


The Evolution of Psychological Distress Levels in University Students in Spain during Different Stages of the COVID-19 Pandemic: Risk and Protective Factors


 ,
,
Abstract
:1. Introduction
1.1. The Impact of the First Wave of COVID-19 on University Students
1.2. COVID-19 and Psychological Distress: Protective and Risk Factors
1.3. The Present Study
2. Materials and Methods
2.1. Participants, Design, and Procedure
2.2. Measures
2.2.1. Psychological Distress
2.2.2. Stressful Events during the COVID-19 Pandemic
2.2.3. Perceived Social Support
2.2.4. Self-Esteem
2.2.5. Sociodemographic Variables
2.3. Data Analysis
3. Results
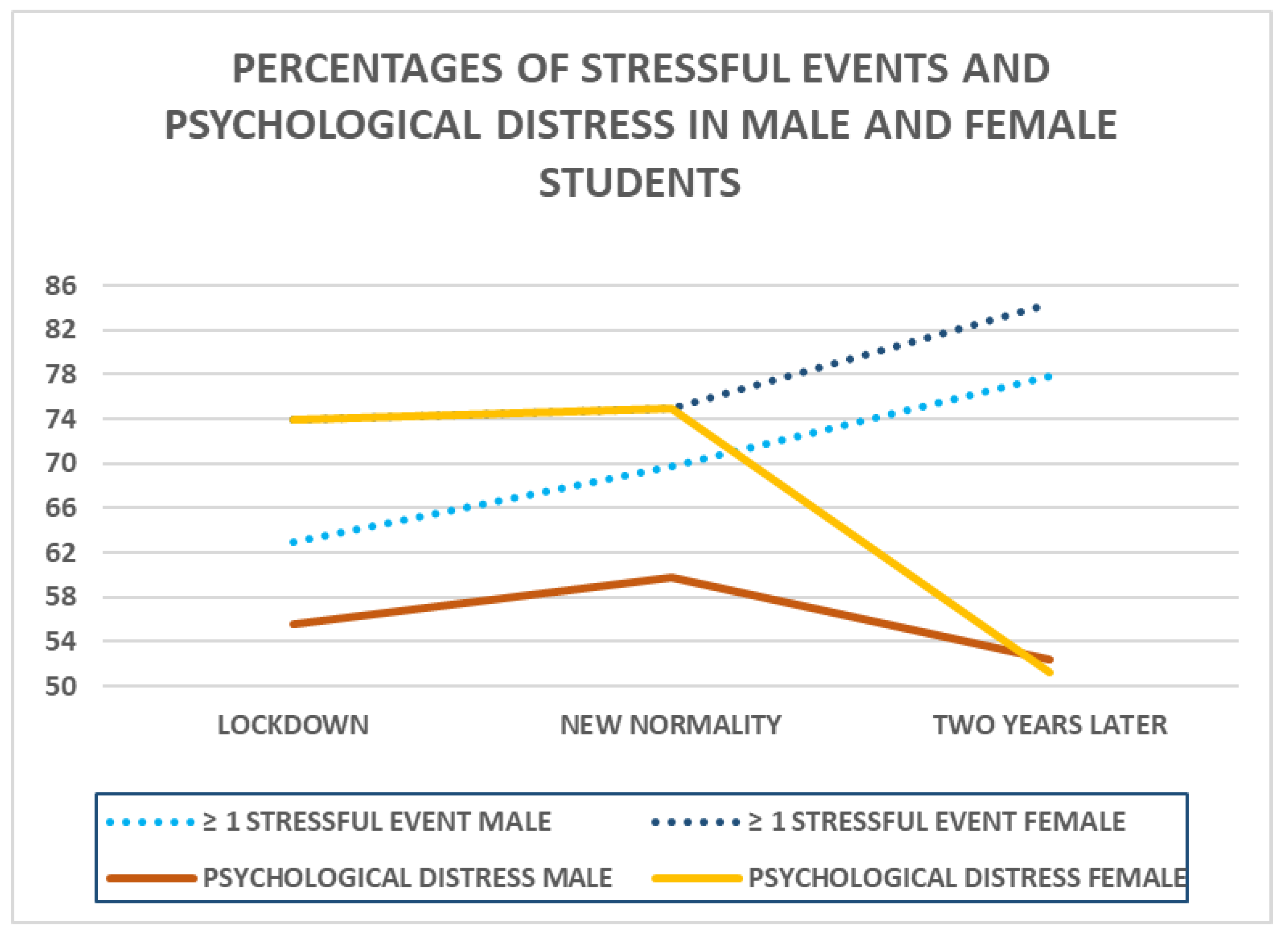
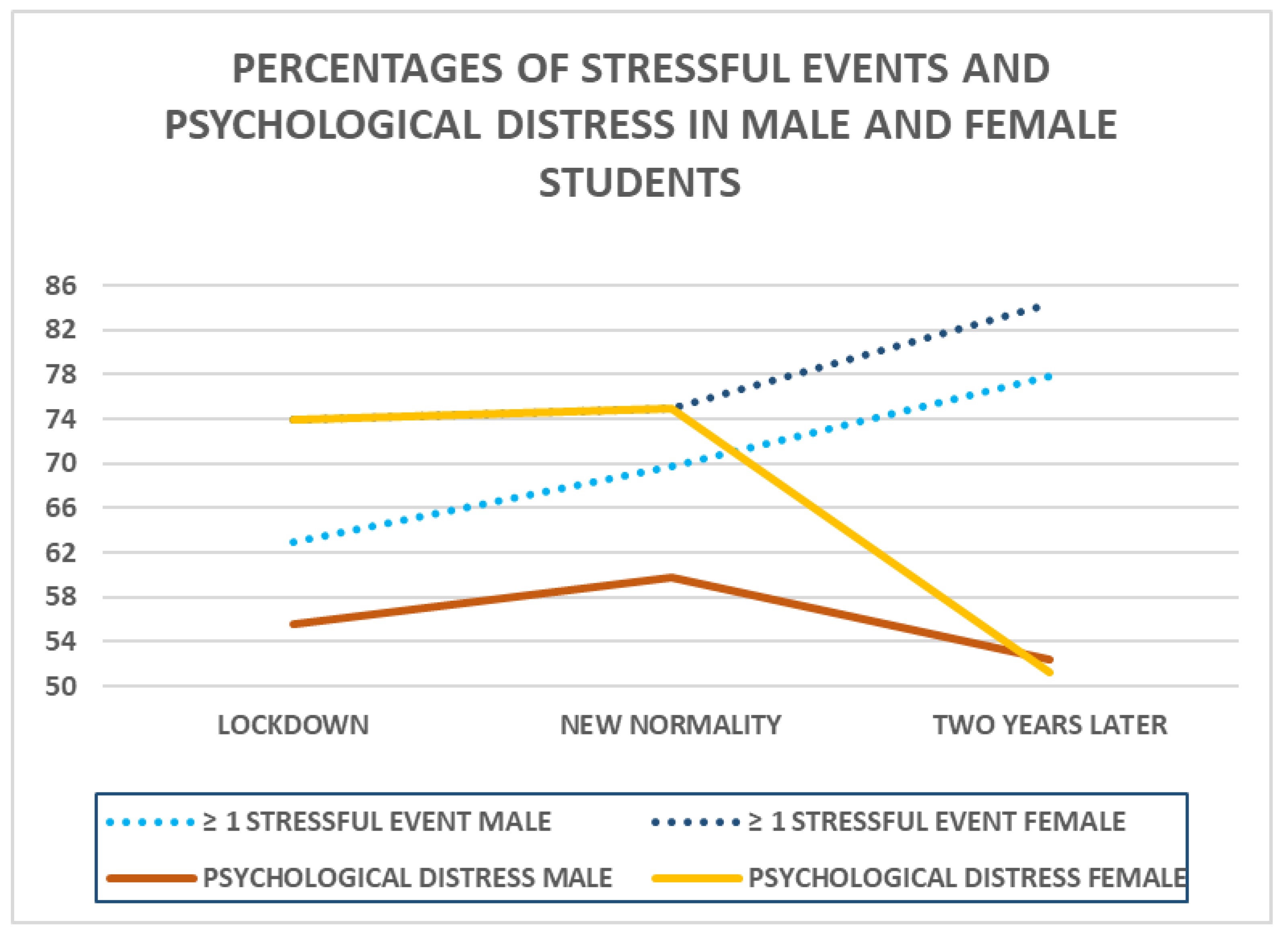
3.1. Differences in Psychological Distress and COVID-19-Associated Stressful Events
3.2. Risk and Protective Factors That Predict Psychological Distress
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19.11-March-2022 (accessed on 20 February 2023).
