
177Lu-PSMA Radioligand Therapy Is Favorable as Third-Line Treatment of Patients with Metastatic Castration-Resistant Prostate Cancer. A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials

 , ,
, , 
Abstract
1. Introduction
2. Material and Methods
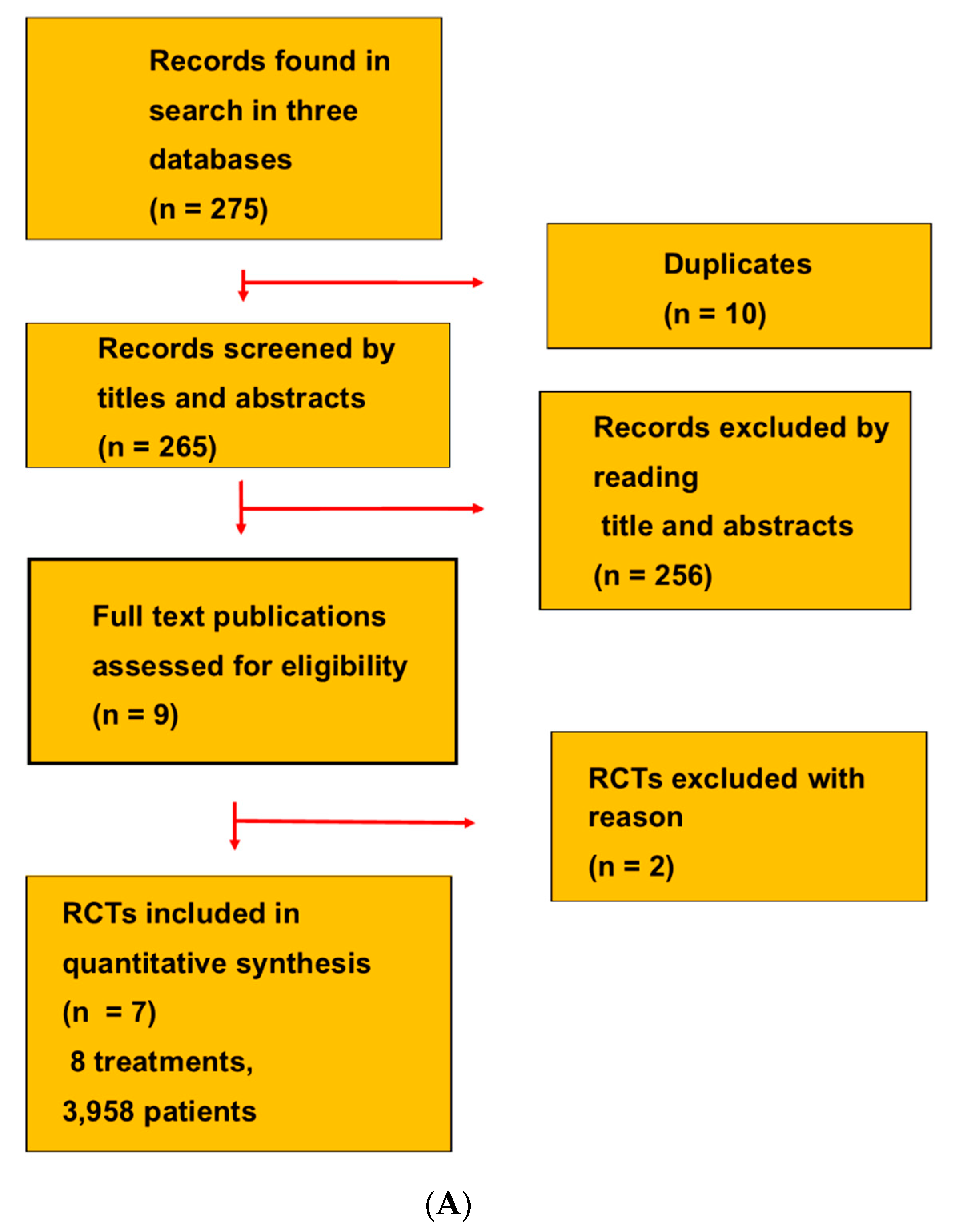
2.1. Selection of Studies
2.2. Search Strategy
2.3. Data Extraction
2.4. Definitions
2.5. Assessment of Risk of Bias
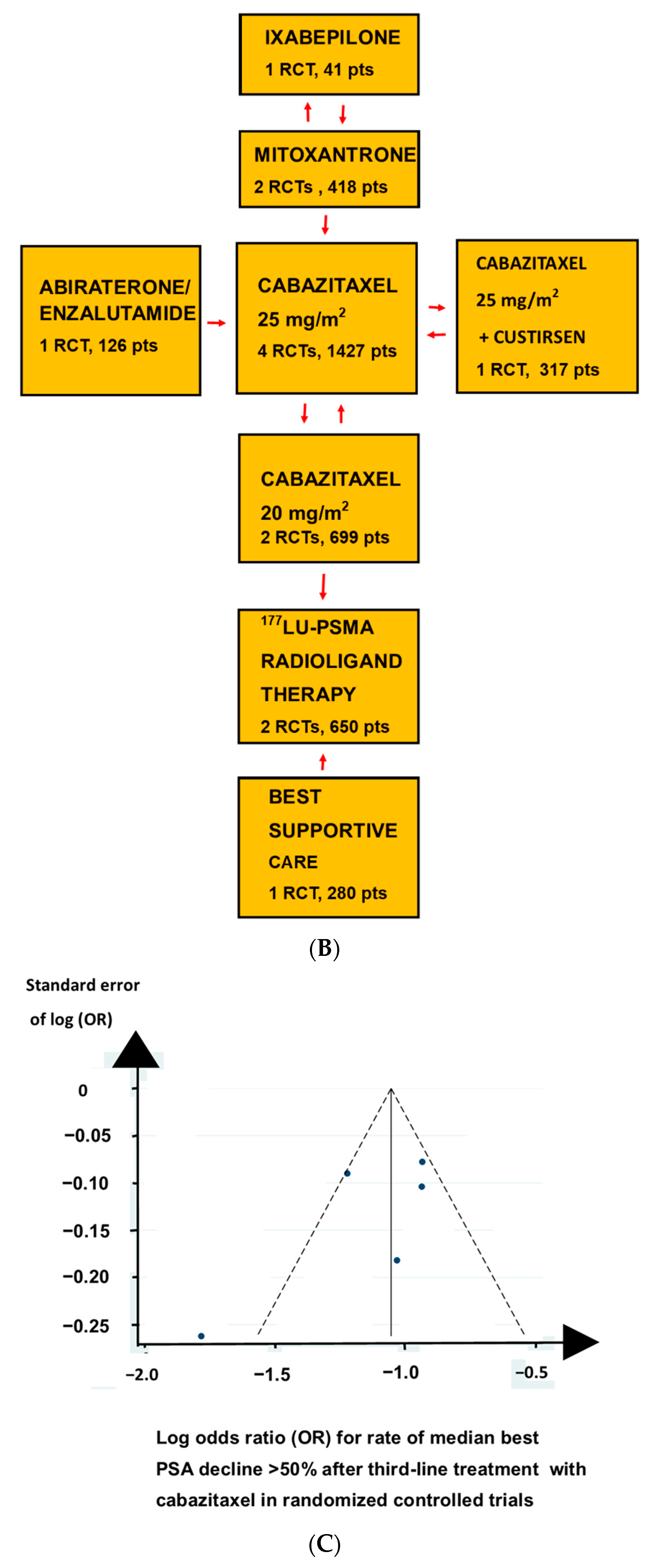
2.6. Statistical Analyses
3. Results
3.1. The Selected RCTs
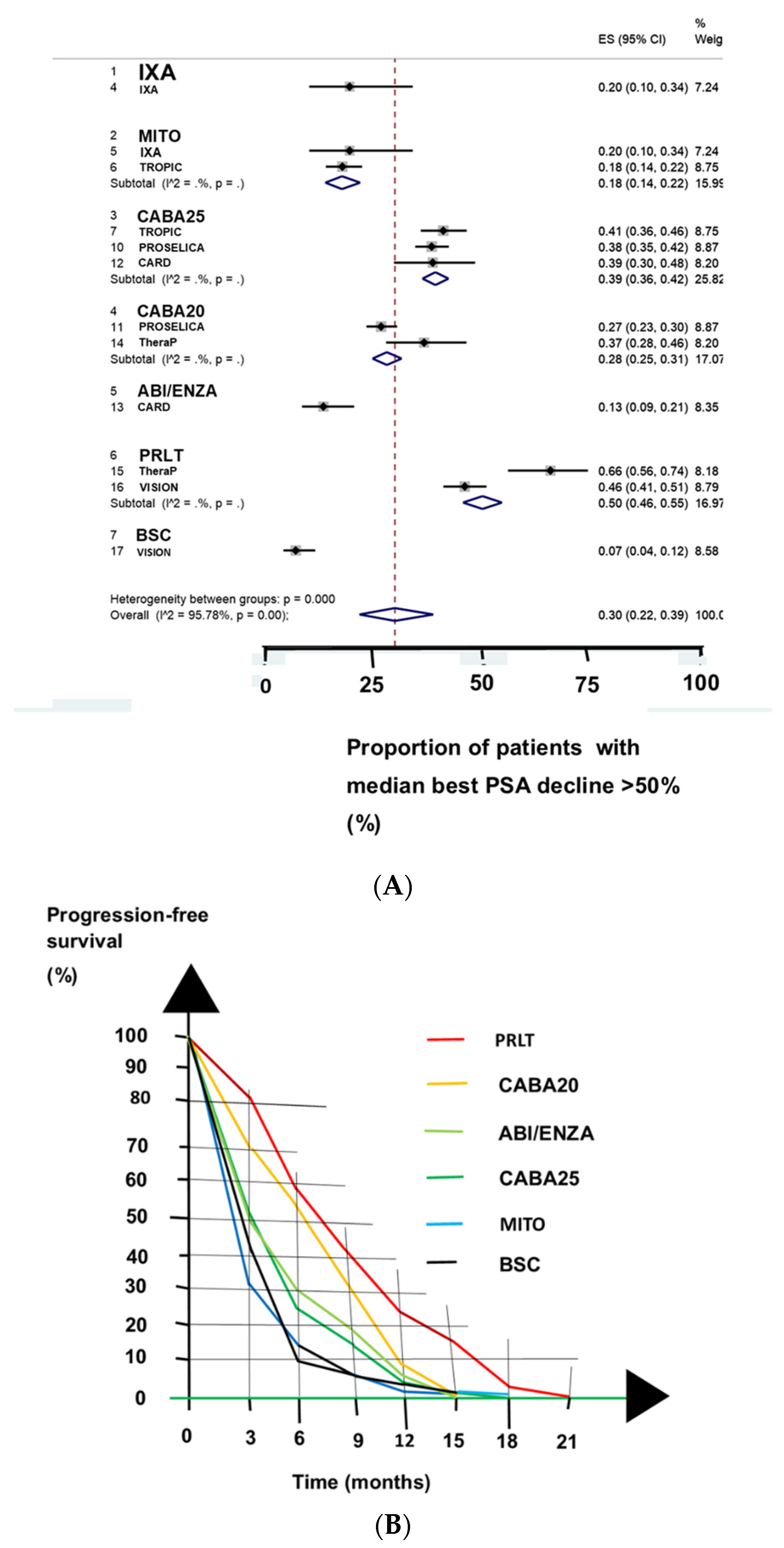
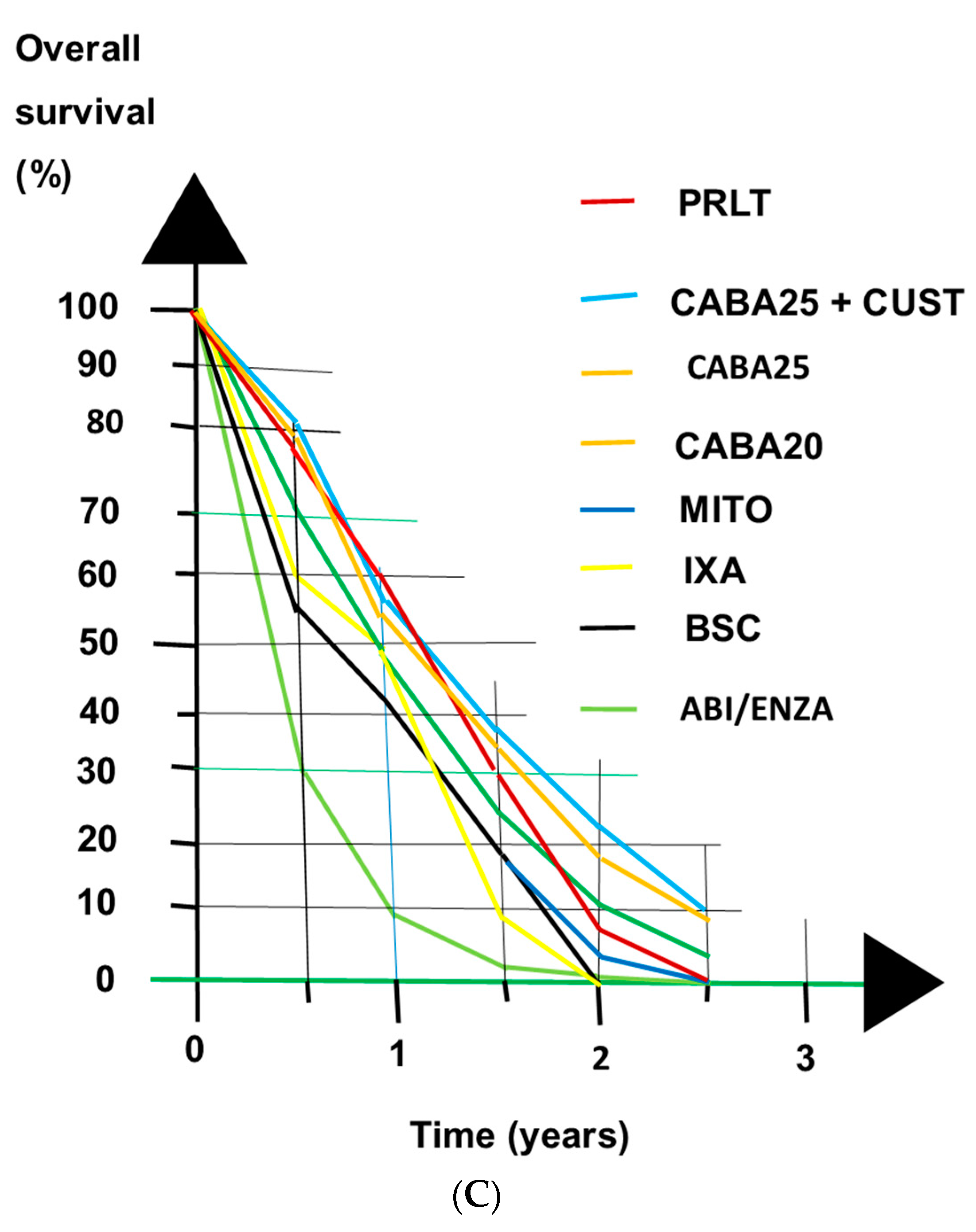
3.2. Clinical Benefits
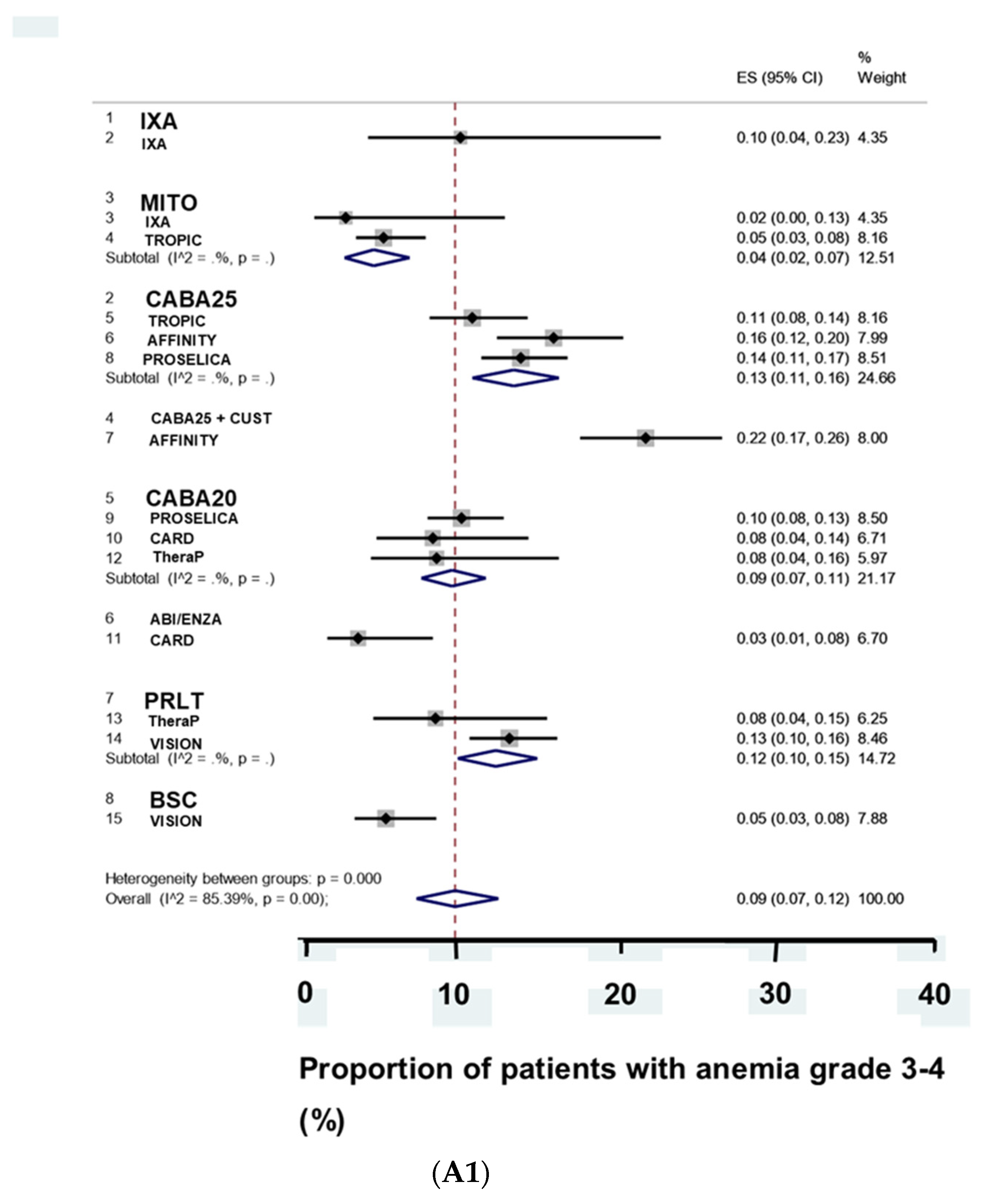
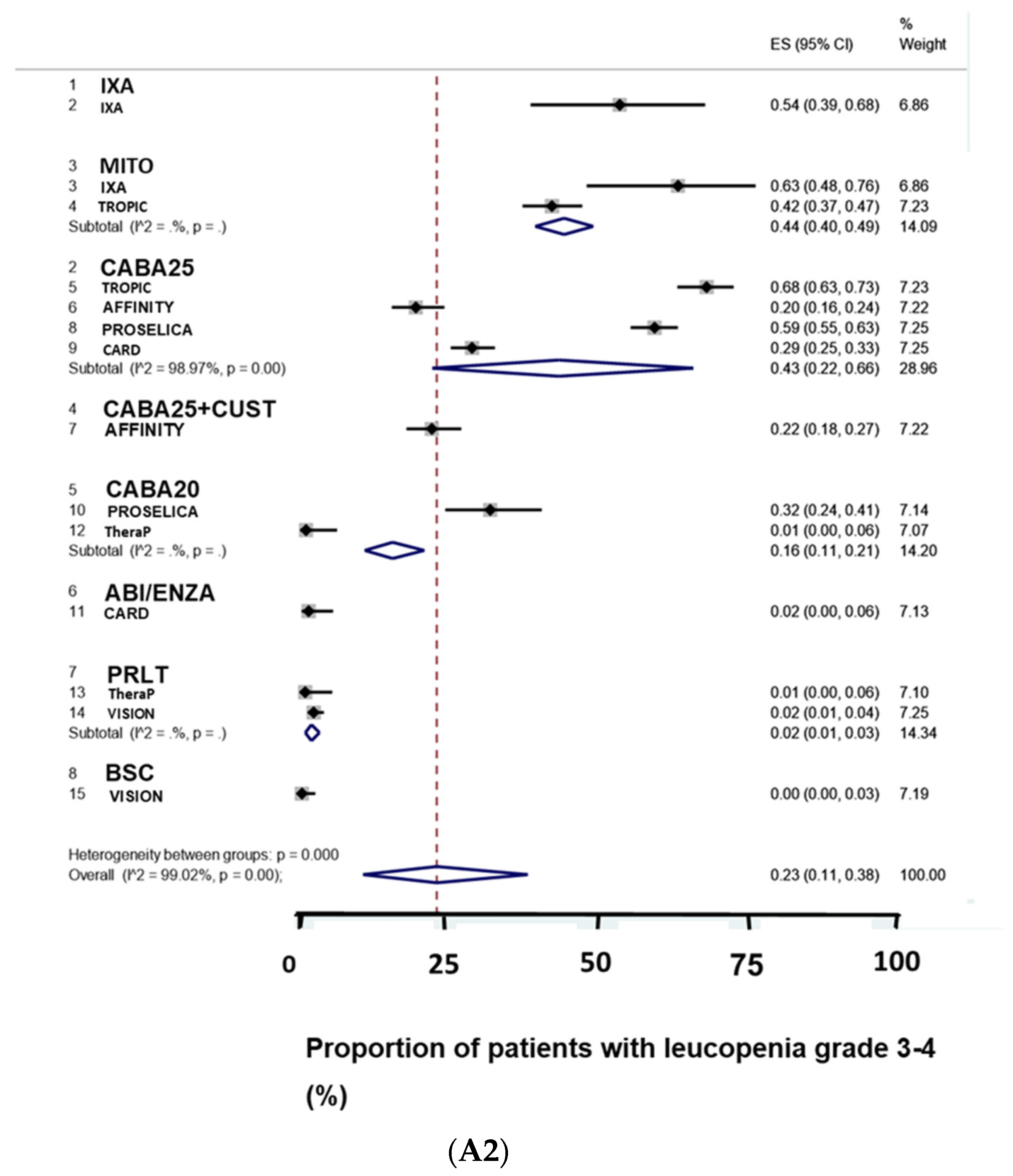
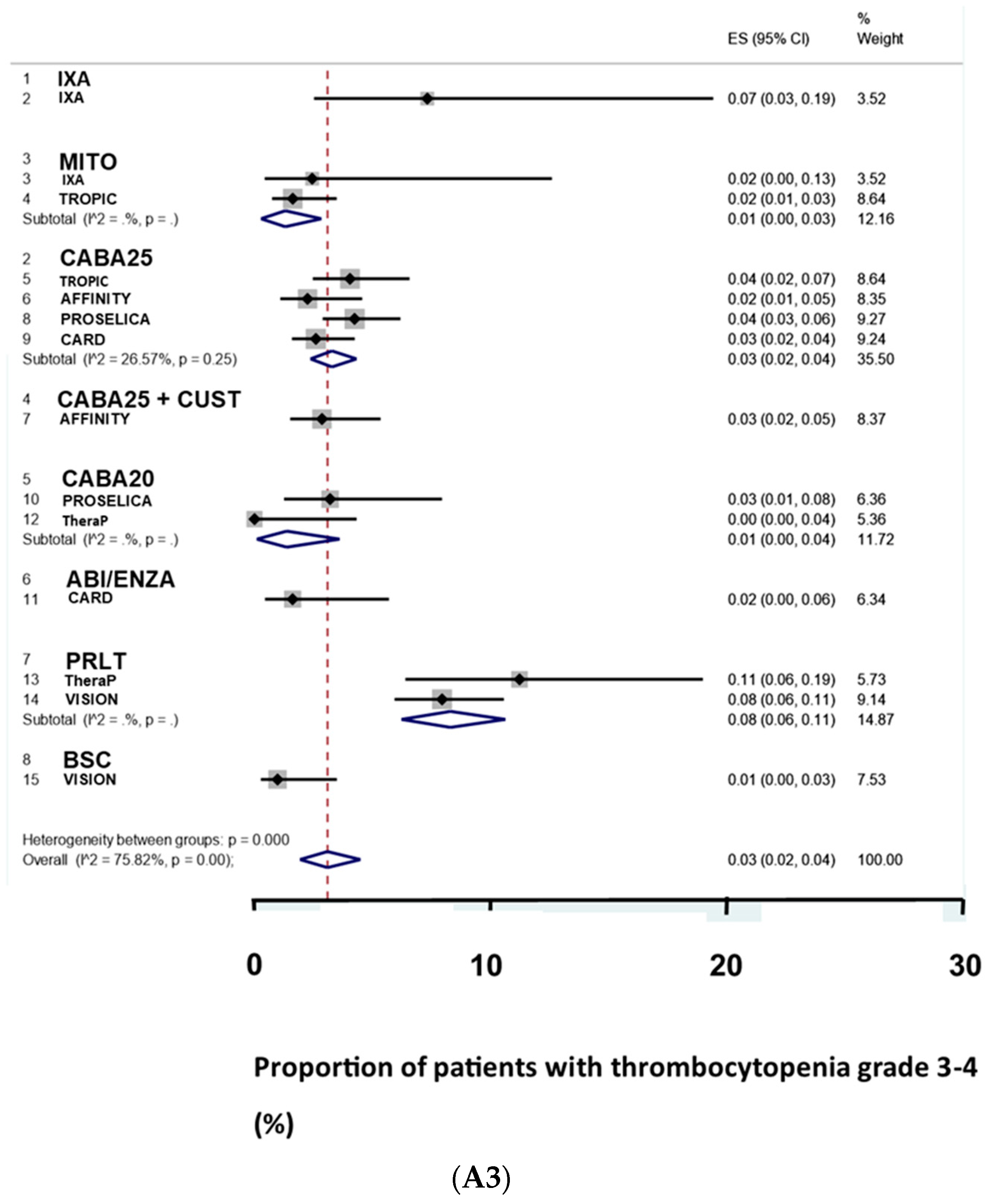
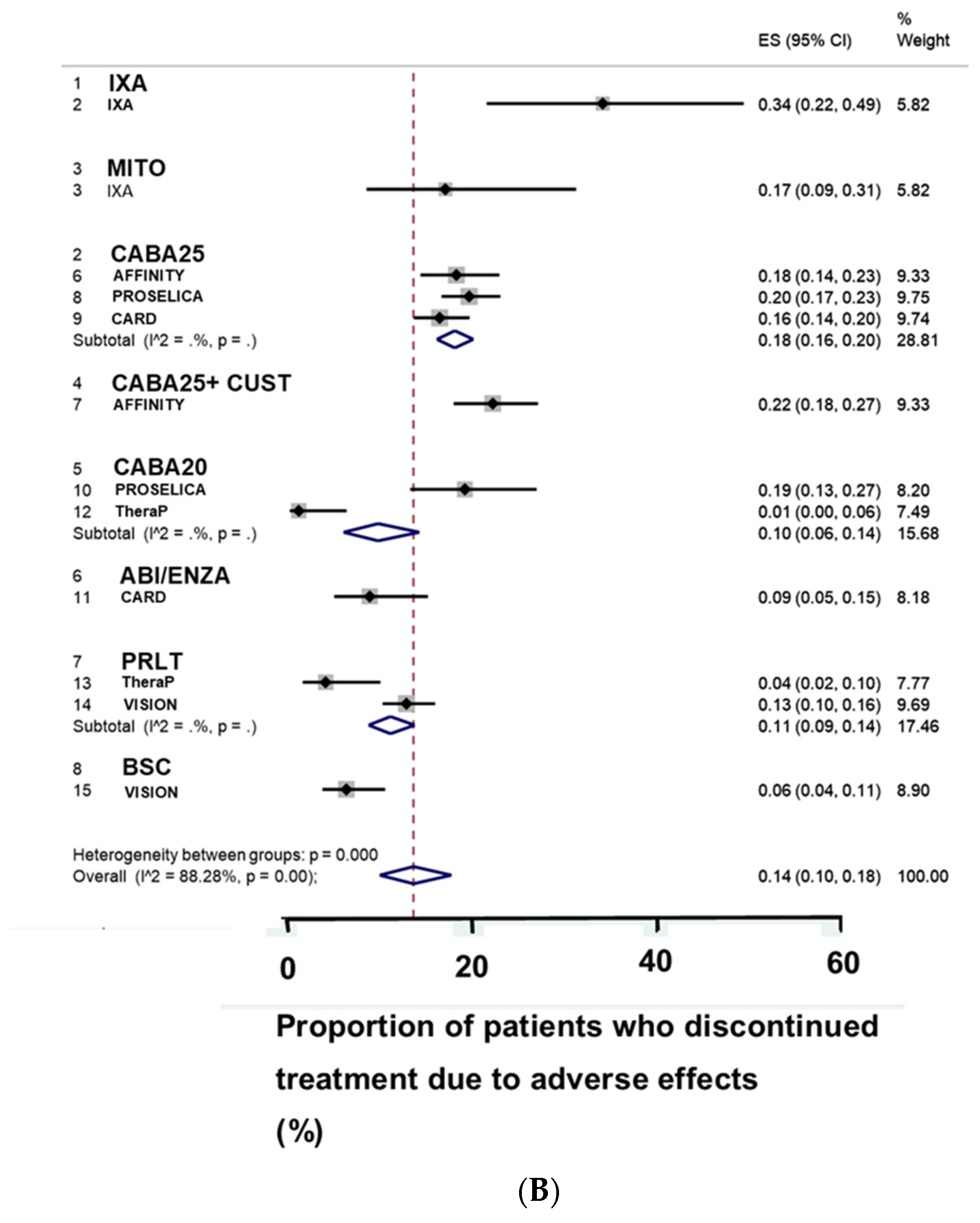
3.3. Adverse Effects
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, S.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer. Part II-2020 Update: Treatment of relapsing and metastatic prostate cancer. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, S.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.J.; Smith, M.R.; de Bono, J.S.; Molina, A.; Logothetis, C.J.; de Souza, P.; Fizazi, K.; Mainwaring, P.; Piulats, L.M.; Ng, S.; et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N. Engl. J. Med. 2013, 368, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Beer, T.M.; Armstrong, A.J.; Rathkopf, D.E.; Loriot, Y.; Sternberg, C.N.; Higano, C.S.; Iversen, P.; Bhattacharya, S.; Carles, J.; Chowdhury, S.; et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N. Engl. J. Med. 2014, 371, 424–433. [Google Scholar] [CrossRef]
- George, D.J.; Sartor, O.; Miller, K.; Saad, F.; Tombal, B.; Kalinovsky, J.; Jiao, X.; Tangirala, K.; Sternberg, C.N.; Higano, C.S.; et al. Treatment patterns and outcomes in patients with metastatic castration-resistant prostate cancer in a real-world clinical practice setting in the United States. Clin. Genitourin. Cancer 2020, 18, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Notohardjo, J.C.L.; Kuppen, M.C.P.; Westgeest, H.M.; van Moorselaar, R.J.A.; Mehra, N.; Coenen, J.; van Oort, I.M.; de Vos, A.I.; Vervenne, W.L.; van den Bergh, A.C.M.; et al. Third-line life-prolonging drug treatment in a real-world metastatic castration-resistant prostate cancer population: Results from the Dutch castration-remistant prostate cancer registry. Eur. Urol. Focus 2020, 27, R713–R715. [Google Scholar] [CrossRef]
- Sathianathen, N.J.; Koschel, S.; Thangasamy, I.A.; Teh, J.; Alghazo, O.; Butcher, G.; Howard, H.; Kapoor, J.; Lawrentschuk, N.; Siva, S.; et al. Indirect comparisons of efficacy between combination approaches in metastatic hormone-sensitive prostate cancer: A systematic review and network meta-analysis. Eur. Urol. 2020, 77, 365–372. [Google Scholar] [CrossRef]
- de Wit, R.; de Bono, J.; Sternberg, C.N.; Fizazi, K.; Tombal, B.; Wulfing, C.; Kramer, G.; Eymard, J.-C.; Bamias, A.; Carles, J.; et al. Cabazitaxel versus abiraterone or enzalutamide in metastatic prostate cancer. N. Engl. J. Med. 2019, 381, 2506–2518. [Google Scholar] [CrossRef]
- von Eyben, F.E.; Roviello, G.; Kiljunen, T.; Uprimny, C.; Virgolini, I.; Kairemo, K.; Joensuu, T. Third-line treatment and 177Lu-PSMA radioligand therapy of metastatic castration-resistant prostate cancer: A systematic review. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 496–508. [Google Scholar] [CrossRef]
