Abstract
Background: Child abuse and neglect (CAN) is considered a serious problem worldwide. Dentists have a significant role in recognizing and reporting CAN cases. Aim: The aim of this study was to assess the CAN-related knowledge and educational experiences among Saudi dental graduates. Design: Self-administered questionnaires were distributed to dental graduates from all dental schools in Saudi Arabia (n = 1552). Bivariate and multivariate logistic regression analyses were performed to assess the associations between knowledge level and different predictors. Results: A total of 988 dental graduates completed the questionnaire. The majority of them were dissatisfied with the amount of education they had received in their school (56.4%). Around 60% of the participants had inadequate knowledge regarding CAN. Graduates from government schools who received dental education about CAN and female participants had significantly higher odds of having adequate knowledge scores than others (odds ratio = 2.0, 3.1, and 1.7, respectively). Only 39.5% of the participants felt confident in their ability to identify CAN cases, and only 9.7% knew how to report such cases. Conclusions: Graduate dental students have insufficient knowledge about CAN. More time should be dedicated to educating students about this important topic in dental curricula.
1. Introduction
The World Health Organization (WHO) defines child abuse and neglect (CAN) as: child abuse or maltreatment constitutes all forms of physical and/or emotional ill-treatment, sexual abuse, neglect or negligent treatment or commercial or other exploitation, resulting in actual or potential harm to the child’s health, survival, development or dignity in the context of a relationship of responsibility, trust or power [1].
CAN is a serious phenomenon that has long-term negative effects on children’s lives and their communities [2]. The effects of CAN may exhibit as inappropriate changes in a child’s physical, social, psychological, and cognitive health [3]. There might be physical injuries noticed immediately, but the impact of CAN can lead to a disturbed mental state, along with behavioral changes [3]. Children with a history of witnessing CAN are more prone to conditions such as malnutrition, vision disturbances, hypertension, diabetes mellitus, and cardiac problems [3], with high chances of several psychological problems such as stress, anxiety, the development of an inferiority complex, low productivity, a lack of social skills, and depression [3].
According to a WHO report published in 2020, every three out of four children aged two to four years suffer physical or psychological violence. One in every five women reports sexual abuse during their childhood, and one in every three men report the same [4]. In the United States, the Centers for Disease Control and Prevention (CDC) stated in 2021 that one in every seven children had faced CAN in the previous year. A previous report published by the CDC reported 1840 deaths of children due to CAN in the United States in 2019 [5]. In Saudi Arabia, the National Family Safety Program reported the registration of 616 CAN cases in 2011, a number almost eight times more than the number of cases reported in 2010 [6]. However, these numbers are likely to underestimate the actual number of CAN cases because they are merely based on hospital-based registries. Unfortunately, a substantial number of CAN cases go unreported, indicating the greater-than-apparent severity of the problem [7].
Dentists play a significant role in identifying and reporting cases of CAN since they mainly deal with the head and neck areas, which are reportedly the most commonly affected in cases of abuse [8,9]. Additionally, a dentist can be the first person that a victim comes in contact with after an incident [9]. Furthermore, dentists usually see patients and their parents regularly, allowing them to recognize any changes in behavior or signs of CAN [10]. Many studies from different parts of the world have demonstrated inadequate awareness and a lack of training among dental practitioners toward the identification and management of cases of CAN [10,11,12,13]. Moreover, although they are ethically and lawfully obligated to detect and report the cases of CAN to social services or law enforcement agencies, most dentists lack sufficient knowledge regarding the reporting process, letting many of the cases go unreported [12,14,15,16,17].
In Saudi Arabia, Al-Dabaan et al. investigated the knowledge and experience of the Saudi Dental Society members regarding CAN and found that only 21% of the participants knew about the child protection policies in the regions of their practice [15]. Likewise, Mogaddam et al. investigated knowledge about child physical abuse among dental interns, postgraduate pediatric dentistry residents, and dentists practicing in dental colleges of the Jeddah city, Saudi Arabia, and they reported inadequate knowledge about the identifying and reporting of suspected cases of child abuse among the participants [11].
