
What Is the Role of Basal Weekly Insulin in Clinical Practice? The State of the Art




Abstract
1. Introduction
2. Methods
3. Basal Weekly Insulin
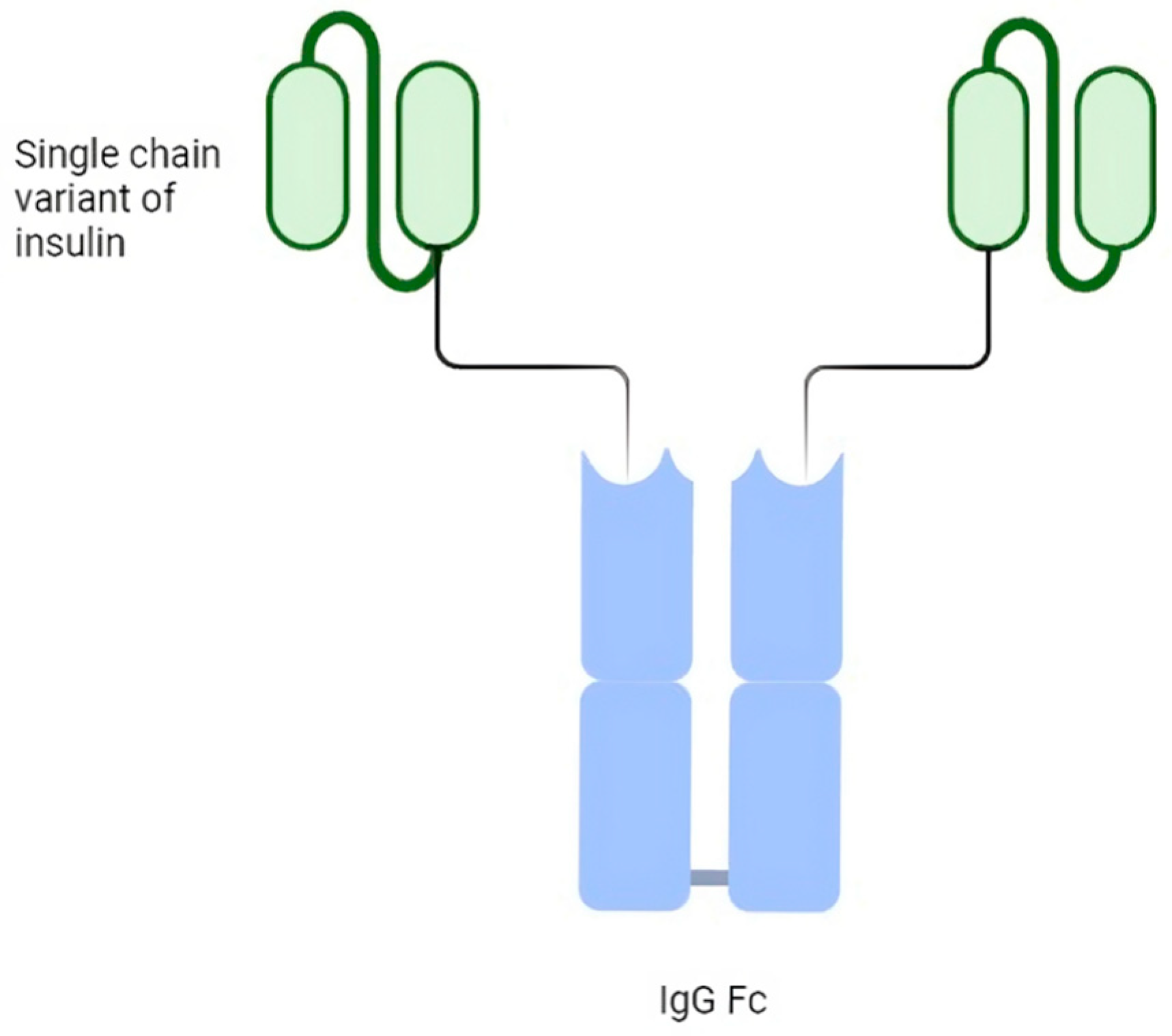
4. Basal Insulin Fc (BIF, LY3209590)
5. Insulin Icodec
6. Type 2 Diabetes Mellitus and Weekly Insulin
7. Type 1 Diabetes Mellitus and Weekly Insulin
8. Discussion
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ong, K.L.; Stafford, L.K.; McLaughlin, S.A.; Boyko, E.J.; Vollset, S.E.; Smith, A.E.; Dalton, B.E.; Duprey, J.; Cruz, J.A.; Hagins, H.; et al. Global, Regional, and National Burden of Diabetes from 1990 to 2021, with Projections of Prevalence to 2050: A Systematic Analysis for the Global Burden of Disease Study 2021. Lancet 2023, 402, 203–234. [Google Scholar] [CrossRef] [PubMed]
- IDF Diabetes Atlas 2021 | IDF Diabetes Atlas. Available online: https://diabetesatlas.org/atlas/tenth-edition/ (accessed on 13 February 2024).
