
Kinetics of Bilirubin and Ammonia Elimination during Hemadsorption Therapy in Secondary Sclerosing Cholangitis Following ECMO Therapy and Severe COVID-19


 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
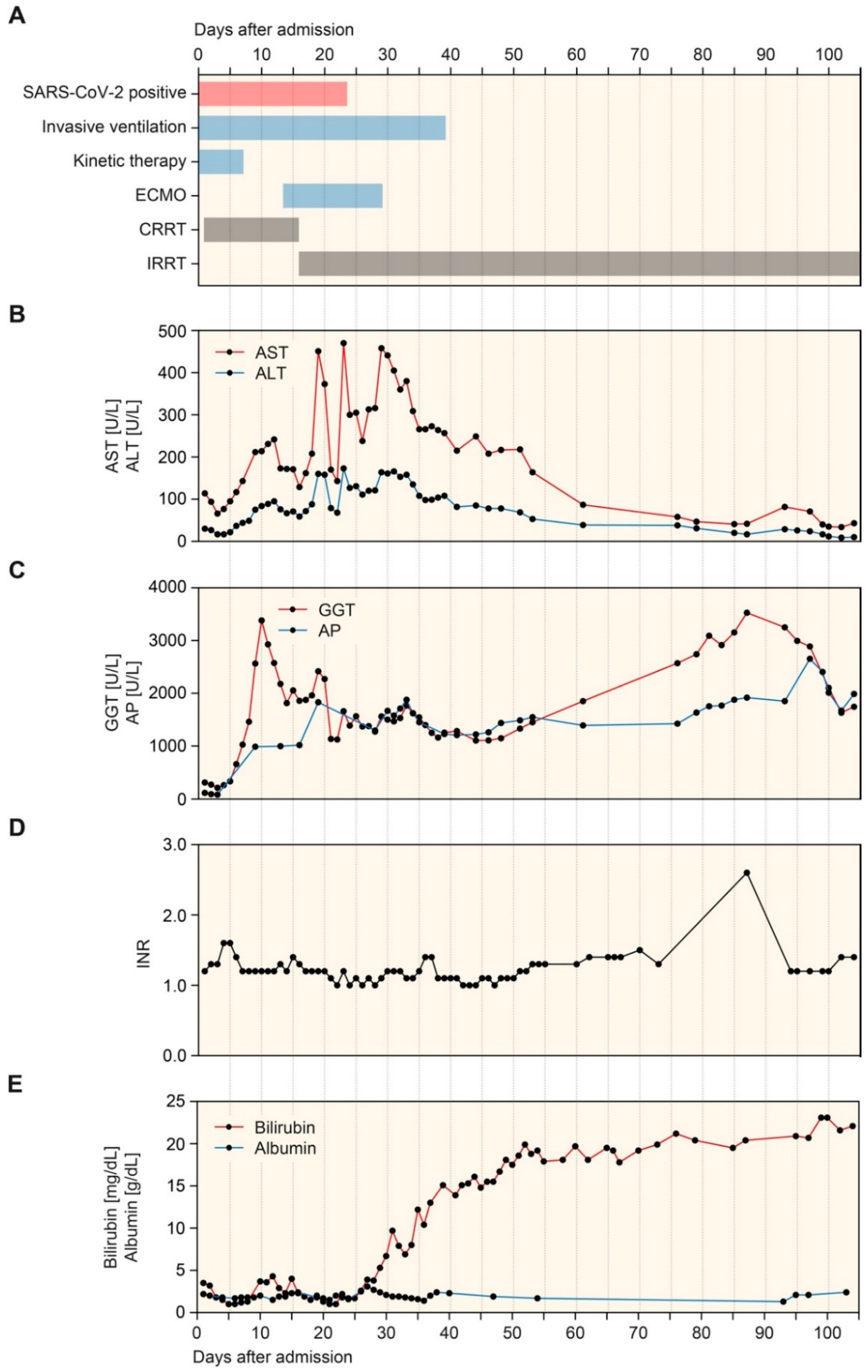
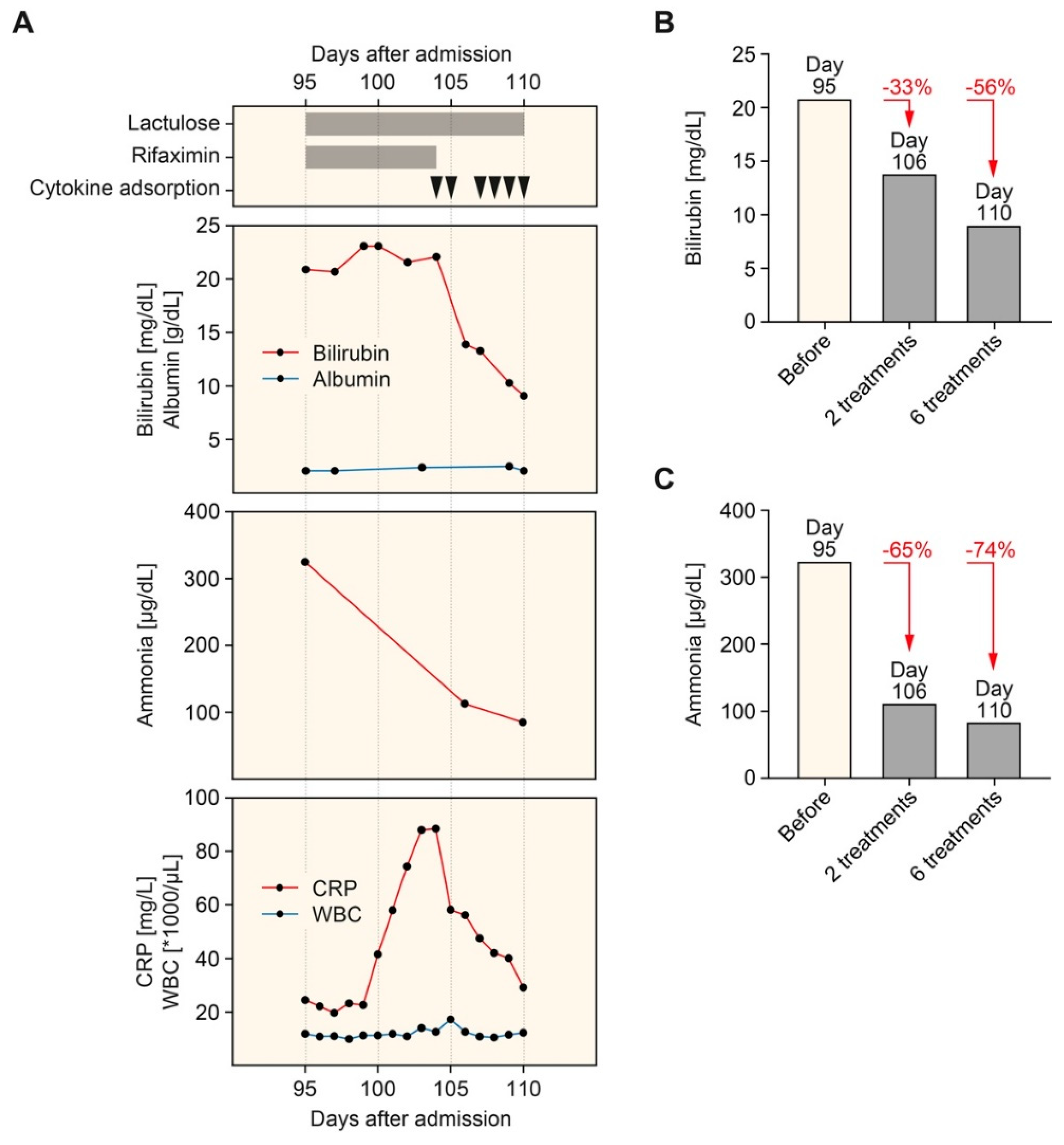
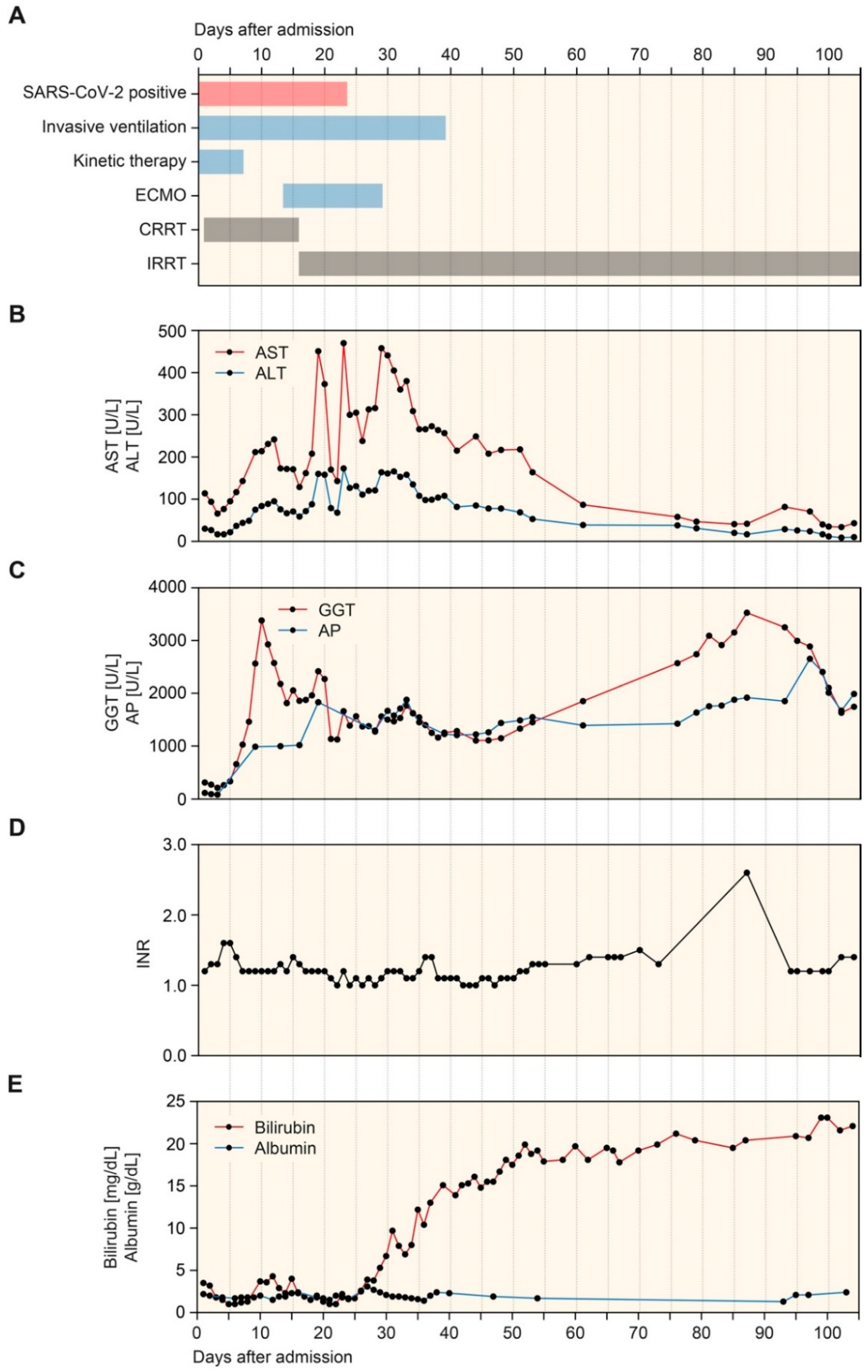
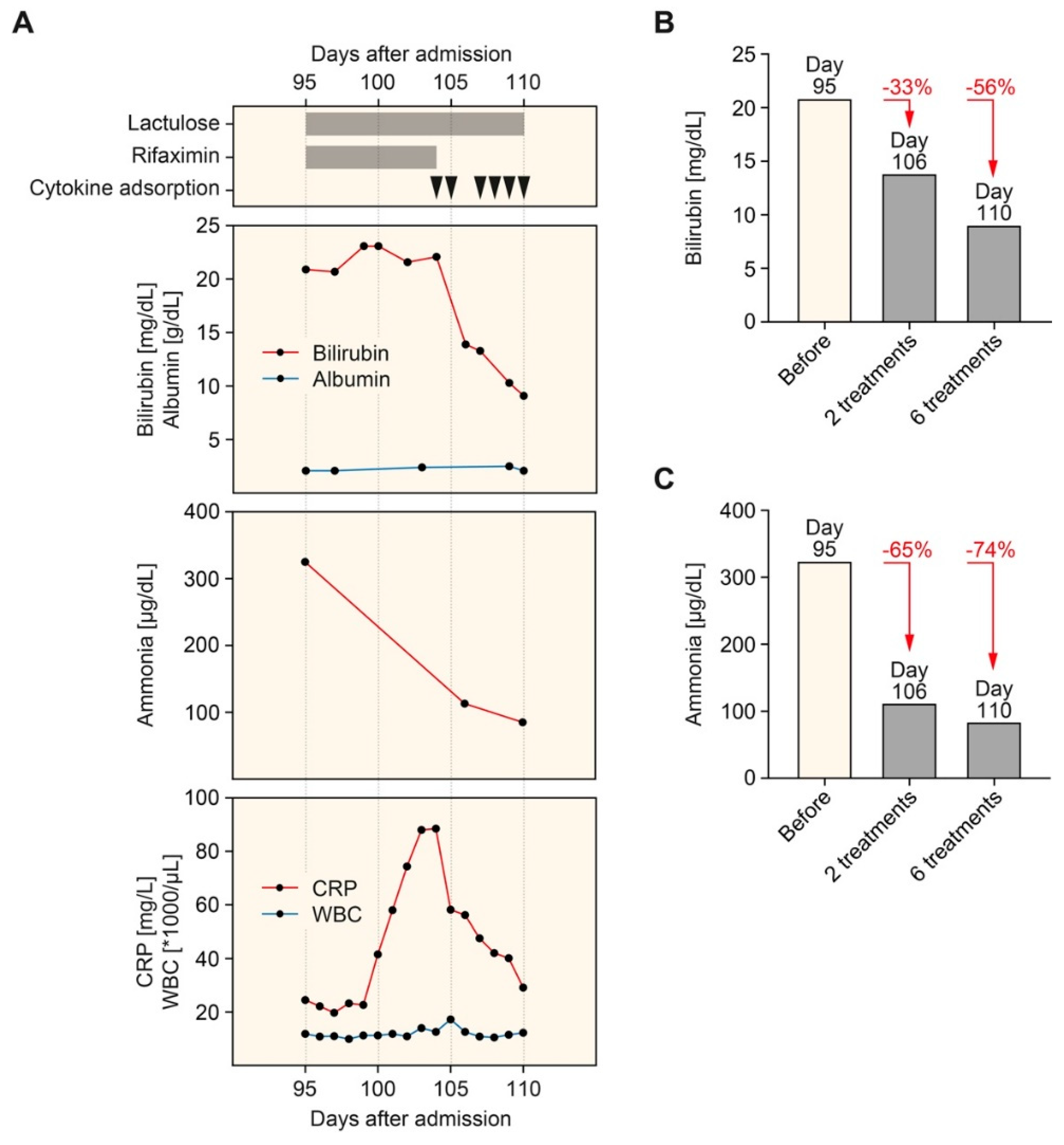
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Reuben, A.; Tillman, H.; Fontana, R.J.; Davern, T.; McGuire, B.; Stravitz, R.T.; Durkalski, V.; Larson, A.M.; Liou, I.; Fix, O.; et al. Outcomes in adults with acute liver failure between 1998 and 2013: An observational cohort study. Ann. Intern. Med. 2016, 164, 724–732. [Google Scholar] [CrossRef]
- Huang, H.; Li, H.; Chen, S.; Zhou, X.; Dai, X.; Wu, J.; Zhang, J.; Shao, L.; Yan, R.; Wang, M.; et al. Prevalence and characteristics of hypoxic hepatitis in COVID-19 patients in the intensive care unit: A first retrospective study. Front. Med. 2020, 7, 607206. [Google Scholar] [CrossRef]
- Stravitz, R.T.; Lee, W.M. Acute liver failure. Lancet 2019, 394, 869–881. [Google Scholar] [CrossRef]
- Real, M.; Barnhill, M.S.; Higley, C.; Rosenberg, J.; Lewis, J.H. Drug-induced liver injury: Highlights of the recent literature. Drug Saf. 2019, 42, 365–387. [Google Scholar] [CrossRef]
- Horvatits, T.; Trauner, M.; Fuhrmann, V. Hypoxic liver injury and cholestasis in critically ill patients. Curr. Opin. Crit. Care. 2013, 19, 128–132. [Google Scholar] [CrossRef]
- Lelubre, C.; Vincent, J.L. Mechanisms and treatment of organ failure in sepsis. Nat. Rev. Nephrol. 2018, 14, 417–427. [Google Scholar] [CrossRef]
- Tunney, R.; Scott, J.; Rudralingam, V.; Liong, S.; Athwal, V.S. Secondary sclerosing cholangitis following extracorporeal membrane oxygenation for acute respiratory distress in polytrauma. Clin. Case Rep. 2018, 6, 1849–1853. [Google Scholar] [CrossRef] [Green Version]
- Vitek, L.; Hubacek, J.A.; Pajak, A.; Dorynska, A.; Kozela, M.; Eremiasova, L.; Danzig, V.; Stefler, D.; Bobak, M. Association between plasma bilirubin and mortality. Ann. Hepatol. 2019, 18, 379–385. [Google Scholar] [CrossRef]