- Gewirtz-Meydan, A.; Lassri, D.A. Profile analysis of COVID-19 stress-related reactions: The importance of early childhood abuse, psychopathology, and interpersonal relationships. Child Abuse Negl. 2022, 130, 105442. [Google Scholar] [CrossRef]
- World Health Organization. Mental Health and Psychosocial Considerations during the COVID-19 Outbreak. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf (accessed on 20 February 2023).
- Almomani, E.Y.; Qablan, A.M.; Almomany, A.M.; Atrooz, F.Y. The coping strategies followed by university students to mitigate the COVID-19 quarantine psychological impact. Curr. Psychol. 2021, 40, 5772–5781. [Google Scholar] [CrossRef]
- Tsur, N.; Abu-Raiya, H. COVID-19-related fear and stress among individuals who experienced child abuse: The mediating effect of complex posttraumatic stress disorder. Child Abuse Negl. 2020, 110, 104694. [Google Scholar] [CrossRef]
- Mahmud, S.; Mohsin, M.; Dewan, M.N.; Muyeed, A. The global prevalence of depression, anxiety, stress, and insomnia among general population during COVID-19 pandemic: A systematic review and meta-analysis. Trends Psychol. 2023, 31, 143–170. [Google Scholar] [CrossRef]
- Cooke, J.E.; Eirich, R.; Racine, N.; Madigan, S. Prevalence of posttraumatic and general psychological stress during COVID-19: A rapid review and meta-analysis. Psychiatry Res. 2020, 292, 113347. [Google Scholar] [CrossRef] [PubMed]
- Gamonal-Limcaoco, S.; Montero-Mateos, E.; Lozano-López, M.T.; Maciá-Casas, A.; Matías-Fernández, J.; Roncero, C. Perceived stress in different countries at the beginning of the coronavirus pandemic. Int. J. Psychiatry Med. 2022, 57, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- de Sousa, G.M.; Tavares, V.; de Meiroz Grilo, M.; Coelho, M.; de Lima-Araújo, G.L.; Schuch, F.B.; Galvão-Coelho, N.L. Mental health in COVID-19 pandemic: A meta-review of prevalence meta-analyses. Front. Psychol. 2021, 12, 703838. [Google Scholar] [CrossRef]
- Al Maqbali, M.; Al Sinani, M.; Al-Lenjawi, B. Prevalence of stress, depression, anxiety and sleep disturbance among nurses during the COVID-19 pandemic: A systematic review and meta-analysis. J. Psychosom. Res. 2021, 141, 110343. [Google Scholar] [CrossRef]
- Ata, S.M.; Eltahir, M.; Albadah, A.; Harun, H.; Hadeel, H.; Alzahrani, K.T. Association between COVID-19 pandemic conditions and perceived stress level among college students in Saudi Arabia. J. Pharm. Res. Int. 2021, 33, 429–436. [Google Scholar] [CrossRef]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.A.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences of the coronavirus 2020 pandemic (COVID-19) in Spain. A Longitudinal Study. Front. Psychiatry 2020, 11, 565474. [Google Scholar] [CrossRef] [PubMed]
- Jacques-Aviñó, C.; López-Jiménez, T.; Medina-Perucha, L.; de Bont, J.; Queiroga-Gonçalves, A.; Duarte-Salles, T.; Berenguera, A. Gender-based approach on the social impact and mental health in Spain during COVID-19 lockdown: A cross-sectional study. BMJ Open 2020, 10, e044617. [Google Scholar] [CrossRef]