- Sadaghiani, M.S.; Sheikhbahaei, S.; Werner, R.A.; Pienta, K.J.; Pomper, M.G.; Solnes, L.B.; Gorin, M.A.; Wang, N.-Y.; Rowe, S.P. A systematic review and meta-analysis of the effectiveness and toxicities of lutetium-177-labeled prostate-specific membrane antigen-targeted radioligand therapy in metastatic castration-resistant prostate cancer. Eur. Urol. 2021, 80, 82–94. [Google Scholar] [CrossRef]
- von Eyben, F.E.; Bauman, G.; von Eyben, R.; Rahbar, K.; Soydal, C.; Haug, A.R.; Virgolini, I.; Kulkarni, H.; Baum, R.; Paganelli, G. Optimizing PSMA radioligand therapy for patients with metastatic castration-resistant prostate cancer. A systematic review and meta-analysis. Int. J. Mol. Sci. 2020, 21, 9054. [Google Scholar] [CrossRef]
- Satapathy, S.; Sood, A.; Das, C.K.; Mittal, B.R. Evolving role of 225Ac-PSMA radioligand therapy in metastatic castration-resistant prostate cancer-a systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2021. [Google Scholar] [CrossRef]
- Sun, M.; Niaz, M.O.; Nelson, A.; Skafida, M.; Niaz, M.J. Review of 177Lu-PSMA-617 in patients with metastatic castration-resistant prostate cancer. Cureus 2020, 12, e8921. [Google Scholar] [CrossRef]
- Satapathy, S.; Mittal, B.R.; Sood, A. Visceral metastases as predictors of response and survival outcomes in patients of castration-resistant prostate cancer treated with 177Lu-labeled prostate-specific membrane antigen radioligand therapy: A systematic review and meta-analysis. Clin. Nucl. Med. 2020, 45, 935–942. [Google Scholar] [CrossRef]
- Yadav, M.P.; Ballal, S.; Sahoo, R.K.; Dwivedi, S.N.; Bal, C. Radioligand therapy with 177Lu-PSMA for metastatic castration-resistant prostate cancer: A systematic review and meta-analysis. Am. J. Roentgenol. 2019, 213, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Kim, Y.I. Therapeutic responses and survival effects of 177Lu-PSMA-617 radioligand therapy in metastatic castrate-resistant prostate cancer: A meta-analysis. Clin. Nucl. Med. 2018, 43, 728–734. [Google Scholar] [CrossRef]
- Calopedos, R.J.S.; Chalasani, V.; Asher, R.; Emmett, L.; Woo, H.H. Lutetium-177-labelled anti-prostate-specific membrane antigen antibody and ligands for the treatment of metastatic castrate-resistant prostate cancer: A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2017, 20, 352–360. [Google Scholar] [CrossRef]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.-H.; Kirkwood, J.D.; Ng, S.; et al. [177Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomised, open-label, phase 2 trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Waishampayan, N.; El-Haddad, G.; et al. Lutetium-177-PSMA-617 for metastatic castration-resistant prostate cancer. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Scher, H.I.; Morris, M.J.; Stadler, W.M.; Higano, C.; Basch, E.; Fizazi, K.; Antonarakis, E.S.; Beer, T.M.; Carducci, M.A.; Chi, K.N.; et al. Trial design and objectives for castration-resistant prostate cancer: Updated recommendations from the Prostate Cancer Clinical Trials Working Group 3. J. Clin. Oncol. 2016, 34, 1402–1418. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Chaimani, A.; Caldwell, D.M.; Schmid, C.; Thorlund, K.; Mills, E.; Catala-Lopez, F.; Turner, L.; Altman, D.G.; et al. The quality of reporting methods and results in network meta-analyses: An overview of reviews and suggestions for improvement. PLoS ONE 2014, 9, e92508. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Jansen, J.P.; Mulrow, C.; Catala-Lopez, F.; Gøtsche, P.C.