- Kramer, L.; Jordan, B.; Druml, W.; Bauer, P.; Metnitz, P.G. Austrian epidemiologic study on intensive care ASG. Incidence and prognosis of early hepatic dysfunction in critically ill patients—A prospective multicenter study. Crit. Care Med. 2007, 35, 1099–1104. [Google Scholar] [CrossRef]
- Kerbert, A.J.; Engelmann, C.; Jalan, R. Neurocritical care management of hepatic encephalopathy and coma in liver failure. Semin. Respir. Crit. Care Med. 2018, 39, 523–537. [Google Scholar] [CrossRef]
- Olivo, R.; Guarrera, J.V.; Pyrsopoulos, N.T. Liver transplantation for acute liver failure. Clin. Liver Dis. 2018, 22, 409–417. [Google Scholar] [CrossRef]
- Khan, R.; Koppe, S. Modern management of acute liver failure. Gastroenterol. Clin. North Am. 2018, 47, 313–326. [Google Scholar] [CrossRef]
- Alshamsi, F.; Alshammari, K.; Belley-Cote, E.; Dionne, J.; Albrahim, T.; Albudoor, B.; Ismail, M.; Al-judaibi, B.; Baw, B.; Subramanian, R.M.; et al. Extracorporeal liver support in patients with liver failure: A systematic review and meta-analysis of randomized trials. Intensive Care Med. 2020, 46, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Larsen, F.S.; Schmidt, L.E.; Bernsmeier, C.; Rasmussen, A.; Isoniemi, H.; Patel, V.C.; Triantafyllou, E.; Bernal, W.; Auzinger, G.; Shawcross, D.; et al. High-volume plasma exchange in patients with acute liver failure: An open randomised controlled trial. J. Hepatol. 2016, 64, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Qian, Y.; Tan, D.; Mo, D.; Li, X. Therapeutic plasma exchange: A prospective randomized trial to evaluate 2 strategies in patients with liver failure. Transfus. Apher. Sci. 2018, 57, 253–258. [Google Scholar] [CrossRef] [Green Version]
- Stahl, K.; Hadem, J.; Schneider, A.; Manns, M.P.; Wiesner, O.; Schmidt, B.M.W.; Hoeper, M.M.; Busch, M.; David, S. Therapeutic plasma exchange in acute liver failure. J. Clin. Apher. 2019, 34, 589–597. [Google Scholar] [CrossRef] [Green Version]
- Stahl, K.; Busch, M.; Fuge, J.; Schneider, A.; Manns, M.P.; Seeliger, B.; Schmidt, J.J.; Wiesner, O.; Schmidt, B.M.W.; Taubert, R.; et al. Therapeutic plasma exchange in acute on chronic liver failure. J. Clin. Apher. 2020, 35, 316–327. [Google Scholar] [CrossRef]