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Argano, C.; Natoli, G.; Mularo, S.; Nobili, A.; Monaco, M.L.; Mannucci, P.M.; Perticone, F.; Pietrangelo, A.; Corrao, S. Impact of Diabetes Mellitus and Its Comorbidities on Elderly Patients Hospitalized in Internal Medicine Wards: Data from the RePoSi Registry. Healthcare 2022, 10, 86. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Natoli, G.; Nobili, A.; Mannucci, P.M.; Perticone, F.; Arcoraci, V.; Argano, C. The “Diabetes Comorbidome”: A Different Way for Health Professionals to Approach the Comorbidity Burden of Diabetes. Healthcare 2022, 10, 1459. [Google Scholar] [CrossRef] [PubMed]
- National Diabetes Statistics Report | Diabetes | CDC. Available online: https://www.cdc.gov/diabetes/data/statistics-report/index.html (accessed on 10 February 2024).
- Europe Diabetes Report 2000–2045. Available online: https://www.diabetesatlas.org/data/ (accessed on 10 February 2024).
- Russell-Jones, D.; Pouwer, F.; Khunti, K. Identification of Barriers to Insulin Therapy and Approaches to Overcoming Them. Diabetes Obes. Metab. 2018, 20, 488–496. [Google Scholar] [CrossRef]
- Khunti, K.; Gomes, M.B.; Pocock, S.; Shestakova, M.V.; Pintat, S.; Fenici, P.; Hammar, N.; Medina, J. Therapeutic Inertia in the Treatment of Hyperglycaemia in Patients with Type 2 Diabetes: A Systematic Review. Diabetes Obes. Metab. 2018, 20, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Boye, K.S.; Curtis, S.E.; Lage, M.J.; Garcia-Perez, L.-E. Associations between Adherence and Outcomes among Older, Type 2 Diabetes Patients: Evidence from a Medicare Supplemental Database. Patient Prefer. Adherence 2016, 10, 1573–1581. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, L.A.; Morris, A.D.; Evans, J.M.M.; DARTS/MEMO Collaboration. Adherence to Insulin and Its Association with Glycaemic Control in Patients with Type 2 Diabetes. J. Assoc. Physicians 2007, 100, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Kuritzky, L.; Reid, T.S.; Wysham, C.H. Practical Guidance on Effective Basal Insulin Titration for Primary Care Providers. Clin. Diabetes 2019, 37, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Peyrot, M.; Rubin, R.R.; Kruger, D.F.; Travis, L.B. Correlates of Insulin Injection Omission. Diabetes Care 2010, 33, 240–245. [Google Scholar] [CrossRef]
- Peyrot, M.; Barnett, A.H.; Meneghini, L.F.; Schumm-Draeger, P.-M. Factors Associated with Injection Omission/Non-Adherence in the Global Attitudes of Patients and Physicians in Insulin Therapy Study. Diabetes Obes. Metab. 2012, 14, 1081–1087. [Google Scholar] [CrossRef] [PubMed]
- Sugumar, V.; Ang, K.P.; Alshanon, A.F.; Sethi, G.; Yong, P.V.C.; Looi, C.Y.; Wong, W.F. A Comprehensive Review of the Evolution of Insulin Development and Its Delivery Method. Pharmaceutics 2022, 14, 1406. [Google Scholar] [CrossRef]
- Qiao, Q.; Ouwens, M.J.; Grandy, S.; Johnsson, K.; Kostev, K. Adherence to GLP-1 Receptor Agonist Therapy Administered by Once-Daily or Once-Weekly Injection in Patients with Type 2 Diabetes in Germany. Diabetes Metab. Syndr. Obes. 2016, 9, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Chen, S.; Flood, E.; Shaunik, A.; Romero, B.; de la Cruz, M.; Alvarez, C.; Grandy, S. Glucagon-Like Peptide-1 Receptor Agonist Treatment Attributes Important to Injection-Experienced Patients with Type 2 Diabetes Mellitus: A Preference Study in Germany and the United Kingdom. Diabetes Ther. 2017, 8, 335–353. [Google Scholar] [CrossRef] [PubMed]
