
Physical and Neurological Development of a Girl Born to a Mother with Methylmalonic Acidemia and Kidney Transplantation and Review of the Literature

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Case Report
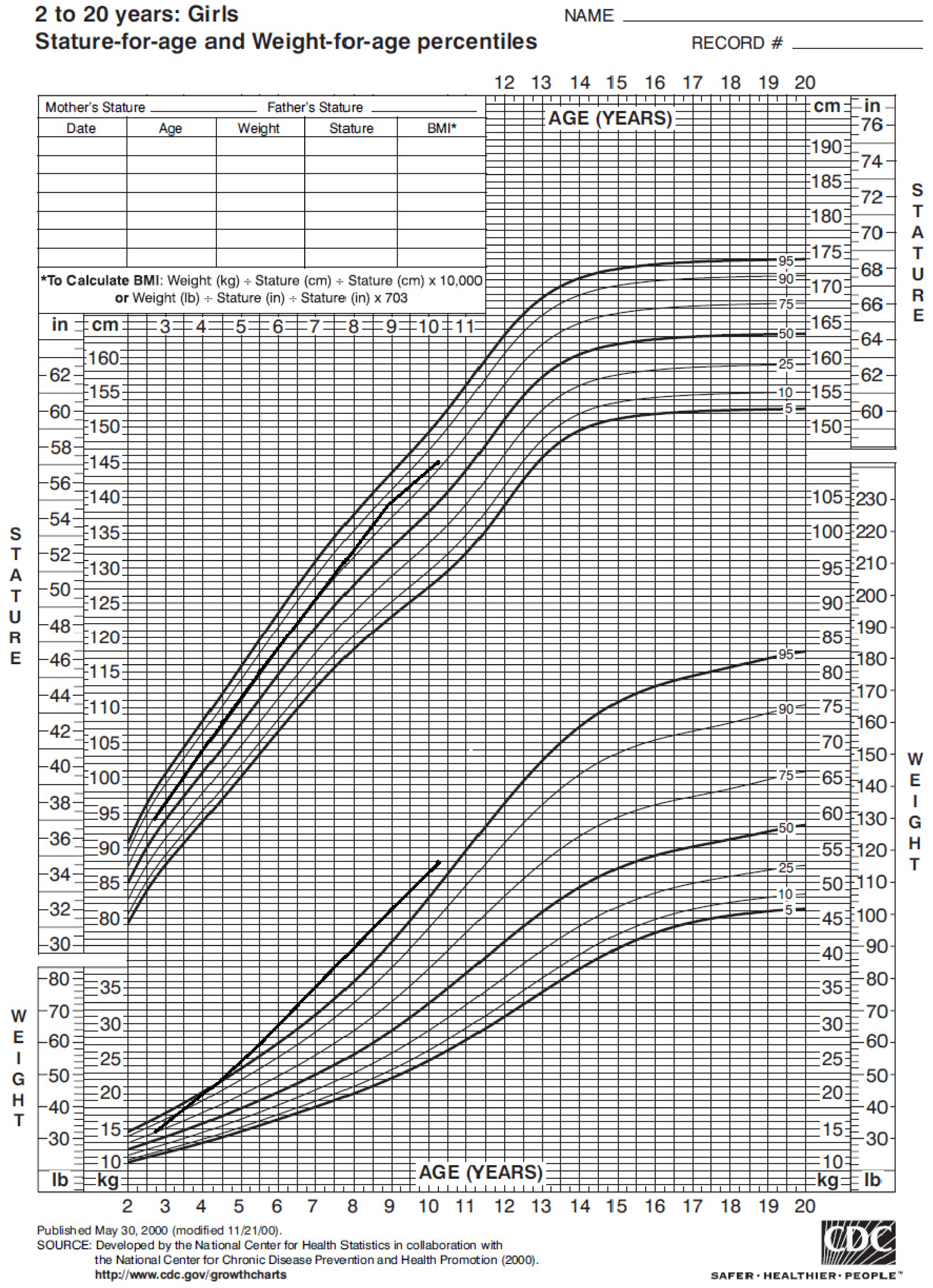
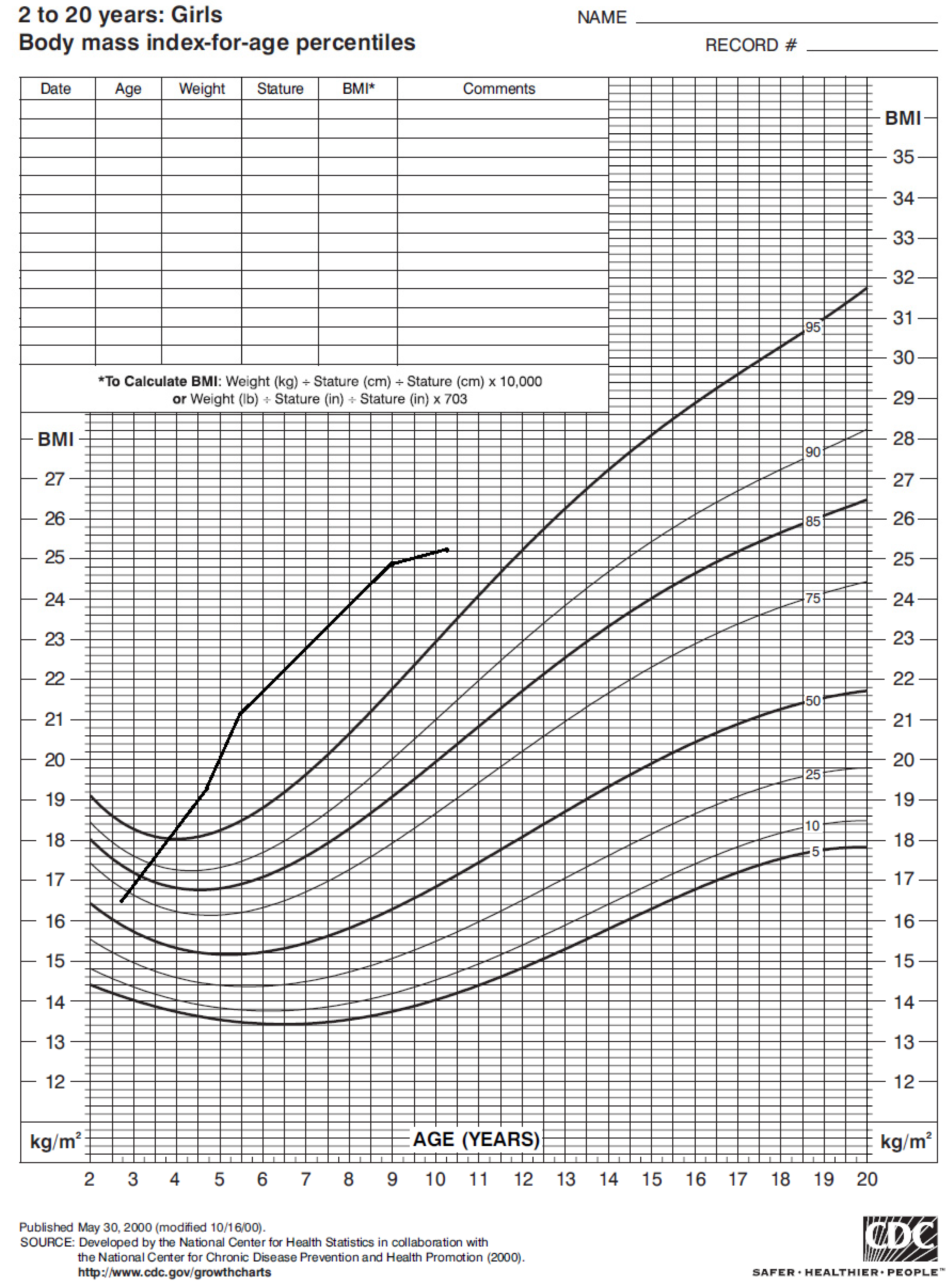
2.1. Pregnancy and Growth
2.2. Neurological Development
2.2.1. Cognitive Profile
2.2.2. Behavioural Profile
2.2.3. Profile of the Development and Adaptive Function
3. Review
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hörster, F.; Baumgartner, M.R.; Viardot, C.; Suormala, T.; Burgard, P.; Fowler, B.; Hoffmann, G.F.; Garbade, S.F.; Kölker, S.; Baumgartner, E.R. Long-Term Outcome in Methylmalonic Acidurias Is Influenced by the Underlying Defect (mut0, mut−, cblA, cblB). Pediatr. Res. 2007, 62, 225–230. [Google Scholar] [CrossRef]
- Melo, D.R.; Kowaltowski, A.J.; Wajner, M.; Castilho, R.F. Mitochondrial energy metabolism in neurodegeneration associated with methylmalonic acidemia. J. Bioenerg. Biomembr. 2011, 43, 39–46. [Google Scholar] [CrossRef]
- Lash, L.H. Mitochondrial glutathione transport: Physiological, pathological and toxicological implications. Chem. Interact. 2006, 163, 54–67. [Google Scholar] [CrossRef] [Green Version]
- Morath, M.A.; Okun, J.G.; Müller, I.B.; Sauer, S.W.; Hörster, F.; Hoffmann, G.F.; Kölker, S. Neurodegeneration and chronic renal failure in methylmalonic aciduria—A pathophysiological approach. J. Inherit. Metab. Dis. 2007, 31, 35–43. [Google Scholar] [CrossRef]
- Baumgartner, M.R.; Hörster, F.; Dionisi-Vici, C.; Haliloglu, G.; Karall, D.; Chapman, A.K.; Huemer, M.; Hochuli, M.; Assoun, M.; Ballhausen, D.; et al. Proposed guidelines for the diagnosis and management of methylmalonic and propionic acidemia. Orphanet J. Rare Dis. 2014, 9, 1–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langendonk, J.G.; Roos, J.C.; Angus, L.; Williams, M.; Karstens, F.P.; De Klerk, J.B.; Maritz, C.; Ben-Omran, T.; Williamson, C.; Lachmann, R.H.; et al. A series of pregnancies in women with inherited metabolic disease. J. Inherit. Metab. Dis. 2011, 35, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Koch, R.; Acosta, P.B.; Williams, J.C. Nutritional Therapy for Pregnant Women with a Metabolic Disorder. Clin. Perinatol. 1995, 22, 1–14. [Google Scholar] [CrossRef]