- Tsipotis, E.; Shuja, A.; Jaber, B.L. Albumin dialysis for liver failure: A systematic review. Adv. Chronic Kidney Dis. 2015, 22, 382–390. [Google Scholar] [CrossRef]
- Falkensteiner, C.; Kortgen, A.; Leonhardt, J.; Bauer, M.; Sponholz, C. Comparison of albumin dialysis devices molecular adsorbent recirculating system and advanced organ support system in critically ill patients with liver failure—A retrospective analysis. Ther. Apher. Dial. 2021, 25, 225–236. [Google Scholar] [CrossRef]
- Fuhrmann, V.; Perez Ruiz de Garibay, A.; Faltlhauser, A.; Tyczynski, B.; Jarczak, D.; Lutz, J.; Weinamnn-Menke, J.; Kribben, A.; Kluge, S. Registry on extracorporeal multiple organ support with the advanced organ support (ADVOS) system: 2-year interim analysis. Medicine 2021, 100, e24653. [Google Scholar] [CrossRef]
- Fuhrmann, V.; Weber, T.; Roedl, K.; Motaabbed, J.; Tariparast, A.; Jarczak, D.; Perez Ruiz de Garibay, A.; Kluwe, J.; Boenisch, O.; Herkner, H.; et al. Advanced organ support (ADVOS) in the critically ill: First clinical experience in patients with multiple organ failure. Ann. Intensive Care 2020, 10, 96. [Google Scholar] [CrossRef]
- Huber, W.; Henschel, B.; Schmid, R.; Al-Chalabi, A. First clinical experience in 14 patients treated with ADVOS: A study on feasibility, safety and efficacy of a new type of albumin dialysis. BMC Gastroenterol. 2017, 17, 32. [Google Scholar] [CrossRef] [Green Version]
- Acar, U.; Gokkaya, Z.; Akbulut, A.; Ferah, O.; Yenidunya, O.; Acik, M.E.; Tokat, Y.; Yentür, E. Impact of cytokine adsorption treatment in liver failure. Transplant. Proc. 2019, 51, 2420–2424. [Google Scholar] [CrossRef]
- Dhokia, V.D.; Madhavan, D.; Austin, A.; Morris, C.G. Novel use of CytoSorb haemadsorption to provide biochemical control in liver impairment. J. Intensive Care Soc. 2019, 20, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Piwowarczyk, P.; Kutnik, P.; Potrec-Studzinska, B.; Sysiak-Slawecka, J.; Rypulak, E.; Borys, M.; Czczuwar, M. Hemoadsorption in isolated conjugated hyperbilirubinemia after extracorporeal membrane oxygenation support. Cholestasis of sepsis: A case report and review of the literature on differential causes of jaundice in ICU patient. Int. J. Artif. Organs. 2019, 42, 263–268. [Google Scholar] [CrossRef]
