
Pseudorandom Noise Forced Oscillation Technique to Assess Lung Function in Prematurely Born Children


Abstract
:1. Introduction
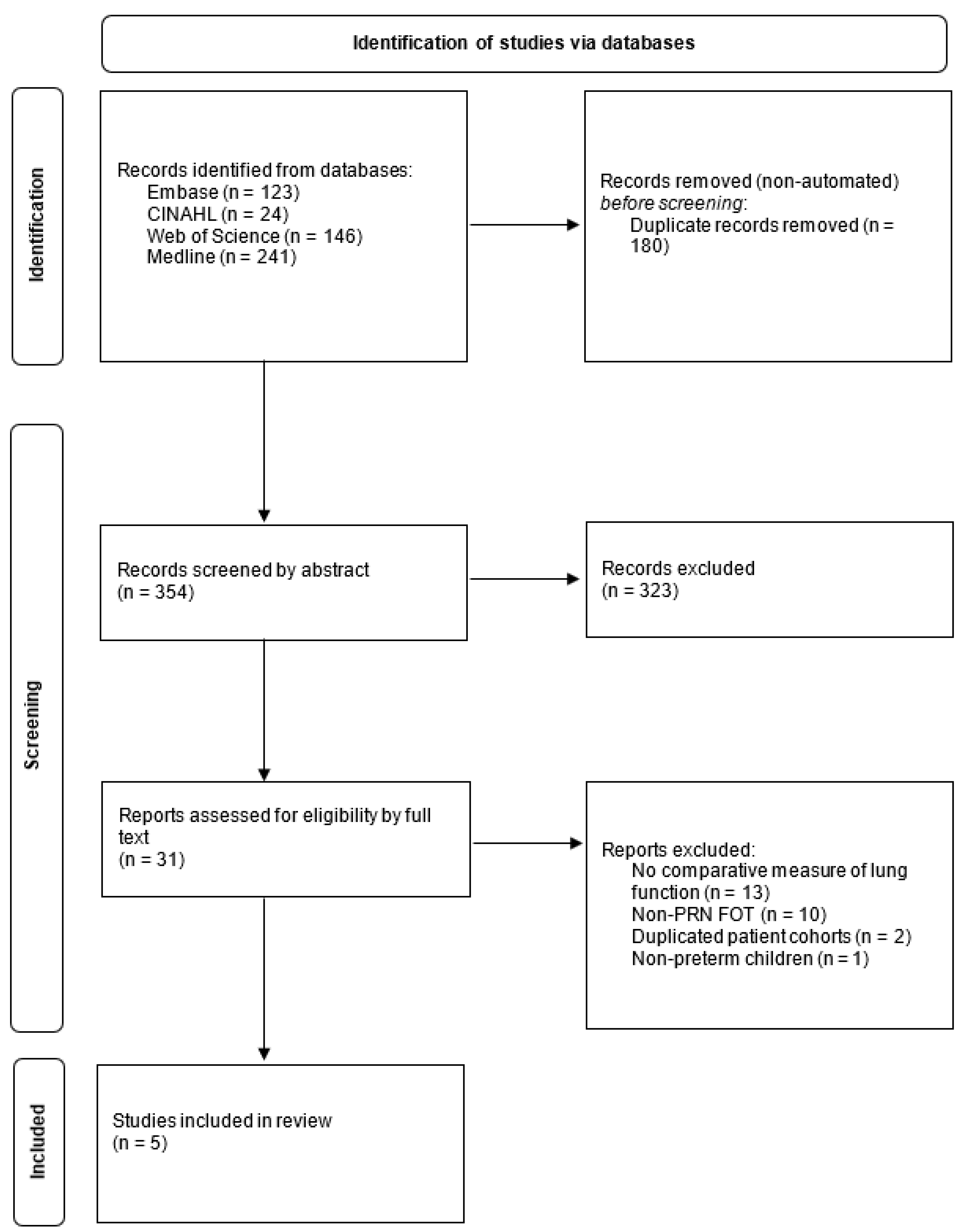
2. Materials and Methods
3. Results
3.1. Device Methodology
3.2. Characteristics of Cohorts Studied
3.3. PRN FOT Compared to Other Lung-Function Tests
3.4. Correlation with Symptoms and Hospitalization
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, A.C.; Blencowe, H.; Lawn, J.E. Small babies, big numbers: Global estimates of preterm birth. Lancet Glob Health 2019, 7, e2–e3. [Google Scholar] [CrossRef] [Green Version]
- Costeloe, K.L.; Hennessy, E.M.; Haider, S.; Stacey, F.; Marlow, N.; Draper, E.S. Short term outcomes after extreme preterm birth in England: Comparison of two birth cohorts in 1995 and 2006 (the EPICure studies). BMJ 2012, 345, e7976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheong, J.L.Y.; Olsen, J.E.; Huang, L.; Dalziel, K.M.; Boland, R.A.; Burnett, A.C.; Haikerwal, A.; Spittle, A.J.; Opie, G.; Stewart, A.E.; et al. Changing consumption of resources for respiratory support and short-term outcomes in four consecutive geographical cohorts of infants born extremely preterm over 25 years since the early 1990s. BMJ Open 2020, 10, e037507. [Google Scholar] [CrossRef] [PubMed]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef] [PubMed]
- Siffel, C.; Kistler, K.D.; Lewis, J.F.M.; Sarda, S.P. Global incidence of bronchopulmonary dysplasia among extremely preterm infants: A systematic literature review. J. Matern.-Fetal Neonatal Med. 2021, 34, 1721–1731. [Google Scholar] [CrossRef] [Green Version]
- Doyle, L.W.; Ranganathan, S.; Cheong, J.; Victorian Infant Collaborative Study, G. Bronchopulmonary dysplasia and expiratory airflow at 8 years in children born extremely preterm in the post-surfactant era. Thorax 2022. [Google Scholar] [CrossRef]
- Ronkainen, E.; Dunder, T.; Peltoniemi, O.; Kaukola, T.; Marttila, R.; Hallman, M. New BPD predicts lung function at school age: Follow-up study and meta-analysis. Pediatric Pulmonol. 2015, 50, 1090–1098. [Google Scholar] [CrossRef]
- Dubois, A.B.; Brody, A.W.; Lewis, D.H.; Burgess, B.F., Jr. Oscillation mechanics of lungs and chest in man. J. Appl. Physiol 1956, 8, 587–594. [Google Scholar] [CrossRef]