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Hoskin, P.; Sartor, O.; O’Sullivan, J.M.; Johannessen, D.C.; Helle, S.I.; Logue, J.; Bottomley, D.; Nilsson, S.; Vogelzang, N.J.; Fang, F.; et al. Efficacy and safety of radium-223 dichloride in patients with castration-resistant prostate cancer and symptomatic bone metastases, with or without previous docetaxel use: A prespecified subgroup analysis from the randomised, double-blind, phase 3 ALSYMPCA trial. Lancet Oncol. 2014, 15, 1397–1406. [Google Scholar]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, R.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Bujkiewicz, S.; Jackson, D.; Thompson, J.R.; Turner, R.M.; Stadler, N.; Abrams, K.R.; White, I.R. Bivariate network meta-analysis for surrogate endpoint evaluation. Stat. Med. 2019, 38, 3322–3341. [Google Scholar] [CrossRef]
- Jackson, D.; Law, M.; Barrett, J.K.; Turner, R.; Higgins, J.P.; Salanti, G.; White, I.R. Extending Der Simonian and Laird’s methodology to perform network meta-analyses with random inconsistency effects. Stat. Med. 2016, 35, 819–839. [Google Scholar] [CrossRef]
- Salanti, G.; Ades, A.E.; Ioannidis, J.P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef]
- Efthimiou, O.; Mavridis, D.; Riley, R.D.; Cipriani, A.; Salanti, G. Joint synthesis of multiple correlated outcomes in networks of interventions. Biostatistics 2015, 16, 84–97. [Google Scholar] [CrossRef]
- Tierney, J.F.; Fisher, D.J.; Vale, C.L.; Burdett, S.; Rydzewska, L.H.; Rogozinska, E.; Godolphin, P.J.; White, I.R.; Parmar, M.K.B. A framework for prospective, adaptive meta-analysis (FAME) of aggregate data from randomised trials. PLoS Med. 2021, 18, e1003629. [Google Scholar] [CrossRef]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef]
- White, I. Network meta-analysis. Stata J. 2015, 15, 951–985. [Google Scholar] [CrossRef]
- Mills, E.J.; Ioannidis, J.P.; Thorlund, K.; Schunemann, H.J.; Puhan, M.A.; Guyatt, G.H. How to use an article reporting a multiple treatment comparison meta-analysis. JAMA 2012, 308, 1246–1253. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Dahm, P.; Shukla, V.K.; Higgins, J.; Falck-Ytter, Y.; et al. GRADE guidelines: 7. Rating the quality of evidence--inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- de Bono, J.S.; Oudard, S.; Ozguroglu, M.; Hansen, S.; Machiels, J.P.; Kocak, I.; Gravis, G.; Bodragi, I.; Mackenzie, M.J.; Shen, L.; et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet 2010, 376, 1147–1154. [Google Scholar] [CrossRef]
- Eisenberger, M.; Hardy-Bessard, A.C.; Kim, C.S.; Geczi, L.; Ford, D.; Mourey, L.; Carles, J.; Parente, P.; Font, A.; Kacso, G.; et al. Phase III study comparing a reduced dose of cabazitaxel (20 mg/m2) and the currently approved dose (25 mg/m2) in postdocetaxel patients with metastatic castration-resistant prostate cancer-proselica. J. Clin. Oncol. 2017, 35, 3198–3206. [Google Scholar] [CrossRef] [PubMed]
- Beer, T.M.; Hotte, S.J.; Saad, F.; Alekseev, B.; Matveev, V.; Flechon, A.; Gravis, G.; Joly, F.; Chi, K.N.; Malik, Z.; et al. Custirsen (OGX-011) combined with cabazitaxel and prednisone versus cabazitaxel and prednisone alone in patients with metastatic castration-resistant prostate cancer previously treated with docetaxel (AFFINITY): A randomised, open-label, international, phase 3 trial. Lancet Oncol. 2017, 18, 1532–1542. [Google Scholar] [PubMed]
