1. Introduction
Congenital clubfoot, also known as talipes equinovarus, is one of the most common foot deformities in newborns, occurring in approximately 1 in 1000 live births [
1]. This complex deformity includes equinus, hindfoot varus, forefoot adductus, and supination of the foot [
2,
3]. If left untreated, clubfeet can lead to progressive deformity and discomfort [
4]. Untreated clubfeet can adversely impact educational and employment opportunities, as well as self-esteem and personal development [
5,
6]. The primary goal of clubfoot treatment is to attain a plantigrade, functionally sound foot with a normal range of motion (ROM).
Historically, the treatment of clubfeet has been predominantly surgical, involving extensive surgical release after prolonged casting in infancy [
7]. However, long-term studies have shown limitations in range of motion, foot function, and quality of life in surgically treated patients [
8]. In addition, patients who undergo fewer surgical procedures tend to have better outcomes, highlighting the potential of conservative treatment approaches. In this context, the Ponseti method, a conservative treatment, has emerged as the global gold standard for clubfoot correction [
9]. Known for its simplicity, cost-effectiveness and high success rate, the Ponseti method involves a combination of manipulative techniques, casting, and bracing [
3].
Although numerous studies have shown the favorable outcomes of the Ponseti method [
10], there are limited data documenting its long-term advantages in terms of morphology, function, and, quality of life compared to the formerly used surgical approach in long-term trials. The aim of this prospective study was to evaluate the long-term outcomes of clubfoot treatment 18 years post-intervention in young adults by comparing the Ponseti method with surgical treatment.
4. Discussion
The aim of this investigation was to evaluate the long-term effects of the Ponseti method for correcting clubfoot on functionality, anatomical structure, and quality of life in comparison to surgical interventions in adult individuals. The data indicate that the Ponseti method results in better outcomes in terms of mobility, walking capabilities, and overall quality of life. Deviations from normal radiographic foot morphology were observed in participants from both treatment cohorts when measured against standard physiological benchmarks.
The Ponseti method is widely regarded as the most effective treatment for clubfoot in recent years. Numerous studies have confirmed its efficacy, particularly in terms of short-term outcomes [
25]. Furthermore, retrospective analyses of long-term efficacy have supported these findings [
10]. However, there is a lack of prospective studies comparing the long-term outcomes of the Ponseti method with surgical interventions in young adults. Prospective studies are crucial for ensuring that therapeutic results for clubfoot treatment remain constant throughout skeletal maturation and can withstand the increasing biomechanical forces exerted on the feet during the transition to ambulation. Ponseti emphasized the importance of such studies and showed that individuals with clubfeet can achieve satisfactory function and mobility even into adolescence and young adulthood [
3].
The Ponseti group had superior outcomes regarding ROM, particularly ankle dorsiflexion. This finding is consistent with previous research on conservative clubfoot management in adolescents [
26,
27]. Notably, similar to retrospective long-term follow-up, our study showed persistent structural deviations in both treatment groups [
10], despite improved ROM in the Ponseti group. Invasive surgical procedures can generate scar tissue that may hinder ankle mobility and restrict range of motion during growth [
28]. It is possible that scar tissue plays a significant role in reduced mobility among clubfoot patients who have undergone surgery due to the early initiation of treatment.
Although, the radiographic evaluations showed minimal distinctions between the groups, there was a noticeable prevalence of flat-top talus in the surgical cohort. The reduced range of motion may be explained by the documented evidence that a flatter talus adversely affects ankle joint mobility [
29,
30]. Additionally, the persistent deformities evident in the radiological assessments of both treatment groups suggest that inferior mobility among patients who underwent surgical intervention could also be attributed to the formation of scar tissue subsequent to surgery.
For individuals with clubfeet, activities of daily living and ambulation are of paramount importance, going beyond the isolated metrics of range of motion and radiological morphology. By employing the function subscales of the FRS, the AOFAS Hindfoot and Midfoot Scales, as well as the ICFSG evaluation, we were able to comprehensively assess and delineate the superior functional outcomes associated with Ponseti-treated clubfeet. Although the FRS did not detect any differences in gait, objective gait analysis revealed significant differences in ankle kinematics and kinetics between the two groups. The Ponseti group demonstrated increased ankle range of motion during walking, consistent with the favorable findings from clinical range of motion assessments. The surgical cohort showed diminished ankle moments and powers, which signify a substantial functional limitation and impede normal propulsion. The reduced ankle power during push-off in the surgical cohort may be due to inadequate lever arm mechanics caused by greater instability in overcorrected clubfeet. These findings align with prior research that elucidates the impact of clubfoot treatment on gait dynamics [
26,
31]. GPS did not show any difference between both groups. This is not surprising, as the GPS might not represent the changes in the ankle kinematics adequately [
32]. While clubfoot treatment has a noticeable effect on ankle joint mechanics, its impact on knee and hip joints is relatively minor.
Beside gait analysis, this study employed several patient-related outcome measures, with assessing perceived pain levels being a crucial component. Individuals within the surgical cohort consistently reported significantly higher levels of pain across all scales used. These findings are consistent with a previous study that compared pain levels between Ponseti clubfoot treatment and surgical intervention [
31]. The increased pain experienced after surgical treatment may be due to limited range of motion in the ankle and subtalar joints, resulting in mechanical overload and subsequent discomfort.