As responsible health care providers, dentists should be able to identify and report any cases of CAN they encounter. Dental education can aid in increasing awareness of the identifying and reporting process among the upcoming dental practitioners, which can further help in reducing CAN. The inadequacy of CAN-related knowledge among dental practitioners may be attributable to the deficiency related to this topic in the dental curricula [13]. To the best of our knowledge, studies assessing undergraduate dental education in Saudi Arabia with regard to CAN are limited, with no available national data about the knowledge of CAN among graduating dentists. Therefore, the aim of this study was to assess the knowledge of recently graduated dental students in Saudi Arabia regarding CAN and to evaluate the extent of training provided to the students for this subject. The results of our study are expected to aid in planning interventions to improve the knowledge of CAN and confidence in dealing with CAN cases among dental graduates.
2. Materials and Methods
2.1. Study Population and Data Collection
This nationwide cross-sectional study was conducted during the academic year of 2018/2019. In Saudi Arabia, new dental graduates are required to complete one year of internship training after they graduate before they can proceed with their future careers. The target population of this study was new dental graduates who were expected to finish their internship training program in the summer of 2019. Out of the 27 dental schools in Saudi Arabia, 23 had dental intern graduates, resulting in a total of 1552 dental interns. Data were collected between February and April 2019. The questionnaires were either mailed or handed in person to the intern’s representative of each dental school to distribute it to dental graduates. To increase the response rate, three reminders were sent to the intern’s representative in two-week intervals. After that, questionnaires were collected from each school’s representatives.
2.2. The Questionnaire
The self-administered questionnaire consisted of 23 questions that were developed based on previous studies [11,12,14,15,18]. The questionnaire was formulated in the form of multiple-choice questions in the English language and consists of three parts. The first part contains questions regarding background information, including the sex, age, and educational institution of the participants. The second part includes questions about the participants’ educational experience regarding CAN and their confidence in their ability to identify and report CAN cases. The third section was designed to test the participants’ knowledge of CAN.
2.3. The Validity and Reliability of the Questionnaire
The content validity for the questionnaire was assessed by two pediatric dentists and two dental public health practitioners who are experts in the field of CAN. They were asked to assess the comprehensiveness, phrasing, and importance of each question in the questionnaire. Minor adjustments to the questionnaire were made based on the experts’ comments to improve the comprehensiveness of the questions. The face validity was assessed by distributing the questionnaire to a group of dental interns (n = 10) to evaluate the clarity of the questionnaire. Moreover, test–retest reliability was assessed by asking ten dental interns to fill out the questionnaire two times with one week between each completion. The results were assessed using kappa statistics, which resulted in an average k of 0.81, indicating good reproducibility and reliability.
2.4. Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki, and ethical approval was obtained from the institutional review board (IRB No. E-18-3417, approval date: 18 November 2018) and the College of Dentistry Research Center (CDRC No. IR0304) of King Saud University.
2.5. Statistical Analysis
Frequencies and percentages were used to report the categorical variables corresponding to the background characteristics of the study sample in addition to their knowledge and educational background regarding CAN. Knowledge scores were calculated for participants based on their answers to 11 knowledge-related items of the questionnaire. A score of 60% was used as a cut-off point between adequate and inadequate knowledge levels which was set according to the regular passing score in dental schools in Saudi Arabia [19]. A multivariate logistic regression analysis was used to assess the associations between knowledge level and different independent variables. The level of significance was set at 0.05. Data were analyzed using SAS 9.4 software (SAS Institute, Inc., Cary, NC, USA).
3. Results
3.1. Sample Characteristics
A total of 1552 surveys were distributed in 23 dental educational institutes. A total of 988 dental graduates completed the questionnaire, resulting in a response rate of 63.7%. Around 55% of our samples were women, with a mean age of 24.9 years.
3.2. Educational Experience
Table 1 illustrates the participants’ educational experience regarding CAN. The majority of the participants (56%) graduated from government schools. Around 27% of the participants did not receive any dental education regarding CAN in their undergraduate training. The majority of the participants were not satisfied with the amount of education they received in their school on the subject (56.4%). Additionally, the vast majority (68.9%) felt that more time should be dedicated to educating students on CAN within the undergraduate curriculum.