- Weeda, E.R.; Muraoka, A.K.; Brock, M.D.; Cannon, J.M. Medication Adherence to Injectable Glucagon-like Peptide-1 (GLP-1) Receptor Agonists Dosed Once Weekly vs Once Daily in Patients with Type 2 Diabetes: A Meta-Analysis. Int. J. Clin. Pract. 2021, 75, e14060. [Google Scholar] [CrossRef] [PubMed]
- Weiss, T.; Carr, R.D.; Pal, S.; Yang, L.; Sawhney, B.; Boggs, R.; Rajpathak, S.; Iglay, K. Real-World Adherence and Discontinuation of Glucagon-Like Peptide-1 Receptor Agonists Therapy in Type 2 Diabetes Mellitus Patients in the United States. Patient Prefer. Adherence 2020, 14, 2337–2345. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, J.; Bajaj, H.S.; Janež, A.; Silver, R.; Begtrup, K.; Hansen, M.V.; Jia, T.; Goldenberg, R.; NN1436-4383 Investigators. Once-Weekly Insulin for Type 2 Diabetes without Previous Insulin Treatment. N. Engl. J. Med. 2020, 383, 2107–2116. [Google Scholar] [CrossRef] [PubMed]
- Skyler, J.S. Weekly Insulin Becoming a Reality. Diabetes Care 2021, 44, 1459–1461. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Colomba, D.; Arnone, S.; Argano, C.; Di Chiara, T.; Scaglione, R.; Licata, G. Improving Efficacy of PubMed Clinical Queries for Retrieving Scientifically Strong Studies on Treatment. J. Am. Med. Inf. Assoc. 2006, 13, 485–487. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Colomba, D.; Argano, C.; Calvo, L.; Scaglione, R.; Licata, G. Optimized Search Strategy for Detecting Scientifically Strong Studies on Treatment through PubMed. Intern. Emerg. Med. 2012, 7, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Haynes, R.B.; McKibbon, K.A.; Wilczynski, N.L.; Walter, S.D.; Werre, S.R.; Hedges Team. Optimal Search Strategies for Retrieving Scientifically Strong Studies of Treatment from Medline: Analytical Survey. BMJ 2005, 330, 1179. [Google Scholar] [CrossRef] [PubMed]
- Rubino, A.; McQuay, L.J.; Gough, S.C.; Kvasz, M.; Tennis, P. Delayed Initiation of Subcutaneous Insulin Therapy after Failure of Oral Glucose-Lowering Agents in Patients with Type 2 Diabetes: A Population-Based Analysis in the UK. Diabet. Med. 2007, 24, 1412–1418. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, W.H.; Fisher, L.; Hessler, D.; Bruhn, D.; Best, J.H. Patient Perspectives on Once-Weekly Medications for Diabetes. Diabetes Obes. Metab. 2011, 13, 144–149. [Google Scholar] [CrossRef]
- Paley, R.G.; Scott, M.H. Severe Insulin Lipodystrophy as a Possible Cause of Instability in Diabetics. Br. Med. J. 1958, 2, 1331–1334. [Google Scholar] [CrossRef] [PubMed]
- Watson, E.M. Non-Hypoglycaemic (Allergic) Insulin Reactions. Can. Med. Assoc. J. 1942, 47, 336–339. [Google Scholar] [PubMed]
- American Diabetes Association 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S98–S110. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, W.H.; Henry, R.R. Poor Medication Adherence in Type 2 Diabetes: Recognizing the Scope of the Problem and Its Key Contributors. Patient Prefer. Adherence 2016, 10, 1299–1307. [Google Scholar] [CrossRef]
- Howard, V.; Church, C.; Oldham, S.; Hornigold, D.; Trevaskis, J.; Baker, D.; Rhodes, C.; Rossi, A.; Naylor, J.; Dhillon, J.; et al. 1086-P: Preclinical Development of an Ultralong-Acting Insulin for Once-Weekly Dosing. Diabetes 2019, 68, 1086-P. [Google Scholar] [CrossRef]
- Rezolute, Inc. Announces Top-Line Results from Phase 1 Trial Evaluating AB101 in Patients with Diabetes. Available online: https://www.biospace.com/article/rezolute-inc-announces-top-line-results-from-phase-1-trial-evaluating-ab101-in-patients-with-diabetes-/ (accessed on 17 February 2024).
- Insulin Long-Acting (HM 12470)—Hanmi Pharmaceutical—AdisInsight. Available online: https://adisinsight.springer.com/drugs/800040862 (accessed on 17 February 2024).
