

Marginal and Para-Marginal Technique in Late Germectomy of Lower Third Molars

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Plaque Index
3.2. BoP Index
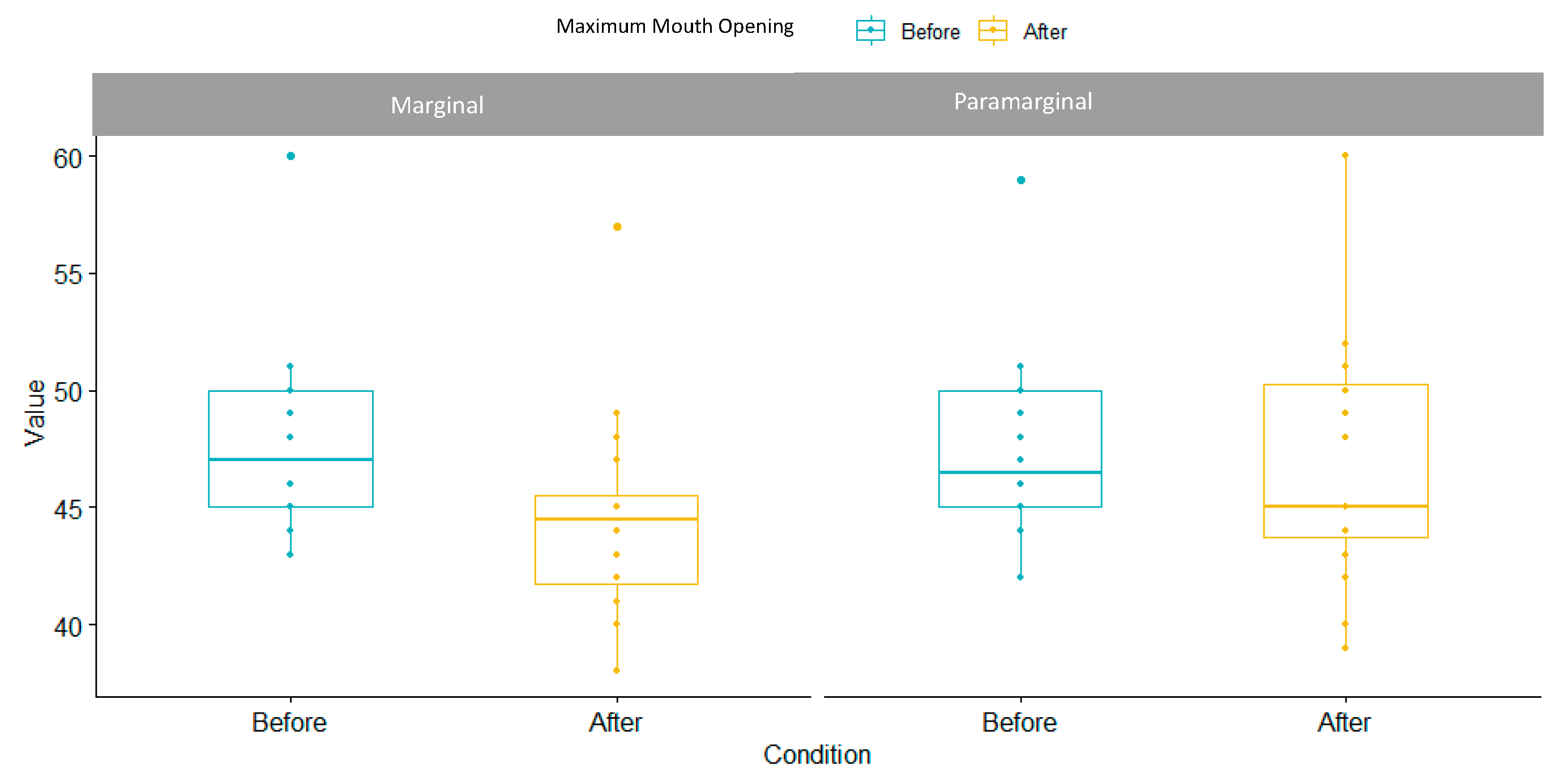
3.3. Maximum Mouth Opening Index
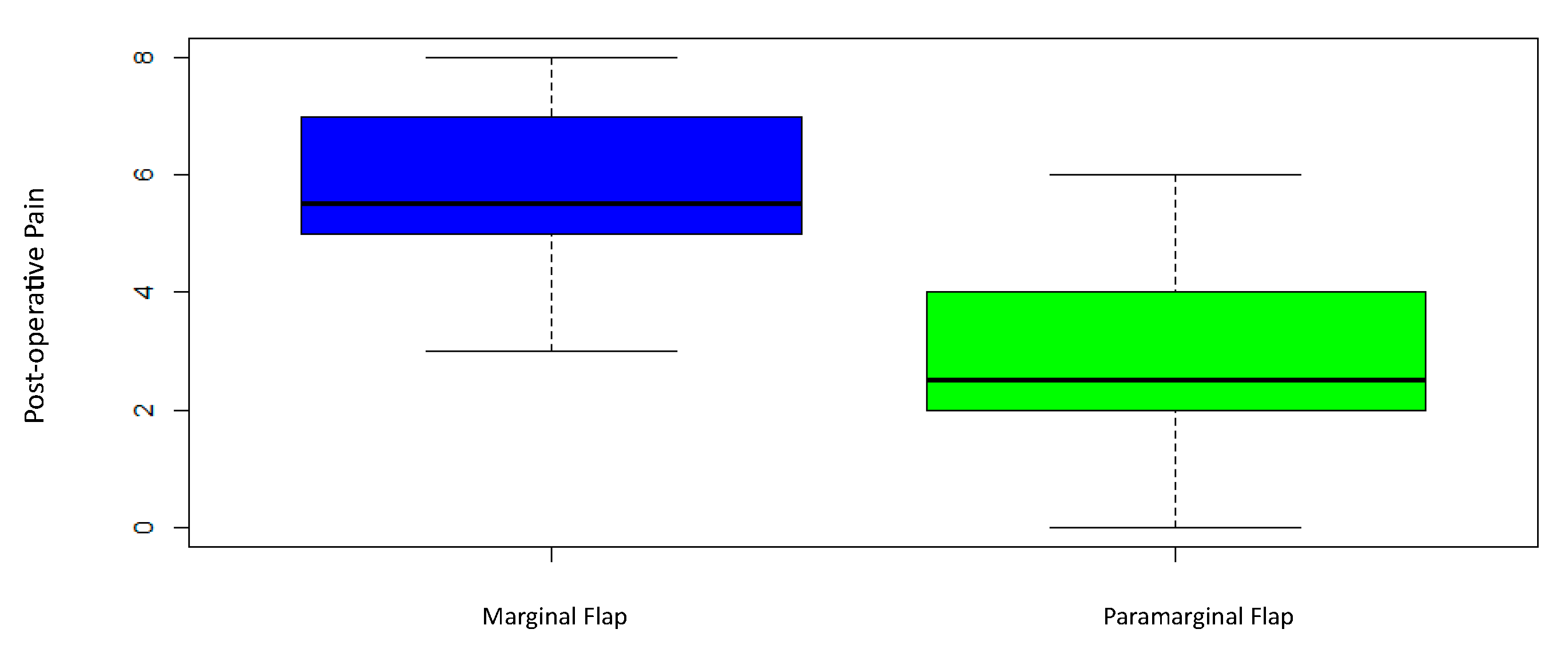
3.4. Post-Operative Pain Perception
3.5. Post-Operative Swelling
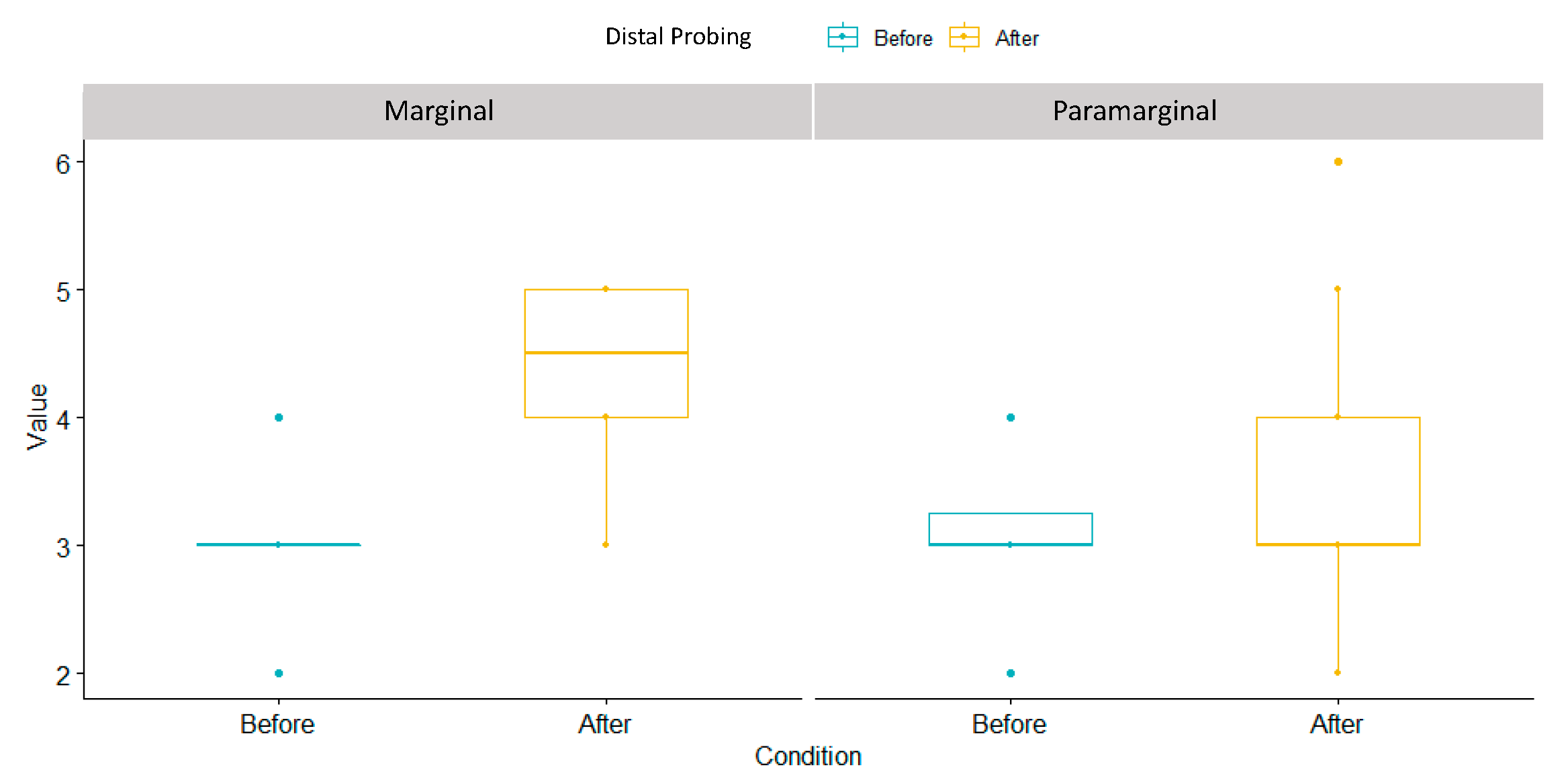
3.6. Distal Probing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garn, S.M.; Lewis, A.B.; Vicinus, J.H. Third molar polymorphism and its significance to dental genetics. J. Dent. Res. 1963, 42, 1344–1363. [Google Scholar] [CrossRef] [PubMed]
- Richardson, M. Impacted third molars. Br. Dent. J. 1995, 178, 92. [Google Scholar] [CrossRef] [PubMed]
- Seward, G.R.; Harris, M.; McGowan, D.A. (Eds.) An Outline of Oral Surgery I; Wright: Oxford, UK, 1999; pp. 52–92. [Google Scholar]