Table 1.
Participants’ educational experience regarding CAN † (n = 988).
3.3. Knowledge Regarding CAN
The mean knowledge score of our samples was 53.27 ± 21.06, with the majority of the participants (59.6%) had inadequate knowledge. Figure 1 presents the percentages of participants who provided correct answers to knowledge-based items in the questionnaire. Almost all the participants (95.3%) believed that a guardian reporting a child’s injuries as self-mutilation-based injuries is an indicator of CAN. Additionally, the majority of the participants (71.5%) agreed that there is an association between CAN and procrastination in seeking medical care for children’s injuries. Around 71% agreed that pediatric dentists are not the only dental professionals who can report suspect cases of CAN. The majority of the participants agreed that there is a correlation between physical and dental neglect, as well as that repeated dental injury can be a sign of CAN (67.8% and 65%, respectively). Additionally, 49.1% knew that CAN is the most prevalent cause of pediatric mortality. Half of the participants thought that victims of CAN tend to inform someone about the experience they faced soon after its occurrence, and more than half were not aware that palatal petechiae can be an indicator of sexual abuse. Less than 30% of the participants disagreed with the statement that bruises over the elbows and knees can be a sign of CAN. Only 44.4% of the participants agreed that confronting the parents and accusing them directly is not the most suitable approach for handling cases of CAN.
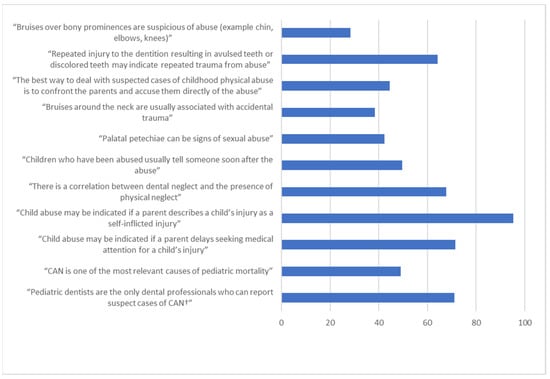
Figure 1.
Percentages of the participants with correct answers to knowledge-based items in the questionnaire (n = 988). † Child abuse and neglect.
3.4. Determinants of Knowledge Level
Table 2 illustrates the participants’ knowledge scores in association with key variables of the study sample. The knowledge score was significantly associated with sex, type of school, and receiving dental education about CAN at dental school (0.002, <0.0001, and <0.0001, respectively). Around 45% of the female participants had adequate knowledge levels compared to 35% of the male participants. Only 31.2% of the participants from private dental schools had an adequate knowledge score compared to 47.6% of those from government schools. Around 48% of those who received dental education about CAN had adequate knowledge scores compared to 20.1% of those who did not.
Table 2.
Participants’ knowledge scores in association with key variables of the study sample (n = 988).
Table 3 presents the results of the multivariate logistic regression analysis. All the factors remained statistically significant after entering the model. Female participants had 1.7 times the odds of having adequate knowledge compared to male participants (confidence interval (CI): 1.3–2.3). Graduating from government schools increased the odds of having adequate knowledge by two times compared to those from private schools (CI: 1.5–2.7). Those who received dental education about CAN had 3.1 times the odds of having adequate knowledge compared to those who did not (CI: 2.2–4.4).
Table 3.
Results of the multivariate logistic regression analysis (n = 988).
3.5. Identifying and Reporting CAN
Only 39.5% and 39.8% of the participants felt confident in their ability to identify (Figure 2) and report cases of CAN, respectively. However, less than 10% of the participants knew where to report cases of CAN.
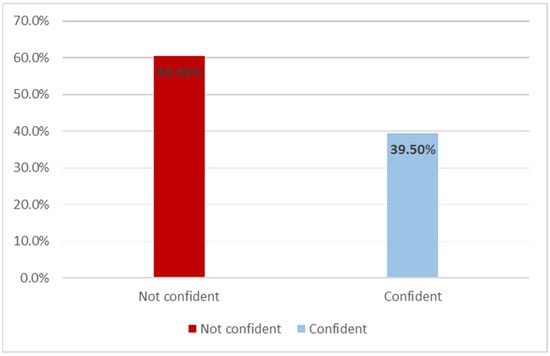
Figure 2.