- Hanmi | Hanmi Pharmaceutical’s Official Site. Available online: https://www.hanmipharm.com/main.hm (accessed on 17 February 2024).
- Kurtzhals, P.; Nishimura, E.; Haahr, H.; Høeg-Jensen, T.; Johansson, E.; Madsen, P.; Sturis, J.; Kjeldsen, T. Commemorating Insulin’s Centennial: Engineering Insulin Pharmacology towards Physiology. Trends Pharmacol. Sci. 2021, 42, 620–639. [Google Scholar] [CrossRef] [PubMed]
- Marquez, F.; Brazg, R.; Christiansen, M.; Free, A.; Matson, M.; Jones, S.; Georgopoulos, L.; Malatesta, J.; Arnold, S.; Kramer, W.; et al. PE0139, the First Recombinant Fully Human Monomeric Super-Long-Acting Basal Insulin to Display a Sustained Nearly Peakless Insulin Profile Following a Single Subcutaneous Dose in Subjects with T2DM Supporting Weekly Dosing. In Proceedings of the 75th Scientific Sessions of the American Diabetes Association, Boston, MA, USA, 5–9 June 2014; p. A26. [Google Scholar]
- Moyers, J.S.; Hansen, R.J.; Day, J.W.; Dickinson, C.D.; Zhang, C.; Ruan, X.; Ding, L.; Brown, R.M.; Baker, H.E.; Beals, J.M. Preclinical Characterization of LY3209590, a Novel Weekly Basal Insulin Fc-Fusion Protein. J. Pharmacol. Exp. Ther. 2022, 382, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Heise, T.; Chien, J.; Beals, J.M.; Benson, C.; Klein, O.; Moyers, J.S.; Haupt, A.; Pratt, E.J. Pharmacokinetic and Pharmacodynamic Properties of the Novel Basal Insulin Fc (Insulin Efsitora Alfa), an Insulin Fusion Protein in Development for Once-Weekly Dosing for the Treatment of Patients with Diabetes. Diabetes Obes. Metab. 2023, 25, 1080–1090. [Google Scholar] [CrossRef] [PubMed]
- Philis-Tsimikas, A.; Bajaj, H.S.; Begtrup, K.; Cailleteau, R.; Gowda, A.; Lingvay, I.; Mathieu, C.; Russell-Jones, D.; Rosenstock, J. Rationale and Design of the Phase 3a Development Programme (ONWARDS 1-6 Trials) Investigating Once-Weekly Insulin Icodec in Diabetes. Diabetes Obes. Metab. 2023, 25, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, E.; Pridal, L.; Glendorf, T.; Hansen, B.F.; Hubálek, F.; Kjeldsen, T.; Kristensen, N.R.; Lützen, A.; Lyby, K.; Madsen, P.; et al. Molecular and Pharmacological Characterization of Insulin Icodec: A New Basal Insulin Analog Designed for Once-Weekly Dosing. BMJ Open Diabetes Res. Care 2021, 9, e002301. [Google Scholar] [CrossRef] [PubMed]
- Danne, T.; Heinemann, L.; Pieber, T.R. New Insulins, Biosimilars, and Insulin Therapy. Diabetes Technol. Ther. 2023, 25, S44–S69. [Google Scholar] [CrossRef] [PubMed]
- Belal, H.; Gandhi, G.Y. In T2DM Uncontrolled with Noninsulin Glucose-Lowering Agents, Weekly Icodec Reduced HbA1c vs. Daily Degludec at 26 Wk. Ann. Intern. Med. 2023, 176, JC112. [Google Scholar] [CrossRef] [PubMed]
- Lingvay, I.; Asong, M.; Desouza, C.; Gourdy, P.; Kar, S.; Vianna, A.; Vilsbøll, T.; Vinther, S.; Mu, Y. Once-Weekly Insulin Icodec vs Once-Daily Insulin Degludec in Adults with Insulin-Naive Type 2 Diabetes: The ONWARDS 3 Randomized Clinical Trial. JAMA 2023, 330, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Bue-Valleskey, J.M.; Kazda, C.M.; Ma, C.; Chien, J.; Zhang, Q.; Chigutsa, E.; Landschulz, W.; Haupt, A.; Frias, J.P. Once-Weekly Basal Insulin Fc Demonstrated Similar Glycemic Control to Once-Daily Insulin Degludec in Insulin-Naive Patients with Type 2 Diabetes: A Phase 2 Randomized Control Trial. Diabetes Care 2023, 46, 1060–1067. [Google Scholar] [CrossRef]