- Peñarrocha-Diago, M.; Camps-Font, O.; Sánchez-Torres, A.; Figueiredo, R.; Sánchez-Garcés, M.A.; Gay-Escoda, C. Indications of the extraction of symptomatic impacted third molars: A systematic review. J. Clin. Exp. Dent. 2021, 13, e278–e286. [Google Scholar] [CrossRef]
- Ghaeminia, H.; Nienhuijs, M.E.; Toedtling, V.; Perry, J.; Tummers, M.; Hoppenreijs, T.J.; Van der Sanden, W.J.; Mettes, T.G. Surgical removal versus retention for the management of asymptomatic disease-free impacted wisdom teeth. Cochrane Database Syst. Rev. 2020, 5, CD003879. [Google Scholar] [CrossRef] [PubMed]
- Mazur, M.; Ndokaj, A.; Marasca, B.; Sfasciotti, G.L.; Marasca, R.; Bossù, M.; Ottolenghi, L.; Polimeni, A. Clinical Indications to Germectomy in Pediatric Dentistry: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 740. [Google Scholar] [CrossRef]
- Sbricoli, L.; Cerrato, A.; Frigo, A.C.; Zanette, G.; Bacci, C. Third Molar Extraction: Irrigation and Cooling with Water or Sterile Physiological Solution: A Double-Blind Randomized Study. Dent. J. 2021, 9, 40. [Google Scholar] [CrossRef]