- Cooper, C.L.; Quick, J.C. (Eds.) The Handbook of Stress and Health: A Guide to Research and Practice; Wiley Blackwell: Hoboken, NJ, USA, 2017. [Google Scholar] [CrossRef]
- Mateos, R.; Fernández, M.; Franco, M.; Sánchez, M. COVID-19 in Spain. Coming back to the “new normality” after 2 months of confinement. Int. Psychogeriatr. 2020, 32, 1169–1172. [Google Scholar] [CrossRef]
- Santamaría, C.; Sermi, F.; Spyratos, S.; Iacus, S.M.; Annunziato, A.; Tarchi, D.; Vespe, M. Measuring the impact of COVID-19 confinement measures on human mobility using mobile positioning data. A European regional analysis. Saf. Sci. 2020, 139, 104925. [Google Scholar] [CrossRef]
- Hagedorn, R.L.; Wattick, R.A.; Olfert, M.D. “My entire world stopped”: College students’ psychosocial and academic frustrations during the COVID-19 pandemic. Appl. Res. Qual. Life 2022, 17, 1069–1090. [Google Scholar] [CrossRef] [PubMed]
- Manchia, M.; Gathier, A.W.; Yapici-Eser, H.; Schmidt, M.V.; de Quervain, D.; van Amelsvoort, T.; Bisson, J.I.; Cryan, J.F.; Howes, O.D.; Pinto, L.; et al. The impact of the prolonged COVID-19 pandemic on stress resilience and mental health: A critical review across waves. Eur. Neuropsychopharmacol. 2022, 55, 22–83. [Google Scholar] [CrossRef]
- Lanza, S.T.; Whetzel, C.A.; Linden-Carmichael, A.N.; Newschaffer, C.J. Change in college student health and well-being profiles as a function of the COVID-19 pandemic. PLoS ONE 2022, 17, e0267724. [Google Scholar] [CrossRef]
- von Keyserlingk, L.; Yamaguchi-Pedroza, K.; Arum, R.; Eccles, J.S. Stress of university students before and after campus closure in response to COVID-19. J. Community Psychol. 2022, 50, 285–301. [Google Scholar] [CrossRef]
- Wang, C.; Havewala, M.; Zhu, Q. COVID-19 stressful life events and mental health: Personality and coping styles as moderators. J. Am. Coll. Health. 2022, 26, 1–10. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on University Students’ Mental Health in the United States: Interview Survey Study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef]
- Saikkonen, S.; Karukivi, M.; Vahlberg, T.; Saarijärvi, S. Associations of social support and alexithymia with psychological distress in Finnish young adults. Scand. J. Psychol. 2018, 59, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Arnett, J.J. Emerging Adulthood: The Winding Road from the Late Teens through the Twenties, 2nd ed.; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Lane, J.A.; Leibert, T.W.; Goka-Dubose, E. The impact of life transition on emerging adult attachment, social support, and well-being: A multiple-group comparison. J. Couns. Dev. 2017, 95, 378–388. [Google Scholar] [CrossRef]
- Doherty, D.T.; Kartalova-O’Doherty, Y. Gender and self-reported mental health problems: Predictors of help seeking from a general practitioner. Br. J. Health Psychol. 2010, 15, 213–228. [Google Scholar] [CrossRef] [PubMed]
