Abstract
Background: Chronic disease self-management (CDSM) programmes are widely recommended for heart failure with reduced ejection fraction (HFrEF), yet evidence on their effectiveness remains mixed. This systematic review synthesises the evidence and critically appraises the findings from multiple systematic reviews on CDSM for congestive heart failure (CHF) with a focus on the impact of nurse-led and multidisciplinary CDSM interventions in adults with HFrEF. Design: Systematic review using PRISMA 2020 and AMSTAR-2 guidelines. Data Sources and Eligibility: We searched MEDLINE, Embase, CINAHL, Cochrane Library, and other sources for reviews published from 2012 to 2024. Included were systematic reviews of CDSM interventions for adults diagnosed with HFrEF, focusing on mortality, hospital readmissions, quality of life, and self-management behaviours. Results: A total of 1050 studies were screened, with 60 studies being counted in the final analysis, including 22 reviews of high quality. Evidence for mortality benefit was limited and inconsistent across reviews. However, moderate-to-high-certainty evidence showed that nurse-led CDSM interventions improved hospital readmission rates and health-related quality of life (HRQoL). Improvements in self-management behaviours such as medication adherence and symptom monitoring were also frequently reported. Conclusions: While evidence for a mortality benefit remains inconclusive, this review highlights consistent benefits of nurse-led CDSM interventions in reducing readmissions and improving HRQoL for HFrEF patients. Future research should prioritise standardised outcome reporting, incorporate economic evaluations, and explore patient-centred and culturally tailored approaches to intervention design. PROSPERO registration number CRD42023431539.
1. Introduction
Chronic disease self-management (CDSM) programmes, a process by which individuals with long-term health conditions actively engage in managing their symptoms, treatment plans, physical and psychosocial consequences, and lifestyle adjustments [1], have been widely studied across a range of long-term conditions, including congestive heart failure (CHF). Yet, despite this extensive body of research, uncertainty remains regarding which models of CDSM—particularly in terms of delivery and workforce configuration—are most effective for improving outcomes in heart failure with reduced ejection fraction (HFrEF). There is growing recognition that previous systematic reviews, while valuable, often examine heterogeneous interventions or broad disease populations, making it difficult to draw specific conclusions about the comparative efficacy of nurse-led and multidisciplinary CDSM approaches in CHF care.
Decades of research underscore the need to consolidate and re-evaluate the evidence base to inform future patient-centred, outcome-driven strategies [1,2,3,4]. Synthesising existing systematic reviews through an umbrella review provides an opportunity to distil common findings, identify gaps, and clarify what models of CDSM offer the greatest benefit for individuals with HFrEF. This includes considering intervention complexity, adaptability to patient casemix, and implementation challenges in diverse real-world settings [1,2,3,4]. Programmes that are overly intricate—or, conversely, oversimplified—can hinder effective delivery and patient engagement, especially when not tailored to the nuanced needs of CHF populations.
While clinical management of CHF has advanced considerably, especially regarding pharmacological therapies, it remains a complex syndrome requiring sustained, multidisciplinary input and substantial healthcare resources. The public health burden continues to rise due to ageing populations and ongoing challenges in ensuring timely, equitable care—particularly in rural and remote areas. Hospital readmission and mortality rates remain high within 6 to 12 months of discharge, ranging from approximately 25% to 50%, with CHF care consuming 1–2% of healthcare budgets in high-income countries [4,5].
Alongside these clinical developments, non-pharmacological strategies have gained prominence. Landmark studies support the use of structured care models and adherence to performance metrics as a means to enhance uptake of guideline-directed therapy and improve clinical outcomes. However, significant disparities persist—particularly for socioeconomically disadvantaged populations—and health literacy remains a key determinant of self-management capacity. Comorbidities such as coronary artery disease, diabetes, hypertension, renal impairment, and substance use disorders affect over 50% of individuals with CHF, further complicating care delivery and the design of effective CDSM interventions [6].
Despite increasing interest in self-management, questions remain about the effectiveness and sustainability of different CDSM models in CHF care [4,7,8,9,10,11]. This umbrella review aims to synthesise findings from existing systematic reviews to better understand the impact of nurse-led and multidisciplinary CDSM interventions for adults with HFrEF. By focusing on delivery models, workforce roles, and implementation contexts, this review contributes new insights into how integrated, team-based approaches can be optimised to improve patient outcomes.
Aims
This umbrella systematic review pools systematic reviews for CHF utilising CDSM interventions in the management programme. This study complements an identification of historical gaps [9] and also seeks to identify effective CDSM strategies. Specific research questions are addressed, to gather evidence from systematic reviews on the efficacy of CDSM programme interventions compared to usual care on major adverse cardiovascular outcomes (MACE), HRQoL, and self-management behaviours in a CHF population, focusing on those with heart failure with reduced ejection fraction (HFrEF).
2. Methods
This umbrella systematic review followed a pre-published protocol [9,10] registered with PROSPERO (CRD42023431539) and adhered to PRISMA 2020 and AMSTAR 2 Statement [12,13,14,15,16,17,18,19,20,21]. The methodology encompassed five core steps: eligibility criteria, search strategy, data extraction, risk of bias assessment, and data analysis.
2.1. Eligibility Criteria
Study Types:
We included systematic reviews and meta-analyses that pooled data from controlled trials examining CDSM interventions in patients with HFrEF. Reviews that relied solely on observational studies were excluded to minimise risk of bias. No restrictions were placed on language or publication date (1980–2024). Grey literature and reference lists were also screened manually, and authors were contacted for unpublished data.
Participants:
Eligible studies enrolled adults (≥18 years) diagnosed with HFrEF (EF < 45%). Participants could have been recruited within 12 months of diagnosis or during admission for acute decompensated heart failure. Studies covering all aetiologies of CHF—such as ischaemic, viral, idiopathic, metabolic, and substance-related causes—were considered. Studies focused solely on HFpEF (EF > 50%) or without a clear description of the CDSM intervention were excluded. No restrictions were applied based on age, gender, or ethnicity.
Interventions:
Eligible interventions involved structured CDSM programmes implemented through a standardised disease management pathway. These included programmes designed to improve MACE and/or self-management behaviours. Health professionals involved ranged from primary care providers and specialists to allied health staff (e.g., nurses, pharmacists, and physiotherapists). Programmes often designated a case manager to coordinate care.
Comparators typically reflected standard guideline-based care in accordance with ACC/AHA and EHA recommendations. Core CDSM components included disease management, self-monitoring, care coordination, coaching, and tailored management strategies.
Types of Outcome Measures:
Primary Outcomes concluded on the level and quality of quantitative evidence for CDSM in CHF in reducing MACE. Secondary Outcomes include data on self-management behaviours.
2.2. Search Strategy
2.2.1. Study Characteristics
Systematic review and meta-analysis of clinical studies were included, and observational studies were limited. However, some pooled studies have a mixture of trial format, hence the need for grading of these reviews and for establishing the quality scale.
2.2.2. Electronic Search
A comprehensive search was conducted in EbscoHost, all databases, Medline, PubMed (1950–2022), the Cochrane Register of Controlled trials (CENTRAL) (2023), Embase (1980 to 2023), CINAHL (1982–2023), PsycINFO (1887–2023), Science Citation Index (1987–2023), and Web of Science. The MeSH terms used to shortlist studies were previously published [8,9]. In addition, a ‘snowball’ search of relevant selected reviews was conducted.
2.2.3. Searching Other Resources and Information Sources
This was conducted as the study evolved and as required. All new changes are documented as an amendment to the protocol.
