
Cardiothoracic CTA in Infants Referred for Aortic Arch Evaluation—Retrospective Comparison of Iomeprol 350, Ioversol 350, Iopromide 370 and Iodixanol 320


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and CTA Data
2.2. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Contrast Agent Data
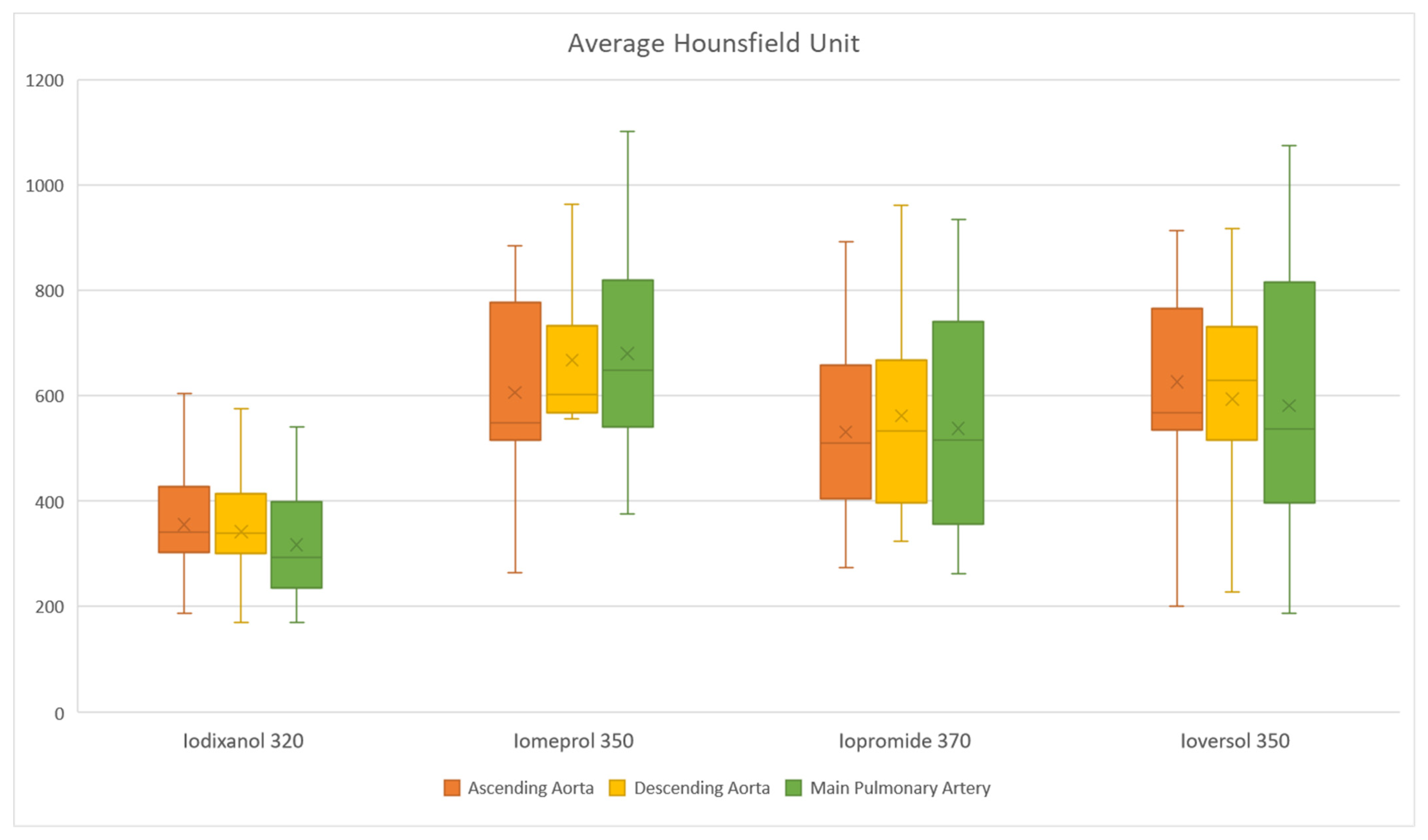
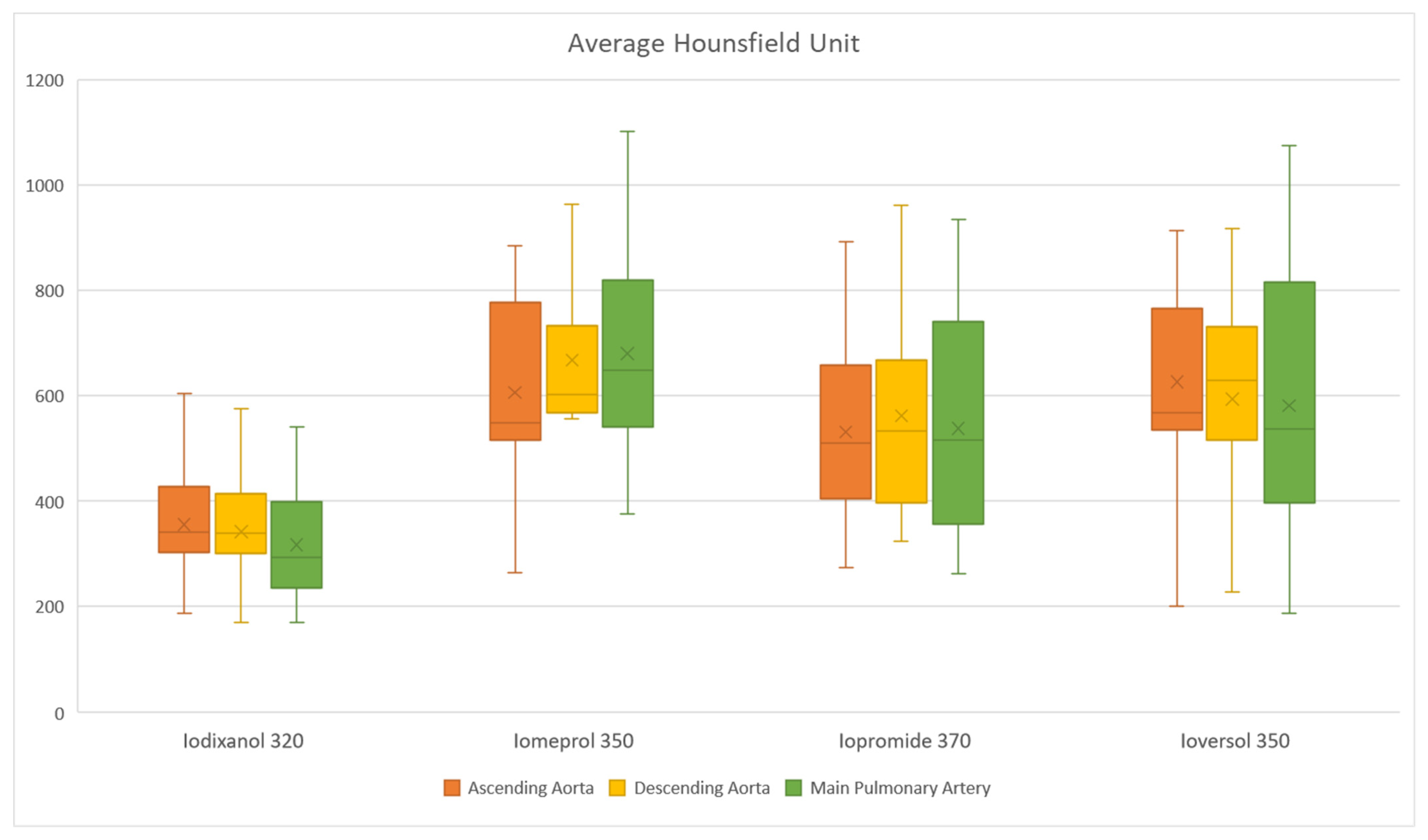
3.3. Thoracic Vessel Enhancement Comparison
4. Discussion
Limitations
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoffman, J.I.; Kaplan, S. The incidence of congenital heart disease. J. Am. Coll. Cardiol. 2002, 39, 1890–1900. [Google Scholar] [CrossRef] [Green Version]
- Young, C.; Taylor, A.M.; Owens, C.M. Paediatric cardiac computed tomography: A review of imaging techniques and radiation dose consideration. Eur. Radiol. 2010, 21, 518–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagy, E.; Tschauner, S.; Marterer, R.; Riedl, R.; Sorantin, E. Chest CTA in children younger than two years—A retrospective comparison of three contrast injection protocols. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Han, B.K.; Rigsby, C.K.; Hlavacek, A.; Leipsic, J.; Nicol, E.D.; Siegel, M.J.; Bardo, D.; Abbara, S.; Ghoshhajra, B.; Lesser, J.R.; et al. Computed Tomography Imaging in Patients with Congenital Heart Disease Part I: Rationale and Utility. An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT): Endorsed by the Society of Pediatric Radiology (SPR) and the North American Society of Cardiac Imaging (NASCI). J. Cardiovasc. Comput. Tomogr. 2015, 9, 475–492. [Google Scholar] [CrossRef] [PubMed]
- Han, B.K.; Rigsby, C.K.; Leipsic, J.; Bardo, D.; Abbara, S.; Ghoshhajra, B.; Lesser, J.R.; Raman, S.V.; Crean, A.M.; Nicol, E.D.; et al. Computed Tomography Imaging in Patients with Congenital Heart Disease, Part 2: Technical Recommendations. An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT): Endorsed by the Society of Pediatric Radiology (SPR) and the North American Society of Cardiac Imaging (NASCI). J. Cardiovasc. Comput. Tomogr. 2015, 9, 493–513. [Google Scholar] [CrossRef] [PubMed]
- Şuteu, C.C.; Muntean, I.; Blesneac, C.; Pop, M.; Togănel, R. Critical Neonatal Congenital Heart Disease—A Rare Complication after Successful Surgical Correction. J. Cardiovasc. Emergencies 2021, 6, 104–108. [Google Scholar] [CrossRef]
- Șuteu, C.C.; Blesneac, C.; Pop, M.; Făgărășan, A.; Gozar, L.; Togănel, R. A Particular Infantile Scimitar Syndrome Variant with Anomalous Systemic Arterial Supply-Inferior Vena Cava Fistula. J. Cardiovasc. Emergencies 2021, 7, 17–21. [Google Scholar] [CrossRef]
- Faria, D.; Augusto, J.B. In Search for Optimal Image Quality in Pediatric Cardiac CT Angiogram. Arq. Bras. Cardiol. 2021, 116, 106–107. [Google Scholar] [CrossRef] [PubMed]
- DiGeorge, N.W.; El-Ali, A.M.; White, A.M.; Harris, M.A.; Biko, D.M. Pediatric Cardiac CT and MRI: Considerations for the General Radiologist. Am. J. Roentgenol. 2020, 215, 1464–1473. [Google Scholar] [CrossRef]
- ACR Manual On Contrast Media 2020 ACR Committee on Drugs and Contrast Media. American College of Radiology. 2020. Available online: https://www.acr.org/-/media/ACR/Files/Clinical-Resources/Contrast_Media.pdf (accessed on 20 August 2021).
