
Long-Term Outcome of Lower Extremity Bypass Surgery in Diabetic and Non-Diabetic Patients with Critical Limb-Threatening Ischaemia in Germany
 ,
on behalf of the DIGG
,
on behalf of the DIGG
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Statistics
3. Results
3.1. Patients
3.2. Perioperative Outcome
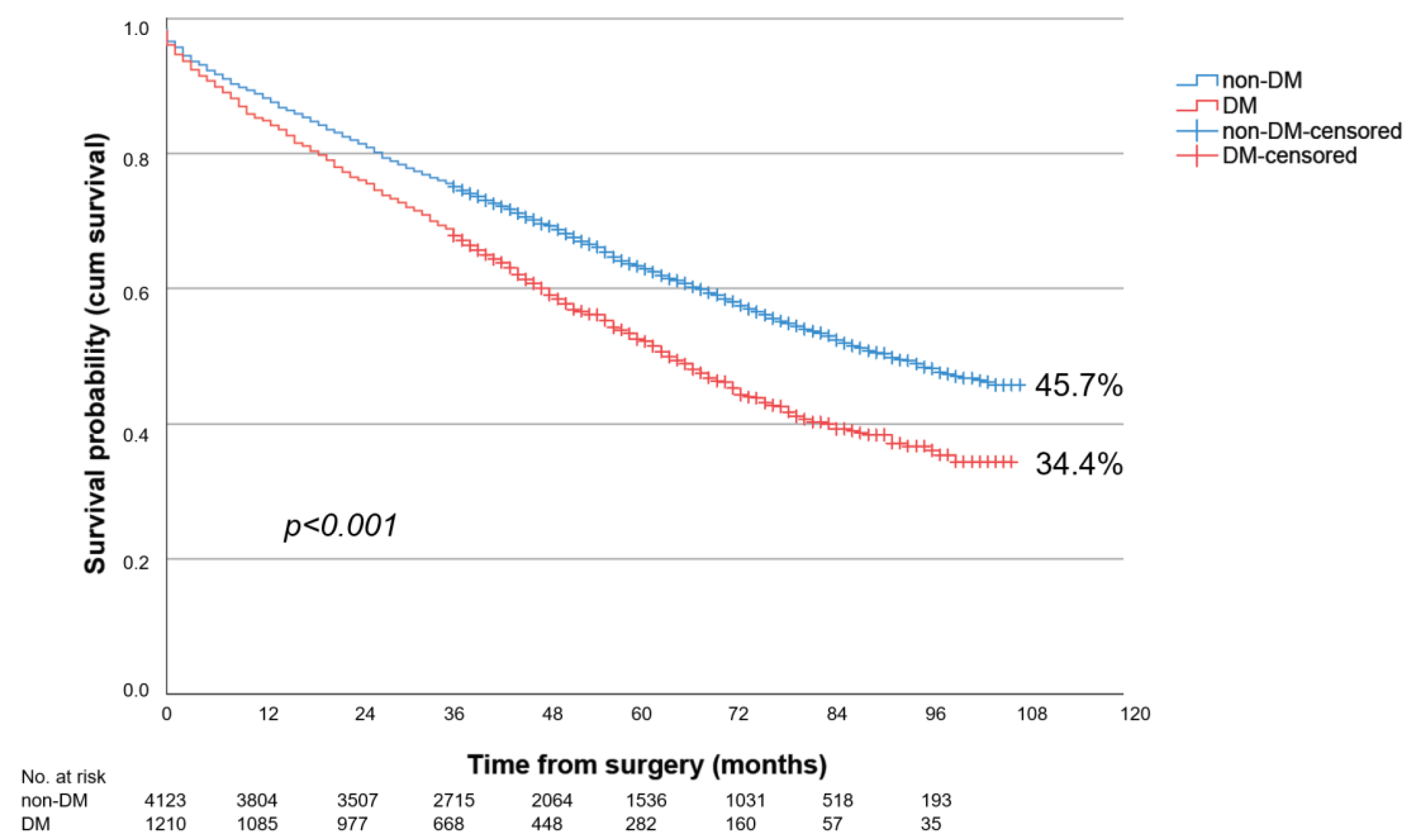
3.3. Long-Term Survival in PAD Stages III and IV
3.4. Long-Term Survival Depending on Bypass Level
3.5. Major Amputation Rates during Follow-Up in PAD Stages III and IV
3.6. Major Amputation Rates during Follow-Up Depending on Bypass Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wallaert, J.B.; Nolan, B.W.; Adams, J.; Stanley, A.C.; Eldrup-Jorgensen, J.; Cronenwett, J.L.; Goodney, P.P. The impact of diabetes on postoperative outcomes following lower-extremity bypass surgery. J. Vasc. Surg. 2012, 56, 1317–1323. [Google Scholar] [CrossRef] [PubMed]
- Darling, J.D.; Bodewes, T.C.F.; Deery, S.E.; Guzman, R.J.; Wyers, M.C.; Hamdan, A.D.; Verhagen, H.J.; Schermerhorn, M.L. Outcomes after first-time lower extremity revascularization for chronic limb-threatening ischemia between patients with and without diabetes. J. Vasc. Surg. 2018, 67, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- Hicks, C.W.; Najafian, A.; Farber, A.; Menard, M.T.; Malas, M.B.; Black, J.H., 3rd; Abularrage, C.J. Diabetes does not worsen outcomes following infrageniculate bypass or endovascular intervention for patients with critical limb ischemia. J. Vasc. Surg. 2016, 64, 1667–1674. [Google Scholar] [CrossRef] [PubMed]
- Hertzer, N.R.; Bena, J.F.; Karafa, M.T. A personal experience with the influence of diabetes and other factors on the outcome of infrainguinal bypass grafts for occlusive disease. J. Vasc. Surg. 2007, 462, 271–279. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lilja, E.; Gottsäter, A.; Miftaraj, M.; Ekelund, J.; Eliasson, B.; Sensson, A.M.; Zarrouk, M.; Acosta, S. Diabetes mellitus was not associated with lower amputation-free survival after open revascularization for chronic limb-threatening ischemia—A nationwide propensity score adjusted analysis. Vasc. Med. 2021, 26, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Lazaris, A.M.; Kontopantelis, E.; Antonopoulos, K.; Mantas, G.; Kouvelos, G.; Moulakakis, K.; Matsagkas, M.I.; Vasdekis, S.N.; Geroulakos, G. Effect of diabetes mellitus on the clinical outcome of lower limb arterial bypass surgery: A propensity score analysis. Vascular 2017, 25, 364–371. [Google Scholar] [CrossRef] [PubMed]