- Rosenberg, J.E.; Weinberg, V.K.; Kelly, W.K.; Michaelson, D.; Hussain, M.H.; Wilding, G.; Gross, M.; Hutcheon, D.; Small, E.J. Activity of second-line chemotherapy in docetaxel-refractory hormone-refractory prostate cancer patients: Randomized phase 2 study of ixabepilone or mitoxantrone and prednisone. Cancer 2007, 110, 556–563. [Google Scholar] [CrossRef]
- von Eyben, F.E.; Kiljunen, T.; Joensuu, T.; Kairemo, K.; Uprimny, C.; Virgolini, I. 177Lu-PSMA-617 radioligand therapy for a patient with lymph node metastatic prostate cancer. Oncotarget 2017, 8, 66112–66116. [Google Scholar] [CrossRef][Green Version]
- von Eyben, F.E.; Kulkarni, H.R.; Baum, R.P. Metastatic extent predicts survival as patients with metastatic castration-resistant prostate cancer are treated with 177Lu-PSMA radioligand therapy. Theranostics 2020, 10, 4900–4902. [Google Scholar] [CrossRef] [PubMed]
- Ahmadzadehfar, H.; Rahbar, K.; Baum, R.P.; Seifert, R.; Kessel, K.; Bogemann, M.; Kulkarni, H.R.; Zhang, J.; Gerke, C.; Fimmers, R.; et al. Prior therapies as prognostic factors of overall survival in metastatic castration-resistant prostate cancer patients treated with [177Lu]Lu-PSMA-617. A WARMTH multicenter study (the 617 trial). Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 113–122. [Google Scholar] [CrossRef] [PubMed]
- von Eyben, F.E.; Singh, A.; Zhang, J.; Nipsch, K.; Meyrick, D.; Lenzo, N.; Kairemo, K.; Joensuu, T.; Virgolini, I.; Soydal, C.; et al. 177Lu-PSMA radioligand therapy of predominant lymph node metastatic prostate cancer. Oncotarget 2019, 10, 2451–2461. [Google Scholar] [CrossRef][Green Version]
- Wang, F.; Li, Z.; Feng, X.; Yang, D.; Lin, M. Advances in PSMA-targeted therapy for prostate cancer. Prostate Cancer Prostatic Dis. 2021. [Google Scholar] [CrossRef]
- Widjaja, L.; Werner, R.A.; Ross, T.L.; Bengel, F.M.; Derlin, T. Comparison of pretherapeutic osseous tumor volume and standard hematology for prediction of hematotoxicity after PSMA-targeted radioligand therapy. Eur. J. Nucl. Med. Mol. Imaging 2021. [Google Scholar] [CrossRef] [PubMed]
- Meyrick, D.; Gallyamov, M.; Sabarimurugan, S.; Falzone, N.; Lenzo, N. Real-world data analysis of efficacy and survival after Lutetium-177 labelled PSMA ligand therapy in metastatic castration-resistant prostate cancer. Target Oncol. 2021, 16, 369–380. [Google Scholar] [CrossRef]
- Barber, T.W.; Singh, A.; Kulkarni, H.R.; Niepsch, K.; Billah, B.; Baum, R.P. Clinical outcomes of 177Lu-PSMA radioligand therapy in earlier and later phases of metastatic castration-resistant prostate cancer grouped by previous taxane chemotherapy. J. Nucl. Med. 2019, 60, 955–962. [Google Scholar] [CrossRef]
- Rasul, S.; Hartenbach, M.; Wollenweber, T.; Kretschmer-Chott, E.; Grubmuller, B.; Kramer, G.; Shariat, S.; Wadsak, W.; Mitterhauser, M.; Pichler, V.; et al. Prediction of response and survival after standardized treatment with 7400 MBq 177Lu-PSMA-617 every 4 weeks in patients with metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1650–1657. [Google Scholar] [CrossRef]
- Maharaj, M.; Heslop, L.; Govender, T.; Korowlay, N.; Singh, A.; Choudhary, P.; Sathekge, M. The outcome and safety of re-challenge Lutetium-177 PSMA (177Lu-PSMA) therapy with low-dose docetaxel as a radiosensitizer-a promising combination in metastatic castrate-resistant prostate cancer (mCRPC): A case report. Nucl. Med. Mol. Imaging 2021, 55, 136–140. [Google Scholar] [CrossRef]