Distribution of the respondents with regard to their confidence in their ability to identify cases of child abuse and neglect (n = 988).
4. Discussion
CAN is a major issue that affects a large number of children all over the world, and it may be an even larger problem than we realize due to underreporting. Dentists have an important role in suspecting and reporting CAN cases. This study was aimed to assess knowledge levels regarding CAN among new dental graduates in Saudi Arabia and to shed light on their educational experiences regarding this crucial topic during their undergraduate study years.
In our study, we found insufficient knowledge regarding CAN among dental graduates in Saudi Arabia. This is in agreement with the study conducted by Duman et al., in which they assessed knowledge regarding CAN among undergraduate students from 11 dental schools across the world [20]. Their study showed that dental students from Australia, Pakistan, Turkey, Jordan, Turkish Republic of Northern Cyprus, Poland, the Republic of South Africa, Nigeria, Cambodia, and the United States of America lack knowledge and experience in recognizing and reporting child abuse.
In Saudi Arabia, Mogaddam et al. found similar results when they investigated knowledge regarding physical abuse among dental interns, postgraduate residents, and pediatric dentists in dental colleges of Jeddah city [11]. In contrast, Al-Dabaan et al. found that most of their participants had sufficient knowledge about CAN [15]. This may have been due to the difference in the study populations, as they targeted members of the Saudi Dental Society, which includes pediatric dentists who are experts in this field. Furthermore, the low response rate (1.6%) might indicate that only individuals who were interested in the research topic participated in their study.
Our results indicate that graduates from government schools who received dental education about CAN and female participants had higher odds of having adequate knowledge scores than the other participants. Our findings are consistent with the results of the study conducted by Mogaddam et al., who found that the female sex and working in a government facility were significantly associated with higher knowledge scores [11]. Similarly, in a study aimed to assess the knowledge of and attitude toward CAN among dentists in Italy, Manea et al. found that women were more likely to correctly answer questions regarding CAN than men [21]. This may be attributed to the compassionate nature of women regarding children and their protection.
Dentists play a significant role in recognizing and reporting cases of CAN because the majority of the signs of abuse are usually seen in the areas they examine [8]. For this reason, dentists should feel confident in their ability to identify and report such cases. In our study, we found that less than 40% of the dental graduates were confident in their ability to identify CAN cases, and only 9.7% of them knew where to report such cases. These results are significantly lower than those of Mogaddam et al., who found that 63% of their participants knew where to report suspected cases of CAN [11]. This may have been related to their sample’s large proportion of postgraduate pediatric dentistry residents and pediatric dentists, who are expected to have more expertise in this field than our sample population.
Despite the important role of education in improving knowledge regarding CAN, only 73% of the participants in our study stated that they received education about CAN during their undergraduate studies. This can be considered low compared to studies conducted in other countries. In a study conducted by Jordan et al., almost 80% of the Croatian senior dental students were found to have received training regarding CAN during their undergraduate training [10]. In a study targeting dental students at the University of Michigan, the United States, Thomas et al. found that all the study participants had learned about the topic in their senior year [14]. In Saudi Arabia, the law of protection from CAN is considered new compared to those of other countries because it did not become official until August 2013 [22]. This may explain the deficiency related to this topic in undergraduate dental curricula in Saudi Arabia, which further highlights the need to update the dental curricula to ensure that dental graduates have adequate knowledge regarding this important topic.