2.3. Data Collection and Analysis
2.3.1. Study Selection
Title and abstract screening was conducted independently by two reviewers (P.I. and T.P.) to assess eligibility based on predefined inclusion criteria. Full texts of potentially relevant studies were then reviewed in detail, also independently and unblinded, by the same reviewers. Discrepancies during the selection process were discussed and resolved by consensus. A third reviewer (F.H.) acted as arbiter and reviewed all stages of the process, resolving any unresolved disagreements or uncertainties.
In some cases, study authors were contacted to clarify missing or unclear results. Where clarification could not be obtained, studies were excluded from the main analysis.
2.3.2. Data Extraction and Management
Data extraction was performed independently by two reviewers using a structured template developed specifically for this review. Key data fields included the following:
- Study quality and risk of bias;
- Review characteristics (e.g., number and type of included studies);
- Population and setting;
- CDSM intervention characteristics;
- Outcomes and findings relevant to CHF.
When results for a single study were reported across multiple publications, data were consolidated to ensure comprehensive representation.
2.3.3. Data Items
The data extraction template incorporated CHF-specific domains and outcome measures based on previous umbrella reviews and disease-specific guidance [6,7,8,9]. Domains included patient adherence, hospitalisation rates, mortality, quality of life, and implementation-related factors.
2.3.4. Quality Appraisal and Risk of Bias
Two reviewers (F.F. and T.P.) independently assessed the methodological quality of the included systematic reviews. The following tools were used:
- AMSTAR 2 for assessing the quality of systematic reviews [12];
- RoB 2.0, the revised Cochrane risk of bias tool, for included RCTs [14,15].
Discrepancies were resolved through discussion or consultation with a third reviewer.
2.3.5. Certainty of Evidence
The certainty of evidence for key outcomes was evaluated using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) framework. This assessment considered five domains:
- Risk of bias;
- Inconsistency;
- Indirectness;
- Imprecision;
- Publication bias.
Evidence was then categorised as very low, low, moderate, or high certainty [21].
Reporting of excluded studies is provided in the PRISMA figure. Information is also provided in the Results and Appendix.
2.3.6. Data Analysis, Assessment of Heterogeneity, and Publication Bias
- Planned methods for study analysis and statistical methodology
The searching process and data extraction was guided by Cochrane Handbook for Systematic Reviews of Interventions [15]. The initial step was summary of included findings in a table and qualitative analysis. Subgroup analyses were performed on key domains, e.g., various comorbid conditions, training of intervention arms, treatment intensity, and other unanticipated factors [10,11,12,13,14,15,16,17,18,19,20,21,22].
- Risk of bias in individual studies
We used the Cochrane Risk of Bias tool, with two reviewers, in pairs, to assess and rate risk of bias from standards defined in the Cochrane Collaboration’s tool [13,14,15,16,17].
2.4. Measures of Treatment Effect
The results are presented as a risk ratio with a 95% confidence interval (CI) to express estimates of effects for dichotomous variables and outcomes. For continuous variables, results are expressed as the mean difference with 95% CI. For outcomes measured using a variety of methods, the size of the intervention effect is presented as standardised mean difference with 95% CI.
2.5. Ethics and Dissemination
Ethical approval is not required for the study as no primary patient data are collected. This review will extract current and comprehensive research publications on CDSM and CHF. At this juncture, it is vital to inform the literature on the efficacy of CDSM within the CHF context. It is important to plan studies to counter the downgrade of evidence and inform future guidelines.
3. Results
Search Results
The summary of the search is highlighted in PRISMA chart (Figure 1). From a total 974 identified potentially eligible systematic reviews, 58 reports from 57 studies were included (Table 1 and Table 2). Studies were divided into three categories: case management (n = 10), nurse-led interventions (n = 8), and non-pharmacological interventions (n = 41). The total number of studies reported for each study is 1430 (range 6–105 articles); the cumulative population from each study is 276,381 (range 467 to 76,582 patients). This value does not factor overlap RCT’s in various SRs.
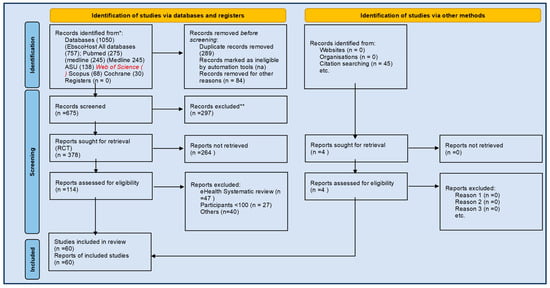
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews, which included searches of databases, registers, and other sources. * Search previously detailed from Refs. [9,10].

Table 1.
Summary (characteristics) of included studies.
Table 2.
Rating (classification) of intervention effectiveness for each outcome and intervention category.
The quality appraisal of studies was conducted as per the systematic protocol, using AMSTAR-2 grading [21,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84]. The mean quality assessment (QA) score was low to moderate 40/61 (66%). The study quality rated 22 high, 21 moderate, 17 low, and 1 very low. Several studies that had a partial yes response were included as high after a secondary review, and gaps were deemed not significant [28,31,32,50,67,68,73,74,81]. AMSTAR-2 questions 2, 4, 7, and 8 on review methods and deviation of methodology, search strategy, list of excluded studies and justifications, description of study details scored the worst where >50% studies were partial yes or no. Meta-analysis was not performed in 14 studies [23,38,41,47,58,64,65,70,71,75,81]. There were fifteen non-randomised trials [38,41,47,50,53,54,55,56,57,58,59,60,64,65,71,77] included in this study. There was no discernible trend in review quality across intervention categories across high-quality studies, and it declined from moderate to very low studies. Scoping data from 2 studies [25,72] informed studies in tables with no own data included in the actual tables. The quality of and type of intervention varied across the studies in Table 3, the high-quality studies in Table 4 and excluded students Table A1.
Table 3.
AMSTAR grading of articles and certainty of evidence.
Table 4.
High-quality systematic reviews, study characteristics, and findings.
AMSTAR Questions
- Did the research questions and inclusion criteria for the review include the components of PICO?
- Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review, and did the report justify any significant deviations from the protocol?
- Did the review authors explain their selection of the study designs for inclusion in the review?
- Did the review authors use a comprehensive literature search strategy?
- Did the review authors perform study selection in duplicate?
- Did the review authors perform data extraction in duplicate?
- Did the review authors provide a list of excluded studies and justify the exclusions?
- Did the review authors describe the included studies in adequate detail?
- Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? (RCTs; NRSI)
- Did the review authors report on the sources of funding for the studies included in the review?
- If meta-analysis was performed, did the review authors use appropriate methods for statistical combination of results? (RCTs; NRSI)
- If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis?
- Did the review authors account for RoB in individual studies when interpreting/discussing the results of the review?
- Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review?
- If they performed quantitative synthesis, did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review?
- Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review?
Table 2 AMSTAR Scoring and interpretation
Rating overall confidence in the results of the review
- High—Zero or one non-critical weakness: The systematic review provides an accurate and comprehensive summary of the results of the available studies that address the question of interest.
- Moderate—More than one non-critical weakness: The systematic review has more than one weakness but no critical flaws. It may provide an accurate summary of the results of the available studies that were included in the review.
- Low—One critical flaw with or without non-critical weaknesses: The review has a critical flaw and may not provide an accurate and comprehensive summary of the available studies that address the question of interest.
- Critically low—More than one critical flaw with or without non-critical weaknesses: The review has more than one critical flaw and should not be relied on to provide an accurate and comprehensive summary of the available studies.