- Raval, D.B.; Merideth, M.; Sloan, J.L.; Braverman, N.E.; Conway, R.L.; Manoli, I.; Venditti, C.P. Methylmalonic acidemia (MMA) in pregnancy: A case series and literature review. J. Inherit. Metab. Dis. 2015, 38, 839–846. [Google Scholar] [CrossRef] [Green Version]
- Lubrano, R.; Perez, B.; Elli, M. Methylmalonic acidemia and kidney transplantation. Pediatr. Nephrol. 2013, 28, 2067–2068. [Google Scholar] [CrossRef]
- Lubrano, R.; Elli, M.; Rossi, M.; Travasso, E.; Raggi, C.; Barsotti, P.; Carducci, C.; Berloco, P. Renal transplant in methylmalonic acidemia: Could it be the best option? Pediatr. Nephrol. 2007, 22, 1209–1214. [Google Scholar] [CrossRef] [PubMed]
- Lubrano, R.; Scoppi, P.; Barsotti, P.; Travasso, E.; Scateni, S.; Cristaldi, S.; Castello, M.A. Kidney transplantation in a girl with methylmalonic acidemia and end stage renal failure. Pediatr. Nephrol. 2001, 16, 848–851. [Google Scholar] [CrossRef] [PubMed]
- Lubrano, R.; Bellelli, E.; Gentile, I.; Paoli, S.; Carducci, C.; Santagata, S.; Pérez, B.; Ugarte, M.; Labriola, D.; Elli, M. Pregnancy in a Methylmalonic Acidemia Patient with Kidney Transplantation: A Case Report. Am. J. Transplant. 2013, 13, 1918–1922. [Google Scholar] [CrossRef] [PubMed]
- Diss, E.; Iams, J.; Reed, N.; Roe, D.S.; Roe, C. Methylmalonic aciduria in pregnancy: A case report. Am. J. Obstet. Gynecol. 1995, 172, 1057–1059. [Google Scholar] [CrossRef]
- Wasserstein, M.P.; Gaddipati, S.; Snyderman, S.E.; Eddleman, K.; Desnick, R.J.; Sansaricq, C. Successful pregnancy in severe methylmalonic acidaemia. J. Inherit. Metab. Dis. 1999, 22, 788–794. [Google Scholar] [CrossRef]
- Deodato, F.; Rizzo, C.; Boenzi, S.; Baiocco, F.; Sabetta, G.; Dionisi-Vici, C. Successful pregnancy in a woman with mut− methylmalonic acidaemia. J. Inherit. Metab. Dis. 2002, 25, 133–134. [Google Scholar] [CrossRef] [PubMed]
- Boneh, A.; Greaves, R.F.; Garra, G.; Pitt, J.J. Metabolic treatment of pregnancy and postdelivery period in a patient with cobalamin A disease. Am. J. Obstet. Gynecol. 2002, 187, 225–226. [Google Scholar] [CrossRef] [PubMed]
- Adeyemi, O.; Girish, T.; Mukhopadhyay, S.; Olczak, S.; Ahmed, Z. Methylmalonic acidaemia: A rare metabolic disorder in pregnancy. J. Obstet. Gynaecol. 2004, 24, 927–928. [Google Scholar] [CrossRef]