- AhChong, A.K.; Chiu, K.M.; Wong, M.W.; Hui, H.K.; Yip, A.W. Diabetes and the outcome of infrainguinal bypass for critical limb ischaemia. ANZ J. Surg. 2004, 74, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Ballotta, E.; Toniato, A.; Piatto, G.; Mazzalai, F.; Da Giau, G. Lower extremity arterial reconstruction for critical limb ischemia in diabetes. J. Vasc. Surg. 2014, 59, 708–719. [Google Scholar] [CrossRef] [PubMed]
- McGinigle, K.L.; Kindell, D.G.; Strassle, P.D.; Crowner, J.R.; Pascarella, L.; Farber, M.A.; Marston, W.A.; Arya, S.; Kalbaugh, C.A. Poor glycemic control is associated with significant increase in major limb amputation and adverse events in the 30-day postoperative period after infrainguinal bypass. J. Vasc. Surg. 2020, 72, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Zeng, C.; Lewinger, J.P.; Wolfson, A.M.; Shavelle, D.; Weaver, F.; Garg, P.K. Preoperative hemoglobin A1c levels and increased risk of adverse limb events in diabetic patients undergoing infrainguinal lower extremity bypass surgery in the Vascular Quality Initiative. J. Vasc. Surg. 2019, 70, 1225–1234.e1. [Google Scholar] [CrossRef] [PubMed]
- Elbadawi, A.; Elgendy, I.Y.; Saad, M.; Elzeneini, M.; Megaly, M.; Omer, M.; Banerjee, S.; Drachman, D.E.; Aronow, H.D. Contemporary Revascularization Strategies and Outcomes Among Patients with Diabetes with Critical Limb Ischemia: Insights from the National Inpatient Sample. JACC Cardiovasc. Interv. 2021, 14, 664–674. [Google Scholar] [CrossRef] [PubMed]
- De Donato, G.; Benedetto, F.; Stilo, F.; Chiesa, R.; Palombo, D.; Pasqui, E.; Panzano, C.; Pulli, R.; Novali, C.; Silingardi, R.; et al. Evaluation of Clinical Outcomes After Revascularization in Patients with Chronic Limb-Threatening Ischemia: Results from a Prospective National Cohort Study (RIVALUTANDO). Angiology 2021, 72, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Fernando, M.E.; Blanchette, V.; Mishra, R.; Zulbaran-Rojas, A.; Rowe, V.; Mills, J.L.; Armstrong, D.G.; Najafi, B. Frailty in People with Chronic Limb Threatening Ischemia and Diabetes-Related Foot Ulcers: A Systematic Review. Ann. Vasc. Surg. 2023, 89, 322–337. [Google Scholar] [CrossRef] [PubMed]
