
Pain Neuroscience Education: State of the Art and Application in Pediatrics



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Why Pain Neuroscience Education?
2.1. Contextual Information about Pain Influences Pain Perception
2.2. Pain Neuroscience Education Provides a Common Language between Provider and Patient
3. Overview of Pain Neuroscience Education
3.1. Explanatory Models
Application of Explanatory Models to Pediatrics
3.2. Current Evidence for PNE among Adults
Current Evidence for Pain Neuroscience Education in Pediatrics
3.3. New Applications of PNE: Preoperative Preparation and Cancer Pain Treatment
3.4. A Combined Approach of Pain Neuroscience Education and Physiotherapy
4. Delivery Methods
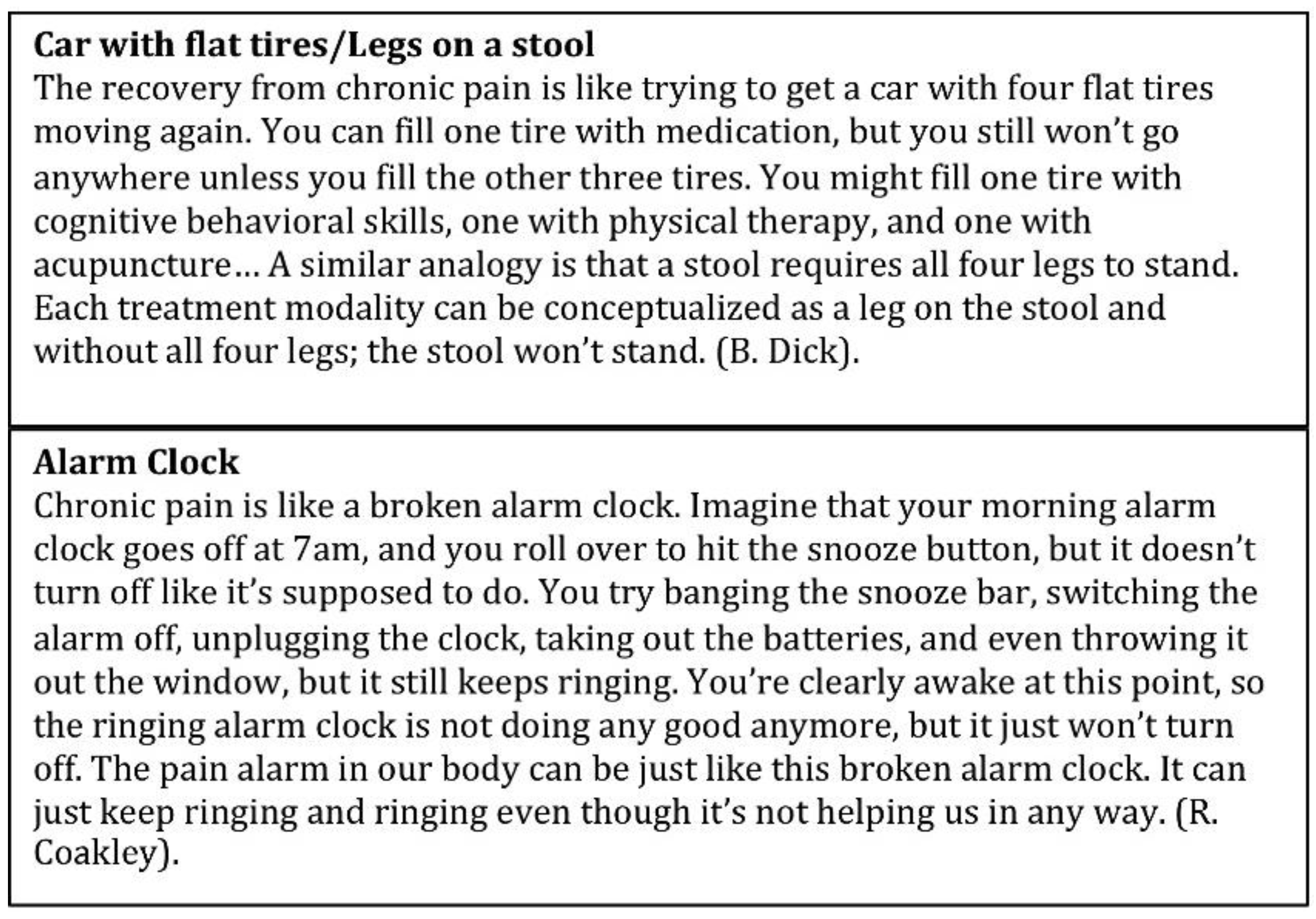
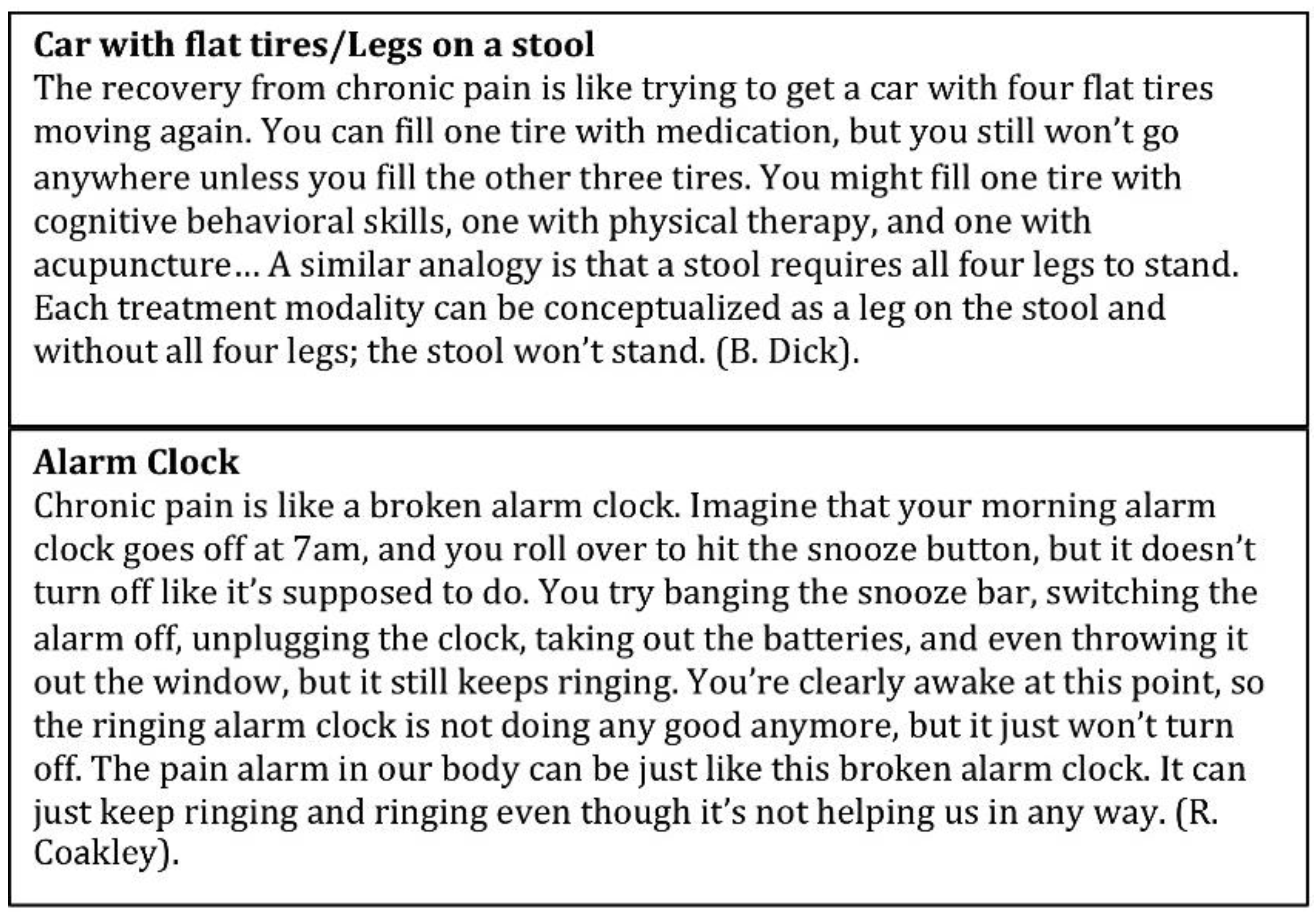
4.1. Metaphor
4.2. Books
4.2.1. Adult Pain Books
4.2.2. Pediatric Pain Books
4.3. Group Education Models
4.4. Video
5. Developmental Considerations and Next Steps
6. Conclusions
Acknowledgments
Conflicts of Interest
References
- Groenewald, C.B.; Essner, B.S.; Wright, D.; Fesinmeyer, M.D.; Palermo, T.M. The Economic Costs of Chronic Pain Among a Cohort of Treatment-Seeking Adolescents in the United States. J. Pain 2014, 15, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L.; Butler, D.S. Fifteen Years of Explaining Pain: The Past, Present, and Future. J. Pain 2015, 16, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L. A pain neuromatrix approach to patients with chronic pain. Man. Ther. 2003, 8, 130–140. [Google Scholar] [CrossRef]
- Louw, A.; Puentedura, E.L.; Zimney, K. Teaching patients about pain: It works, but what should we call it? Physiother. Theory Pract. 2016, 32, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Puentedura, E.J.; Zimney, K.; Schmidt, S. Know Pain, Know Gain? A Perspective on Pain Neuroscience Education in Physical Therapy. J. Orthop. Sports Phys. Ther. 2016, 46, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Paul van Wilgen, C.; Van Oosterwijck, J.; van Ittersum, M.; Meeus, M. How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: Practice guidelines. Man. Ther. 2011, 16, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Jackson, T.; Pope, L.; Nagasaka, T.; Fritch, A.; Iezzi, T.; Chen, H. The impact of threatening information about pain on coping and pain tolerance. Br. J. Health Psychol. 