- Staderini, E.; Patini, R.; Guglielmi, F.; Camodeca, A.; Gallenzi, P. How to Manage Impacted Third Molars: Germectomy or Delayed Removal? A Systematic Literature Review. Medicina 2019, 55, 79. [Google Scholar] [CrossRef]
- Angelo, C.; Nicole, P.C.; Garg, A.K. Early Third Molar Extraction: When Germectomy Is the Best Choise. Interv. Pediatr. Dent. Open Access J. 2020, 4, 350–353. [Google Scholar] [CrossRef]
- Lysell, L.; Rohlin, M. A study of indications used for removal of mandibular third molar. Int. J. Oral Maxillofac. Surg. 1988, 17, 161–164. [Google Scholar] [CrossRef]
- Chen, Y.-W.; Lee, C.-T.; Hum, L.; Chuang, S.-K. Effect of flap design on periodontal healing after impacted third molar extraction: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 363–372. [Google Scholar] [CrossRef]
- Woolf, R.H.; Malmquist, J.P.; Wright, W.H. Third molar extractions: Periodontal implication of two flap designs. Gen. Dent. 1978, 26, 52–56. [Google Scholar]
- Shofield, I.D.; Kogon, S.L.; Donner, A. Long-term comparison of two surgical flap designs for third molar surgery on the health of the periodontal tissue of the second molar tooth. J. Can. Dent. Assoc. 1988, 54, 689–691. [Google Scholar]
- Suarez-Cunqueiro, M.M.; Gutwald, R.; Reichman, J.; Otero-Cepeda, X.L.; Schmelzeisen, R. Marginal flap versus paramarginal flap in impacted third molar surgery: A prospective study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2003, 95, 403–408. [Google Scholar] [CrossRef]
- Shahzad, M.A.; Chatha, M.R.; Sohail, A. Outcome of management of mandibular third molar impaction by comparing two different flap designs. Pak. Oral Dent. J. 2014, 34, pp. 235–238. Available online: https://Link.gale.com/apps/doc/A381474429/AONE?u=anon~19344d62&sid=googleScholar&xid=96bb8df2 (accessed on 20 February 2023).