- Calabro, M.G.; Febres, D.; Recca, G.; Lembo, R.; Fominskiy, E.; Scandroglio, A.M.; Zangrillo, A.; Pappalardo, F. Blood purification with CytoSorb in critically ill patients: Single-center preliminary experience. Artif. Organs. 2019, 43, 189–194. [Google Scholar] [CrossRef]
- Brooling, J.; Leal, R. Secondary sclerosing cholangitis: A review of recent literature. Curr. Gastroenterol. Rep. 2017, 19, 44. [Google Scholar] [CrossRef]
- Visentin, M.; Lenggenhager, D.; Gai, Z.; Kullak-Ublick, G.A. Drug-induced bile duct injury. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 1498–1506. [Google Scholar] [CrossRef] [PubMed]
- Lo, R.S.; Krishnamoorthy, R.; Freeman, J.G.; Austin, A.S. Cholestasis and biliary dilatation associated with chronic ketamine abuse: A case series. Singapore Med. J. 2011, 52, e52–e55. [Google Scholar] [PubMed]
- Wakim-Fleming, J. Hepatic encephalopathy: Suspect it early in patients with cirrhosis. Cleve Clin. J. Med. 2011, 78, 597–605. [Google Scholar] [CrossRef] [Green Version]
- Bernal, W.; Wendon, J. Acute liver failure. N. Engl. J Med. 2013, 369, 2525–2534. [Google Scholar] [CrossRef] [PubMed]
- Bernal, W.; Lee, W.M.; Wendon, J.; Larsen, F.S.; Williams, R. Acute liver failure: A curable disease by 2024? J. Hepatol. 2015, 62 (Suppl. S1), S112–S120. [Google Scholar] [CrossRef] [Green Version]
- Slack, A.J.; Auzinger, G.; Willars, C.; Dew, T.; Musto, R.; Corsilli, D.; Sherwood, R.; Wendon, J.A.; Bernal, W. Ammonia clearance with haemofiltration in adults with liver disease. Liver Int. 2014, 34, 42–48. [Google Scholar] [CrossRef]
- Cardoso, F.S.; Gottfried, M.; Tujios, S.; Olson, J.C.; Karvellas, C.J.; Group USALFS. Continuous renal replacement therapy is associated with reduced serum ammonia levels and mortality in acute liver failure. Hepatology 2018, 67, 711–720. [Google Scholar] [CrossRef] [Green Version]