Mobility, functional capacity, and pain perception are important factors in assessing quality of life. Limitations faced by those who underwent surgical treatment may significantly impede daily functioning. Individuals who underwent surgical intervention reported lower levels of satisfaction and quality of life, consistent with diminished functional outcomes, gait parameters, and pain levels. Additionally, the Ponseti group reported better outcomes in satisfaction scores, as evidenced by the FRS subscale, and the group demonstrated superior scores in the SF-36 assessment, particularly in domains concerning general health and health-related changes. Prior research has reinforced these findings, highlighting the superior quality of life associated with Ponseti treatment in comparison to surgical interventions [
26,
31].
In addition to previously mentioned findings, it is important to address the supplementary interventions observed in both treatment cohorts. In the Ponseti group, four clubfeet required further intervention due to forefoot supination during the swing phase. In contrast, the surgical cohort required additional surgery, with six clubfeet undergoing such procedures. Although some subjects in the Ponseti group may require subsequent surgical interventions, the Ponseti method still remains less invasive than surgical treatments.
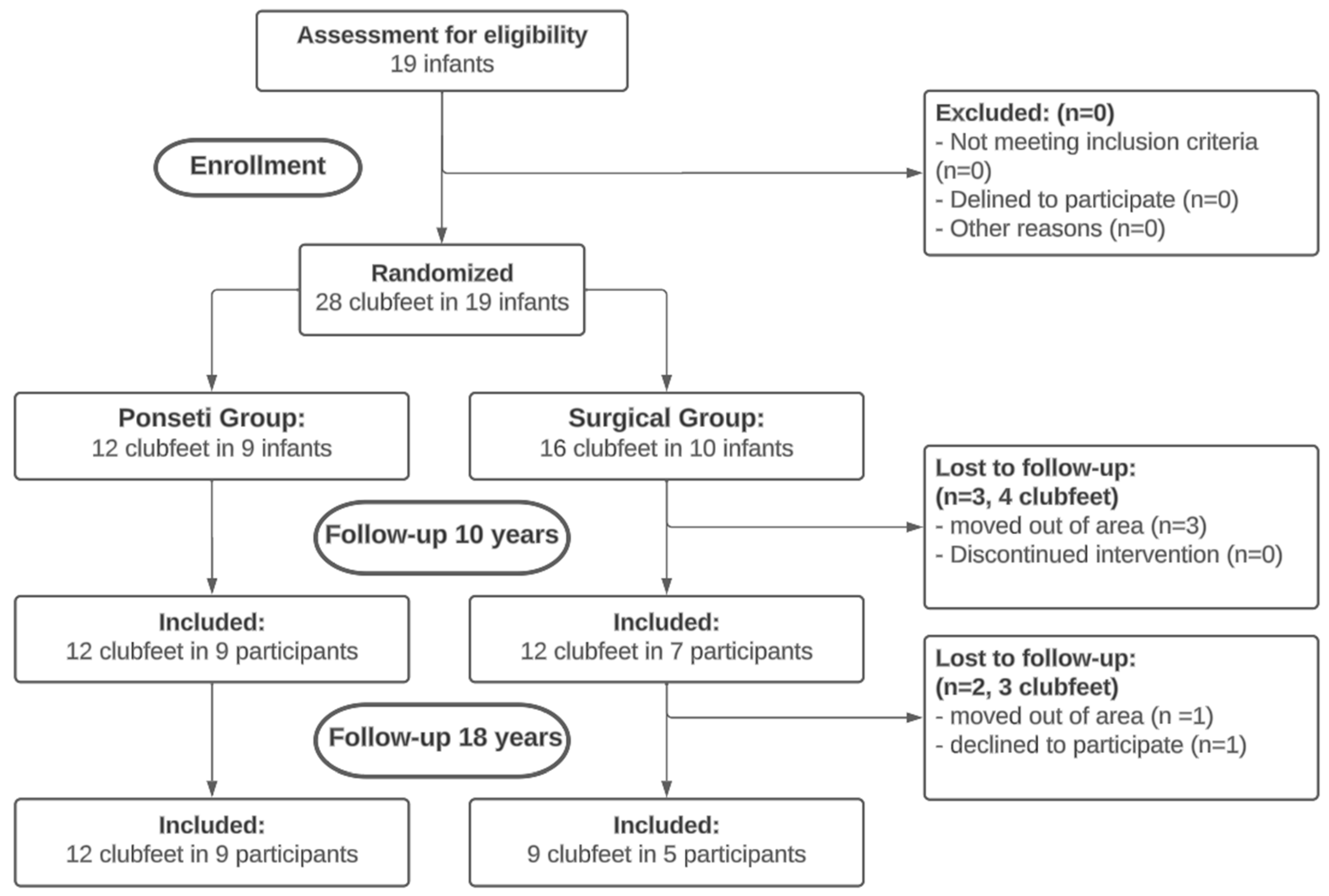
There are several limitations that need to be considered carefully when interpreting the results presented in this paper. The most significant of these is the modest sample size. Following an interim report, the ethical committee halted participant recruitment due to the larger and more invasive interventions required in the surgical group compared to the Ponseti group. The decision was made after enrolling only half of the initially planned subjects, which prevented the attainment of the calculated sample size and a power of 0.9, as outlined by Zwick et al. [
13]. The trial was also affected by dropout, with two participants from the surgical arm leaving the trial, reducing the sample size for long-term follow-up. Furthermore, the lack of blinding among assessors to the treatment allocation presents a limitation. Blinding was impractical due to the conspicuous scarring evident in the surgical group. Therefore, the findings of this study should be interpreted cautiously, recognizing their limited generalizability to the broader population. However, it is important to note that this study is the only prospective randomized trial with such a long follow-up duration in the existing literature.

 ,
, 

{kind=link}