The main limitation of our study is related to the self-reporting design of the study, which made it more prone to recall bias. Despite this limitation, to the best of our knowledge, this study is the first nationwide study to assess the knowledge and educational levels regarding CAN among dental graduates in Saudi Arabia. The large sample size with a relatively high response rate (63.7%) indicates a reduced risk of non-response bias, supporting the validity of the study. Our findings can be the foundation for establishing future interventions to improve graduates’ knowledge and confidence levels in identifying and reporting CAN cases. The intervention may include changing dental schools’ curricula by conducting awareness programs, seminars, and lectures; incorporating clinical workshop-based training; and initiating collaborations with different organizations to establish a multidisciplinary approach to handle suspected cases of CAN. Training should focus on increasing the student’s knowledge regarding the epidemiology, signs, and risk factors of CAN. Moreover, it should introduce Saudi Arabia’s child protection laws to dental students, highlight the importance of this crucial issue, and provide step by step standardized procedures for reporting suspected cases of CAN. Available evidence indicates training increases knowledge and changes attitudes [23], subsequently increasing the number of incidents reported [24]. Moreover, our results can be used as baseline data for evaluating the effectiveness of any possible future interventions that are aimed at improving graduates’ knowledge.
5. Conclusions
Our study demonstrates that there is insufficient knowledge regarding CAN among dental graduates in Saudi Arabia. Graduating from government schools, female sex, and receiving dental education about CAN were associated with higher knowledge levels on CAN; however, the majority of the participants did not feel confident in their ability to identify or report cases of CAN. Our findings indicate that dental curricula should be revised to ensure that dental graduates are confident in dealing with suspected cases they might encounter during their future careers.
Author Contributions
Conceptualization, A.M.S., A.A., A.A.A., M.A. and N.A.; methodology, A.M.S., O.A.B. and H.M.H.; software, A.M.S., H.M.H.; validation, A.A., A.A.A., M.A. and N.A.; formal analysis, H.M.H. and A.M.S.; investigation, A.A., A.A.A., M.A. and N.A.; data curation, A.A., A.A.A., M.A. and N.A.; writing—original draft preparation, A.A., A.A.A., M.A. and N.A.; writing—review and editing, A.M.S., H.M.H. and O.A.B.; visualization, A.M.S., H.M.H. and O.A.B.; supervision, A.M.S. and H.M.H.; project administration, A.M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and ethical approval was obtained from the institutional review board (IRB No. E-18-3417) and the College of Dentistry Research Center (CDRC No. IR0304) of King Saud University.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available.
Acknowledgments
The authors would like to acknowledge the Deanship of the Scientific Research and Research Center, College of Dentistry, King Saud University, Saudi Arabia, for supporting this study. The authors would like to extend their gratitude to the dental graduates for spending their valuable time in filling our questionnaire.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Report of the Consultation on Child Abuse Prevention; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Centers for Disease Prevention and Control. Preventing Child Abuse & Neglect. Available online: https://www.cdc.gov/violenceprevention/childabuseandneglect/fastfact.html (accessed on 1 May 2020).
- Institute of Medicine and National Research Council. New Directions in Child Abuse and Neglect Research; The National Academies Press: Washington, DC, USA, 2014. [Google Scholar] [CrossRef]
- World Health Organization. Child Maltreatment [Fact Sheet]. Available online: https://www.who.int/news-room/fact-sheets/detail/child-maltreatment (accessed on 1 March 2021).
- Violence Prevention. Preventing Child Abuse & Neglect [Fact Sheet]. Center for Disease Control and Prevention. 2021. Available online: https://www.cdc.gov/violenceprevention/pdf/can/CAN-factsheet_508.pdf (accessed on 3 March 2021).
- Child Maltreatment Prevention Readiness Assessment Country Report: Saudi Arabia. Available online: https://www.who.int/violence_injury_prevention/violence/child/saudi_arabia_rap_cm.pdf.pdf? (accessed on 11 May 2019).
- Cepal, N.U.; UNICEF. Child Abuse: A Painful Reality behind Closed Doors. 2009. Available online: https://repositorio.cepal.org/bitstream/handle/11362/36006/Challenges9-cepal-unicef_en.pdf?sequence=1&isAllowed=y (accessed on 1 May 2019).