- Boer, D.P.; Mourik, S.L.; van den Hoogen, M.W.F.; Langendonk, J.G.; de Geus, H.R.H. Successful treatment of severe hyperammonaemia with ultra-high dose continuous veno-venous haemodiafiltration. Blood Purif. 2019, 48, 283–285. [Google Scholar] [CrossRef]
- Mikhalovsky, S.V. Emerging technologies in extracorporeal treatment: Focus on adsorption. Perfusion 2003, 18 (Suppl. S1), 47–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, C.; Linsberger, I.; Rafiee-Tehrani, M.; Falkenhagen, D. Permeability and adsorption capacity of dialysis membranes to lipid A. Int. J. Artif. Organs. 1997, 20, 144–152. [Google Scholar] [CrossRef]
- Gemelli, C.; Cuoghi, A.; Magnani, S.; Atti, M.; Ricci, D.; Siniscalchi, A.; Mancini, E.; Faenza, S. Removal of Bilirubin with a new adsorbent system: In vitro kinetics. Blood Purif. 2019, 47, 10–15. [Google Scholar] [CrossRef]
- Dominik, A.; Stange, J. Similarities, differences, and potential synergies in the mechanism of action of albumin dialysis using the MARS albumin dialysis device and the CytoSorb hemoperfusion device in the treatment of liver failure. Blood Purif. 2021, 50, 119–128. [Google Scholar] [CrossRef]
- Niewinski, G.; Raszeja-Wyszomirska, J.; Hrenczuk, M.; Rozga, A.; Malkowski, P.; Rozga, J. Intermittent high-flux albumin dialysis with continuous venovenous hemodialysis for acute-on-chronic liver failure and acute kidney injury. Artif. Organs. 2020, 44, 91–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerth, H.U.; Pohlen, M.; Tholking, G.; Pavenstadt, H.; Brand, M.; Wilms, C.; Hüsing-Kabar, A.; Görlich, D.; Kabar, I.; Schmidt, H.H.J. Molecular adsorbent recirculating system (MARS) in acute liver injury and graft dysfunction: Results from a case-control study. PLoS ONE 2017, 12, e0175529. [Google Scholar] [CrossRef] [Green Version]
- Gruda, M.C.; Ruggeberg, K.G.; O’Sullivan, P.; Guliashvili, T.; Scheirer, A.R.; Golobish, T.D.; Capponi, V.J.; Chan, P.P. Broad adsorption of sepsis-related PAMP and DAMP molecules, mycotoxins, and cytokines from whole blood using CytoSorb(R) sorbent porous polymer beads. PLoS ONE 2018, 13, e0191676. [Google Scholar] [CrossRef]