- Note: Multiple non-critical weaknesses may diminish confidence in the review, and it may be appropriate to move the overall appraisal down from moderate to low confidence.
- i.
- Effects by cardiovascular outcomes
- a.
- Mortality
Mortality outcomes were reported in 31 studies across the included reviews. Of these,
- 12 studies reported a significant reduction in mortality associated with CDSM interventions, particularly those delivered through nurse-led or team-based models [23,24,26,31,32,39,43,46,57,67,68,80].
- Three studies indicated a positive trend toward mortality reduction, though not statistically significant [63,66,79].
- Six studies presented equivocal findings, with mixed or inconclusive mortality outcomes [30,33,34,49,64,76].
- 10 studies found no mortality benefit or reported a negative effect, including either no change or increased mortality rates [27,28,35,44,47,48,49,62,81,82].
- 28 studies did not report mortality outcomes [25,29,36,37,38,40,41,42,45,50,51,52,53,54,55,56,58,59,60,61,65,69,70,72,74,75,77,78].
By Study Quality:
High-Quality Reviews
- Significant mortality reduction: [31,32,67,68,71,80].
- Equivocal: [30,49,66,79].
- Negative: [27,35,62,81,82].
- Not reported: [42,50,52,72,74,77,78].
Moderate-Quality Reviews
- Significant mortality reduction: [43].
- Equivocal: [33,76].
- Negative: [47,48,73,75].
- Not reported: [36,38,41,51,53,54,56,58,59,65].
Summary Insight
Evidence for the impact of CDSM on mortality was mixed. A minority of high-quality studies showed significant mortality reduction, particularly in structured nurse-led or integrated multidisciplinary models. However, a substantial number of studies either reported no mortality benefit or did not assess this outcome at all. The inconsistency may reflect variations in study design, follow-up duration, or intervention intensity. As mortality was not a primary outcome in many included reviews, these findings should be interpreted with caution.
- ii.
- Hospital readmissions
Hospital readmission data were reported in 34 studies across the umbrella review. Of these,
- 25 studies reported a significant reduction in readmissions following CDSM interventions. These effects were most commonly associated with structured, nurse-led models [23,24,27,29,31,32,35,39,41,43,46,47,52,56,57,58,59,62,66,67,68,71,73,74,81,82].
- Three studies showed a positive trend, though it was not statistically significant [26,63,79].
- Seven studies were equivocal, showing mixed or inconclusive results [30,33,34,37,49,64,76].
- Three studies reported no improvement or a negative effect on readmissions [28,44,48].
- 21 studies did not report readmission outcomes [25,33,38,42,45,50,51,53,54,55,60,61,65,69,70,72,75,77,78,80].
By Study Quality:
High-Quality Reviews
- Significant reduction in readmissions: [27,31,32,35,62,66,67,68,71,74,81,82].
- Equivocal findings: [30,49,79].
- Negative findings: None reported.
- Not reported: [42,50,67,77,78,80].
Moderate-Quality Reviews
- Significant reduction in readmissions: [39,41,43,46,47,56,58,59,73].
- Equivocal: [33,76].
- Negative: [48].
- Not reported: [36,38,45,51,53,54,65,75].
Summary Insight
Evidence for the impact of CDSM interventions on hospital readmissions was generally favourable. A substantial number of both high- and moderate-quality reviews reported significant reductions, particularly for nurse-led and structured multidisciplinary programmes. While a small number of studies found no effect or had equivocal results, no high-quality studies reported a significant worsening of readmission outcomes. Variability in follow-up duration and outcome reporting, however, limits the strength of causal claims in some cases.
- b.
- Health-related quality of life
HRQoL outcomes were reported across the 29 studies included in the umbrella review. Of these,
- 23 studies showed statistically significant improvements in HRQoL following CDSM interventions, particularly those led by nurses or multidisciplinary teams [23,24,25,29,33,34,35,37,38,43,44,45,46,47,50,57,58,59,65,66,67,68,69,70,71,73,74,80].
- Seven studies reported a positive trend toward HRQoL improvement, though it was not always statistically significant [32,48,61,62,63,79,82].
- Nine studies were equivocal, with mixed or inconclusive findings [31,40,42,49,56,60,64,76,81].
- Four studies found no improvement or a decline in HRQoL scores [29,40,52,61].
- 14 studies did not report on HRQoL at all [26,27,30,36,41,52,53,54,55,72,75,77,78].
Improvements were most consistent in nurse-led interventions, especially those involving structured education, regular follow-up, and patient goal-setting. Reviews highlighted the importance of culturally and contextually adapted delivery models in optimising patient-reported quality of life outcomes.
- c.
- Self-management behaviours
Self-management (SM) outcomes were reported across 31 studies in the umbrella review. Of these,
- 25 studies showed statistically significant improvements in SM behaviours, including medication adherence, symptom monitoring, dietary/lifestyle modifications, and patient confidence [23,25,26,28,29,36,38,42,43,44,46,47,49,50,51,53,57,58,59,60,67,69,70,71,73,74,75,76,77,78,80].
- Four studies reported a positive trend toward SM improvement, though it was not statistically significant [62,64,67,79].
- 10 studies had equivocal findings, with mixed or inconclusive evidence [34,36,39,40,53,54,55,63,67,81].
- Four studies found no improvement or a decline in SM behaviours [39,45,48,61].
- Nine studies did not report on self-management outcomes [24,27,30,31,32,33,34,52,66].
By Study Quality:
High-Quality Reviews
- Significant SM improvement reported: [42,49,50,67,68,71,74,77,78,80].
- Equivocal findings: [35,68,72,79,81,82].
- Negative outcome: [62].
- Not reported: [27,30,31,32,52,66].
Moderate-Quality Reviews
- Significant SM improvement reported: [33,36,38,43,46,47,51,53,58,59,73,75,76].
- Equivocal findings: [41,54,56,65].
- Negative outcome: [39,45,48].
- Not reported: [33].
Summary Insight
Overall, the studies led by nurses or delivered through structured, multidisciplinary approaches with patient education and follow-up performed best. Improvements were particularly robust in high-quality reviews, though some heterogeneity in outcomes remains—likely due to differences in intervention intensity, population characteristics, and outcome measures used.
- iii.
- Effects by intervention on health services
Cost-effectiveness of studies was not well documented or not reported in most studies. Three areas including the utility of emergency services including emergency rooms showed positive benefits in [26,57], trends in [63,64], and no benefit [28,29]; the length of hospital stay as beneficial [28,56,57,66,71], equivocal [63,64], or with no benefits [30] and the cost of care were explored also as beneficial [28,29,35,46,52,56,57,71,74,80,81,82], negative [62], or equivocal [63,64]. Only these studies were of moderate-to-high quality [33,35,46,52,56,62,66,71,74,80,81,82]. The details of the studies, care domains, lead providers, and self-management domains are reported below.
- iv.
- Results synthesis and summary
Across the umbrella review, consistent patterns emerged regarding the impact of nurse-led and multidisciplinary CDSM interventions on key outcomes in HFrEF care. Improvements in HRQoL and self-management behaviours were the most consistently reported benefits, with the strongest effects observed in nurse-led models, particularly those involving structured education, regular follow-up, and tailored patient engagement. These findings were supported by both high- and moderate-quality reviews.
Secondary outcomes such as hospital readmissions and mortality were less frequently reported and demonstrated more variability, with trends suggesting potential benefit but limited conclusive evidence. Multidisciplinary interventions that included pharmacists, psychologists, or allied health professionals showed added value, particularly in addressing comorbidities and social determinants of health.
