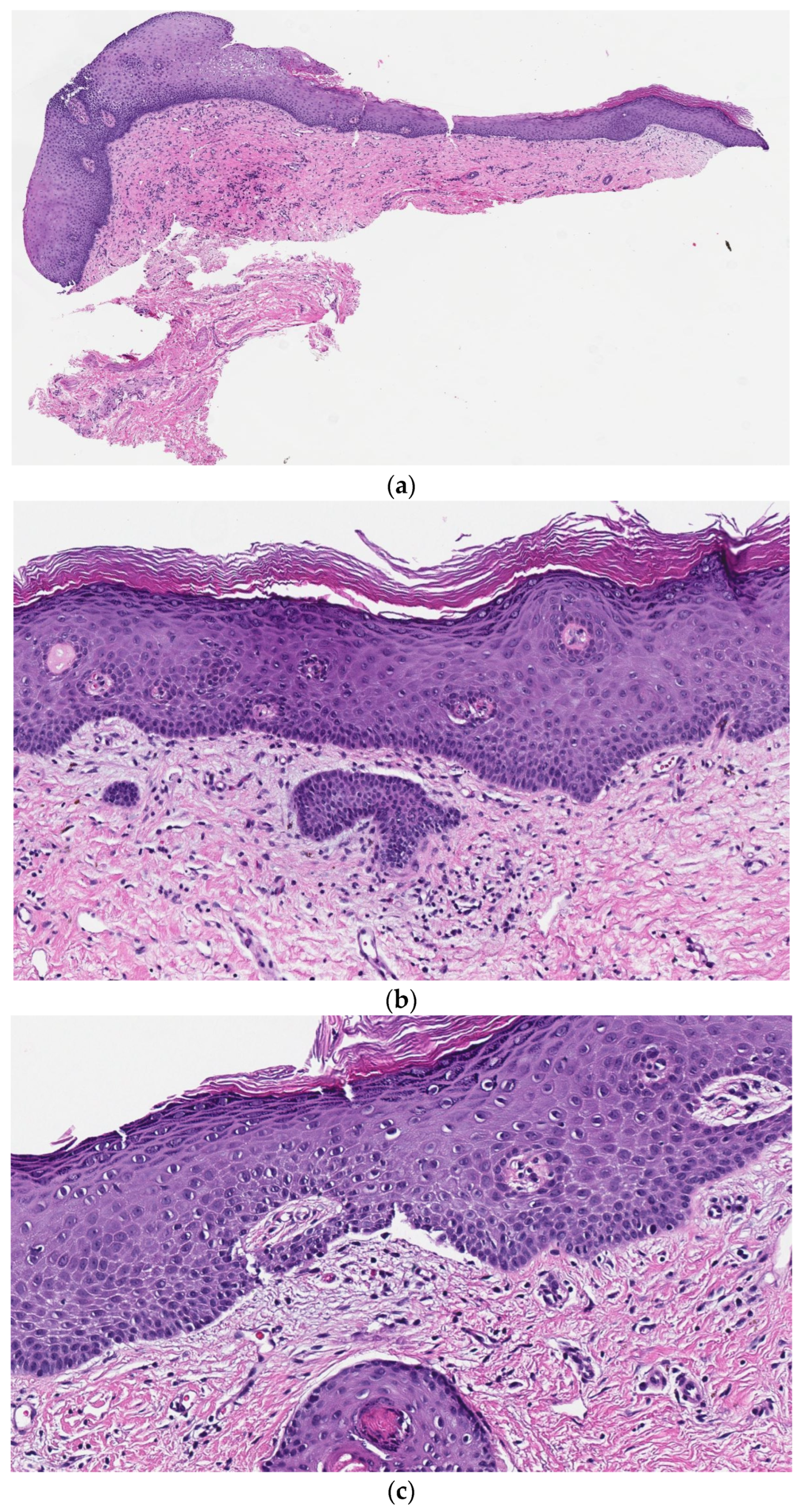
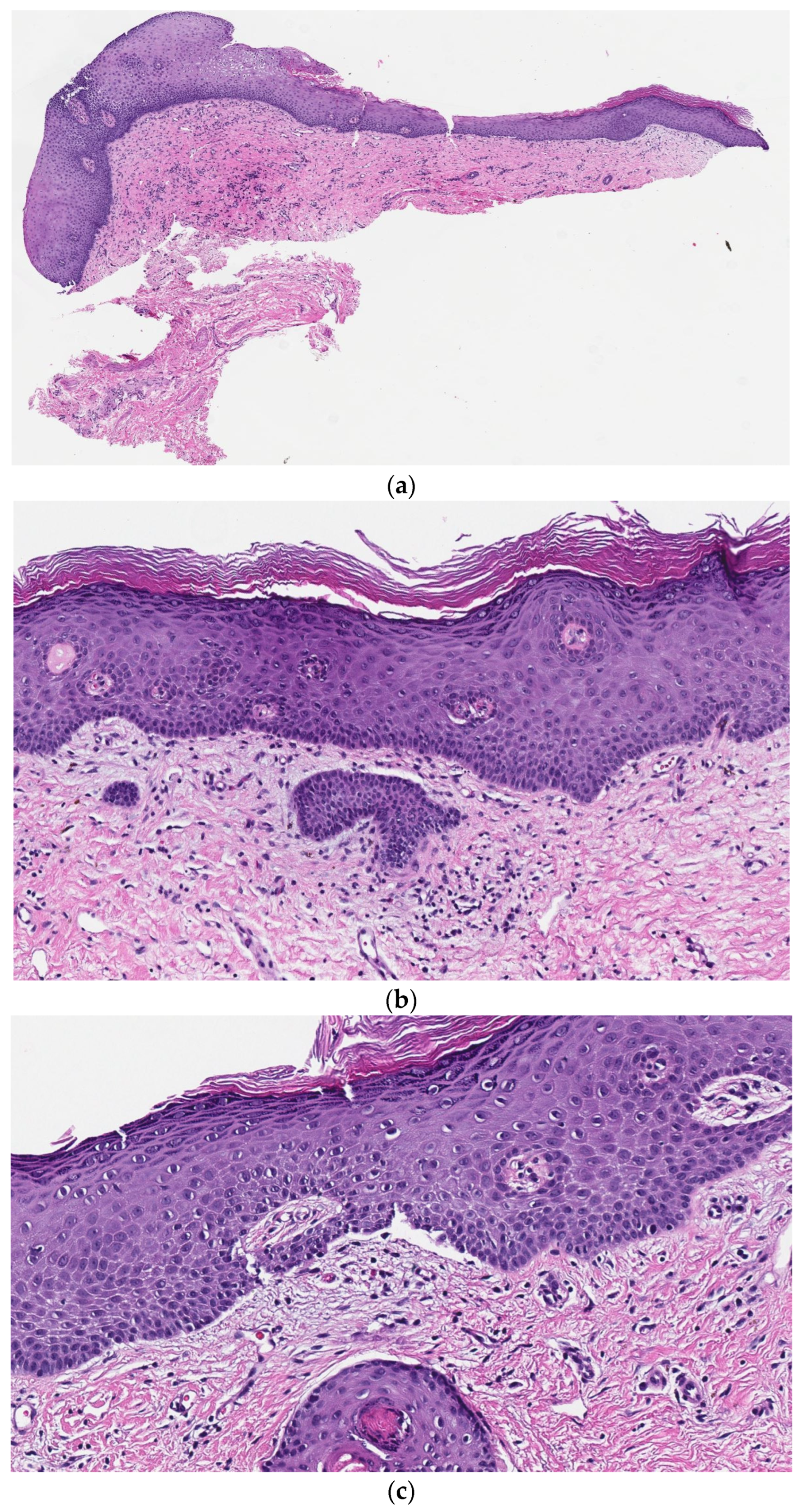
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, H.-H.; Werth, V.P.; Parisi, E.; Sollecito, T.P. Mucous membrane pemphigoid. Dent. Clin. N. Am. 2013, 57, 611–630. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.R.; Kurgis, B.S.; Rogers, R.S. Cicatricial pemphigoid. J. Am. Acad. Dermatol. 1991, 24, 987–1001. [Google Scholar] [CrossRef] [PubMed]
- Dainichi, T.; Koga, H.; Tsuji, T.; Ishii, N.; Ohyama, B.; Ueda, A.; Natsuaki, Y.; Karashima, T.; Nakama, T.; Yasumoto, S.; et al. From anti-p200 pemphigoid to anti-laminin γ1 pemphigoid. J. Dermatol. 2010, 37, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Natsuga, K.; Nishie, W.; Shinkuma, S.; Moriuchi, R.; Shibata, M.; Nishimura, M.; Hashimoto, T.; Shimizu, H. Circulating IgA and IgE autoantibodies in antilaminin-332 mucous membrane pemphigoid: IgA and IgE autoantibodies in antilaminin-332 MMP. Br. J. Dermatol. 2010, 162, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.S.; Ahmed, A.R.; Anhalt, G.J.; Bernauer, W.; Cooper, K.D.; Elder, M.J.; Fine, J.-D.; Foster, C.S.; Ghohestani, R.; Hashimoto, T.; et al. The first international consensus on mucous membrane pemphigoid: Definition, diagnostic criteria, pathogenic factors, medical treatment, and prognostic indicators. Arch. Dermatol. 