- Pop, M. ECR 2019 Book of abstracts. Comparison of Iodixanol 320, Iomeprol 350 and Iopromide 370 effectiveness in CT cardiothoracic angiography in infants. In Proceedings of the Insights into Imaging; Springer Science and Business Media LLC: Berlin/Heidelberg, Germany, 2019; Volume 10, p. 220. [Google Scholar]
- Pasternak, J.J.; Williamson, E.E. Clinical Pharmacology, Uses, and Adverse Reactions of Iodinated Contrast Agents: A Primer for the Non-radiologist. Mayo Clin. Proc. 2012, 87, 390. [Google Scholar] [CrossRef] [Green Version]
- Reiser, M.F.; Hricak, H.; Knauth, M.; Thomsen, H.S.; Webb, J.A.W. Contrast Media. Safety Issues and ESUR Guidelines; Thomsen, H.S., Webb, J.A.W., Eds.; Medical Radiology; Springer: Berlin/Heidelberg, Germany, 2014; ISBN 978-3-642-36723-6. [Google Scholar]
- Tsai, I.-C.; Lee, T.; Tsai, W.-L.; Chen, M.-C.; Wu, M.-J.; Lee, W.-L.; Ting, H.-J. Contrast Enhancement in Cardiac MDCT: Comparison of Iodixanol 320 Versus Iohexol 350. Am. J. Roentgenol. 2008, 190, W47–W53. [Google Scholar] [CrossRef] [PubMed]
- Ozbulbul, N.I.; Yurdakul, M.; Tola, M. Comparison of a low-osmolar contrast medium, iopamidol, and an iso-osmolar contrast medium, iodixanol, in MDCT coronary angiography. Coron. Artery Dis. 2010, 21, 414–419. [Google Scholar] [CrossRef]
- Svensson, A.; Ripsweden, J.; Rück, A.; Aspelin, P.; Cederlund, K.; Brismar, B.T. Heart rate variability and heat sensation during CT coronary angiography: Low-osmolar versus iso-osmolar contrast media. Acta Radiol. 2010, 51, 722–726. [Google Scholar] [CrossRef] [Green Version]
- Choi, T.Y.; Woo, V.; Gupta, M.; Sourayanezhad, S.; Li, D.; Mao, S.S.; Budoff, M. Comparison of iodixanol 320 and iohexol 350 in image quality during 64-slice multidetector computed tomography: Prospective randomized study. Int. J. Cardiol. 2012, 158, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Nakazato, R.; Arsanjani, R.; Shalev, A.; Leipsic, J.A.; Gransar, H.; Lin, F.Y.; Gomez, M.; Berman, D.S.; Min, J.K. Diagnostic Accuracy, Image Quality, and Patient Comfort for Coronary CT Angiography Performed Using Iso-Osmolar versus Low-Osmolar Iodinated Contrast: A Prospective International Multicenter Randomized Controlled Trial. Acad. Radiol. 2016, 23, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Lubbers, M.M.; Kock, M.; Niezen, A.; Galema, T.; Kofflard, M.; Bruning, T.; Kooij, H.S.; van Valen, H.; Dijkshoorn, M.; Booij, R.; et al. Iodixanol versus Iopromide at Coronary CT Angiography: Lumen Opacification and Effect on Heart Rhythm—The Randomized IsoCOR. Radiology 2017, 286, 71–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saade, C.; Karout, L.; El Asmar, K.; Naffaa, L.; El Merhi, F.; Salman, R.; Abi-Ghanem, A.S. Impact of various iodine concentrations of iohexol and iodixanol contrast media on image reconstruction techniques in a vascular-specific contrast media phantom: Quantitative and qualitative image quality assessment. Radiol. Med. 2021, 126, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Honoris, L.; Zhong, Y.; Chu, E.; Rosenthal, D.; Li, D.; Lam, F.; Budoff, M.J. Comparison of contrast enhancement, image quality and tolerability in Coronary CT angiography using 4 contrast agents: A prospective randomized trial. Int. J. Cardiol. 