- King, G.G.; Bates, J.; Berger, K.I.; Calverley, P.; de Melo, P.L.; Dellaca, R.L.; Farre, R.; Hall, G.L.; Ioan, I.; Irvin, C.G.; et al. Technical standards for respiratory oscillometry. Eur. Respir. J. 2020, 55, 1900753. [Google Scholar] [CrossRef]
- Smith, H.; Reinhold, P.; Goldman, M. Forced oscillation technique and impulse oscillometry. Eur. Respir. Monogr. 2005, 31, 72. [Google Scholar]
- Wells, G.; Shea, B.; O’Connell, J. The Newcastle-Ottawa Scale (NOS) for Assessing The Quality of Nonrandomised Studies in Meta-analyses. In Ottawa Health Research Institute Web Site; Ottawa Health Research Institute: Ottawa, ON, Cnanda, 2014; Volume 7. [Google Scholar]
- Accorsi, B.F.; Friedrich, F.O.; Corso, A.L.; da Rosa, J.P.; Jones, M.H. Intra-breath oscillometry for the evaluation of lung function in children and adolescents with a history of preterm birth. J. Bras. Pneumol. 2022, 48, e20210290. [Google Scholar] [CrossRef] [PubMed]
- Hall, G.L.; Sly, P.D.; Fukushima, T.; Kusel, M.M.; Franklin, P.J.; Horak, F.; Patterson, H.; Gangell, C.; Stick, S.M. Respiratory function in healthy young children using forced oscillations. Thorax 2007, 62, 521–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrijlandt, E.J.; Boezen, H.M.; Gerritsen, J.; Stremmelaar, E.F.; Duiverman, E.J. Respiratory health in prematurely born preschool children with and without bronchopulmonary dysplasia. J. Pediatrics 2007, 150, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Simpson, S.J.; Logie, K.M.; O’Dea, C.A.; Banton, G.L.; Murray, C.; Wilson, A.C.; Pillow, J.J.; Hall, G.L. Altered lung structure and function in mid-childhood survivors of very preterm birth. Thorax 2017, 72, 702–711. [Google Scholar] [CrossRef]
- Lombardi, E.; Fainardi, V.; Calogero, C.; Puglia, M.; Voller, F.; Cuttini, M.; Rusconi, F. Lung function in a cohort of 5-year-old children born very preterm. Pediatric Pulmonol. 2018, 53, 1633–1639. [Google Scholar] [CrossRef]
- Verheggen, M.; Wilson, A.C.; Pillow, J.J.; Stick, S.M.; Hall, G.L. Respiratory function and symptoms in young preterm children in the contemporary era. Pediatric Pulmonol. 2016, 51, 1347–1355. [Google Scholar] [CrossRef]
- Soon, B.T. The Global Action Report on Preterm Birth; World Health Organization: Geneva, Switzerland, 2012.