2005, 10, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Arntz, A.; Claassens, L. The meaning of pain influences its experienced intensity. Pain 2004, 109, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L.; Arntz, A. The context of a noxious stimulus affects the pain it evokes. Pain 2007, 133, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Boerner, K.E.; Noel, M.; Birnie, K.A.; Caes, L.; Petter, M.; Chambers, C.T. Impact of Threat Level, Task Instruction, and Individual Characteristics on Cold Pressor Pain and Fear among Children and Their Parents. Pain Pract. 2016, 16, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Caes, L.; Vervoort, T.; Trost, Z.; Goubert, L. Impact of parental catastrophizing and contextual threat on parents’ emotional and behavioral responses to their child’s pain. Pain 2012, 153, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Murray, E.; Lo, B.; Pollack, L.; Donelan, K.; Catania, J.; Lee, K.; Zapert, K.; Turner, R. The impact of health information on the Internet on health care and the physician-patient relationship: National U.S. survey among 1.050 U.S. physicians. J. Med. Internet Res. 2003, 5, e17. [Google Scholar] [CrossRef] [PubMed]
- Geisser, M.E.; Roth, R.S. Knowledge of and agreement with chronic pain diagnosis: Relation to affective distress, pain beliefs and coping, pain intensity, and disability. J. Occup. Rehabil. 1998, 8, 73–88. [Google Scholar] [CrossRef]
- Williams, D.A.; Keefe, F.J. Pain beliefs and the use of cognitive-behavioral coping strategies. Pain 1991, 46, 185–190. [Google Scholar] [PubMed]
- Jaaniste, T.; Hayes, B.; von Baeyer, C.L. Providing Children with Information about Forthcoming Medical Procedures: A Review and Synthesis. Clin. Psychol. Sci. Pract. 2007, 14, 124–143. [Google Scholar] [CrossRef]
- Jordan, A.L.; Eccleston, C.; Osborne, M. Being a parent of the adolescent with complex chronic pain: An interpretative phenomenological analysis. Eur. J. Pain 2007, 11, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Moseley, L. Unraveling the barriers to reconceptualization of the problem in chronic pain: The actual and perceived ability of patients and health professionals to understand the neurophysiology. J. Pain 2003, 4, 184–189. [Google Scholar] [CrossRef]
- Nutkiewicz, M. Diagnosis versus dialogue: Oral testimony and the study of pediatric pain. Oral. Hist. Rev. 2008, 35, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Chorney, J.M.; Crofton, K.; McClain, B.C. Theories on Common Adolescent Pain Syndromes. In Handbook of Pediatric Chronic Pain; McClain, B.C., Suresh, S., Eds.; Springer: New York, NY, USA, 2011; pp. 27–44. [Google Scholar]