Table 5, Table 6 and Table 7 provide a consolidation of these findings by outcome domain, allowing clearer comparison across studies and quality tiers. Overall, the evidence supports a growing consensus around the effectiveness of integrated, nurse-led, or team-based CDSM approaches in improving patient-reported outcomes in HFrEF populations.
Table 5.
(a) Summary of self-management (SM) behaviour outcomes across included studies. (b) Study quality subgroup breakdown.
Table 6.
(a) Summary of hospital readmission outcomes across included studies. (b) Study quality subgroup breakdown.
Table 7.
Meta-summary of findings across key outcomes.
4. Discussion
Summary of Evidence
This umbrella review synthesises four decades of systematic reviews on chronic disease self-management (CDSM) in heart failure with reduced ejection fraction (HFrEF). While CDSM has long been considered a foundational strategy in chronic disease care, recent revisions to the 2022 ACC/AHA guidelines have downgraded it from a performance to a quality measure. This reflects evolving priorities in guideline development and growing emphasis on health-related quality of life (HRQoL) rather than major adverse cardiovascular events (MACEs) as the primary outcome of interest.
The findings from this review reaffirm that well-structured, nurse-led, and multidisciplinary CDSM interventions can improve patient outcomes when implemented with fidelity and contextual relevance. However, variability in study quality, design, delivery models, and reporting standards remains a key challenge, particularly in comparing outcomes across clinical settings and populations [83,84,85,86,87,88,89].
Mortality
While some reviews report mortality benefits associated with CDSM, the overall picture remains mixed. Differences in intervention intensity, care models, and follow-up periods likely contribute to inconsistent findings. Our review reflects similar variability reported in other chronic conditions. For instance, a recent CDSM study in COPD populations also failed to demonstrate consistent mortality reduction, despite improvements in other outcomes [88]. These findings suggest that while mortality is an important endpoint, its sensitivity to complex, non-pharmacological interventions may be limited—particularly when therapeutic environments and standard care are already optimised.
Hospital Readmissions
Hospital readmissions were more consistently impacted by CDSM interventions, particularly those involving structured follow-up and multidisciplinary collaboration. These findings are consistent with other chronic disease settings, where CDSM training and patient support strategies have reduced healthcare utilisation [70,88]. Standardising how readmissions are reported and tracked will further support the integration of these interventions into care models and funding frameworks.
Health-Related Quality of Life (HRQoL)
HRQoL improvements emerged as one of the most consistent benefits across reviewed studies. Interventions that included emotional, educational, and behavioural support were particularly associated with better quality of life. These findings align with the broader literature, which shows that HRQoL can be effectively enhanced through patient-centred self-management approaches [88,89]. Given the multidimensional nature of HRQoL, interventions must be adaptable to patient preferences, cultural norms, and health literacy levels to optimise impact.
Self-Management Behaviours
CDSM interventions demonstrated strong potential to enhance patient engagement, medication adherence, and proactive health behaviours. This is further supported by external literature; for example, a systematic review and meta-analysis by Cho and Kim found that nurse-led self-management programmes improved behavioural outcomes and significantly reduced HbA1c in people living with diabetes [89]. These findings highlight the cross-condition benefits of nurse-led education and support, which are central to empowering patients and reducing dependency on acute services.
Health Service Effects
While evidence on service use and cost-effectiveness was less frequently reported, the available data point to potential reductions in emergency visits and shorter hospital stays. However, without consistent reporting and economic modelling, conclusions remain tentative. Given the rising burden on healthcare systems, particularly in the context of multimorbidity and an ageing population, future evaluations must include resource utilisation and cost data to guide scale-up and investment decisions.
Making Sense of High-Quality Evidence
Earlier high-quality reviews—such as those by Roccafort, Ruppar, Jonkman, Boren, and Inglis—provided strong evidence of benefit across outcomes including mortality, self-management, and hospitalisation. These reviews consistently included structured, multidisciplinary, and nurse-led programmes with extended follow-up durations and involvement of family carers. Importantly, these studies were conducted before widespread uptake of modern pharmacotherapies, suggesting that CDSM interventions held value even in the absence of today’s advanced therapies.
In contrast, more recent high-quality reviews such as those by Lee [48], Ditewig, and Paranjuli [79] offered more equivocal or negative conclusions. These differences may reflect changes in comparator care (e.g., higher baseline quality), variability in delivery agents (e.g., pharmacists vs. nurses), or inconsistency in intervention scope. Nonetheless, these findings reinforce that the effectiveness of CDSM is not solely about content but also who delivers it, how, and in what context.
Strengths and Limitations
This umbrella review is the first to synthesise systematic reviews specifically focused on nurse-led and multidisciplinary CDSM in HFrEF. A key strength lies in its comprehensive scope, inclusion of high-quality evidence, and alignment with chronic disease management frameworks.
However, limitations include the inability to perform meta-analysis and the reliance on secondary interpretations of primary study data. The heterogeneity in intervention formats, delivery personnel, and outcome definitions across reviews limits the precision with which definitive conclusions can be drawn. Additionally, many reviews lacked detailed reporting on economic outcomes, cultural adaptations, or implementation factors—key elements for translating findings into policy and practice.
Implications for Practice and Policy
- Nurse-led CDSM should be embedded into routine HFrEF care as part of standard, multidisciplinary disease management programmes.
- Future trials should adopt a core outcomes set that includes HRQoL, hospital readmissions, self-management behaviours, and cost-effectiveness.
- Co-design and cultural tailoring should be prioritised to enhance relevance and patient engagement across diverse settings.
- Economic evaluations must be incorporated into programme design to support scale-up and policy adoption.
5. Conclusions
This umbrella review highlights consistent benefits of nurse-led and multidisciplinary CDSM interventions for individuals with HFrEF, particularly in reducing hospital readmissions and improving HRQoL. While evidence for mortality reduction remains mixed—even among high-quality reviews, these interventions appear to play a critical role in stabilising patient trajectories and enhancing everyday functioning.
Persistent gaps include underreporting of cost-effectiveness, limited analysis of culturally tailored models, and variability in outcome measurement. Addressing these gaps through more standardised, equity-oriented, and economically evaluated research will be essential to support broader implementation and inform future policy decisions.
Author Contributions
P.I., F.H. and M.d.C. participated in research design, data analysis, and writing of the paper. P.I., F.H., B.G. and T.P. participated in the performance of the research and data collection. P.I., D.A., I.S., B.G., F.H. and M.d.C. provided advice and support. P.I. assisted F.H. in statistical analysis. All authors have read and agreed to the published version of the manuscript.
Funding
P.I. was a recipient of RACP, Fellow Contributions Fund (2023RES00137).
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Not Applicable.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
Support from relevant University and clinic administration.
Conflicts of Interest
Professor Malcolm Battersby is co-inventor of the ‘Flinders Model of Chronic Condition Self-Management’ and has received competitive and Federal Government funding for research in chronic condition self-management. All other authors have received government and non-governmental funding. None pose a conflict of interest for this publication.
Appendix A
Table A1.
Details of excluded studies.
Table A1.