- Prive, B.M.; Peters, S.M.B.; Muselaers, C.H.J.; van Oort, I.M.; Janssen, M.J.R.; Sedelaar, J.P.M.; Konijnenberg, M.W.; Zamecnik, P.; Verzijlbergen, J.F.; Gerritsen, W.R.; et al. Lutetium-177-PSMA-617 in low-volume hormone-sensitive metastatic prostate cancer: A prospective pilot study. Clin. Cancer Res. 2021, 27, 3595–3601. [Google Scholar] [CrossRef]
- Dhiantravan, N.; Emmett, L.; Joshua, A.M.; Pattison, D.A.; Francis, R.J.; Williams, S.; Sandhu, S.; Davis, I.D.; Vela, J.; Neha, N.; et al. UpFrontPSMA: A randomized phase 2 study of sequential 177Lu-PSMA-617 and docetaxel vs docetaxel in metastatic hormone-naive prostate cancer (clinical trial protocol). BJU. Int. 2021. [Google Scholar] [CrossRef] [PubMed]
- Emmett, L.; Subramaniam, S.; Joshua, A.M.; Crumbaker, M.; Martin, A.; Zhang, A.Y.; Rana, N.; Langford, N.; Mitchell, J.; Yip, S.; et al. ENZA-p trial protocol: A randomized phase II trial using prostate-specific membrane antigen as a therapeutic target and prognostic indicator in men with metastatic castration-resistant prostate cancer treated with enzalutamide (ANZUP 1901). BJU. Int. 2021. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Chen, W.K.; Zhang, W.; Zhang, J.S.; Liu, J.H.; Jiang, Y.M.; Fang, K.-W. Network meta-analysis of the efficacy and adverse effects of several treatments for advanced/metastatic prostate cancer. Oncotarget 2017, 8, 59709–59719. [Google Scholar] [CrossRef] [PubMed]
- Feyerabend, S.; Saad, F.; Li, T.; Ito, T.; Diels, J.; Van Sanden, S.; De Porre, P.; Roiz, R.; Abogunrin, S.; Koufopoulou, M. Survival benefit, disease progression and quality-of-life outcomes of abiraterone acetate plus prednisone versus docetaxel in metastatic hormone-sensitive prostate cancer: A network meta-analysis. Eur. J. Cancer 2018, 103, 78–87. [Google Scholar] [CrossRef]
- McCool, R.; Fleetwood, K.; Glanville, J.; Arber, M.; Goodall, H.; Naidoo, S. Systematic review and network meta-analysis of treatments for chemotherapy-naive patients with symptomatic/Mildly symptomatic metastatic castration-resistant prostate cancer. Value Health 2018, 21, 1259–1268. [Google Scholar] [CrossRef]
- Kassem, L.; Shohdy, K.S.; Abdel-Rahmar, O. Abiraterone acetate/androgen deprivation therapy combination versus docetaxel/androgen deprivation therapy combination in advanced hormone-sensitive prostate cancer: A network meta-analysis on safety and efficacy. Curr. Med. Res. Opin. 2018, 34, 903–910. [Google Scholar] [CrossRef]
- Song, P.; Huang, C.; Wang, Y. The efficacy and safety comparison of docetaxel, cabazitaxel, estramustine, and mitoxantrone for castration-resistant prostate cancer: A network meta-analysis. Int. J. Surg. 2018, 56, 133–140. [Google Scholar] [CrossRef]
- Sun, G.; Zhang, X.; Chen, J.; Liao, B.; Liu, Z.; Zhao, J.; Gao, A.C.; Yang, Y.; Shu, K.; Liu, J.; et al. What kind of patients with castration-naive prostate cancer can benefit from upfront docetaxel and abiraterone: A systematic review and a network meta-analysis. Urol. Oncol. 2018, 36, 505–517. [Google Scholar] [CrossRef]
- Tan, P.S.; Aguiar, P., Jr.; Haaland, B.; Lopes, G. Addition of abiraterone, docetaxel, bisphosphonate, celecoxib or combinations to androgen-deprivation therapy (ADT) for metastatic hormone-sensitive prostate cancer (mHSPC): A network meta-analysis. Prostate Cancer Prostatic Dis. 2018, 21, 516–523. [Google Scholar] [CrossRef]