- Weissman, J.; Russell, D.; Mann, J. Sociodemographic characteristics, financial worries and serious psychological distress in U.S. adults. Community Men. Health J. 2020, 56, 606–613. [Google Scholar] [CrossRef]
- Drapeau, A.; Marchand, A.; Beaulieu-Prévost, D. Epidemiology of Psychological Distress. In Mental Illnesses; L’Abata, L., Ed.; InTech: Rieka, Croatia, 2011; pp. 105–123. [Google Scholar] [CrossRef]
- Twenge, J.M.; Cooper, A.B.; Joiner, T.E.; Duffy, M.E.; Binau, S.G. Age, period, and cohort trends in mood disorder indicators and suicide-related outcomes in a nationally representative dataset, 2005–2017. J. Abnorm. Psychol. 2019, 128, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Auerbach, R.P.; Mortier, P.; Bruffaerts, R.; Alonso, J.; Benjet, C.; Cuijpers, P.; Demyttenaere, K.; Ebert, D.D.; Green, J.G.; Hasking, P.; et al. WHO World Mental Health Surveys International University Student Project: Prevalence and distribution of mental disorders. J. Abnorm. Psychol. 2018, 127, 623–638. [Google Scholar] [CrossRef]
- Tang, F.; Byrne, M.; Qin, P. Psychological distress and risk for suicidal behavior among university students in contemporary China. J. Affect Disord. 2018, 228, 101–108. [Google Scholar] [CrossRef]
- Adefris, D.; Moges, B. The psychological impact and coping of Covid-19 pandemic among Arsi university students-Ethiopia. Curr. Psychol. 2023, 42, 2415–2421. [Google Scholar] [CrossRef]
- Bulut, N.S.; Yorguner, N.; Akvardar, Y. Impact of COVID-19 on the life of higher-education students in İstanbul: Relationship between social support, health-risk behaviors, and mental/academic well-being. Alpha Psychiat. 2021, 22, 291–300. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: Berlin/Heidelberg, Germany, 1984. [Google Scholar]
- Biggs, A.; Brough, P.; Drummond, S. Lazarus and Folkman’s psychological stress and coping theory. In The Handbook of Stress and Health: A Guide to Research and Practice; Cooper, C.L., Quick, J.C., Eds.; Wiley Blackwell: Oxford, UK, 2017; pp. 351–364. [Google Scholar] [CrossRef]
- Kowal, M.; Coll-Martín, T.; Ikizer, G.; Rasmussen, J.; Eichel, K.; Studzińska, A.; Koszałkowska, K.; Karwowski, M.; Najmussaqib, A.; Pankowski, D.; et al. Who is the Most Stressed during the COVID-19 Pandemic? Data from 26 Countries and Areas. Appl. Psychol. Health Well Being 2020, 12, 946–966. [Google Scholar] [CrossRef]
- Lelek-Kratiuk, M.; Szczygieł, M. Stress appraisal as a mediator between the sense of coherence and the frequency of stress coping strategies in women and men during COVID-19 lockdown. Scand. J. Psychol. 2022, 63, 365–375. [Google Scholar] [CrossRef]
- Li, X.; Wu, H.; Meng, F.; Li, L.; Wang, Y.; Zhou, M. Relations of COVID-19-related stressors and social support with Chinese college students’ psychological response during the COVID-19 pandemic. Front. Psychiatry 2020, 11, 551315. [Google Scholar] [CrossRef]