Details of excluded studies.
| Study | Reason for Exclusion |
|---|---|
| Kent B, Cull E, Phillips N. A systematic review of the effectiveness of current interventions to assist adults with heart failure to comply with therapy and enhance self-care behaviours. JBI Library of Systematic Reviews. 2010;8:1–12. | Protocol |
| Inglis SC, Clark RA, Dierckx R, Prieto-Merino D, Cleland JGF. Structured telephone support or non-invasive telemonitoring for patients with heart failure. The Cochrane database of systematic reviews. 2015;(10):CD007228. | Update in 2015 |
| Buck HG, Harkness K, Wion R, et al. Caregivers’ contributions to heart failure self-care: a systematic review. European journal of cardiovascular nursing. 2015;14(1):79–89. | No outcome data |
| Lancey, A.; Slater, C.E. Heart failure self-management: A scoping review of interventions implemented by allied health pro-fessionals. Disabil. Rehabil. 2023, 46, 4848–4859. | Scoping Review |
| McBain H, Shipley M, Newman S. The impact of self-monitoring in chronic illness on healthcare utilisation: a systematic review of reviews. BMC health services research. 2015;15:565. | Telemonitoring |
| Ballester M, Orrego C, Heijmans M, et al. Comparing the effectiveness and cost-effectiveness of self-management interventions in four high-priority chronic conditions in Europe (COMPAR-EU): a research protocol. BMJ open. 2020;10(1):e034680. | Not SR |
| Riegel B, Westland H, Iovino P, Barelds I, Bruins Slot J, Stawnychy MA, Osokpo O, Tarbi E, Trappenburg JCA, Vellone E, Strömberg A, Jaarsma T. Characteristics of self-care interventions for patients with a chronic condition: A scoping review. Int J Nurs Stud. 2021 Apr;116:103713 | Scoping Review |
| Salahodinkolah MK, Ganji J, Moghadam SH, Shafipour V, Jafari H, Salari S. Educational intervention for improving self-care behaviors in patients with heart failure: A narrative review. Journal of Nursing & Midwifery Sciences. 2020;7(1):60–68. | Not SR |
| Noonan MC, Wingham J, Dalal HM, Taylor RS. Involving caregivers in self-management interventions for patients with heart failure and chronic obstructive pulmonary disease. A systematic review and meta-analysis. J Adv Nurs. 2019 Dec;75(12):3331–3345. | No MACE data |
| Kyriakou M, Middleton N, Ktisti S, Philippou K, Lambrinou E. Supportive Care Interventions to Promote Health-Related Quality of Life in Patients Living With Heart Failure: A Systematic Review and Meta-Analysis. Heart Lung Circ. 2020 Nov;29(11):1633–1647. | No MACE data |
| Bayly J, Bone AE, Ellis-Smith C, et al. Common elements of service delivery models that optimise quality of life and health service use among older people with advanced progressive conditions: a tertiary systematic review. BMJ open. 2021;11(12):e048417. | No MACE data |
| WANG Sixiong, ZHU Meiyi. Influence of motivational interviewing on self-care behavior in patients with chronic heart failure: a Meta-analysis. Chinese Evidence-based Nursing. 2021;5:598–603. | Article not accessible |
| Pinto Braga P, Barbosa de Castro EA, de Medeiros Souza T, Rocha Raimundo Leone D, Sabrina de Souza M, Lara da Silva K. Costs and Benefits of Home Care for People with Complex Chronic Conditions: An Integrative Review. Ciencia, Cuidado e Saude. 2022;21:1–11. | Integrative review |
| LIU Mengdie, XIONG Xiaoyun, SUN Xinglan, et al. Summary of the best evidence for self-management in patients with chronic heart failure. Chinese Journal of Nursing. 2022;57(23):2937–2944. | No relevant data |
| Ali AA, Sagheer S. A Review to Access Knowledge, Attitudes, and Practices among Nurses of Cardiac Medicine for Heart Failure Patients to Prevent Readmission in Hospitals. i-manager’s Journal on Nursing. 2023;12(4):42–48. | Not relevant to this review |
| McGreal MH, Hogan MJ, Walsh-Irwin C, Maggio NJ, Jurgens CY. Heart failure self-care interventions to reduce clinical events and symptom burden. Research Reports in Clinical Cardiology. 2014;5:243–257. | No relevant data |
| Koirala B, Himmelfarb CD, Budhathoki C, Tankumpuan T, Asano R, Davidson PM. Factors affecting heart failure self-care: An integrative review. Heart & Lung. 2018;47(6):539–545. | Integrative review |
| King AJL, Johnson R, Cramer H, Purdy S, Huntley AL. Community case management and unplanned hospital admissions in patients with heart failure: A systematic review and qualitative evidence synthesis. Journal of advanced nursing. 2018;74(7):1463–1473. | Only qualitative data |
| Purdey S, Huntley A. Predicting and preventing avoidable hospital admissions: a review. The journal of the Royal College of Physicians of Edinburgh. 2013;43(4):340–344. | No relevant data |
| Imran HM, Baig M, Erqou S, Taveira TH, Shah NR, Morrison A, Choudhary G, Wu WC. Home-Based Cardiac Rehabilitation Alone and Hybrid With Center-Based Cardiac Rehabilitation in Heart Failure: A Systematic Review and Meta-Analysis. J Am Heart Assoc. 2019 Aug 20;8(16):e012779. | CDSM not described |
| Son Y-J, Lee Y, Lee H-J. Effectiveness of Mobile Phone-Based Interventions for Improving Health Outcomes in Patients with Chronic Heart Failure: A Systematic Review and Meta-Analysis. International journal of environmental research and public health. 2020;17(5). | Telemonitoring |
References
- Allegrante, J.P.; Wells, M.T.; Peterson, J.C. Interventions to Support Behavioral Self-Management of Chronic Diseases. Annu. Rev. Public Health 2019, 40, 127–146. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.M.; Savard, L.A.; Thompson, D.R. What Is the Strength of Evidence for Heart Failure Disease-Management Programs? J. Am. Coll. Cardiol. 2009, 54, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Krumholz, H.M.; Currie, P.M.; Riegel, B.; Phillips, C.O.; Peterson, E.D.; Smith, R.; Yancy, C.W.; Faxon, D.P.; American Heart Association Disease Management Taxonomy Writing Group. A taxonomy for disease management. Circulation 2006, 114, 1432–1445. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Fonarow, G.C.; Breathett, K.; Jurgens, C.Y.; Pisani, B.A.; Pozehl, B.J.; Spertus, J.A.; Taylor, K.G.; Thibodeau, J.T.; Yancy, C.W.; et al. 2020 ACC/AHA Clinical Performance and Quality Measures for Adults with Heart Failure. J. Am. Coll. Cardiol. 2020, 76, 2527–2564. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary. J. Am. Coll. Cardiol. 2022, 79, 1757–1780. [Google Scholar] [CrossRef]
- Iyngkaran, P.; Liew, D.; Neil, C.; Driscoll, A.; Marwick, T.H.; Hare, D.L. Moving From Heart Failure Guidelines to Clinical Practice: Gaps Contributing to Readmissions in Patients with Multiple Comorbidities and Older Age. Clin. Med. Insights Cardiol. 2018, 12, 1179546818809358. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Abraham, W.T.; Albert, N.M.; Stough, W.G.; Gheorghiade, M.; Greenberg, B.H.; O’Connor, C.M.; Pieper, K.; Sun, J.L.; Yancy, C.; et al. Association between performance measures and clinical outcomes for patients hospitalized with heart failure. JAMA 2007, 297, 61–70. [Google Scholar] [CrossRef]
- Toukhsati, S.R.; Jaarsma, T.; Babu, A.S.; Driscoll, A.; Hare, D.L. Self-Care Interventions That Reduce Hospital Readmissions in Patients With Heart Failure; Towards the Identification of Change Agents. Clinical Medicine Insights. Cardiology 2019, 13, 1179546819856855. [Google Scholar] [CrossRef]
- Iyngkaran, P.; Buhler, M.; de Courten, M.; Hanna, F. Effectiveness of self-management programmes for heart failure with reduced ejection fraction: A systematic review protocol. BMJ Open 2024, 14, e079830. [Google Scholar] [CrossRef]
- Iyngkaran, P.; Fazli, F.; Nguyen, H.; Patel, T.; Hanna, F. Historical Gaps in the Integration of Patient-Centric Self-Management Components in HFrEF Interventions: An Umbrella Narrative Review. J. Clin. Med. 2025, 14, 2832. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Iyngkaran, P.; Toukhsati, S.R.; Harris, M.; Connors, C.; Kangaharan, N.; Ilton, M.; Nagel, T.; Moser, D.K.; Battersby, M. Self Managing Heart Failure in Remote Australia—Translating Concepts into Clinical Practice. Curr. Cardiol. Rev. 2016, 12, 270–284. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Hartling, L.; Ospina, M.; Liang, Y.; Dryden, D.M.; Hooton, N.; Krebs Seida, J.; Klassen, T.P. Risk of bias versus quality assessment of randomised controlled trials: Cross sectional study. BMJ 2009, 339, b4012. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, version 6.2 (updated February 2021); Cochrane: London, UK, 2021; Available online: https://www.training.cochrane.org/handbook (accessed on 12 July 2025).