- Kenshalo, D.R.; Florida State University. The Skin Senses; Proceedings; Thomas: Springfield, IL, USA, 1968. [Google Scholar]
- Basch, M.C.; Chow, E.T.; Logan, D.E.; Schechter, N.L.; Simons, L.E. Perspectives on the clinical significance of functional pain syndromes in children. J. Pain Res. 2015, 8, 675–686. [Google Scholar] [PubMed]
- Meeus, M.; Nijs, J.; Van Oosterwijck, J.; Van Alsenoy, V.; Truijen, S. Pain physiology education improves pain beliefs in patients with chronic fatigue syndrome compared with pacing and self-management education: A double-blind randomized controlled trial. Arch. Phys. Med. Rehabil. 2010, 91, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Bushnell, M.C.; Ceko, M.; Low, L.A. Cognitive and emotional control of pain and its disruption in chronic pain. Nat. Rev. Neurosci. 2013, 14, 502–511. [Google Scholar] [CrossRef] [PubMed]
- Mansour, A.; Baria, A.T.; Tetreault, P.; Vachon-Presseau, E.; Chang, P.C.; Huang, L.; Apkarian, A.V.; Baliki, M.N. Global disruption of degree rank order: A hallmark of chronic pain. Sci. Rep. 2016, 6, 34853. [Google Scholar] [CrossRef] [PubMed]
- Leventhal, H.; Brisette, I.; Leventhal, E.A. The common-sense model of self-regulation of health and illness. In the Self-Regulation of Health and Illness Behavior; Cameron, L.D., Leventhal, H., Eds.; Routledge: London, UK, 2003; pp. 42–65. [Google Scholar]
- Hale, E.D.; Treharne, G.J.; Kitas, G.D. The common-sense model of self-regulation of health and illness: How can we use it to understand and respond to our patients’ needs? Rheumatology (Oxford) 2007, 46, 904–906. [Google Scholar] [CrossRef] [PubMed]
- Siemonsma, P.C.; Schroder, C.D.; Dekker, J.H.; Lettinga, A.T. The benefits of theory for clinical practice: Cognitive treatment for chronic low back pain patients as an illustrative example. Disabil. Rehabil. 2008, 30, 1309–1317. [Google Scholar] [CrossRef] [PubMed]
- Ward, S.; Donovan, H.; Gunnarsdottir, S.; Serlin, R.C.; Shapiro, G.R.; Hughes, S. A randomized trial of a representational intervention to decrease cancer pain (RIDcancerPain). Health Psychol. 2008, 27, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Loeser, J.D. Chapter 2 Pain as a disease. Handb. Clin. Neurol. 2006, 81, 11–20. [Google Scholar] [PubMed]
- Vlaeyen, J.W.; Linton, S.J. Fear-Avoidance model of chronic musculoskeletal pain: 12 years on. Pain 2012, 153, 1144–1147. [Google Scholar] [CrossRef] [PubMed]