- Monneret, G.; Finck, M.E.; Venet, F.; Debard, A.L.; Bohe, J.; Bienvenu, J.; Lepape, A. The anti-inflammatory response dominates after septic shock: Association of low monocyte HLA-DR expression and high interleukin-10 concentration. Immunol. Lett. 2004, 95, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Frencken, J.F.; van Vught, L.A.; Peelen, L.M.; Ong, D.S.Y.; Klein Klouwenberg, P.M.C.; Horn, J.; Bonten, M.J.M.; van der Poll, T.; Cremer, O.L. An unbalanced inflammatory cytokine response is not associated with mortality following sepsis: A prospective cohort study. Crit. Care Med. 2017, 45, e493–e499. [Google Scholar] [CrossRef] [PubMed]
- De Vriese, A.S.; Colardyn, F.A.; Philippe, J.J.; Vanholder, R.C.; De Sutter, J.H.; Lameire, N.H. Cytokine removal during continuous hemofiltration in septic patients. J. Am. Soc. Nephrol. 1999, 10, 846–853. [Google Scholar] [CrossRef] [PubMed]
- Lukaszewicz, A.C.; Payen, D. Purification methods: A way to treat severe acute inflammation related to sepsis? Crit. Care. 2013, 17, 159. [Google Scholar] [CrossRef] [Green Version]
- Cole, L.; Bellomo, R.; Journois, D.; Davenport, P.; Baldwin, I.; Tipping, P. High-volume haemofiltration in human septic shock. Intensive Care Med. 2001, 27, 978–986. [Google Scholar] [CrossRef] [PubMed]
- Honore, P.M.; Jamez, J.; Wauthier, M.; Lee, P.A.; Dugernier, T.; Pirenne, B.; Hanique, G.; Matson, J.R. Prospective evaluation of short-term, high-volume isovolemic hemofiltration on the hemodynamic course and outcome in patients with intractable circulatory failure resulting from septic shock. Crit. Care Med. 2000, 28, 3581–3587. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Song, M.; Venkataraman, R. Hemoadsorption removes tumor necrosis factor, interleukin-6, and interleukin-10, reduces nuclear factor-kappaB DNA binding, and improves short-term survival in lethal endotoxemia. Crit. Care Med. 2004, 32, 801–805. [Google Scholar] [CrossRef]