2015, 186, 126–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cademartiri, F.; Nieman, K.; van der Lugt, A.; Raaijmakers, R.H.; Mollet, N.R.; Pattynama, P.M.T.; de Feyter, P.J.; Krestin, G.P.; Maffei, E.; Palumbo, A.; et al. Intravenous contrast material administration at 16-detector row helical CT coronary angiography: Test bolus versus bolus-tracking technique. Radiology 2004, 233, 817–823. [Google Scholar] [CrossRef]
- Mcdermott, M.; Kemper, C.; Barone, W.; Jost, G.; Endrikat, J. Impact of CT Injector Technology and Contrast Media Viscosity on Vascular Enhancement: Evaluation in a Circulation Phantom. Br. J. Radiol. 2020, 93, 20190868. [Google Scholar] [CrossRef] [PubMed]
- Becker, C.R.; Vanzulli, A.; Fink, C.; De Faveri, D.; Fedeli, S.; Dore, R.; Biondetti, P.; Kuettner, A.; Krix, M.; Ascenti, G. Multicenter comparison of high concentration contrast agent iomeprol-400 with iso-osmolar iodixanol-320: Contrast enhancement and heart rate variation in coronary dual-source computed tomographic angiography. Investig. Radiol. 2011, 46, 457–464. [Google Scholar] [CrossRef]
- IBM Corp IBM SPSS Statistics for Windows 2017. Available online: https://www.ibm.com/products/spss-statistics (accessed on 20 August 2021).
- Hwang, J.Y.; Choo, K.S.; Choi, Y.Y.; Kim, J.H.; Ryu, H.; Han, J.; Kim, Y.W.; Jeon, U.B.; Nam, K.J. Subjective and objective image differences in pediatric computed tomography cardiac angiography using lower iodine concentration. Pediatr. Radiol. 2017, 47, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Pascanu, I.; Pop, R.; Barbu, C.G.; Dumitrescu, C.P.; Gherlan, I.; Marginean, O.; Preda, C.; Procopiuc, C.; Vulpoi, C.; Hermanussen, M. Development of synthetic growth charts for Romanian population. Acta Endocrinol. 2016, 12, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Pop, R.M.; Pop, M.; Dogaru, G.; Bacarea, V.C. A web-based nutritional assessment tool. Stud. Inform. Control 2013, 22, 307–314. [Google Scholar] [CrossRef]
- Bae, K.T. Intravenous contrast medium administration and scan timing at CT: Considerations and approaches. Radiology 2010, 256, 32–61. [Google Scholar] [CrossRef] [PubMed]
- Schueller-Weidekamm, C.; Schaefer-Prokop, C.M.; Weber, M.; Herold, C.J.; Prokop, M. CT Angiography of Pulmonary Arteries to Detect Pulmonary Embolism: Improvement of Vascular Enhancement with Low Kilovoltage Settings1. Radiology 2006, 241, 899–907. [Google Scholar] [CrossRef]
- Faggioni, L.; Neri, E.; Sbragia, P.; Pascale, R.; D’Errico, L.; Caramella, D.; Bartolozzi, C.; D’Errico, L.; Caramella, D.; Bartolozzi, C. 80-kV Pulmonary CT Angiography With 40 mL of Iodinated Contrast Material in Lean Patients: Comparison of Vascular Enhancement With Iodixanol (320 mg I/mL)and Iomeprol (400 mg I/mL). Am. J. Roentgenol. 2012, 199, 1220–1225. [Google Scholar] [CrossRef] [PubMed]
- Visipaque FDA NDA 20-351/S-013 Volume 1. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2003/20351slr013_visipaque_lbl.pdf (accessed on 23 August 2021).