- De Jong, J.R.; Vlaeyen, J.W.; van Eijsden, M.; Loo, C.; Onghena, P. Reduction of pain-related fear and increased function and participation in work-related upper extremity pain (WRUEP): Effects of exposure in vivo. Pain 2012, 153, 2109–2118. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.; Linton, S.J. Fear-Avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain 2000, 85, 317–332. [Google Scholar] [CrossRef]
- Den Hollander, M.; Goossens, M.; de Jong, J.; Ruijgrok, J.; Oosterhof, J.; Onghena, P.; Smeets, R.; Vlaeyen, J.W. Expose or protect? A randomized controlled trial of exposure in vivo vs pain-contingent treatment as usual in patients with complex regional pain syndrome type 1. Pain 2016, 157, 2318–2329. [Google Scholar] [CrossRef] [PubMed]
- Coakley, R.; Schechter, N. Chronic pain is like... The clinical use of analogy and metaphor in the treatment of chronic pain in children. Pediatr. Pain Lett. 2013, 15, 1–8. [Google Scholar]
- Brown, L.K.; Beattie, R.M.; Tighe, M.P. Practical management of functional abdominal pain in children. Arch. Dis. Child. 2016, 101, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Huston, S.A.; Houk, C.P. Common sense model of illness in youth with type 1 diabetes or sickle cell disease. J. Pediatr. Pharmacol. Ther. 2011, 16, 270–280. [Google Scholar] [PubMed]
- McGrath, P.J.; Stevens, B.J.; Walker, S.M.; Zempsky, W.T. Oxford Textbook of Paediatric Pain; Oxford University Press: Oxford, UK; New York, NY, USA, 2014. [Google Scholar]
- Simons, L.E.; Smith, A.; Kaczynski, K.; Basch, M. Living in fear of your child’s pain: The Parent Fear of Pain Questionnaire. Pain 2015, 156, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Simons, L.E.; Kaczynski, K.J. The Fear Avoidance model of chronic pain: Examination for pediatric application. J. Pain 2012, 13, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Clarke, C.L.; Ryan, C.G.; Martin, D.J. Pain neurophysiology education for the management of individuals with chronic low back pain: Systematic review and meta-analysis. Man. Ther. 2011, 16, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Zimney, K.; Puentedura, E.J.; Diener, I. The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Physiother. Theory Pract. 2016, 32, 332–355. [Google Scholar] [CrossRef] [PubMed]
- Abram, H.S.; Buckloh, L.M.; Schilling, L.M.; Wiltrout, S.A.; Ramirez-Garnica, G.; Turk, W.R. A randomized, controlled trial of a neurological and psychoeducational group appointment model for pediatric headaches. Child. Health Care 2007, 36, 249–265. [Google Scholar] [CrossRef]