- Cochrane Effective Practice and Organisation of Care Group. Available online: http://www.epoc.cochrane.org (accessed on 10 July 2025).
- Freund, T. Improving the Quality of Quality Assessment in Systematic Reviews. Rapid Response to: Risk of Bias Versus Quality Assessment of Randomised Controlled Trials: Cross Sectional Study. BMJ 2009, 339, b4012. Available online: https://www.bmj.com/rapid-response/2011/11/02/improving-quality-quality-assessment-systematic-reviews (accessed on 10 July 2025).
- Freund, T.; Kayling, F.; Miksch, A.; Szecsenyi, J.; Wensing, M. Effectiveness and efficiency of primary care based case management for chronic diseases: Rationale and design of a systematic review and meta-analysis of randomized and non-randomized trials [CRD32009100316]. BMC Health Serv. Res. 2010, 10, 112. [Google Scholar] [CrossRef]
- Shepperd, S.; Lewin, S.; Straus, S.; Clarke, M.; Eccles, M.P.; Fitzpatrick, R.; Wong, G.; Sheikh, A. Can we systematically review studies that evaluate complex interventions? PLoS Med. 2009, 6, e1000086. [Google Scholar] [CrossRef]
- Belbasis, L.; Bellou, V.; Ioannidis, J.P.A. Conducting umbrella reviews. BMJ Med. 2022, 1, e000071. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.; Holly, C.; Khalil, H.; Tungpunkom, P. Chapter 10: Umbrella Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 17 April 2025).
- Zhao, X.; Wu, S.; Luo, N.; Lin, Q.; Zhao, X.; Li, K. Care models for patients with heart failure at home: A systematic review. J. Clin. Nurs. 2024, 33, 1295–1305. [Google Scholar] [CrossRef]
- Chen, C.W.; Lee, M.-C.; Wu, S.-F.V. Effects of a collaborative health management model on people with congestive heart failure: A systematic review and meta-analysis. J. Adv. Nurs. 2023, 80, 2290–2307. [Google Scholar] [CrossRef]
- Li, X.; Liu, Y. Effect of Transitional Care Strategies on Health-Related Quality of Life (HRQoL) in Heart Failure with Reduced Ejection Fraction (HFrEF): A Systematic Review and Meta-analysis of Randomized Controlled Trails. Altern. Ther. Health Med. 2023, 29, AT8909. [Google Scholar]
- Yang, Y.-F.; Hoo, J.-X.; Tan, J.-Y.; Lim, L.-L. Multicomponent integrated care for patients with chronic heart failure: Systematic review and meta-analysis. ESC Heart Fail. 2023, 10, 791–807. [Google Scholar] [CrossRef] [PubMed]
- Hafkamp, F.J.; Tio, R.A.; Otterspoor, L.C.; de Greef, T.; van Steenbergen, G.J.; van de Ven, A.R.; Smits, G.; Post, H.; van Veghel, D. Optimal effectiveness of heart failure management—An umbrella review of meta-analyses examining the effectiveness of interventions to reduce (re)hospitalizations in heart failure. Heart Fail. Rev. 2022, 27, 1683–1748. [Google Scholar] [CrossRef] [PubMed]
- Hsu, S.-F.; Lee, S.-Y.; Hsu, T.-F.; Li, J.-Y.; Tung, H.-H. Patient Navigators for Transition Care of Heart Failure: A Systematic Review and Meta-Analysis. Int. J. Gerontol. 2022, 16, 76–82. [Google Scholar]
- Toback, M.; Clark, N. Strategies to improve self-management in heart failure patients. Contemp. Nurse 2017, 53, 105–120. [Google Scholar] [CrossRef]
- Taylor, S.J.; Bestall, J.C.; Cotter, S.; Falshaw, M.; Hood, S.G.; Parsons, S.; Wood, L.; Underwood, M. Clinical service organization for heart failure. Cochrane Database Syst. Rev. 2005, 2, CD002752. [Google Scholar]
- Roccaforte, R.; Demers, C.; Baldassarre, F.; Teo, K.K.; Yusuf, S. Effectiveness of comprehensive disease management programmes in improving clinical outcomes in heart failure patients. A meta-analysis. Eur. J. Heart Fail. 2005, 7, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Gonseth, J.; Guallar-Castillón, P.; Banegas, J.R.; Rodríguez-Artalejo, F. The effectiveness of disease management programmes in reducing hospital re-admission in older patients with heart failure: A systematic review and meta-analysis of published reports. Eur. Heart J. 2004, 25, 1570–1595. [Google Scholar] [CrossRef]
- Huang, Z.; Liu, T.; Gao, R.; Chair, S.Y. Effects of nurse-led self-care interventions on health outcomes among people with heart failure: A systematic review and meta-analysis. J. Clin. Nurs. 2023, 33, 1282–1294. [Google Scholar] [CrossRef]
- Nwosu, W.O.; Rajani, R.; McDonaugh, T.; Goulder, A.; Smith, D.; Hughes, L. The impact of nurse-led patient education on quality of life in patients with heart failure. Br. J. Card. Nurs. 2023, 18, 1–13. [Google Scholar] [CrossRef]
- Checa, C.; Canelo-Aybar, C.; Suclupe, S.; Ginesta-López, D.; Berenguera, A.; Castells, X.; Brotons, C.; Posso, M. Effectiveness and Cost-Effectiveness of Case Management in Advanced Heart Failure Patients Attended in Primary Care: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 13823. [Google Scholar] [CrossRef]
- Huang, Z.; Liu, T.; Chair, S.Y. Effectiveness of nurse-led self-care interventions on self-care behaviors, self-efficacy, depression and illness perceptions in people with heart failure: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2022, 132, 104255. [Google Scholar] [CrossRef]
- do Céu Sá, M.; Nabais, A. How to care for patients with heart failure—A systematic review of nursing interventions. New Trends Qual. Res. 2022, 11, e557. [Google Scholar]
- Tonapa, S.I.; Inayati, A.; Sithichoksakulchai, S.; Daryanti Saragih, I.; Efendi, F.; Chou, F.H. Outcomes of nurse-led telecoaching intervention for patients with heart failure: A systematic review and meta-analysis of randomised controlled trials. J. Clin. Nurs. 2022, 31, 1125–1135. [Google Scholar] [CrossRef]
- Son, Y.J.; Choi, J.; Lee, H.J. Effectiveness of Nurse-Led Heart Failure Self-Care Education on Health Outcomes of Heart Failure Patients: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6559. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.C. A Nurse Led Clinic’s contribution to Patient Education and Promoting Self-care in Heart Failure Patients: A Systematic Review. Int. J. Integr. Care 2017, 17, 492. [Google Scholar] [CrossRef]
- Alnomasy, N.; Still, C.H. Nonpharmacological Interventions for Preventing Rehospitalization Among Patients with Heart Failure: A Systematic Review and Meta-Analysis. SAGE Open Nurs. 2023, 9, 23779608231209220. [Google Scholar] [CrossRef]