- Smedby, Ö. Smedby Viscosity of some contemporary contrast media before and after mixing with whole blood. Acta Radiol. 1992, 33, 600–605. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Total | Iomeprol 350 | Ioversol 350 | Iopromide 370 | Iodixanol 320 | p-Value | |
|---|---|---|---|---|---|---|
| N(%) | 48 (100%) | 11 (22.91%) | 13 (27.08%) | 12 (25%) | 12 (25%) | |
| Male:Female ratio | 0.92 | 0.57 | 2.25 | 0.71 | 0.71 | |
| Age (days), Median (IQR) | 10.5 (6–74) | 7 (4–28) | 11 (5–23) | 10 (7.75–21.75) | 111 (20.5–198.5) | 0.056 |
| Weight (kg), Median (IQR) | 3.37 (2.9–4) | 3.3 (2.95–3.72) | 3.4 (2.7–4) | 3.27 (2.92–3.41) | 3.9 (3.17–7.11) | 0.58 |
| Length (cm), Median (IQR) | 53 (51–57) | 53 (51–54.5) | 52 (51–55) | 53 (50.75–56.5) | 56.5 (52.75–67.25) | 0.33 |
| Scanned at 70 kV | 4 (8.33%) | 4 (100%) | ||||
| Scanned at 80 kV | 43 (89.58%) | 11 (25.58%) | 13 (30.23%) | 11 (25.58%) | 8 (18.6%) | |
| Scanned at 100 kV | 1 (2.08%) | 1 (100%) |
| Variables | Iomeprol 350 | Ioversol 350 | Iopromide 370 | Iodixanol 320 | p-Value |
|---|---|---|---|---|---|
| Volume, Median (IQR) | 8 (7–8.75) | 7 (6.75–9.25) | 7 (6.5–8) | 7 (5.5–10) | 0.68 |
| Flow, Mean (SD) | 0.92 (0.17) | 0.94 (0.15) | 0.81 (0.15) | 1.08 (0.34) | 0.03 *,† |
| Iodine mg/kg body weight, Mean (SD) | 816.66 (98.08) | 820.56 (85.22) | 795.75 (157.55) | 564.81 (92.13) | <0.001 *,† |
| Iodine mg/kg body weight/s, Median (IQR) | 93.33 (79.72–97.22) | 96.25 (89.66–106.94) | 87.13 (74.42–98.28) | 77.19 (54.82–109.53) | 0.33 |
| Location | Iomeprol 350 | Ioversol 350 | Iopromide 370 | Iodixanol 320 | p-Value |
|---|---|---|---|---|---|
| Main pulmonary artery, Mean (SD) | 679.54 (191.29) | 580.69 (256.73) | 538 (225.93) | 316.66 (105.63) | 0.001 * |
| Ascending aorta, Mean (SD) | 605.9 (177.23) | 626 (183.83) | 530.83 (175.65) | 354.91 (115.81) | 0.001 * |
| Descending aorta, Mean (SD) | 677 (145.68) | 613.69 (190.33) | 564.08 (219) | 345.5 (93.96) | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pop, M. Cardiothoracic CTA in Infants Referred for Aortic Arch Evaluation—Retrospective Comparison of Iomeprol 350, Ioversol 350, Iopromide 370 and Iodixanol 320. Children 2021, 8, 949. https://doi.org/10.3390/children8110949
Pop M. Cardiothoracic CTA in Infants Referred for Aortic Arch Evaluation—Retrospective Comparison of Iomeprol 350, Ioversol 350, Iopromide 370 and Iodixanol 320. Children. 2021; 8(11):949. https://doi.org/10.3390/children8110949
Chicago/Turabian StylePop, Marian. 2021. "Cardiothoracic CTA in Infants Referred for Aortic Arch Evaluation—Retrospective Comparison of Iomeprol 350, Ioversol 350, Iopromide 370 and Iodixanol 320" Children 8, no. 11: 949. https://doi.org/10.3390/children8110949
APA StylePop, M. (2021). Cardiothoracic CTA in Infants Referred for Aortic Arch Evaluation—Retrospective Comparison of Iomeprol 350, Ioversol 350, Iopromide 370 and Iodixanol 320. Children, 8(11), 949. https://doi.org/10.3390/children8110949