- Fisher, E.; Heathcote, L.; Palermo, T.M.; de C Williams, A.C.; Lau, J.; Eccleston, C. Systematic review and meta-analysis of psychological therapies for children with chronic pain. J. Pediatr. Psychol. 2014, 39, 763–782. [Google Scholar] [CrossRef] [PubMed]
- Kashikar-Zuck, S.; Ting, T.V.; Arnold, L.M.; Bean, J.; Powers, S.W.; Graham, T.B.; Passo, M.H.; Schikler, K.N.; Hashkes, P.J.; Spalding, S.; et al. Cognitive behavioral therapy for the treatment of juvenile fibromyalgia: A multisite, single-blind, randomized, controlled clinical trial. Arthritis. Rheum. 2012, 64, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Levy, R.L.; Langer, S.L.; Walker, L.S.; Romano, J.M.; Christie, D.L.; Youssef, N.; DuPen, M.M.; Feld, A.D.; Ballard, S.A.; Welsh, E.M.; et al. Cognitive-Behavioral Therapy for Children With Functional Abdominal Pain and Their Parents Decreases Pain and Other Symptoms. Am. J. Gastroenterol. 2010, 105, 946–956. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Butler, D.S.; Diener, I.; Puentedura, E.J. Development of a preoperative neuroscience educational program for patients with lumbar radiculopathy. Am. J. Phys. Med. Rehabil. 2013, 92, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Puentedura, E.J.; Diener, I.; Peoples, R.R. Preoperative therapeutic neuroscience education for lumbar radiculopathy: A single-case fMRI report. Physiother. Theory Pract. 2015, 31, 496–508. [Google Scholar] [CrossRef] [PubMed]
- Aubin, M.; Vezina, L.; Parent, R.; Fillion, L.; Allard, P.; Bergeron, R.; Dumont, S.; Giguère, A. Impact of an educational program on pain management in patients with cancer living at home. Oncol. Nurs. Forum 2006, 33, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- Chambers, C.T.; Reid, G.J.; McGrath, P.J.; Finley, G.A.; Ellerton, M.L. A randomized trial of a pain education booklet: Effects on parents’ attitudes and postoperative pain management. Child. Health Care 1997, 26, 1–13. [Google Scholar] [CrossRef]
- Sadegh Tabrizi, J.; Seyedhejazi, M.; Fakhari, A.; Ghadimi, F.; Hamidi, M.; Taghizadieh, N. Preoperative Education and Decreasing Preoperative Anxiety Among Children Aged 8–10 Years Old and Their Mothers. Anesth. Pain Med. 2015, 5, e25036. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.G.; Gray, H.G.; Newton, M.; Granat, M.H. Pain biology education and exercise classes compared to pain biology education alone for individuals with chronic low back pain: A pilot randomised controlled trial. Man. Ther. 2010, 15, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Pires, D.; Cruz, E.B.; Caeiro, C. Aquatic exercise and pain neurophysiology education versus aquatic exercise alone for patients with chronic low back pain: A randomized controlled trial. Clin. Rehabil. 2015, 29, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Mannerkorpi, K.; Nyberg, B.; Ahlmen, M.; Ekdahl, C. Pool exercise combined with an education program for patients with fibromyalgia syndrome. A prospective, randomized study. J. Rheumatol. 2000, 27, 2473–2481. [Google Scholar] [PubMed]
- Moseley, L. Combined physiotherapy and education is efficacious for chronic low back pain. Aust. J. Physiother. 2002, 48, 297–302. [Google Scholar] [CrossRef]
- Moseley, G.L. Joining forces—Combining cognition-targeted motor control training with group or individual pain physiology education: A successful treatment for chronic low back pain. J. Man. Manip. Ther. 2003, 11, 88–94. [Google Scholar] [CrossRef]
- Salvetti Mde, G.; Cobelo, A.; Vernalha Pde, M.; Vianna, C.I.; Canarezi, L.C.; Calegare, R.G. Effects of a psychoeducational program for chronic pain management. Rev. Lat. Am. Enfermagem. 2012, 20, 896–902. [Google Scholar] [CrossRef] [PubMed]
- Campos, A.A.; Amaria, K.; Campbell, F.; McGrath, P.A. Clinical Impact and Evidence Base for Physiotherapy in Treating Childhood Chronic Pain. Physiother. Can. 2011, 63, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, L.; McAuley, J.; Moseley, G.L. A randomized-controlled trial of using a book of metaphors to reconceptualize pain and decrease catastrophizing in people with chronic pain. Clin. J. Pain 2013, 29, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L. Painful Yarns: Metaphors and Stories to Help Understand the Biology of Pain; Dancing Giraffe Press: Minneapolis, MN, USA, 2007. [Google Scholar]
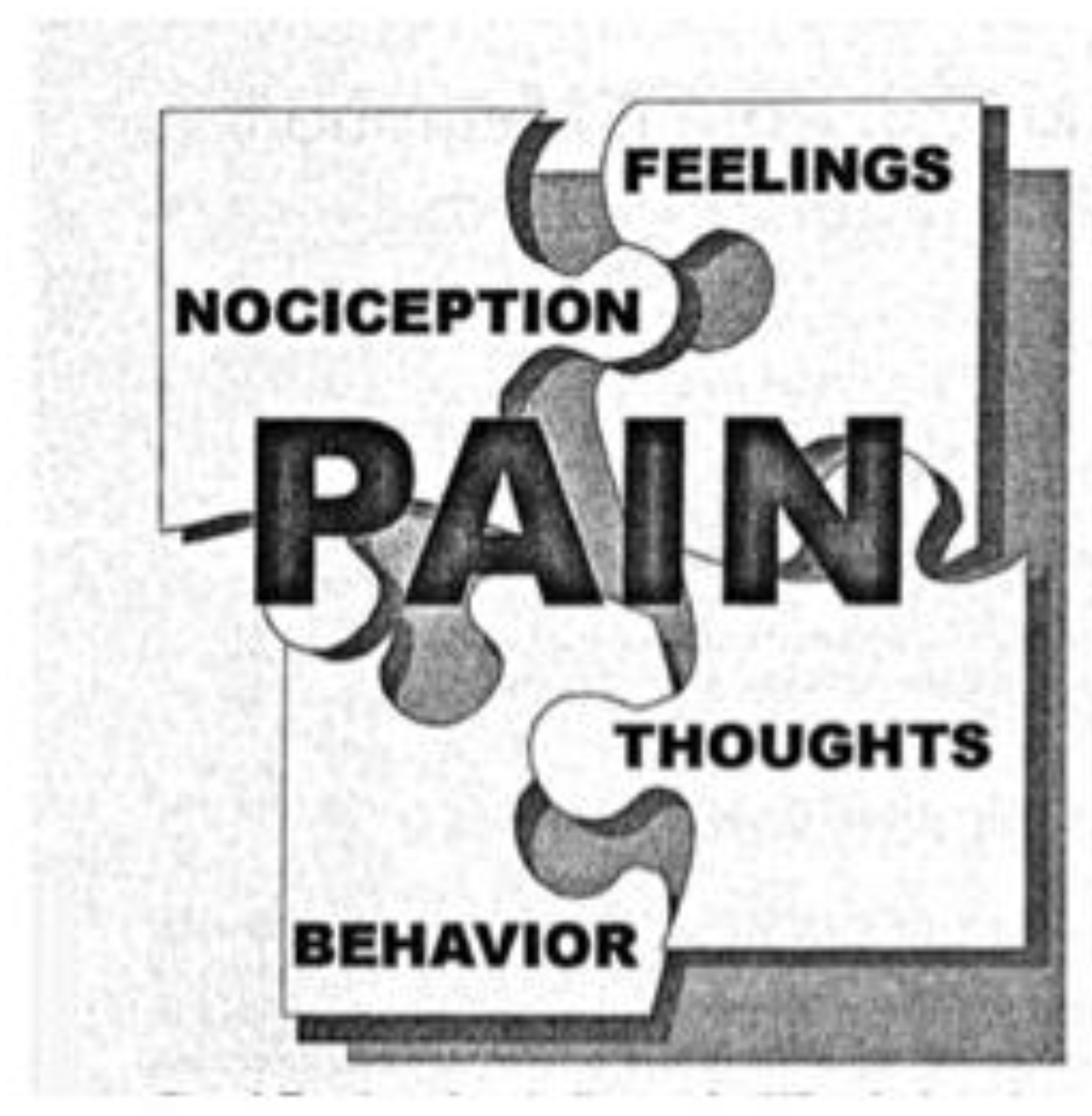
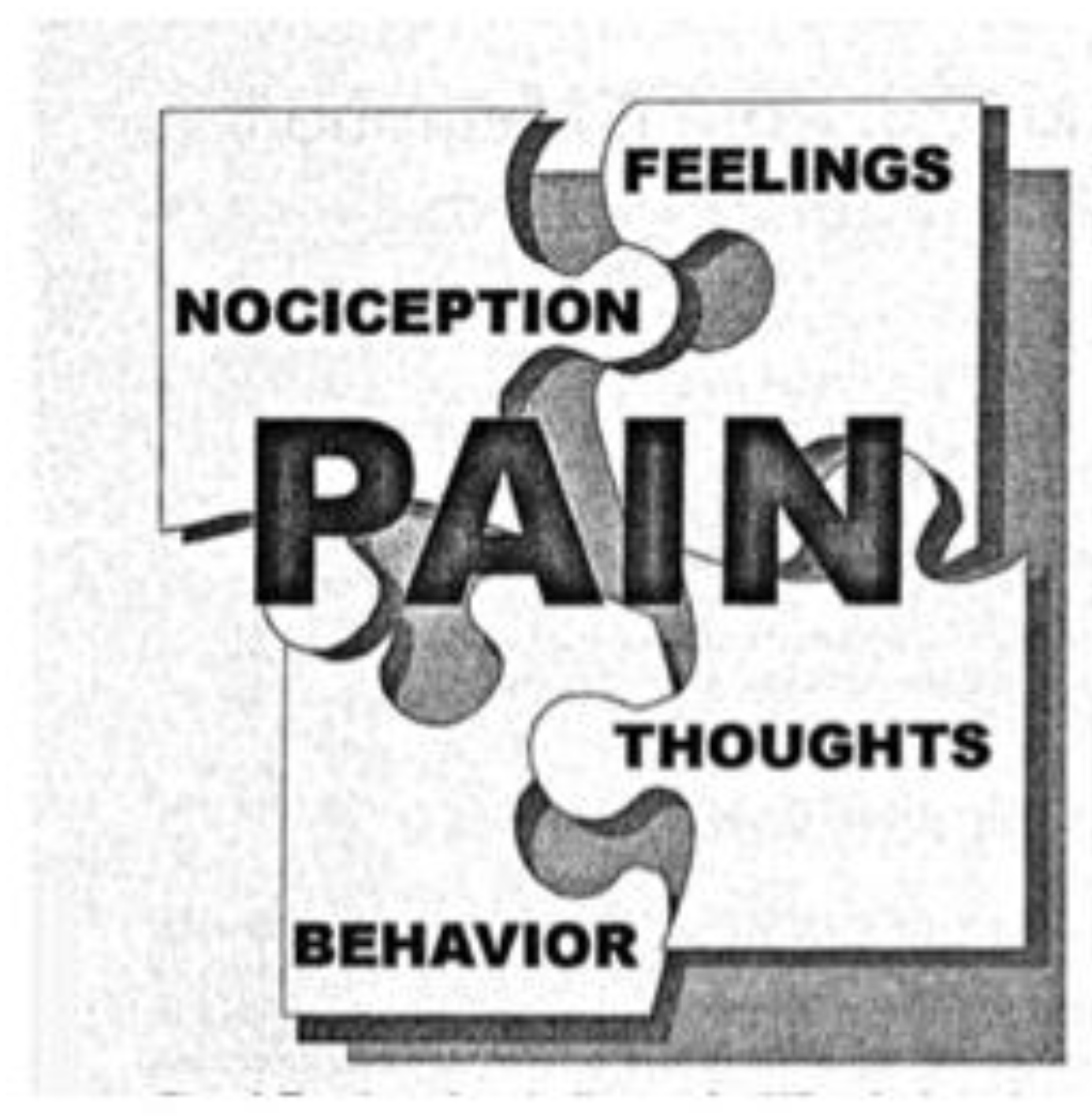
- Rapoff, M.A.; Lindsley, C.B. The pain puzzle: A visual and conceptual metaphor for understanding and treating pain in pediatric rheumatic disease. J. Rheumatol. Suppl. 2000, 58, 29–33. [Google Scholar] [PubMed]
- Butler, D.S.; Moseley, G. Explain Pain; Noigroup Publications: Adelaide, Australia, 2013. [Google Scholar]