- House, J.S. Work Stress and Social Support; Madison Wesley: Reading, MA, USA, 1981. [Google Scholar]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Allen, S.F.; Stoltenberg, C.D. Psychological separation of older adolescents and young adults from their parents: An investigation of gender differences. J. Couns. Dev. 1995, 73, 542–546. [Google Scholar] [CrossRef]
- Matud, M.P.; Zueco, J.; Díaz, A.; Del Pino, M.J.; Fortes, D. Gender differences in mental distress and affect balance during the first wave of COVID-19 pandemic in Spain. Curr. Psychol. 2023, 42, 21790–21804. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M. Rosenberg self-esteem scale (RSE): Acceptance and commitment therapy. Measur. Pack 1965, 61, 52. [Google Scholar]
- Goodwin, R.; Costa, P.; Adonu, J. Social support and its consequences: ‘Positive’ and ‘deficiency’ values and their implications for support and self-esteem. Br. J. Soc. Psychol. 2004, 43, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.; Zhao, J.; You, X. Self-esteem as mediator and moderator of the relationship between social support and subjective well-being among Chinese university students. Soc. Indic. Res. 2013, 112, 151–161. [Google Scholar] [CrossRef]
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O.; Rutter, C. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef]
- Lundin, A.; Åhs, J.; Åsbring, N.; Kosidou, K.; Dal, H.; Tinghög, P.; Saboonchi, F.; Dalman, C. Discriminant validity of the 12-item version of the general health questionnaire in a Swedish case-control study. Nord. J. Psychiatry 2017, 71, 171–179. [Google Scholar] [CrossRef]
- Matud, M.P. Social Support Scale; Database Record; APA PsycTESTS: Washington, DC, USA, 1998. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Jiménez, M.; Guerrero-Barona, E.; García-Gómez, A. Mental health and psychological capital among Spanish health care workers during COVID-19 pandemic. Med. Clin. 2021, 156, 357–358. [Google Scholar] [CrossRef]
- Rens, E.; Smith, P.; Nicaise, P.; Lorant, V.; Van den Broeck, K. Mental distress and its contributing factors among young people during the first wave of COVID-19: A Belgian survey study. Front. Psychiatry 2021, 12, 575553. [Google Scholar] [CrossRef] [PubMed]
- Arias-de la Torre, J.; Fernández-Villa, T.; Molina, A.J.; Amezcua-Prieto, C.; Mateos, R.; Cancela, J.M.; Delgado-Rodríguez, M.; Ortíz-Moncada, R.; Alguacil, J.; Redondo, S.; et al. Psychological distress, family support and employment status in first-year university students in Spain. Int. J. Environ. Res. Public Health 2019, 16, 1209. [Google Scholar] [CrossRef]
- Dongol, E.; Shaker, K.; Abbas, A.; Assar, A.; Abdelraoof, M.; Saady, E.; Hassan, A.; Youssef, O.; Essam, M.; Mahmoud, M.; et al. Sleep quality, stress level and COVID-19 in university students; the forgotten dimension. Sleep Sci. 2022, 15, 347–354. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19. Spain Situation. Available online: https://covid19.who.int/region/euro/country/es (accessed on 12 September 2023).