- Namas, R.A.; Namas, R.; Lagoa, C.; Barclay, D.; Mi, Q.; Zamora, R.; Peng, Z.; Wen, X.; Fedorchak, M.V.; Valenti, I.E.; et al. Hemoadsorption reprograms inflammation in experimental gram-negative septic peritonitis: Insights from in vivo and in silico studies. Mol. Med. 2012, 18, 1366–1374. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.Y.; Carter, M.J.; Kellum, J.A. Effects of hemoadsorption on cytokine removal and short-term survival in septic rats. Crit. Care Med. 2008, 36, 1573–1577. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.Y.; Wang, H.Z.; Carter, M.J.; Dileo, M.V.; Bishop, J.V.; Zhou, F.H.; Wen, X.-Y.; Rimmelé, T.; Singbartl, K.; Federspiel, W.J.; et al. Acute removal of common sepsis mediators does not explain the effects of extracorporeal blood purification in experimental sepsis. Kidney Int. 2012, 81, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Akil, A.; Ziegeler, S.; Reichelt, J.; Rehers, S.; Abdalla, O.; Semik, M.; Fischer, S. Combined use of CytoSorb and ECMO in patients with severe pneumogenic sepsis. Thorac. Cardiovasc. Surg. 2021, 69, 246–251. [Google Scholar] [CrossRef]
- Singh, A.; Mehta, Y.; Trehan, N. Bilirubin removal using CytoSorb filter in a cardiac surgical patient. J. Cardiothorac. Vasc. Anesth. 2019, 33, 881–883. [Google Scholar] [CrossRef] [Green Version]
- Scharf, C.; Liebchen, U.; Paal, M.; Becker-Pennrich, A.; Irlbeck, M.; Zoller, M.; Schroeder, I. Successful elimination of bilirubin in critically ill patients with acute liver dysfunction using a cytokine adsorber and albumin dialysis: A pilot study. Sci. Rep. 2021, 11, 10190. [Google Scholar] [CrossRef]
- Buttner, S.; Patyna, S.; Koch, B.; Finkelmeier, F.; Geiger, H.; Sarrazin, C.; Farnik, H. Application of hemoadsorption in a case of liver cirrhosis and alcohol-related steatohepatitis with preexisting hepatitis C infection. Blood Purif. 2017, 44, 30–31. [Google Scholar] [CrossRef]
- Leonhardt, S.; Veltzke-Schlieker, W.; Adler, A.; Schott, E.; Eurich, D.; Faber, W.; Neuhaus, P.; Seehofer, D. Secondary sclerosing cholangitis in critically ill patients: Clinical presentation, cholangiographic features, natural history, and outcome: A series of 16 cases. Medicine 2015, 94, e2188. [Google Scholar] [CrossRef] [PubMed]