- Van Oosterwijck, J.; Meeus, M.; Paul, L.; De Schryver, M.; Pascal, A.; Lambrecht, L.; Nijs, J. Pain physiology education improves health status and endogenous pain inhibition in fibromyalgia: A double-blind randomized controlled trial. Clin. J. Pain 2013, 29, 873–882. [Google Scholar] [CrossRef] [PubMed]
- Van Oosterwijck, J.; Nijs, J.; Meeus, M.; Truijen, S.; Craps, J.; Van den Keybus, N.; Paul, L. Pain neurophysiology education improves cognitions, pain thresholds, and movement performance in people with chronic whiplash: A pilot study. J. Rehabil. Res. Dev. 2011, 48, 43–58. [Google Scholar] [CrossRef] [PubMed]
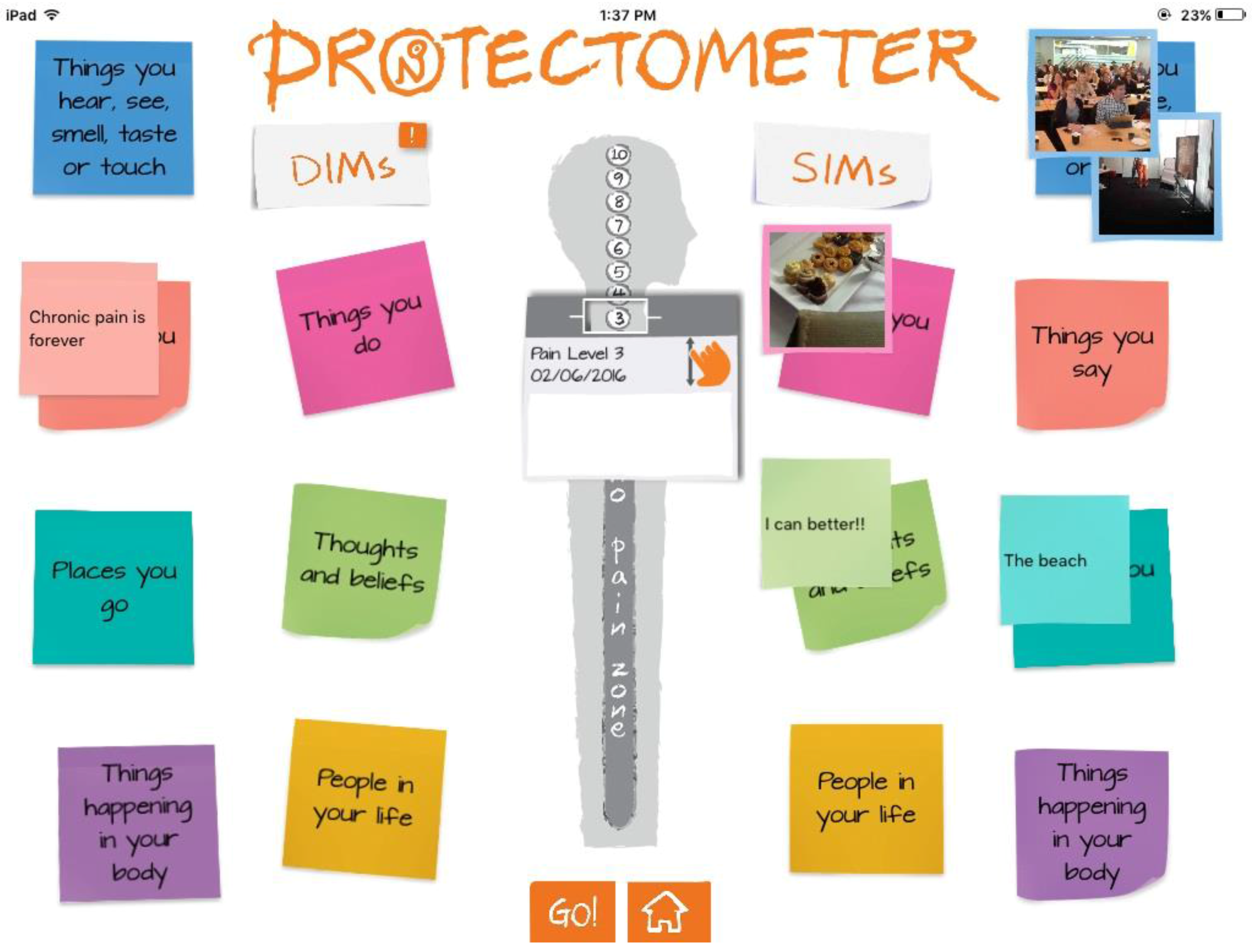
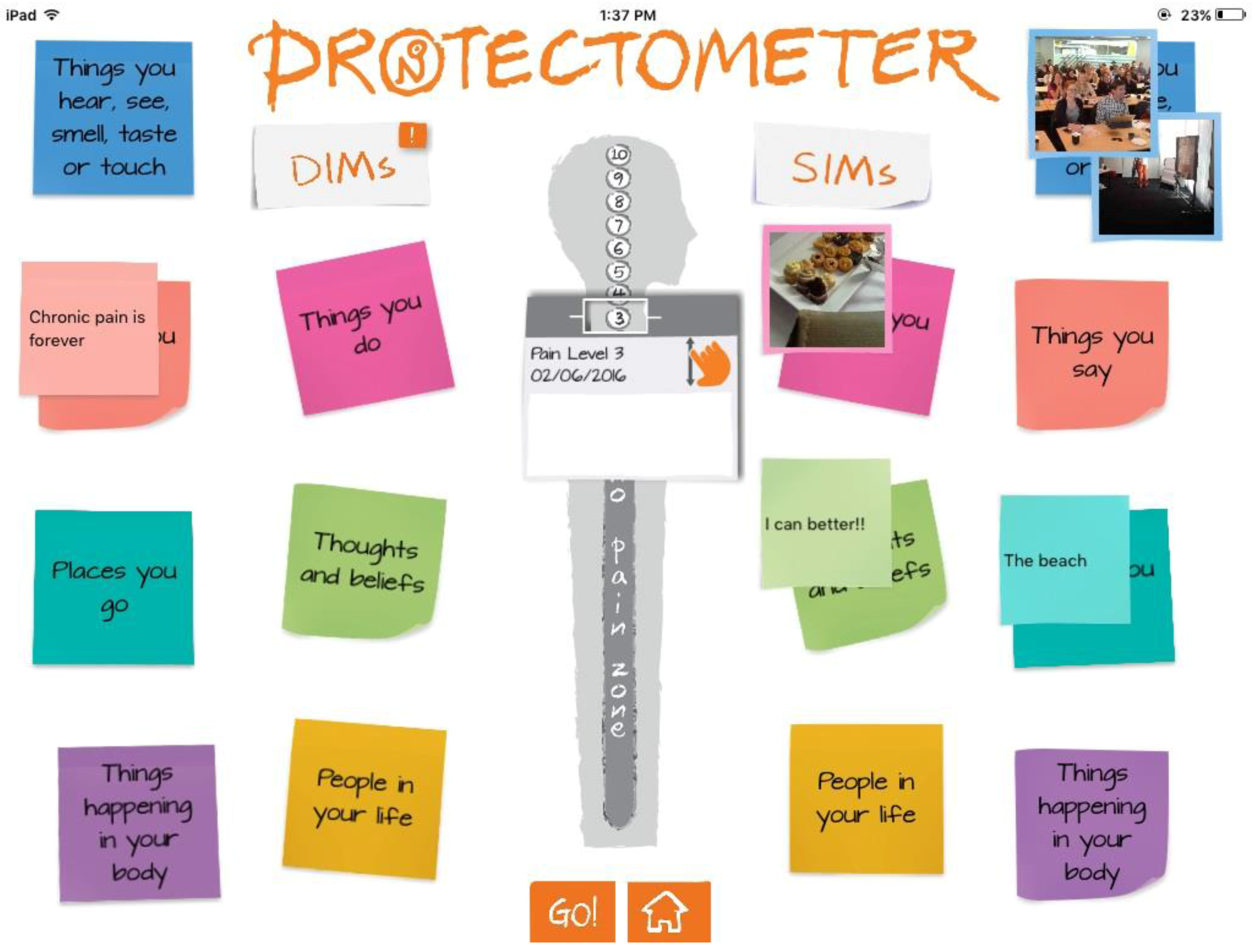
- Moseley, G.L.; Butler, D.S. The Explain Pain Handbook: Protectometer; Noigroup Publications: Adelaide, Australia, 2015. [Google Scholar]
- Louw, A. Why do I hurt?: A Patient Book about the Neuroscience of Pain, 1st ed.; International Spine and Pain Institute: Story City, IA, USA, 2013. [Google Scholar]
- Louw, A.; Hilton, S.; Vandyken, C. Why Pelvic Pain Hurts, 1st ed.; International Spine And Pain Institute: Story City, IA, USA, 2014. [Google Scholar]
- Louw, A.; Diener, I. Your Headache Isn’t all in Your Head: Neuroscience Education for Patients with Headache Pain, 1st ed.; International Spine and Pain Institute: Story City, IA, USA, 2014. [Google Scholar]
- Louw, A. Whiplash: An Alarming Message from Your Nerves; International Spine and Pain Institute: Story City, IA, USA, 2012. [Google Scholar]
- Louw, A. Your Nerves Are Having Back Surgery, 1st ed.; International Spine and Pain Institute: Story City, IA, USA, 2012. [Google Scholar]
- Louw, A.; Flynn, T.; Puentedura, E.J. Everyone Has Back Pain, 1st ed.; International Spine and Pain Institute: Story City, IA, USA, 2015. [Google Scholar]
- Louw, A.; Puentedura, E.J. Therapeutic Neuroscience Education: Teaching Patients about Pain, 1st ed.; International Spine and Pain Institute: Story City, IA, USA, 2013. [Google Scholar]
- Louw, A. Why You Hurt: Therapeutic Neuroscience Education System; International Spine and Pain Institute: Story City, IA, USA, 2014. [Google Scholar]
- Appliquette. Protectometer. Appliquette. 2016. Available online: http://www.appliquette.com.au/project/protectometer/ (accessed on 30 July 2016).