- Roussel, R.; Charbonnel, B.; Behar, M.; Gourmelen, J.; Emery, C.; Detournay, B. Persistence with Insulin Therapy in Patients with Type 2 Diabetes in France: An Insurance Claims Study. Diabetes Ther. 2016, 7, 537–549. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, D.G.; Ozcan, S.; Deyneli, O. Adherence to Insulin Treatment in Insulin-Naïve Type 2 Diabetic Patients Initiated on Different Insulin Regimens. Patient Prefer. Adherence 2015, 9, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Morrison, F.; Zhao, Z.; Haynes, G.; He, X.; Ali, A.K.; Shubina, M.; Malmasi, S.; Ge, W.; Peng, X.; et al. Reasons for Discontinuing Insulin and Factors Associated with Insulin Discontinuation in Patients with Type 2 Diabetes Mellitus: A Real-World Evidence Study. Clin. Diabetes Endocrinol. 2021, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, J.; Bain, S.C.; Gowda, A.; Jódar, E.; Liang, B.; Lingvay, I.; Nishida, T.; Trevisan, R.; Mosenzon, O.; ONWARDS 1 Trial Investigators. Weekly Icodec versus Daily Glargine U100 in Type 2 Diabetes without Previous Insulin. N. Engl. J. Med. 2023, 389, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Philis-Tsimikas, A.; Asong, M.; Franek, E.; Jia, T.; Rosenstock, J.; Stachlewska, K.; Watada, H.; Kellerer, M. Switching to Once-Weekly Insulin Icodec versus Once-Daily Insulin Degludec in Individuals with Basal Insulin-Treated Type 2 Diabetes (ONWARDS 2): A Phase 3a, Randomised, Open Label, Multicentre, Treat-to-Target Trial. Lancet Diabetes Endocrinol. 2023, 11, 414–425. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Zhang, Y.; Xu, W.; He, J.; Peng, L.; Feng, Y.; Xu, P.; Chong, W.; Hai, Y.; Jia, L.; et al. Efficacy and Safety of Once-Weekly Insulin Regimes on Glycemic Control for Type 2 Diabetes: A Systematic Review and Network Meta-Analysis. Diabetol. Metab. Syndr. 2024, 16, 3. [Google Scholar] [CrossRef] [PubMed]
- Frias, J.; Chien, J.; Zhang, Q.; Chigutsa, E.; Landschulz, W.; Syring, K.; Wullenweber, P.; Haupt, A.; Kazda, C. Safety and Efficacy of Once-Weekly Basal Insulin Fc in People with Type 2 Diabetes Previously Treated with Basal Insulin: A Multicentre, Open-Label, Randomised, Phase 2 Study. Lancet Diabetes Endocrinol. 2023, 11, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Lingvay, I.; Buse, J.B.; Franek, E.; Hansen, M.V.; Koefoed, M.M.; Mathieu, C.; Pettus, J.; Stachlewska, K.; Rosenstock, J. A Randomized, Open-Label Comparison of Once-Weekly Insulin Icodec Titration Strategies Versus Once-Daily Insulin Glargine U100. Diabetes Care 2021, 44, 1595–1603. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Nobili, A.; Natoli, G.; Mannucci, P.M.; Perticone, F.; Pietrangelo, A.; Argano, C.; REPOSI Investigators. Hyperglycemia at admission, comorbidities, and in-hospital mortality in elderly patients hospitalized in internal medicine wards: Data from the RePoSI Registry. Acta Diabetol. 2021, 58, 1225–1236, Correction in Acta Diabetol. 2021, 58, 1237. [Google Scholar] [CrossRef]
- Candido, R.; Nicolucci, A.; Larosa, M.; Rossi, M.C.; Napoli, R.; Gabellieri, E.; Tortato, E.; Rabini, R.A.; Crazzolara, D.; Lucibelli, L.; et al. Treatment Intensification Following Glucagon-like Peptide-1 Receptor Agonist Treatment in Type 2 Diabetes: The RESTORE-G Real-World Study. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 2294–2305. [Google Scholar] [CrossRef]
- Guerci, B.; Chanan, N.; Kaur, S.; Jasso-Mosqueda, J.G.; Lew, E. Lack of Treatment Persistence and Treatment Nonadherence as Barriers to Glycaemic Control in Patients with Type 2 Diabetes. Diabetes Ther. 2019, 10, 437–449. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, J.; Del Prato, S. Basal Weekly Insulins: The Way of the Future! Metabolism 2022, 126, 154924. [Google Scholar] [CrossRef] [PubMed]