- Malyar, N.M.; Freisinger, E.; Meyborg, M.; Lüders, F.; Gebauer, K.; Reinecke, H.; Lawall, H. Amputations and mortality in in-hospital treated patients with peripheral artery disease and diabetic foot syndrome. J. Diabetes Complicat. 2016, 30, 1117–1122. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Non-DM n = 15,367 | DM n = 7266 | p Value | |
|---|---|---|---|
| Male sex, n (%) | 9930 (64.6) | 4593 (63.2) | 0.040 |
| Female sex, n (%) | 5437 (35.4) | 2673 (36.8) | 0.040 |
| PAD Fontaine stage III, n (%) | 4641 (30.2) | 1419 (19.5) | <0.001 |
| PAD Fontaine stage IV, n (%) | 10,726 (69.8) | 5847 (80.5) | <0.001 |
| Bypass above-the-knee PAD III, n (%) | 1735 (37.4) | 564 (39.7) | 0.109 |
| Bypass below-the-knee PAD III, n (%) | 1525 (32.9) | 438 (30.9) | 0.160 |
| Bypass crural/pedal PAD III, n (%) | 1381 (29.8) | 417 (29.4) | 0.790 |
| Bypass above-the-knee PAD IV, n (%) | 3292 (30.7) | 1655 (28.3) | 0.001 |
| Bypass below-the-knee PAD IV, n (%) | 3232 (30.1) | 1634 (27.9) | 0.003 |
| Bypass crural/pedal PAD IV, n (%) | 4202 (39.2) | 2558 (43.7) | <0.001 |
| Age, mean ± SD in years; median (min-max) | 72.2 ± 10.8; 73 (19–101) | 73.2 ± 9.7; 74 (28–100) | <0.001 |
| Age men, mean ± SD in years; median (min-max) | 69.6 ± 10.3; 71 (19–99) | 71.3 ± 9.4; 73 (28–95) | <0.001 |
| Age women, mean ± SD in years; median (min-max) | 76.8 ± 10.3; 78 (27–101) | 76.5 ± 9.4; 78 (41–100) | 0.015 |
| Arterial hypertension, n (%) | 6154 (40.0) | 6017 (82.8) | <0.001 |
| Left heart failure (NYHA 2-4 and unspecified), n (%) | 1675 (10.9) | 2394 (32.9) | <0.001 |
| History of myocardial infarction, n (%) | 1058 (6.9) | 1487 (20.5) | <0.001 |
| History of stroke, n (%) | 450 (2.9) | 490 (6.7) | <0.001 |
| History of TIA, n (%) | 217 (1.4) | 192 (2.6) | <0.001 |
| COPD, n (%) | 1542 (10.0) | 1250 (17.2) | <0.001 |
| Renal insufficiency (stages 3–5), n (%) | 1707 (11.1) | 2655 (36.5) | <0.001 |
| Non-DM n = 15,367 | DM n = 7266 | p Value | |
|---|---|---|---|
| Perioperative mortality all patients, n (%) | 1259 (8.2) | 729 (10.0) | <0.001 |
| Perioperative mortality men, n (%) | 729/9930 (7.3) | 418/4593 (9.1) | <0.001 |
| Perioperative mortality women, n (%) | 530/5437 (9.7) | 311/2673 (11.6) | 0.009 |
| Perioperative mortality PAD III, n (%) | 199/4641 (4.3) | 76/1419 (5.4) | 0.091 |
| Perioperative mortality PAD IV, n (%) | 1060/10,726 (9.9) | 653/5847 (11.2) | 0.009 |