- Van Ittersum, M.W.; van Wilgen, C.P.; van der Schans, C.P.; Lambrecht, L.; Groothoff, J.W.; Nijs, J. Written pain neuroscience education in fibromyalgia: A multicenter randomized controlled trial. Pain Pract. 2014, 14, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Van Ittersum, M.W.; van Wilgen, C.P.; Groothoff, J.W.; van der Schans, C.P. Is appreciation of written education about pain neurophysiology related to changes in illness perceptions and health status in patients with fibromyalgia? Patient Educ. Couns. 2011, 85, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Zeltzer, L.; Schlank, C.B. Conquering Your Child’s Chronic Pain: A Pediatrician’s Guide for Reclaiming a Normal Childhood; HarperCollins: New York, NY, USA, 2005. [Google Scholar]
- Krane, E.J.; Mitchell, D. Relieve Your Child’s Chronic Pain: A Doctor’s Program for Easing Headaches, Abdominal Pain, Fibromyalgia, Juvenile Rheumatoid Arthritis, and More; Simon & Schuster: New York, NY, USA, 2005. [Google Scholar]
- Palermo, T.M.; Law, E.F. Managing Your Child’s Chronic Pain; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Wilson, D.; Mackintosh, S.; Nicholas, M.K.; Moseley, G.L. Harnessing group composition-related effects in pain management programs: A review and recommendations. Pain Manag. 2016, 6, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Migraine: How it works and how to get it under control. Deutsches Kinderschmerzzentrum; Center, G.P.P. Available online: https://www.youtube.com/watch?v=JrCdyuDsg6c (accessed on 30 July 2016).
- Hunter Integrated Pain Service. Understanding Pain and What to Do about it in Less Than Five Minutes; HIPS: New Lambton, Australia, 2014. [Google Scholar]
- Noel, M.; Palermo, T.M.; Chambers, C.T.; Taddio, A.; Hermann, C. Remembering the pain of childhood: Applying a developmental perspective to the study of pain memories. Pain 2015, 156, 31–34. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robins, H.; Perron, V.; Heathcote, L.C.; Simons, L.E. Pain Neuroscience Education: State of the Art and Application in Pediatrics. Children 2016, 3, 43. https://doi.org/10.3390/children3040043
Robins H, Perron V, Heathcote LC, Simons LE. Pain Neuroscience Education: State of the Art and Application in Pediatrics. Children. 2016; 3(4):43. https://doi.org/10.3390/children3040043
Chicago/Turabian StyleRobins, Hannah, Victoria Perron, Lauren C. Heathcote, and Laura E. Simons. 2016. "Pain Neuroscience Education: State of the Art and Application in Pediatrics" Children 3, no. 4: 43. https://doi.org/10.3390/children3040043
APA StyleRobins, H., Perron, V., Heathcote, L. C., & Simons, L. E. (2016). Pain Neuroscience Education: State of the Art and Application in Pediatrics. Children, 3(4), 43. https://doi.org/10.3390/children3040043