- Jacquemyn, Y.; Hartog, M.D.; Eyskens, F. Methylmalonic acidaemia in pregnancy. BMJ Case Rep. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- Wilcox, G. Impact of pregnancy on inborn errors of metabolism. Rev. Endocr. Metab. Disord. 2018, 19, 13–33. [Google Scholar] [CrossRef] [Green Version]
- Spronsen, F.; Smit, G.; Erwich, J. Inherited metabolic diseases and pregnancy. BJOG Int. J. Obstet. Gynaecol. 2005, 112, 2–11. [Google Scholar] [CrossRef]
- Murphy, E. Pregnancy in women with inherited metabolic disease. Obstet. Med. 2015, 8, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Schuck, P. Inhibition of mitochondrial creatine kinase activity from rat cerebral cortex by methylmalonic acid. Neurochem. Int. 2004, 45, 661–667. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, B.; Nelson, D.; Silver, I.; Erecinska, M.; Chesselet, M.-F. Methylmalonate toxicity in primary neuronal cultures. Neurosci. 1998, 86, 279–290. [Google Scholar] [CrossRef]
- Okun, J.G.; Hörster, F.; Farkas, L.M.; Feyh, P.; Hinz, A.; Sauer, S.; Hoffmann, G.F.; Unsicker, K.; Mayatepek, E.; Kölker, S. Neurodegeneration in Methylmalonic Aciduria Involves Inhibition of Complex II and the Tricarboxylic Acid Cycle, and Synergistically Acting Excitotoxicity. J. Biol. Chem. 2002, 277, 14674–14680. [Google Scholar] [CrossRef] [Green Version]
- Maciel, E.N.; Kowaltowski, A.J.; Schwalm, F.D.; Rodrigues, J.M.; Souza, D.O.; Vercesi, A.E.; Wajner, M.; Castilho, R.F. Mitochondrial permeability transition in neuronal damage promoted by Ca2+ and respiratory chain complex II inhibition. J. Neurochem. 2004, 90, 1025–1035. [Google Scholar] [CrossRef] [PubMed]
- Kowaltowski, A.J.; Maciel, E.N.; Fornazari, M.; Castilho, R.F. Diazoxide protects against methylmalonate-induced neuronal toxicity. Exp. Neurol. 2006, 201, 165–171. [Google Scholar] [CrossRef]
- Kölker, S.; Ahlmeyer, B.; Krieglstein, J.; Hoffmann, G.F. Methylmalonic acid induces excitotoxic neuronal damage in vitro. J. Inherit. Metab. Dis. 2000, 23, 355–358. [Google Scholar] [CrossRef]
- Remacle, N.; Forny, P.; Cudré-Cung, H.-P.; Gonzalez-Melo, M.; Vale-Pereira, S.D.; Henry, H.; Teav, T.; Gallart-Ayala, H.; Braissant, O.; Baumgartner, M.; et al. New in vitro model derived from brain-specific Mut-/- mice confirms cerebral ammonium accumulation in methylmalonic aciduria. Mol. Genet. Metab. 2018, 124, 266–277. [Google Scholar] [CrossRef]