- Cairns, A.M.; Mok, J.Y.Q.; Welbury, R. Injuries to the head, face, mouth and neck in physically abused children in a community setting. Int. J. Paediatr. Dent. 2005, 15, 310–318. [Google Scholar] [CrossRef]
- Nuzzolese, E.; Lepore, M.; Montagna, F.; Marcario, V.; De Rosa, S.; Solarino, B.; Di Vella, G. Child abuse and dental neglect: The dental team’s role in identification and prevention. Int. J. Dent. Hyg. 2009, 7, 96–101. [Google Scholar] [CrossRef]
- Jordan, A.; Welbury, R.; Tiljak, M.K.; Cukovic-Bagic, I. Croatian Dental Students’ Educational Experiences and Knowledge in Regard to Child Abuse and Neglect. J. Dent. Educ. 2012, 76, 1512–1519. [Google Scholar] [CrossRef] [PubMed]
- Mogaddam, M.; Kamal, I.; Merdad, L.; Alamoudi, N. Knowledge, attitudes, and behaviors of dentists regarding child physical abuse in Jeddah, Saudi Arabia. Child Abus. Negl. 2016, 54, 43–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashim, R.; Al-Ani, A. Child physical abuse: Assessment of dental students’ attitudes and knowledge in United Arab Emirates. Eur. Arch. Paediatr. Dent. 2013, 14, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Al-Jundi, S.H.; Zawaideh, F.I.; Al-Rawi, M.H. Jordanian Dental Students’ Knowledge and Attitudes in Regard to Child Physical Abuse. J. Dent. Educ. 2010, 74, 1159–1165. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.E.; Straffon, L.; Inglehart, M. Child Abuse and Neglect: Dental and Dental Hygiene Students’ Educational Experiences and Knowledge. J. Dent. Educ. 2006, 70, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Al-Dabaan, R.; Newton, J.; Asimakopoulou, K. Knowledge, attitudes, and experience of dentists living in Saudi Arabia toward child abuse and neglect. Saudi Dent. J. 2014, 26, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azevedo, M.S.; Goettems, M.L.; Brito, A.; Possebon, A.P.; Domingues, J.; Demarco, F.F.; Torriani, D.D. Child maltreatment: A survey of dentists in southern Brazil. Braz. Oral Res. 2012, 26, 5–11. [Google Scholar] [CrossRef] [Green Version]
- Owais, A.I.N.; Qudeimat, M.; Qodceih, S. Dentists’ involvement in identification and reporting of child physical abuse: Jordan as a case study. Int. J. Paediatr. Dent. 2009, 19, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Adair, S.M.; Yaresbi, S.; Wray, I.A.; Hanes, C.M.; Sama, D.R.; Russell, C.M. Demographic, educational, and experiential factors associated with dentist’s decision to report hypothetical cases of child maltreatment. Pediatr. Dent. 1997, 19, 466–469. [Google Scholar] [PubMed]
- Yousef, M.K.; Alshawwa, L.A.; Farsi, J.M.; Tekian, A.; Soo, P.Y. Determining defensible cut-off scores for dental courses. Eur. J. Dent. Educ. 2019, 24, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Duman, C.; Al-Batayneh, O.B.; Ahmad, S.; Durward, C.S.; Kobylińska, A.; Vieira, A.R.; Tredoux, S.; Okutan, A.E.; Egil, E.; Kalaoglu, E.E.; et al. Self-reported knowledge, attitudes, and practice of final-year dental students in relation to child abuse: A multi-centre study. Int. J. Paediatr. Dent. 2021. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Manea, S.; Favero, G.A.; Stellini, E.; Romoli, L.; Mazzucato, M.; Facchin, P. Dentists’ Perceptions, Attitudes, Knowledge, and Experience about Child Abuse and Neglect in Northeast Italy. J. Clin. Pediatr. Dent. 2007, 32, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Social Affairs. Law of Protection from Abuse; Bureau of Experts at the Council of Ministers: Riyadh, Saudi Arabia, 2013; Available online: https://www.nfsp.org.sa/ar/awareness/DocLib/english_law.pdf (accessed on 20 June 2019).
- Al-Dabaan, R.; Asimakopoulou, K.; Newton, J.T. Effectiveness of a web-based child protection training programme designed for dental practitioners in Saudi Arabia: A pre- and post-test study. Eur. J. Dent. Educ. 2015, 20, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Mathews, B.; Lee, X.; Norman, R.E. Impact of a new mandatory reporting law on reporting and identification of child sexual abuse: A seven year time trend analysis. Child Abus. Negl. 2016, 56, 62–79. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).