- Mhanna, M.; Sauer, M.C.; Al-Abdouh, A.; Jabri, A.; Abusnina, W.; Safi, M.; Beran, A.; Mansour, S. Cognitive behavioral therapy for depression in patients with heart failure: A systematic review and metanalysis of randomized control trials. Heart Fail. Rev. 2023, 28, 1091–1100. [Google Scholar] [CrossRef]
- Olano-Lizarraga, M.; Wallström, S.; Martín-Martín, J.; Wolf, A. Interventions on the social dimension of people with chronic heart failure: A systematic review of randomized controlled trials. Eur. J. Cardiovasc. Nurs. 2023, 22, 113–125. [Google Scholar] [CrossRef]
- Nso, N.M.; Emmanuel, K.; Nassar, M.M.; Bookani, K.R.; Antwi-Amoabeng, D.M.; Alshamam, M.; Kondaveeti, R.; Kompella, R.; Lakhdar, S.; Rizzo, V.M.; et al. Efficacy of Cognitive Behavioral Therapy in Heart Failure Patients: A Systematic Review and Meta-Analysis. Cardiol. Rev. 2023, 31, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Balata, M.; Gbreel, M.I.; Elrashedy, A.A.; Westenfeld, R.; Pfister, R.; Zimmer, S.; Nickenig, G.; Becher, M.U.; Sugiura, A. Clinical effects of cognitive behavioral therapy in heart failure patients: A meta-analysis of randomized controlled trials. BMC Complement. Med. Ther. 2023, 23, 280. [Google Scholar] [CrossRef]
- Koikai, J.; Khan, Z. The Effectiveness of Self-Management Strategies in Patients with Heart Failure: A Narrative Review. Cureus 2023, 15, e41863. [Google Scholar] [CrossRef]
- Feng, C.; Wang, Y.; Li, S.; Qu, Z.; Zheng, S. Effect of self-management intervention on prognosis of patients with chronic heart failure: A meta-analysis. Nurs. Open 2023, 10, 2015–2029. [Google Scholar] [CrossRef]
- Nahlén Bose, C. A meta-review of systematic reviews and meta-analyses on outcomes of psychosocial interventions in heart failure. Front. Psychiatry 2023, 14, 1095665. [Google Scholar] [CrossRef]
- Lee, C.S.; Westland, H.; Faulkner, K.M.; Iovino, P.; Thompson, J.H.; Sexton, J.; Farry, E.; Jaarsma, T.; Riegel, B. The effectiveness of self-care interventions in chronic illness: A meta-analysis of randomized controlled trials. Int. J. Nurs. Stud. 2022, 134, 104322. [Google Scholar] [CrossRef]
- Villero-Jiménez, A.I.; Martínez-Torregrosa, N.; Olano Lizarraga, M.; Garai-López, J.; Vázquez-Calatayud, M. Dyadic self-care interventions in chronic heart failure in hospital settings: A systematic review. An. Sis. Sanit. Navar. 2022, 45, e1001. [Google Scholar] [CrossRef] [PubMed]
- Ghizzardi, G.; Arrigoni, C.; Dellafiore, F.; Vellone, E.; Caruso, R. Efficacy of motivational interviewing on enhancing self-care behaviors among patients with chronic heart failure: A systematic review and meta-analysis of randomized controlled trials. Heart Fail. Rev. 2022, 27, 1029–1041. [Google Scholar] [CrossRef] [PubMed]
- Suksatan, W.; Tankumpuan, T. The Effectiveness of Transition Care Interventions from Hospital to Home on Rehospitalization in Older Patients with Heart Failure: An Integrative Review. Home Health Care Manag. Pract. 2022, 34, 63–71. [Google Scholar] [CrossRef]
- Meng, X.; Wang, Y.; Tang, X.; Gu, J.; Fu, Y. Self-management on heart failure: A meta-analysis. Diabetes Metab. Syndr. 2021, 15, 102176. [Google Scholar] [CrossRef]
- de Melo Vellozo Pereira Tinoco, J.; da Silva Figueiredo, L.; Flores, P.V.P.; de Padua, B.L.R.; Mesquita, E.T.; Cavalcanti, A.C.D. Effectiveness of health education in the self-care and adherence of patients with heart failure: A meta-analysis. Rev. Latino-Am. Enferm. 2021, 29, e3389. [Google Scholar]
- Aghajanloo, A.; Negarandeh, R.; Janani, L.; Tanha, K.; Hoseini-Esfidarjani, S.S. Self-care status in patients with heart failure: Systematic review and meta-analysis. Nurs. Open 2021, 8, 2235–2248. [Google Scholar] [CrossRef]
- Cañon-Montañez, W.; Duque-Cartagena, T.; Rodríguez-Acelas, A.L. Effect of Educational Interventions to Reduce Readmissions due to Heart Failure Decompensation in Adults: A Systematic Review and Meta-analysis. Investig. Educ. Enferm. 2021, 39, e05. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.A.; Clemett, V. What impact do specialist and advanced-level nurses have on people living with heart failure compared to physician-led care? A literature review. J. Res. Nurs. 2021, 26, 229–249. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Chen, C.; Zhang, J.; Ye, Y.; Fan, X. Effects of self-management interventions on heart failure: Systematic review and meta-analysis of randomized controlled trials. Int. J. Nurs. Stud. 2021, 116, 103909. [Google Scholar] [CrossRef] [PubMed]
- Poudel, N.; Kavookjian, J.; Scalese, M.J. Motivational Interviewing as a Strategy to Impact Outcomes in Heart Failure Patients: A Systematic Review. Patient 2020, 13, 43–55. [Google Scholar] [CrossRef]
- Świątoniowska-Lonc, N.A.; Sławuta, A.; Dudek, K.; Jankowska, K.; Jankowska-Polańska, B.K. The impact of health education on treatment outcomes in heart failure patients. Adv. Clin. Exp. Med. 2020, 29, 481–492. [Google Scholar] [CrossRef]
- Peng, Y.; Fang, J.; Huang, W.; Qin, S. Efficacy of Cognitive Behavioral Therapy for Heart Failure. Int. Heart J. 2019, 60, 665–670. [Google Scholar] [CrossRef]
- Parajuli, D.R.; Kourbelis, C.; Franzon, J.; Newman, P.; Mckinnon, R.A.; Shakib, S.; Whitehead, D.; Clark, R.A. Effectiveness of the Pharmacist-Involved Multidisciplinary Management of Heart Failure to Improve Hospitalizations and Mortality Rates in 4630 Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Card. Fail. 2019, 25, 744–756. [Google Scholar] [CrossRef]
- Shanbhag, D.; Graham, I.D.; Harlos, K.; Haynes, R.B.; Gabizon, I.; Connolly, S.J.; Van Spall, H.G.C. Effectiveness of implementation interventions in improving physician adherence to guideline recommendations in heart failure: A systematic review. BMJ Open 2018, 8, e017765. [Google Scholar] [CrossRef]
- Sterling, M.R.; Shaw, A.L.; Leung, P.B.; Safford, M.M.; Jones, C.D.; Tsui, E.K.; Delgado, D. Home care workers in heart failure: A systematic review. J. Multidiscip. Healthc. 2018, 11, 481–492. [Google Scholar] [CrossRef]