- Vale, C.L.; Fisher, D.J.; White, I.R.; Carpenter, J.R.; Burdett, S.; Clarke, N.W.; Fizazi, K.; Gravis, G.; James, N.D.; Mason, J.D.; et al. What is the optimal systemic treatment of men with metastatic, hormone-naive prostate cancer? A STOPCAP systematic review and network meta-analysis. Ann. Oncol. 2018, 29, 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- Wallis, C.J.D.; Klaassen, Z.; Bhindi, B.; Goldberg, H.; Chandrasekar, T.; Farrell, A.M.; Boorjian, S.A.; Kulkarni, G.S.; Karnes, R.J.; Satkunasivam, R. Comparison of abiraterone acetate and docetaxel with androgen deprivation therapy in high-risk and metastatic hormone-naive prostate cancer: A systematic review and network meta-analysis. Eur. Urol. 2018, 73, 834–844. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Huang, H.; Chen, C.; Liu, H.; Liu, H.; Su, F.; Bi, S.; Lam, T.B.; Li, J.; Lin, T.; et al. Efficacy and safety of different interventions in castration resistant prostate cancer progressing after docetaxel-based chemotherapy: Bayesian network analysis of randomized controlled trials. J. Cancer 2018, 9, 690–701. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Ni, Y.; Sun, G.; Liao, B.; Zhang, X.; Zhao, J.; Zhu, S.; Wang, Z.; Shen, P.; Zeng, P. Comparison of current systemic combination therapies for metastatic hormone-sensitive prostate cancer and selection of candidates for pptimal treatment: A systematic review and Bayesian network meta-analysis. Front. Oncol. 2020, 10, 519388. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, S.; Oudard, S.; Uemura, H.; Joniau, S.; Pilon, D.; Lefevbre, P.; McQuarrie, K.; Lio, J.; Dearden, L.; Sermon, J.; et al. Matching-adjusted indirect comparison of the efficacy of apalutamide and enzalutamide with ADT in the treatment of non-metastatic castration-resistant prostate cancer. Adv. Ther. 2020, 37, 501–511. [Google Scholar] [CrossRef]
- Hird, A.E.; Magee, D.E.; Bhindi, B.; Ye, X.Y.; Chandrasekar, T.; Goldberg, H.; Kloz, L.; Fleshner, N.; Satkunasivam, R.; Klaassen, R. A systematic review and network meta-analysis of novel androgen receptor inhibitors in non-metastatic castration-resistant prostate cancer. Clin. Genitourin. Cancer 2020, 18, 343–350. [Google Scholar] [CrossRef]
- Kumar, J.; Jazayeri, S.B.; Gautam, S.; Norez, D.; Alam, M.U.; Tanneru, K.; Bazargani, S.; Costa, J.; Bandyk, M.; Ganapathi, H.P.; et al. Comparative efficacy of apalutamide darolutamide and enzalutamide for treatment of non-metastatic castrate-resistant prostate cancer: A systematic review and network meta-analysis. Urol. Oncol. 2020, 38, 826–834. [Google Scholar] [CrossRef]
- Liu, Z.; Zhang, T.; Ma, Z.; Zheng, S.; Chen, J.; Wu, Z.; Zheng, X.; Liu, Z. Systemic management for nonmetastatic castration-resistant prostate cancer: A systematic review and network meta-analysis. Am. J. Clin. Oncol. 2020, 43, 288–297. [Google Scholar] [CrossRef]
- Marchioni, M.; Di Nicola, M.; Primiceri, G.; Novara, G.; Castellan, P.; Paul, A.K.; Veccia, A.; Autorino, R.; Cindolo, L. New antiandrogen compounds compared to docetaxel for metastatic hormone sensitive prostate cancer: Results from a network meta-analysis. J. Urol. 2020, 203, 751–759. [Google Scholar] [CrossRef]
- Mori, K.; Mostafaei, H.; Pradere, B.; Motlagh, R.S.; Quhal, F.; Laukhtina, E.; Schuetfort, V.M.; Abufaraj, M.; Karakiewicz, P.I.; Kimura, T.; et al. Apalutamide, enzalutamide, and darolutamide for non-metastatic castration-resistant prostate cancer: A systematic review and network meta-analysis. Int. J. Clin. Oncol. 2020, 25, 1892–1900. [Google Scholar] [CrossRef]