- Shahzad, M.A.; Munir, M.F.; Chatha, M.R.; Sohail, A. Effect of two triangular flap designs for removal of impacted third molar on maximal mouth opening. Pak. Oral Dent. J. 2015, 35, 190. [Google Scholar]
- Köşger, H.; Polat, H.B.; Demirer, S.; Ozdemir, H.; Ay, S. Periodontal healing of marginal flap versus paramarginal flap in palatally impacted canine surgery: A prospective study. J. Oral Maxillofac. Surg. 2009, 67, 1826–1831. [Google Scholar] [CrossRef]
- Ottria, L.; Luciani, F.; Piva, P.; Alagna, A.M.; Arcuri, C.; Bartuli, F.N. The flap recovery on the impacted lower third molar surgery comparing 3 different flap designs: A clinical study. Oral Implantol. 2017, 10, 270–275. [Google Scholar] [CrossRef]
- Barbato, L.; Kalemaj, Z.; Buti, J.; Baccini, M.; La Marca, M.; Duvina, M.; Tonelli, P. Effect of Surgical Intervention for Removal of Mandibular Third Molar on Periodontal Healing of Adjacent Mandibular Second Molar: A Systematic Review and Bayesian Network Meta-Analysis. J. Periodontol. 2016, 87, 291–302. [Google Scholar] [CrossRef]
- Jakse, N.; Bankaoglu, V.; Wimmer, G.; Eskici, A.; Pertl, C. Primary wound healing after lower third molar surgery: Evaluation of 2 different flap designs. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 93, 7–12. [Google Scholar] [CrossRef]
- Shevel, E.; Koepp, W.G.; Butow, K.W. A subjective assessment of pain and swelling following the surgical removal of impacted third molar teeth using different surgical techniques. SADJ 2001, 56, 238–241. [Google Scholar]
- Glera-Suárez, P.; Soto-Peñaloza, D.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M. Patient morbidity after impacted third molar extraction with different flap designs. A systematic review and meta-analysis. Med. Oral Patol. Oral y Cirugía Buccal 2020, 25, e233–e239. [Google Scholar] [CrossRef] [PubMed]
- de Marco, G.; Lanza, A.; Cristache, C.M.; Capcha, E.B.; Espinoza, K.I.; Rullo, R.; Vernal, R.; Cafferata, E.A.; di Francesco, F. The influence of flap design on patients’ experiencing pain, swelling, and trismus after mandibular third molar surgery: A scoping systematic review. J. Appl. Oral Sci. 2021, 29, e20200932. [Google Scholar] [CrossRef] [PubMed]
- Garcia Garcia, A.; Gude Sampedro, F.; Gandara Rey, J.; Gallas Torreira, M. Trismus and pain after removal of impacted lower third molars. J. Oral Maxillofac. Surg. 1997, 55, 1223–1226. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Herrera, R.S.; Esparza-Villalpando, V.; Bermeo-Escalona, J.R.; Martínez-Rider, R.; Pozos-Guillén, A. Agreement analysis of three mandibular third molar retention classifications. Gac. Med. Mex. 2020, 156, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Karaca, I.; Şimşek, Ş.; Uğar, D.; Bozkaya, S. Review of flap design influence on the health of the periodontium after mandibular third molar surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, 18–23. [Google Scholar] [CrossRef]
- do Nascimento-Júnior, E.M.; Dos Santos, G.M.S.; Tavares Mendes, M.L.; Cenci, M.; Correa, M.B.; Pereira-Cenci, T.; Martins-Filho, P.R.S. Cryotherapy in reducing pain, trismus, and facial swelling after third-molar surgery: Systematic review and meta-analysis of randomized clinical trials. J. Am. Dent. Assoc. 2019, 150, 269–277.e1. [Google Scholar] [CrossRef]
- Duarte de Oliveira, F.J.; Brasil, G.M.L.C.; Araújo Soares, G.P.; Fernandes Paiva, D.F.; de Assis de Souza Júnior, F. Use of low-level laser therapy to reduce postoperative pain, edema, and trismus following third molar surgery: A systematic review and meta-analysis. J. Craniomaxillofac. Surg. 2021, 49, 1088–1096. [Google Scholar] [CrossRef]