- Prout, T.A.; Zilcha-Mano, S.; Aafjes-van Doorn, K.; Békés, V.; Christman-Cohen, I.; Whistler, K.; Kui, T.; Di Giuseppe, M. Identifying predictors of psychological distress during COVID-19: A machine learning approach. Front. Psychol. 2020, 11, 586202. [Google Scholar] [CrossRef]
- Krauss, S.; Orth, U.; Robins, R.W. Family environment and self-esteem development: A longitudinal study from age 10 to 16. J. Pers. Soc. Psychol. 2020, 119, 457–478. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Yang, X.; Zeng, C.; Wang, Y.; Shen, Z.; Li, X.; Lin, D. Resilience, social support, and coping as mediators between COVID-19-related stressful experiences and acute stress disorder among university students in China. Appl. Psychol. Health Well-Being 2020, 12, 1074–1094. [Google Scholar] [CrossRef]

{kind=link}
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | B | SE B | β | B | SE B | β | B | SE B | β | B | SE B | β |
| MALE (n = 189) | ||||||||||||
| Age | 0.16 | 0.19 | 0.06 | 0.21 | 0.18 | 0.08 | 0.27 | 0.18 | 0.11 | 0.43 | 0.17 | 0.12 |
| Social Support | −0.28 | 0.06 | −0.32 *** | −0.25 | 0.06 | −0.29 *** | −0.11 | 0.06 | −0.14 * | |||
| Stressful Events | 1.02 | 0.38 | 0.19 ** | 0.77 | 0.35 | 0.14 * | ||||||
| Self-Esteem | −0.53 | 0.09 | −0.41 *** | |||||||||
| R2 | 0.01 | 0.11 | 0.14 | 0.27 | ||||||||
| F for change in R2 | 0.74 | 21.33 *** | 7.23 ** | 33.34 *** | ||||||||
| 1 − β | 0.55 | 0.87 | 1 | 1 | ||||||||
| f2 | 0.04 | 0.12 | 0.16 | 0.37 | ||||||||
| FEMALE (n = 211) | ||||||||||||
| Age | −0.21 | 0.20 | −0.07 | −0.20 | 0.19 | −0.07 | −0.27 | 0.18 | −0.09 | −0.00 | 0.17 | 0.00 |
| Social Support | −0.22 | 0.06 | −0.25 *** | −0.13 | 0.06 | −0.15 * | −0.02 | 0.05 | −0.03 | |||
| Stressful Events | 2.20 | 0.36 | 0.39 *** | 1.62 | 0.34 | 0.29 *** | ||||||
| Self-Esteem | −0.60 | 0.09 | −0.44 *** | |||||||||
| R2 | 0.01 | 0.07 | 0.21 | 0.36 | ||||||||
| F for change in R2 | 1.09 | 13.41 *** | 37.31 *** | 48.48 *** | ||||||||
| 1 − β | 0.66 | 0.63 | 1 | 1 | ||||||||
| f2 | 0.01 | 0.07 | 0.27 | 0.56 | ||||||||
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | B | SE B | β | B | SE B | β | B | SE B | β | B | SE B | β |
| MALE (n = 189) | ||||||||||||
| Age | −0.04 | 0.22 | −0.01 | −0.06 | 0.22 | −0.02 | −0.05 | 0.21 | −0.02 | 0.06 | 0.19 | 0.02 |
| Social Support | −0.16 | 0.07 | −0.18 * | −0.13 | 0.06 | −0.14 * | 0.05 | 0.06 | 0.06 | |||
| Stressful Events | 1.62 | 0.39 | 0.29 *** | 1.44 | 0.34 | 0.26 *** | ||||||
| Self-Esteem | −0.73 | 0.10 | −0.51 *** | |||||||||
| R2 | 0.00 | 0.03 | 0.12 | 0.33 | ||||||||
| F for change in R2 | 0.03 | 6.41 * | 17.39 *** | 58.48 *** | ||||||||
| 1 − β | 0.00 | 0.35 | 0.88 | 1 | ||||||||
| f2 | 0.00 | 0.03 | 0.14 | 0.49 | ||||||||
| FEMALE (n = 211) | ||||||||||||
| Age | 0.18 | 0.24 | 0.05 | 0.06 | 0.23 | 0.02 | 0.11 | 0.22 | 0.03 | 0.17 | 0.19 | 0.05 |
| Social Support | −0.24 | 0.07 | −0.24 *** | −0.20 | 0.07 | −0.20 ** | −0.03 | 0.06 | −0.03 | |||
| Stressful Events | 1.45 | 0.31 | 0.30 *** | 1.30 | 0.27 | 0.27 *** | ||||||
| Self-Esteem | −0.69 | 0.08 | −0.50 *** | |||||||||