- Wang, L.; Paller, C.J.; Hong, H.; De Felice, A.; Alexander, G.C.; Brawley, O. Comparison of systemic treatments for metastatic castration-sensitive prostate cancer: A systematic review and network meta-analysis. JAMA Oncol. 2021, 7, 412–420. [Google Scholar] [CrossRef]
- Alberts, I.L.; Seide, S.E.; Mingels, C.; Bohn, K.P.; Shi, K.; Zacho, H.D.; Rominger, A.; Afshar-Oromieh, A. Comparing the diagnostic performance of radiotracers in recurrent prostate cancer: A systematic review and network meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2978–2989. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, M.; Wurnschimmel, C.; Nocera, L.M.; Colla Ruvolo, C.; Tian, Z.; Shariat, S.F.; Saad, F.; Tilki, D.; Graefen, M.; Kluth, L.A.; et al. Overall survival after systemic treatment in high-volume versus low-volume metastatic hormone-sensitive prostate cancer: Systematic review and network meta-analysis. Eur. Urol. Focus 2021. [Google Scholar] [CrossRef]
- Zhang, Q.; Cheng, H.; Wang, Y.; Tian, Y.; Xia, J.; Wang, Y.; Gu, M.; Song, M. Different therapeutic regimens in the treatment of metastatic prostate cancer by performing a Bayesian network meta-analysis. Int. J. Surg. 2019, 66, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, H.; Shen, W.; He, P.; Zhou, Z. Effectiveness and tolerability of targeted drugs for the treatment of metastatic castration-resistant prostate cancer: A network meta-analysis of randomized controlled trials. J. Cancer Res. Clin. Oncol. 2018, 144, 1751–1768. [Google Scholar] [CrossRef]
- Miyawaki, M.; Naoki, K.; Yoda, S.; Nakayama, S.; Satomi, R.; Sato, T.; Ikemura, S.; Ohgino, K.; Ishioka, K.; Arai, D.; et al. Erlotinib as second- or third-line treatment in elderly patients with advanced non-small cell lung cancer: Keio Lung Oncology Group Study 001 (KLOG001). Mol. Clin. Oncol. 2017, 6, 409–414. [Google Scholar] [CrossRef]
- Gennatas, C.; Michalaki, V.; Carvounis, E.; Psychogios, J.; Poulakaki, N.; Katsiamis, G.; Voros, D.; Kouloulias, V.; Mouratidou, D.; Isavaris, N. Third-line hormonal treatment with exemestane in postmenopausal patients with advanced breast cancer progressing on letrozole or anastrozole. A phase II trial conducted by the Hellenic Group of Oncology (HELGO). Tumori J. 2006, 92, 13–17. [Google Scholar] [CrossRef]
- Rondeau, V.; Cornet, E.; Moreau, P.; Troussard, X. Prediction of patients with multiple myeloma eligible for second- or third-line treatment in France. Ann. Hematol. 2016, 95, 1307–1313. [Google Scholar] [CrossRef]
- Feuerecker, B.; Tauber, R.; Knorr, K.; Heck, M.; Beheshti, A.; Seidl, C.; Bruchertseifer, F.; Pickhard, A.; Gafita, A.; Kratochwil, C.; et al. Activity and adverse events of actinium-225-PSMA-617 in advanced metastatic castration-resistant prostate cancer after failure of Lutetium-177-PSMA. Eur. Urol. 2021, 79, 343–350. [Google Scholar] [CrossRef]
- de Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for metastatic castration-resistant prostate cancer. N. Engl. J. Med. 2020, 382, 2091–2102. [Google Scholar] [CrossRef]
- Hussain, M.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Survival with olaparib in metastatic castration-resistant prostate cancer. N. Engl. J. Med. 2020, 383, 2345–2357. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | IXA | IXA | TRO | TRO | PROS | PROS | AFFI | AFFI | CARD | CARD | Ther | Ther | VISI | VISI |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Treat | MIT | IXA | MIT | C25 | C25 | C20 | C25 | C25+C | C25 | ABI | C20 | PRL | BSC | PRL |