- Meersseman, P.; Blondeel, J.; De Vlieger, G.; van der Merwe, S.; Monbaliu, D. Collaborators leuven liver transplant p. Secondary sclerosing cholangitis: An emerging complication in critically ill COVID-19 patients. Intensive Care Med. 2021, 47, 1037–1040. [Google Scholar] [CrossRef]
- Kaltschmidt, B.; Fitzek, A.D.E.; Schaedler, J.; Forster, C.; Kaltschmidt, C.; Hansen, T.; Steinfurth, F.; Windmöller, B.A.; Pilger, C.; Kong, C.; et al. Hepatic vasculopathy and regenerative responses of the liver in fatal Cases of COVID-19. Clin. Gastroenterol. Hepatol. 2021, 19, 1726–1729.e3. [Google Scholar] [CrossRef]
- Roedl, K.; Jarczak, D.; Drolz, A.; Wichmann, D.; Boenisch, O.; de Heer, G.; Burdelski, C.; Frings, D.; Sensen, B.; Nierhaus, A.; et al. Severe liver dysfunction complicating course of COVID-19 in the critically ill: Multifactorial cause or direct viral effect? Ann. Intensive Care 2021, 11, 44. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tampe, D.; Korsten, P.; Bremer, S.C.B.; Winkler, M.S.; Tampe, B. Kinetics of Bilirubin and Ammonia Elimination during Hemadsorption Therapy in Secondary Sclerosing Cholangitis Following ECMO Therapy and Severe COVID-19. Biomedicines 2021, 9, 1841. https://doi.org/10.3390/biomedicines9121841
Tampe D, Korsten P, Bremer SCB, Winkler MS, Tampe B. Kinetics of Bilirubin and Ammonia Elimination during Hemadsorption Therapy in Secondary Sclerosing Cholangitis Following ECMO Therapy and Severe COVID-19. Biomedicines. 2021; 9(12):1841. https://doi.org/10.3390/biomedicines9121841
Chicago/Turabian StyleTampe, Désirée, Peter Korsten, Sebastian C. B. Bremer, Martin S. Winkler, and Björn Tampe. 2021. "Kinetics of Bilirubin and Ammonia Elimination during Hemadsorption Therapy in Secondary Sclerosing Cholangitis Following ECMO Therapy and Severe COVID-19" Biomedicines 9, no. 12: 1841. https://doi.org/10.3390/biomedicines9121841
APA StyleTampe, D., Korsten, P., Bremer, S. C. B., Winkler, M. S., & Tampe, B. (2021). Kinetics of Bilirubin and Ammonia Elimination during Hemadsorption Therapy in Secondary Sclerosing Cholangitis Following ECMO Therapy and Severe COVID-19. Biomedicines, 9(12), 1841. https://doi.org/10.3390/biomedicines9121841