- Wenchich, L.; Zeman, J.; Hansíková, H.; Plavka, R.; Sperl, W.; Houstek, J. Mitochondrial energy metabolism in very premature neonates. Biol. Neonate 2002, 81, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Honzik, T.; Wenchich, L.; Böhm, M.; Hansikova, H.; Pejznochova, M.; Zapadlo, M.; Plavka, R.; Zeman, J. Activities of respiratory chain complexes and pyruvate dehydrogenase in isolated muscle mitochondria in premature neonates. Early Hum. Dev. 2008, 84, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Ravera, S.; Podestà, M.; Sabatini, F.; Fresia, C.; Columbaro, M.; Bruno, S.; Fulcheri, E.; Ramenghi, L.A.; Frassoni, F. Mesenchymal stem cells from preterm to term newborns undergo a significant switch from anaerobic glycolysis to the oxidative phosphorylation. Cell. Mol. Life Sci. 2018, 75, 889–903. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.D.; Yoon, N.A.; Jin, S.; Diano, S. Microglial UCP2 Mediates Inflammation and Obesity Induced by High-Fat Feeding. Cell Metab. 2019, 30, 952–962.e5. [Google Scholar] [CrossRef]
- Chiurazzi, M.; Di Maro, M.; Cozzolino, M.; Colantuoni, A. Mitochondrial Dynamics and Microglia as New Targets in Metabolism Regulation. Int. J. Mol. Sci. 2020, 21, 3450. [Google Scholar] [CrossRef] [PubMed]
- De Graaf-Peters, V.B.; Hadders-Algra, M. Ontogeny of the human central nervous system: What is happening when? Early Hum. Dev. 2006, 82, 257–266. [Google Scholar] [CrossRef]
- Ment, L.R.; Hirtz, D.; Hüppi, P. Imaging biomarkers of outcome in the developing preterm brain. Lancet Neurol. 2009, 8, 1042–1055. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Published Case | Type of MMA | Pregnancy Metabolic Complications | Adjunctive Therapy | Protein Intake | Obstetrical/ Delivery Complications |
|---|---|---|---|---|---|
| Diss 1995 | mut0 | Hyperemesis | Carnitine | 3.6 → 4.1 → 1.6 g/kg/die | None |
| Wasserstein 1999 | mut− | None | Oral bicarbonate Amoxicillin/Metronidazole | 40–55 g/die | pPROM Pre-eclampsia |
| Deodato 2002 | mut− | None | Carnitine Vitamin B12 IM | 1.5 g/Kg/die | None |
| Boneh 2002 | CblA | None | Vitamin B12 IM | Reported as “normal” | Fetal distress |