- Baser, O.; Tangirala, K.; Wei, W.; Xie, L. Real-World Outcomes of Initiating Insulin Glargine-Based Treatment versus Premixed Analog Insulins among US Patients with Type 2 Diabetes Failing Oral Antidiabetic Drugs. Clin. Outcomes Res. 2013, 5, 497–505. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mathieu, C.; Ásbjörnsdóttir, B.; Bajaj, H.S.; Lane, W.; Matos, A.L.S.A.; Murthy, S.; Stachlewska, K.; Rosenstock, J. Switching to Once-Weekly Insulin Icodec versus Once-Daily Insulin Glargine U100 in Individuals with Basal-Bolus Insulin-Treated Type 2 Diabetes (ONWARDS 4): A Phase 3a, Randomised, Open-Label, Multicentre, Treat-to-Target, Non-Inferiority Trial. Lancet 2023, 401, 1929–1940. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, H.S.; Aberle, J.; Davies, M.; Donatsky, A.M.; Frederiksen, M.; Yavuz, D.G.; Gowda, A.; Lingvay, I.; Bode, B. Once-Weekly Insulin Icodec with Dosing Guide App versus Once-Daily Basal Insulin Analogues in Insulin-Naive Type 2 Diabetes (ONWARDS 5): A Randomized Trial. Ann. Intern. Med. 2023, 176, 1476–1485. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, M.J.; Dinneen, S.F. In Type 2 Diabetes, Weekly Basal Insulin Fc Was Noninferior to Daily Insulin Degludec for HbA1c at 26 Wk. Ann. Intern. Med. 2023, 176, JC81. [Google Scholar] [CrossRef] [PubMed]
- Kazda, C.M.; Bue-Valleskey, J.M.; Chien, J.; Zhang, Q.; Chigutsa, E.; Landschulz, W.; Wullenweber, P.; Haupt, A.; Dahl, D. Novel Once-Weekly Basal Insulin Fc Achieved Similar Glycemic Control with a Safety Profile Comparable to Insulin Degludec in Patients with Type 1 Diabetes. Diabetes Care 2023, 46, 1052–1059. [Google Scholar] [CrossRef] [PubMed]
- Russell-Jones, D.; Babazono, T.; Cailleteau, R.; Engberg, S.; Irace, C.; Kjaersgaard, M.I.S.; Mathieu, C.; Rosenstock, J.; Woo, V.; Klonoff, D.C. Once-Weekly Insulin Icodec versus Once-Daily Insulin Degludec as Part of a Basal-Bolus Regimen in Individuals with Type 1 Diabetes (ONWARDS 6): A Phase 3a, Randomised, Open-Label, Treat-to-Target Trial. Lancet 2023, 402, 1636–1647. [Google Scholar] [CrossRef] [PubMed]
- Fifer, S.; Rose, J.; Hamrosi, K.K.; Swain, D. Valuing Injection Frequency and Other Attributes of Type 2 Diabetes Treatments in Australia: A Discrete Choice Experiment. BMC Health Serv. Res. 2018, 18, 675. [Google Scholar] [CrossRef] [PubMed]
- Blonde, L.; Meneghini, L.; Peng, X.V.; Boss, A.; Rhee, K.; Shaunik, A.; Kumar, S.; Balodi, S.; Brulle-Wohlhueter, C.; McCrimmon, R.J. Probability of Achieving Glycemic Control with Basal Insulin in Patients with Type 2 Diabetes in Real-World Practice in the USA. Diabetes Ther. 2018, 9, 1347–1358. [Google Scholar] [CrossRef] [PubMed]
- Khunti, K.; Nikolajsen, A.; Thorsted, B.L.; Andersen, M.; Davies, M.J.; Paul, S.K. Clinical Inertia with Regard to Intensifying Therapy in People with Type 2 Diabetes Treated with Basal Insulin. Diabetes Obes. Metab. 2016, 18, 401. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Zhang, H.; Li, X.; Chen, M.; Wang, D.; Ji, L. Factors and Outcomes Associated with Discontinuation of Basal Insulin Therapy in Patients with Type 2 Diabetes Mellitus. Endocrinol. Diabetes Metab. 2020, 3, e00122. [Google Scholar] [CrossRef] [PubMed]
- Khunti, K.; Giorgino, F.; Berard, L.; Mauricio, D.; Harris, S.B. The Importance of the Initial Period of Basal Insulin Titration in People with Diabetes. Diabetes Obes. Metab. 2020, 22, 722–733. [Google Scholar] [CrossRef] [PubMed]
- Abuelazm, M.; Ibrahim, A.A.; Khlidj, Y.; Badr, A.; Amin, A.M.; Elzeftawy, M.A.; Gowaily, I.; Elsaeidy, A.S.; Abdelazeem, B. Once-weekly Insulin Icodec versus Once-daily Long-acting Insulin for Type II Diabetes: A Meta-analysis of Randomized Controlled Trials. J. Endocr. Soc. 2023, 8, bvad177. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, H.S.; Bergenstal, R.M.; Christoffersen, A.; Davies, M.J.; Gowda, A.; Isendahl, J.; Lingvay, I.; Senior, P.A.; Silver, R.J.; Trevisan, R.; et al. Switching to Once-Weekly Insulin Icodec versus Once-Daily Insulin Glargine U100 in Type 2 Diabetes Inadequately Controlled on Daily Basal Insulin: A Phase 2 Randomized Controlled Trial. Diabetes Care 2021, 44, 1586–1594. [Google Scholar] [CrossRef] [PubMed]