| R2 | 0.03 | 0.06 | 0.15 | 0.36 | ||||||||
| F for change in R2 | 0.55 | 12.13 *** | 21.51 *** | 70.03 *** | ||||||||
| 1 − β | 0.97 | 0.59 | 0.98 | 1 | ||||||||
| f2 | 0.03 | 0.06 | 0.18 | 0.56 | ||||||||
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | B | SE B | β | B | SE B | β | B | SE B | β | B | SE B | β |
| MALE (n = 189) | ||||||||||||
| Age | −0.29 | 0.22 | −0.01 | −0.37 | 0.20 | −0.12 | −0.42 | 0.20 | −0.14 * | −0.22 | 0.17 | −0.07 |
| Social Support | −0.31 | 0.05 | −0.40 *** | −0.29 | 0.05 | −0.38 *** | −0.10 | 0.04 | −0.13 * | |||
| Stressful Events | 0.55 | 0.27 | 0.14 * | 0.23 | 0.23 | 0.06 | ||||||
| Self-Esteem | −0.73 | 0.08 | −0.59 *** | |||||||||
| R2 | 0.01 | 0.17 | 0.19 | 0.46 | ||||||||
| F for change in R2 | 1.75 | 35.84 *** | 4.09 * | 91.40 *** | ||||||||
| 1 − β | 0.28 | 1 | 1 | 1 | ||||||||
| f2 | 0.01 | 0.21 | 0.24 | 0.85 | ||||||||
| FEMALE (n = 211) | ||||||||||||
| Age | 0.79 | 0.25 | 0.22 ** | 0.70 | 0.23 | 19 ** | 0.61 | 0.23 | 0.17 ** | 0.30 | 0.20 | 0.08 |
| Social Support | −0.32 | 0.06 | −0.32 *** | −0.25 | 0.07 | −0.25 *** | −0.06 | 0.06 | −0.06 | |||
| Stressful Events | 0.92 | 0.30 | 0.21 ** | 0.52 | 0.26 | 0.12 * | ||||||
| Self-Esteem | −0.68 | 0.08 | −0.52 *** | |||||||||
| R2 | 0.05 | 0.15 | 0.18 | 0.39 | ||||||||
| F for change in R2 | 10.25 ** | 24.38 *** | 9.55 ** | 69.70 *** | ||||||||
| 1 − β | 0.91 | 1 | 1 | 1 | ||||||||
| f2 | 0.05 | 0.18 | 0.22 | 0.64 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matud, M.P.; Zueco, J.; Del Pino-Espejo, M.J.; Fortes, D.; Beleña, M.Á.; Santos, C.; Díaz, A. The Evolution of Psychological Distress Levels in University Students in Spain during Different Stages of the COVID-19 Pandemic: Risk and Protective Factors. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 2583-2598. https://doi.org/10.3390/ejihpe13110180
Matud MP, Zueco J, Del Pino-Espejo MJ, Fortes D, Beleña MÁ, Santos C, Díaz A. The Evolution of Psychological Distress Levels in University Students in Spain during Different Stages of the COVID-19 Pandemic: Risk and Protective Factors. European Journal of Investigation in Health, Psychology and Education. 2023; 13(11):2583-2598. https://doi.org/10.3390/ejihpe13110180
Chicago/Turabian StyleMatud, María Pilar, Jesús Zueco, Maria José Del Pino-Espejo, Demelsa Fortes, María Ángeles Beleña, Cristina Santos, and Amelia Díaz. 2023. "The Evolution of Psychological Distress Levels in University Students in Spain during Different Stages of the COVID-19 Pandemic: Risk and Protective Factors" European Journal of Investigation in Health, Psychology and Education 13, no. 11: 2583-2598. https://doi.org/10.3390/ejihpe13110180
APA StyleMatud, M. P., Zueco, J., Del Pino-Espejo, M. J., Fortes, D., Beleña, M. Á., Santos, C., & Díaz, A. (2023). The Evolution of Psychological Distress Levels in University Students in Spain during Different Stages of the COVID-19 Pandemic: Risk and Protective Factors. European Journal of Investigation in Health, Psychology and Education, 13(11), 2583-2598. https://doi.org/10.3390/ejihpe13110180