| Adeyemi 2004 | mut− | IV fluids once | Vitamin B12 OS Carnitine | Reported as “low” | pPROM Prepartum Chlamydia Infection Chorioamnionitis |
| Langendonk 2011 | N/A | Hyper ammoniaemia twice | Carnitine Vitamin B12 IM Vitamin B9 | 45–60 g/die | None |
| Langendonk 2011 | mut− | Poor treatment compliance | Carnitine Vitamin B12 IM | 35 g/die | IUGR Difficulty feeding |
| Lubrano 2013 | CblA | None | None | Reported as “low” | None |
| Jacquemyn 2014 | CblA | None | Carnitine Vitamin B12 OS | 1 g/Kg/die | None |
| Raval 2015 | mut− | IV Fluids twice | Carnitine | 64 g/die | Fetal distress Post-partum infection |
| Raval 2015 | CblA | None | N/A | 45 g/die | Pre-eclampsia Fetal distress |
| Raval 2015 | CblA | None | Carnitine, Vitamin B12 IM | 45 --> 80 g/die | Pre-eclampsia Gestational diabetes pPROM Fetal distress |
| Raval 2015 | mut− | None | Carnitine | 47 g/die | None |
| Wilcox 2018 | N/A | None | N/A | N/A | None |
| Published Case | Gestational Age | Birth Weight | Neurological Outcome of the Child | Methods of Evaluation | Methylmalonic Acid MB µmol/L MU mmol/mol Cr AF µmol/L | Newborn’s Levels of Methylmalonic Acid CB µmol/L NB µmol/L NU mmol/mol Cr |
|---|---|---|---|---|---|---|
| Diss 1995 | Term | 3500 g (AGA) | Normal at 3 years | Denver Developmental Screening Tests | 1st trim. 16.4 (MB) 2nd trim. 8.2 (MB) 3rd trim. 9 (MB) 1st trim. 2.59 (MU) mmol/24 h 2nd trim. 1.29 (MU) mmol/24 h 3rd trim. 0.78 (MU) mmol/24 h N/A (AF) | N/A |
| Wasserstein 1999 | 36 weeks + 4 days | 3220 g (AGA) | Normal at 1 year | N/A | 484 (MB) 4.98 (MU) 608.7 (AF) | 58 (CB) Undectable at 5 days (NB) |
| Deodato 2002 | 38 weeks | 2940 g (AGA) | Normal at 2 years | N/A | N/A (MB) 1st trim. 17049 (MU) 2nd trim. 4177 (MU) 3rd trim. 3236 (MU) 305 (AF) | 200 (CB) 1129 (NU) at birth 82 (NU) at 48 h |
| Boneh 2002 | 36 weeks | N/A | N/A | N/A | N/A (MB) 210-385-600 (MU) N/A (AF) | N/A |
| Adeyemi 2004 | 34 weeks | 1900 g (AGA) | Normal at 5 months | N/A | N/A (MB) Reported as “raised” (MU) N/A (AF) | Undectable (NU) |
| Langendonk 2011 | 38 weeks | 2850 g (AGA) | Normal at 5 years | N/A | N/A | N/A |
| Langendonk 2011 | 35 weeks | 1530 g (SGA) | Normal at 1 year | N/A | N/A | N/A |