- Jiang, Y.; Shorey, S.; Seah, B.; Chan, W.X.; Tam, W.W.S.; Wang, W. The effectiveness of psychological interventions on self-care, psychological and health outcomes in patients with chronic heart failure-A systematic review and meta-analysis. Int. J. Nurs. Stud. 2018, 78, 16–25. [Google Scholar] [CrossRef]
- Jonkman, N.H.; Westland, H.; Groenwold, R.H.; Ågren, S.; Anguita, M.; Blue, L.; de la Porte, P.W.B.-A.; DeWalt, D.A.; Hebert, P.L.; Heisler, M.; et al. What Are Effective Program Characteristics of Self-Management Interventions in Patients with Heart Failure? An Individual Patient Data Meta-analysis. J. Card. Fail. 2016, 22, 861–871. [Google Scholar] [CrossRef] [PubMed]
- Ruppar, T.M.; Cooper, P.S.; Mehr, D.R.; Delgado, J.M.; Dunbar-Jacob, J.M. Medication Adherence Interventions Improve Heart Failure Mortality and Readmission Rates: Systematic Review and Meta-Analysis of Controlled Trials. J. Am. Heart Assoc. 2016, 5, e002606. [Google Scholar] [CrossRef]
- Jonkman, N.H.; Westland, H.; Groenwold, R.H.; Ågren, S.; Atienza, F.; Blue, L.; Bruggink-André de la Porte, P.W.; DeWalt, D.A.; Hebert, P.L.; Heisler, M.; et al. Do Self-Management Interventions Work in Patients with Heart Failure? An Individual Patient Data Meta-Analysis. Circulation 2016, 133, 1189–1198. [Google Scholar] [CrossRef]
- Srisuk, N.; Cameron, J.; Ski, C.F.; Thompson, D.R. Heart failure family-based education: A systematic review. Patient Educ. Couns. 2016, 99, 326–338. [Google Scholar] [CrossRef] [PubMed]
- Ha Dinh, T.T.; Bonner, A.; Clark, R.; Ramsbotham, J.; Hines, S. The effectiveness of the teach-back method on adherence and self-management in health education for people with chronic disease: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2016, 14, 210–247. [Google Scholar] [CrossRef]
- Inglis, S.C.; Clark, R.A.; Dierckx, R.; Prieto-Merino, D.; Cleland, J.G.F. Structured telephone support or non-invasive telemonitoring for patients with heart failure. Cochrane Database Syst. Rev. 2015, 10, CD007228. [Google Scholar] [CrossRef]
- Ruppar, T.M.; Delgado, J.M.; Temple, J. Medication adherence interventions for heart failure patients: A meta-analysis. Eur. J. Cardiovasc. Nurs. 2015, 14, 395–404. [Google Scholar] [CrossRef]
- Casimir, Y.E.; Williams, M.M.; Liang, M.Y.; Pitakmongkolkul, S.; Slyer, J.T. The effectiveness of patient-centered self-care education for adults with heart failure on knowledge, self-care behaviors, quality of life, and readmissions: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2014, 12, 188–262. [Google Scholar] [CrossRef]
- Wakefield, B.J.; Boren, S.A.; Groves, P.S.; Conn, V.S. Heart failure care management programs: A review of study interventions and meta-analysis of outcomes. J. Cardiovasc. Nurs. 2013, 28, 8–19. [Google Scholar] [CrossRef]
- Barnason, S.; Zimmerman, L.; Young, L. An integrative review of interventions promoting self-care of patients with heart failure. J. Clin. Nurs. 2012, 21, 448–475. [Google Scholar] [CrossRef] [PubMed]
- Boyde, M.; Turner, C.; Thompson, D.R.; Stewart, S. Educational interventions for patients with heart failure: A systematic review of randomized controlled trials. J. Cardiovasc. Nurs. 2011, 26, E27–E35. [Google Scholar] [CrossRef] [PubMed]
- Dickson, V.V.; Buck, H.; Riegel, B. A qualitative meta-analysis of heart failure self-care practices among individuals with multiple comorbid conditions. J. Card. Fail. 2011, 17, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Yehle, K.S.; Plake, K.S. Self-efficacy and educational interventions in heart failure: A review of the literature. J. Cardiovasc. Nurs. 2010, 25, 175–188. [Google Scholar] [CrossRef]
- Ditewig, J.B.; Blok, H.; Havers, J.; van Veenendaal, H. Effectiveness of self-management interventions on mortality, hospital readmissions, chronic heart failure hospitalization rate and quality of life in patients with chronic heart failure: A systematic review. Patient Educ. Couns. 2010, 78, 297–315. [Google Scholar] [CrossRef]
- Boren, S.A.; Wakefield, B.J.; Gunlock, T.L.; Wakefield, D.S. Heart failure self-management education: A systematic review of the evidence. Int. J. Evid. Based Healthc. 2009, 7, 159–168. [Google Scholar] [CrossRef]
- Jovicic, A.; Holroyd-Leduc, J.M.; Straus, S.E. Effects of self-management intervention on health outcomes of patients with heart failure: A systematic review of randomized controlled trials. BMC Cardiovasc. Disord. 2006, 6, 43. [Google Scholar] [CrossRef]
- McAlister, F.A.; Stewart, S.; Ferrua, S.; McMurray, J.J. Multidisciplinary strategies for the management of heart failure patients at high risk for admission: A systematic review of randomized trials. J. Am. Coll. Cardiol. 2004, 44, 810–819. [Google Scholar]
- Available online: https://www.emro.who.int/uhc-health-systems/access-health-services/phc-oriented-models-of-care.html (accessed on 22 March 2025).
- Son, Y.-J.; Lee, Y.; Lee, H.-J. Effectiveness of Mobile Phone-Based Interventions for Improving Health Outcomes in Patients with Chronic Heart Failure: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 1749. [Google Scholar] [CrossRef]
- Imran, H.M.; Baig, M.; Erqou, S.; Taveira, T.H.; Shah, N.R.; Morrison, A.; Choudhary, G.; Wu, W.C. Home-Based Cardiac Rehabilitation Alone and Hybrid with Center-Based Cardiac Rehabilitation in Heart Failure: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2019, 8, e012779. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.flindersprogram.com.au (accessed on 17 April 2025).
- Lenferink, A.; Brusse-Keizer, M.; van der Valk, P.D.; A Frith, P.; Zwerink, M.; Monninkhof, E.M.; van der Palen, J.; Effing, T.W. Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2017, 8, CD011682. [Google Scholar] [CrossRef]
- Moreno-Ligero, M.; Moral-Munoz, J.A.; Salazar, A.; Failde, I. mHealth Intervention for Improving Pain, Quality of Life, and Functional Disability in Patients with Chronic Pain: Systematic Review. JMIR mHealth uHealth 2023, 11, e40844. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.K.; Kim, M.Y. Self-Management Nursing Intervention for Controlling Glucose among Diabetes: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12750. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).