2002, 138, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Setterfield, J.; Theron, J.; Vaughan, R.W.; Welsh, K.I.; Mallon, E.; Wojnarowska, F.; Challacombe, S.J.; Black, M.M. Mucous membrane pemphigoid: HLA-DQB1*0301 is associated with all clinical sites of involvement and may be linked to antibasement membrane IGG production. Br. J. Dermatol. 2008, 145, 406–414. [Google Scholar] [CrossRef]
- Ackerman, B.A. Algorithms for Histologic Diagnosis of Inflammatory Skin Diseases, 2nd ed.; Baltimore, M.D., Ed.; Williams & Wilkins: Philadelphia, PA, USA, 1997; pp. 283–284. [Google Scholar]
- Garg, T.; Mittal, S. Vesicobullous disorders of female genitalia. Indian J. Sex. Transm. Dis. AIDS 2012, 33, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, E.; Rashid, H.; Marzano, A.V.; Lamberts, A.; Di Zenzo, G.; Diercks, G.F.H.; Alberti-Violetti, S.; Barry, R.J.; Borradori, L.; Caproni, M.; et al. European guidelines (S3) on diagnosis and management of mucous membrane pemphigoid, initiated by the European Academy of Dermatology and Venereology–Part II. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1926–1948. [Google Scholar] [CrossRef] [PubMed]
- Shimanovich, I.; Nitz, J.M.; Zillikens, D. Multiple and repeated sampling increases the sensitivity of direct immunofluorescence testing for the diagnosis of mucous membrane pemphigoid. J. Am. Acad. Dermatol. 