| Lubrano 2013 | 37 weeks | 2480 g (AGA) | Normal at 3 months | WISC | N/A (MB) 1st trim. N/A (MU) 2nd trim. 72 (MU) 3rd trim. 52 (MU) 127.3 (AF) | 7 (NU) at 48 h 0.2 (NB) at 28 days |
| Jacquemyn 2014 | 40 weeks | 3300 g (AGA) | Reported as “normal” | N/A | N/A | N/A |
| Raval 2015 | 38 weeks | 3288 g (AGA) | Normal at 10 years | N/A | N/A | N/A |
| Raval 2015 | 42 weeks | 3714 g (AGA) | Normal at 14 years | N/A | N/A | N/A |
| Raval 2015 | 32 weeks | 1459 g (AGA) | Normal at 3 years | N/A | 1st trim. 39 (MB) 2nd trim. 45 (MB) 3rd trim. 15 (MB) N/A (MU) N/A (AF) | N/A |
| Raval 2015 | 39 weeks | 3095 g (AGA) | Normal at 3 months | N/A | N/A (MB) 765 (MU) N/A (AF) | N/A |
| Wilcox 2018 | N/A | N/A | N/A | N/A | N/A | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcellino, A.; Guido, C.A.; Bloise, S.; Mallardo, S.; Isoldi, S.; Del Giudice, E.; Dilillo, A.; Martucci, V.; Sanseviero, M.; Iorfida, D.; et al. Physical and Neurological Development of a Girl Born to a Mother with Methylmalonic Acidemia and Kidney Transplantation and Review of the Literature. Children 2021, 8, 1013. https://doi.org/10.3390/children8111013
Marcellino A, Guido CA, Bloise S, Mallardo S, Isoldi S, Del Giudice E, Dilillo A, Martucci V, Sanseviero M, Iorfida D, et al. Physical and Neurological Development of a Girl Born to a Mother with Methylmalonic Acidemia and Kidney Transplantation and Review of the Literature. Children. 2021; 8(11):1013. https://doi.org/10.3390/children8111013
Chicago/Turabian StyleMarcellino, Alessia, Cristiana Alessia Guido, Silvia Bloise, Saverio Mallardo, Sara Isoldi, Emanuela Del Giudice, Anna Dilillo, Vanessa Martucci, Mariateresa Sanseviero, Donatella Iorfida, and et al. 2021. "Physical and Neurological Development of a Girl Born to a Mother with Methylmalonic Acidemia and Kidney Transplantation and Review of the Literature" Children 8, no. 11: 1013. https://doi.org/10.3390/children8111013
APA StyleMarcellino, A., Guido, C. A., Bloise, S., Mallardo, S., Isoldi, S., Del Giudice, E., Dilillo, A., Martucci, V., Sanseviero, M., Iorfida, D., Spalice, A., & Lubrano, R. (2021). Physical and Neurological Development of a Girl Born to a Mother with Methylmalonic Acidemia and Kidney Transplantation and Review of the Literature. Children, 8(11), 1013. https://doi.org/10.3390/children8111013