- Sciacca, L.; Vella, V.; Frittitta, L.; Tumminia, A.; Manzella, L.; Squatrito, S.; Belfiore, A.; Vigneri, R. Long-actinginsulinanalogs and cancer. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Aktas, G.; Taslamacioglu Duman, T. Current usage of long-acting insulin analogs in patients with type 2 diabetes mellitus. Expert Rev. Endocrinol. Metab. 2024, 19, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Argano, C.; Natoli, G.; Nobili, A.; Corazza, G.R.; Mannucci, P.M.; Perticone, F.; REPOSI Investigators. Sex-Differences in the Pattern of Comorbidities, Functional Independence, and Mortality in Elderly Inpatients: Evidence from the RePoSI Register. J. Clin. Med. 2019, 8, 81. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Insulin Fc vs. Degludec in DMt2 Patients Previously Treated with Basal Insulin [40] | Insulin Fc vs. Degludec in DMt2 Patients Insulino-Naïve [43] | Insulin Fc vs. Degludec in DMt1 Patients [44] | |
|---|---|---|---|
| Study design |
|
|
|
| Period | November 2018–February 2020 | 5 March 2021–19 July 2023 | 6 June 2020–22 January 2021 |
| Endpoint I | HbA1c reduction at 32 weeks | HbA1c reduction at 26 weeks | HbA1c reduction at 26 weeks |
| Endpoint II |
|
|
|
| Titration protocol | The loading and initial weekly doses were based on their previous daily basal insulin dose and their glycemic control according to baseline HbA1c (using a threshold of 8.5. BIF dosing in the Phase 2 program used mg increments and not insulin international units (IU)) | Initial dose 10 IU/day (70 IU/week for icodec) Weekly titration on average FPG of the last 3 days Target: FPG 80–130 mg/dL | Titration was based on mean fasting blood glucose levels using CGM measurements on at least 3 days of the week using a paper-based algorithm. BIF was titrated weekly for weeks 1–12 and then every 4 weeks until the end of the treatment period |
| Numbers of patients |
|
|
|
| Population |
|
|
|
| Results |
|
|
|
| Hypoglycemic events | The event rates of all documented hypoglycemia were about 25% lower in the Fc groups, and those for nocturnal hypoglycemia were at least 33% lower from baseline to week 32 compared with insulin degludec | The rate of severe hypoglycemic events was not significant between treatment groups (p 0.64) | Hypoglycemia occurrence over 24 h was similar for BIF and degludec for level 1 (p = 0.960) or level 2 (p = 0.517) hypoglycemia during treatment. The occurrence of serious adverse events was similar between the BIF and degludec groups. |
| Adverse events | Mostly mild/moderate events and not associated with treatment Deaths: 3 (2%) in degludec, 1 (1%) in glargine No reactions at the injection site or critical issues related to medication errors described | Mostly mild/moderate events and not associated with treatment: Fc 5.6% (n = 143) Degludec 3% (n = 135) Deaths: 2 (1%) in Fc, 3 (1.5%) in degludec | Mostly mild/moderate events and not associated with treatment. The occurrence of serious adverse events was similar between the BIF and degludec groups. |
| ONWARDS 1 Icodec vs. Glargine U100 in DT2 Insulino-Naïve [45] | ONWARDS 2 Icodec vs. Degludec U100 in Basal Bolus [46] | ONWARDS 3 Icodec vs. Degludec in DT2 Insulino-Naïve [47] | ONWARDS 4 Icodec vs. Glargine U100 in DT2 in Basal Bolus [48] | ONWARDS 5 Icodec vs. Once-Daily Insulin in DT2 Insulino-Naïve with Dosing Guide App [49] | ONWARDS 6 Icodec vs. Degludec in T1D [50] | |
|---|---|---|---|---|---|---|
| Study design |
|
|
|
|
|
|
| Period | November 2020–May 2023 | 5 March 2021–19 July 2023 | March 2021–June 2022 | March 2021–October 2021 | 1 March 2021–12 August 2022 | 30 April 2021–15 October 2021 |
| Endpoint I | HbA1c reduction at 52 weeks | HbA1c reduction at 26 weeks | HbA1c reduction at 26 weeks | HbA1c reduction at 26 weeks | HbA1c reduction at 52 weeks | HbA1c reduction at 26 weeks |