| Pts | 41 | 41 | 377 | 378 | 602 | 598 | 318 | 317 | 129 | 126 | 101 | 99 | 280 | 551 |
| Age | 69 | 67 | 67 | 68 | 68 | 68 | 68 | 68 | 70 | 71 | 72 | 72 | 72 | 71 |
| RP | 15 | 16 | 205 | 198 | 264 | 272 | NR | NR | NR | NR | NR | NR | 82 | 159 |
| EBRT | 7 | 10 | 222 | 232 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| ADT | 41 | 41 | 375 | 375 | 594 | 583 | NR | NR | 128 | 126 | NR | NR | 280 | 551 |
| ABI | NR | NR | NR | NR | 165 | 158 | NR | NR | 128 | 126 | 91 | 91 | 280 | 551 |
| DOCE | 41 | 41 | 377 | 378 | 601 | 584 | 318 | 317 | 129 | 126 | NR | NR | 280 | 551 |
| PS0-1 | 28 | 28 | 344 | 350 | 540 | 539 | NR | NR | 123 | 119 | 96 | 95 | 258 | 510 |
| Visc | NR | NR | 94 | 94 | 186 | 187 | 115 | 108 | 21 | 25 | 13 | 7 | 66 | 112 |
| Liver | NR | NR | NR | NR | 90 | 94 | NR | NR | NR | NR | NR | NR | 12 | 47 |
| PSA | 141 | 137 | 128 | 144 | 172 | 160 | NR | NR | 62 | 61 | 110 | 94 | 91 | 91 |
| F-up | NR | NR | 13 | 13 | NR | NR | 30 | 30 | 9 | 9 | 18 | 18 | 21 | 21 |
| L4 | 30 | 16 | NR | NR | NR | NR | NR | NR | 30 | 42 | NR | NR | 221 | 301 |
| Study | IXA | IXA | TROP | TROP | PROS | PROS | AFFI | AFFI | CARD | CARD | Ther | Ther | VISI | VISI |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Treat | MIT | IXA | MIT | C25 | C25 | C20 | C25 | C25+C | C25 | ABI | C20 | PRLT | BSC | PRLT |
| PSA | 20 | 17 | 18 | 39 | 43 | 31 | NR | NR | 36 | 14 | 37 | 66 | 7 | 46 |
| rPFS | NR | NR | 1 | 3 | 9 | 9 | NR | NR | 4 | 3 | 5 | 5 | 3 | 9 |
| OS | 10 | 10 | 13 | 15 | 15 | 13 | 13 | 14 | 14 | 11 | NR | NR | 11 | 15 |
| Treatment | IXA | MITO | ABI/ENZA | CABA20 | CABA25 | PRLT | BSC |
|---|---|---|---|---|---|---|---|
| Best treatment | 0.1 | 0.0 | 0.0 | 0.0 | 2.3 | 97.6 | 0.0 |
| Worst treatment | 0.0 | 0.0 | 59.1 | 0.0 | 0.0 | 0.0 | 33.1 |
| Treatment | CABA20 | PRLT | BSC |
|---|---|---|---|
| Best treatment | 18.5 | 81.5 | 0.0 |
| Worst treatment | 0.0 | 0.0 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
von Eyben, F.E.; Kairemo, K.; Paller, C.; Hoffmann, M.A.; Paganelli, G.; Virgolini, I.; Roviello, G. 177Lu-PSMA Radioligand Therapy Is Favorable as Third-Line Treatment of Patients with Metastatic Castration-Resistant Prostate Cancer. A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Biomedicines 2021, 9, 1042. https://doi.org/10.3390/biomedicines9081042
von Eyben FE, Kairemo K, Paller C, Hoffmann MA, Paganelli G, Virgolini I, Roviello G. 177Lu-PSMA Radioligand Therapy Is Favorable as Third-Line Treatment of Patients with Metastatic Castration-Resistant Prostate Cancer. A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Biomedicines. 2021; 9(8):1042. https://doi.org/10.3390/biomedicines9081042
Chicago/Turabian Stylevon Eyben, Finn E., Kalevi Kairemo, Channing Paller, Manuela Andrea Hoffmann, Giovanni Paganelli, Irene Virgolini, and Giandomenico Roviello. 2021. "177Lu-PSMA Radioligand Therapy Is Favorable as Third-Line Treatment of Patients with Metastatic Castration-Resistant Prostate Cancer. A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials" Biomedicines 9, no. 8: 1042. https://doi.org/10.3390/biomedicines9081042
APA Stylevon Eyben, F. E., Kairemo, K., Paller, C., Hoffmann, M. A., Paganelli, G., Virgolini, I., & Roviello, G. (2021). 177Lu-PSMA Radioligand Therapy Is Favorable as Third-Line Treatment of Patients with Metastatic Castration-Resistant Prostate Cancer. A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Biomedicines, 9(8), 1042. https://doi.org/10.3390/biomedicines9081042