2017, 77, 700–705.e3. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McFadden, J.R.; Chaudhari, A.S.; Birenbaum, D.; Margesson, L.; Gonzalez, J.; Sriharan, A. An Underrecognized Histologic Clue to the Diagnosis of Mucous Membrane Pemphigoid: A Case Report and Review of Diagnostic Guidelines. Dermatopathology 2023, 10, 63-69. https://doi.org/10.3390/dermatopathology10010009
McFadden JR, Chaudhari AS, Birenbaum D, Margesson L, Gonzalez J, Sriharan A. An Underrecognized Histologic Clue to the Diagnosis of Mucous Membrane Pemphigoid: A Case Report and Review of Diagnostic Guidelines. Dermatopathology. 2023; 10(1):63-69. https://doi.org/10.3390/dermatopathology10010009
Chicago/Turabian StyleMcFadden, Jason R., Advaita S. Chaudhari, Debra Birenbaum, Lynette Margesson, Jorge Gonzalez, and Aravindhan Sriharan. 2023. "An Underrecognized Histologic Clue to the Diagnosis of Mucous Membrane Pemphigoid: A Case Report and Review of Diagnostic Guidelines" Dermatopathology 10, no. 1: 63-69. https://doi.org/10.3390/dermatopathology10010009
APA StyleMcFadden, J. R., Chaudhari, A. S., Birenbaum, D., Margesson, L., Gonzalez, J., & Sriharan, A. (2023). An Underrecognized Histologic Clue to the Diagnosis of Mucous Membrane Pemphigoid: A Case Report and Review of Diagnostic Guidelines. Dermatopathology, 10(1), 63-69. https://doi.org/10.3390/dermatopathology10010009