- Kampschmidt, J.C.; Brooks, E.G.; Cherry, D.C.; Guajardo, J.R.; Wood, P.R. Feasibility of spirometry testing in preschool children. Pediatric Pulmonol. 2016, 51, 258–266. [Google Scholar] [CrossRef]
- Tirakitsoontorn, P.; Crookes, M.; Fregeau, W.; Pabelonio, N.; Morphew, T.; Shin, H.W.; Galant, S.P. Recognition of the peripheral airway impairment phenotype in children with well-controlled asthma. Ann. Allergy Asthma Immunol. 2018, 121, 692–698. [Google Scholar] [CrossRef]
- Bjorn, L.; Erik, M.; Per, T.; Mikael, N.; Jenny, H. Agreement between spirometry and impulse oscillometry for lung function assessment in 6-year-old children born extremely preterm and at term. Pediatric Pulmonol. 2020, 55, 2745–2753. [Google Scholar] [CrossRef]
- Durlak, W.; Klimek, M.; Wronski, M.; Trybulska, A.; Kwinta, P. Multimodal longitudinal respiratory function assessment in very low birth weight 7-year-old children. Adv. Med. Sci. 2021, 66, 81–88. [Google Scholar] [CrossRef]
- Hellinckx, J.; Cauberghs, M.; De Boeck, K.; Demedts, M. Evaluation of impulse oscillation system: Comparison with forced oscillation technique and body plethysmography. Eur. Respir. J. 2001, 18, 564–570. [Google Scholar] [CrossRef] [Green Version]
- Oostveen, E.; Boda, K.; van der Grinten, C.P.; James, A.L.; Young, S.; Nieland, H.; Hantos, Z. Respiratory impedance in healthy subjects: Baseline values and bronchodilator response. Eur. Respir. J. 2013, 42, 1513–1523. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, S.C.; Watts, J.C.; Bertolin, A.; Jetmalani, K.; King, G.G.; Thamrin, C. Discrepancy between in vivo and in vitro comparisons of forced oscillation devices. J. Clin. Monit. Comput. 2018, 32, 509–512. [Google Scholar] [CrossRef] [PubMed]
- Calogero, C.; Simpson, S.J.; Lombardi, E.; Parri, N.; Cuomo, B.; Palumbo, M.; de Martino, M.; Shackleton, C.; Verheggen, M.; Gavidia, T.; et al. Respiratory impedance and bronchodilator responsiveness in healthy children aged 2–13 years. Pediatric Pulmonol. 2013, 48, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Thamrin, C.; Robinson, P.D.; Farah, C.S.; King, G.G. Technical standards for respiratory oscillometry and bronchodilator response cut-offs. Eur. Respir. J. 2022, 59, 2102663. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; van der Grinten, C.P.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef]
- Duiverman, E.J.; Clement, J.; Van De Woestijne, K.P.; Neijens, H.J.; Bergh, A.C.V.D.; Kerrebijn, K.F. Forced oscillation technique. Reference values for resistance and reactance over a frequency spectrum of 2–26 Hz in healthy children aged 2.3–12.5 years. Clin. Respir. Physiol. 1985, 21, 171–178. [Google Scholar]
- Calogero, C.; Parri, N.; Fenu, G.; Cuomo, B.; Palumbo, M.; Novembre, E.; Azzari, C.; De Martino, M.; Sly, P.D.; Lombardi, E. Respiratory impedance in healthy italian children aged 3 to 18 years. Am. J. Respir. Crit. Care Med. 2010, 181, A3920. [Google Scholar]
- Navanandan, N.; Hamlington, K.L.; Mistry, R.D.; Szefler, S.J.; Liu, A.H. Oscillometry for acute asthma in the pediatric emergency department: A feasibility study. Ann. Allergy Asthma Immunol. 2020, 125, 607–609. [Google Scholar] [CrossRef]
- Timmins, S.C.; Diba, C.; Thamrin, C.; Berend, N.; Salome, C.M.; King, G.G. The feasibility of home monitoring of impedance with the forced oscillation technique in chronic obstructive pulmonary disease subjects. Physiol. Meas. 2013, 34, 67–81. [Google Scholar] [CrossRef]


{kind=link}
| Author | Lung-Function Measures | Study Groups | Preterm (n) | Female (%) | Age (years) | GA (Weeks) | PRN FOT | Spirometry | Intra-Breath Oscillometry | Interrupter Technique (Rint) |
|---|---|---|---|---|---|---|---|---|---|---|