- Passarelli, P.C.; Lopez, M.A.; Netti, A.; Rella, E.; Leonardis, M.; Svaluto Ferro, L.; Lopez, A.; Garcia-Godoy, F.; D’Addona, A. Effects of Flap Design on the Periodontal Health of Second Lower Molars after Impacted Third Molar Extraction. Healthcare 2022, 10, 2410. [Google Scholar] [CrossRef]
- Low, S.H.; Lu, S.L.; Lu, H.K. Evidence-based clinical decision making for the management of patients with periodontal osseous defect after impacted third molar extraction: A systematic review and meta-analysis. J. Dent. Sci. 2021, 16, 71–84. [Google Scholar] [CrossRef]
- Hassan, K.S.; Marei, H.F.; Alagl, A.S. Does grafting of third molar extraction sockets enhance periodontal measures in 30- to 35-year-old patients? J. Oral Maxillofac. Surg. 2012, 70, 757–764. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Flap Design | Min | Median | Mean | Variance | Standar Deviation | Max | p-Value |
|---|---|---|---|---|---|---|---|
| Marginal | 2 | 12.5 | 13.3 | 106 | 10.3 | 49 | 0.001264 |
| Paramarginal | −5 | 3 | 3.85 | 35.6 | 5.97 | 18 |
| Pre-Surgical BoP | Flap Design | n | prop |
|---|---|---|---|
| No bleeding | Marginal | 13 | 65% |
| No bleeding | Paramarginal | 11 | 55% |
| Bleeding | Marginal | 7 | 35% |
| Bleeding | Paramarginal | 9 | 45% |
| Post-surgical Bop | Flap design | n | prop |
| No bleeding | Marginal | 1 | 5% |
| No bleeding | Paramarginal | 14 | 70% |
| Bleeding | Marginal | 19 | 95% |
| Bleeding | Paramarginal | 6 | 30% |
| Flap Design | Min | Median | Mean | Variance | Standar Deviation | Max | p-Value |
|---|---|---|---|---|---|---|---|
| Marginal | −8 | −3 | −3.5 | 3.32 | 1.82 | 0 | 0.001264 |
| Paramarginal | −6 | −0.5 | −0.7 | 4.75 | 2.18 | 3 |
| Flap Design | Min | Median | Mean | Variance | Standar Deviation | Max | p-Value |
|---|---|---|---|---|---|---|---|
| Marginal | 3 | 5.5 | 5.75 | 1.88 | 1.37 | 8 | 0.000005 |
| Paramarginal | 0 | 2.5 | 2.95 | 3.73 | 1.93 | 6 |
| Post-Operative Swelling | Flap Design | n | prop |
|---|---|---|---|
| No | Paramarginal | 11 | 55% |
| Yes | Paramarginal | 9 | 45% |
| Yes | Marginal | 20 | 100% |
| Flap Design | Min | Median | Mean | Variance | Standar Deviation | Max | p-Value |
|---|---|---|---|---|---|---|---|
| Marginal | 1 | 1 | 1.3 | 0.221 | 0.47 | 2 | 0.0000275 |
| Paramarginal | −1 | 0 | 0.4 | 0.463 | 0.681 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ludovichetti, F.S.; Mazzoleni, S.; Menin, M.; Parcianello, R.G.; Romanowski, F.; Stellini, E.; Zuccon, A. Marginal and Para-Marginal Technique in Late Germectomy of Lower Third Molars. Children 2023, 10, 1077. https://doi.org/10.3390/children10061077
Ludovichetti FS, Mazzoleni S, Menin M, Parcianello RG, Romanowski F, Stellini E, Zuccon A. Marginal and Para-Marginal Technique in Late Germectomy of Lower Third Molars. Children. 2023; 10(6):1077. https://doi.org/10.3390/children10061077
Chicago/Turabian StyleLudovichetti, Francesco Saverio, Sergio Mazzoleni, Manuel Menin, Roberta Gaia Parcianello, Francielle Romanowski, Edoardo Stellini, and Andrea Zuccon. 2023. "Marginal and Para-Marginal Technique in Late Germectomy of Lower Third Molars" Children 10, no. 6: 1077. https://doi.org/10.3390/children10061077
APA StyleLudovichetti, F. S., Mazzoleni, S., Menin, M., Parcianello, R. G., Romanowski, F., Stellini, E., & Zuccon, A. (2023). Marginal and Para-Marginal Technique in Late Germectomy of Lower Third Molars. Children, 10(6), 1077. https://doi.org/10.3390/children10061077