| Endpoint II |
|
|
|
|
|
|
| Titration protocol | Initial dose of 10 IU/day (70 IU/week for icodec) Weekly titration on average FPG of the last 3 days Target: FPG 80–130 mg/dL | Initial dose of 10 IU/day (70 IU/week for icodec) Weekly titration on average FPG of the last 3 days Target: FPG 80–130 mg/dL | Initial dose of 10 IU/day (70 IU/week for icodec) Weekly titration on average FPG of the last 3 days Target: FPG 80–130 mg/dL Increments of 3 IU/day (20 IU/week for icodec) | Initial dose of 10 IU/day (70 IU/week for icodec) Weekly titration on average FPG of the last 3 days Target: FPG 80–130 mg/dL | Icodec titrated with a dosing guide app (icodec with app) | Initial dose of 10 IU/day (70 IU/week for icodec) Weekly titration on average FPG of the last 3 days Target: FPG 80–130 mg/dL Increments of 3 IU/day (20 IU/week for icodec) |
| Numbers of patients |
|
|
|
|
|
|
| Population |
|
|
|
|
|
|
| Results |
|
|
| At week 26, the mean change in HbA1c was −1.16 percentage points in the icodec group (baseline 8.29%) and −1.18 percentage points in the glargine U100 group (baseline 8.31%). Combined level 2 and level 3 hypoglycemia rates were similar between treatment groups. | At week 52, insulin icodec used in conjunction with the dosing guide app demonstrated non-inferiority and superiority versus the basal insulin analogues in reducing the estimated mean HbA1c from baseline |
|
| Hypoglycemic events | Icodecs:
Glargine:
| Clinically significant hypoglycemia rates were not significant between the two groups at week 31 | Icodecs:
Degludec:
| Icodecs:
Degludec U100:
| Clinically significant or severe hypoglycemia rates were not significantly different between the treatment groups at week 57 | Icodecs:
Degludec:
|
| Adverse events | Mostly mild/moderate events and not associated with treatment Deaths: 5 in icodec, 4 in glargine No reactions at the injection site or critical issues related to medication errors described | Mostly mild/moderate events and not associated with treatment Deaths: 5 in icodec, 4 in glargine No reactions at the injection site or critical issues related to medication errors described | Mostly mild/moderate events and not associated with treatment Deaths: 2 in icodec, 1 in degludec 8.5 vs. 4.4% injection site reactions for icodec vs. degludec Usage errors <5% | Mostly mild/moderate events and not associated with treatment No reactions at the injection site or critical issues related to medication errors described | Mostly mild/moderate events and not associated with treatment No reactions at the injection site or critical issues related to medication errors described | Mostly mild/moderate events and not associated with treatment Deaths: 1 in icodec, 0 in degludec 0.07% vs. 0.06% injection site reactions for icodec vs. degludec |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Argano, C.; Priola, L.; Manno, F.; Corrao, S. What Is the Role of Basal Weekly Insulin in Clinical Practice? The State of the Art. Biomedicines 2024, 12, 900. https://doi.org/10.3390/biomedicines12040900
Argano C, Priola L, Manno F, Corrao S. What Is the Role of Basal Weekly Insulin in Clinical Practice? The State of the Art. Biomedicines. 2024; 12(4):900. https://doi.org/10.3390/biomedicines12040900
Chicago/Turabian StyleArgano, Christiano, Laura Priola, Francesco Manno, and Salvatore Corrao. 2024. "What Is the Role of Basal Weekly Insulin in Clinical Practice? The State of the Art" Biomedicines 12, no. 4: 900. https://doi.org/10.3390/biomedicines12040900
APA StyleArgano, C., Priola, L., Manno, F., & Corrao, S. (2024). What Is the Role of Basal Weekly Insulin in Clinical Practice? The State of the Art. Biomedicines, 12(4), 900. https://doi.org/10.3390/biomedicines12040900