| Accorsi et al. [12] | PRN FOT; Spirometry; Intra-breath FOT | Term; preterm | 35 | 51 | 12.9 (12.8–13.4) | 33.5 +/− 1.5 | Lower X6, X10 and Fres in preterm, not statistically significant | FVC, FEV1, FEV1/FVC and FEF25-75 all lower in preterm vs. term, not statistically significant | Lower change in resistance (0.06 vs. 0.46, p = 0.003), reactance at end-inspiration (−0.28 vs. −0.06, p = 0.027) in preterm | N/A |
| Lombardi et al. | PRN FOT; interrupter technique | BPD preterm; non-BPD preterm | 194 | 46 | 5.2 (4.5–6.3) * | 28 (25–31) * | Lower R8, X8 and AX in BPD vs. non-BPD groups, not statistically significant | N/A | N/A | Lower Rint score in BPD vs. non-BPD groups, not statistically significant |
| Simpson et al. | PRN FOT; spirometry; DLCO; multiple breath washout | Term: BPD preterm; non-BPD preterm | 163 | 39 | 10.9 +/− 0.6 | 28.5 (25.0–29.6) | Lower X8 (−0.43 vs. 0.14, p < 0.05), higher AX (0.29 vs. −0.44, p < 0.001) and higher Fres (0.64 vs. −0.18 p < 0.05) in preterm vs. term | Lower FEV1 (−0.72 vs. 0.04, p < 0.001), FEV1/FVC (−1.25 vs. −0.27, p < 0.001), FEF25-75 (−1.46 vs. −0.42, p < 0.001) in preterm vs. term | N/A | N/A |
| Verheggen et al. | PRN FOT; spirometry | Term; BPD preterm; non-BPD preterm | 118 | 40 | BPD: 5.8 (4.4–7.3) **; Non-BPD: 6.0 (4.6–7.8) ** | BPD: 26.1 (24.2–30.2) **; non-BPD: 29.4 (27.7–30.5) | Lower X8 in BPD vs. non-BPD preterm groups (−1.48 vs. −0.89, p < 0.02) | Lower FEV1 and FEV1/FVC in BPD vs. non-BPD groups, not statistically significant | N/A | N/A |
| Vrijlandt et al. | PRN FOT: interrupter technique | Term; BPD preterm; non-BPD preterm | 77 | 48 | BPD: 4.7 +/− 0.8; non-BPD: 4.8 +/− 0.8 | BPD: 28 +/− 2 non-BPD: 29 +/− 2 | Higher Fres (26.8 vs. 22.7, p = 0.001) and lower X4-24 (−3.0 vs. −1.95, p = 0.008) in BPD vs. non-BPD preterm groups | N/A | N/A | No significant differences between the groups |
| Author | Selection | Comparability | Outcome | Total | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representative of the Exposed Cohort | Selection of the Non-Exposed Cohort | Ascertainment of Exposure | Demonstration That Outcome of Interest Was Not Present at Start of Study | Comparability of Cohorts on the Basis of the Design or Analysis | Assessment of Outcome | Was Follow-Up Long Enough for Outcomes to Occur? | Adequacy of Follow-Up of Cohorts | ||
| Accorsi | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 5 |
| Lombardi | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Simpson | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Verheggen | 0 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 7 |
| Vrijlandt | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 6 |
| Author | X8 | R8 | AX |
|---|---|---|---|
| Lombardi | −0.28 | −0.03 | 0.29 |
| Simpson | −0.43 | 0.33 | 0.29 |
| Verheggen | −1.25 | 0.54 | 1.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gunawardana, S.; Harris, C.; Greenough, A. Pseudorandom Noise Forced Oscillation Technique to Assess Lung Function in Prematurely Born Children. Children 2022, 9, 1267. https://doi.org/10.3390/children9081267
Gunawardana S, Harris C, Greenough A. Pseudorandom Noise Forced Oscillation Technique to Assess Lung Function in Prematurely Born Children. Children. 2022; 9(8):1267. https://doi.org/10.3390/children9081267
Chicago/Turabian StyleGunawardana, Shannon, Christopher Harris, and Anne Greenough. 2022. "Pseudorandom Noise Forced Oscillation Technique to Assess Lung Function in Prematurely Born Children" Children 9, no. 8: 1267. https://doi.org/10.3390/children9081267
APA StyleGunawardana, S., Harris, C., & Greenough, A. (2022). Pseudorandom Noise Forced Oscillation Technique to Assess Lung Function in Prematurely Born Children. Children, 9(8), 1267. https://doi.org/10.3390/children9081267