| Perioperative mortality above-the-knee bypass, n (%) | 317/5027 (6.3) | 178/2219 (8.0) | 0.008 |
| Perioperative mortality below-the-knee bypass, n (%) | 384/4757 (8.1) | 225/2072 (10.9) | <0.001 |
| Perioperative mortality crural/pedal bypass, n (%) | 558/5583 (10.0) | 326/2975 (11.0) | 0.163 |
| LOS, mean ± SD in days; median (min-max) | 25.6 ± 19.7; 20 (0–298) | 28.9 ± 22.2; 22 (1–232) | <0.001 |
| Major amputation, n (%) | 892 (5.8) | 539 (7.4) | <0.001 |
| Minor amputation, n (%) | 2676 (17.4) | 2103 (28.9) | <0.001 |
| Dialysis, n (%) | 478 (3.1) | 536 (7.4) | <0.001 |
| Blood transfusions, n (%) | 6027 (39.2) | 3613 (49.7) | <0.001 |
| Intensive care treatment, n (%) | 2607 (17.0) | 1587 (21.8) | <0.001 |
| Wound infections, n (%) | 1639 (10.7) | 868 (11.9) | 0.004 |
| Myocardial infarction, n (%) | 344 (2.2) | 223 (3.1) | <0.001 |
| Complication-free, n (%) | 10,636 (69.2) | 4100 (56.4) | <0.001 |
| Non-DM n = 15,367 | DM n = 7266 | p Value | |
|---|---|---|---|
| Survival all patients, n (%) | 6354 (31.1) | 2373 (21.5) | <0.001 |
| Survival PAD III, n (%) | 2652 (45.7) | 692 (34.3) | <0.001 |
| Survival PAD IV, n (%) | 3702 (25.0) | 1681 (18.5) | <0.001 |
| Survival above-the-knee bypass PAD III, n (%) | 1068 (49.4) | 290 (37.9) | <0.001 |
| Survival below-the-knee bypass PAD III, n (%) | 858 (45.5) | 211 (33.1) | <0.001 |
| Survival crural/pedal bypass PAD III, n (%) | 726 (41.3) | 191 (32.3) | 0.001 |
| Survival above-the-knee bypass PAD IV, n (%) | 1227 (27.0) | 518 (21.5) | <0.001 |
| Survival below-the-knee bypass PAD IV, n (%) | 1109 (23.4) | 474 (17.3) | <0.001 |
| Survival crural/pedal bypass PAD IV, n (%) | 1366 (24.3) | 689 (17.2) | <0.001 |
| HR | 95% CI | p Value | |
|---|---|---|---|
| Male gender (vs. female gender) | 1.16 | 1.12–1.21 | <0.001 |
| Age (increased by 1 year) | 1.04 | 1.04–1.05 | <0.001 |
| Bypass crural/pedal and below-the-knee (vs. above-the-knee) | 1.02 | 0.98–1.06 | 0.323 |
| PAD Fontaine stage IV (vs. III) | 1.62 | 1.55–1.69 | <0.001 |
| Diabetes mellitus type 2 | 1.10 | 1.05–1.14 | <0.001 |
| Left heart failure (NYHA 2-4 and unspecified) | 1.28 | 1.22–1.35 | <0.001 |
| COPD | 1.35 | 1.29–1.42 | <0.001 |
| Renal insufficiency (stages 3–5) | 1.44 | 1.38–1.51 | <0.001 |
| Arterial hypertension | 0.90 | 0.87–0.94 | <0.001 |
| History of myocardial infarction | 1.05 | 0.99–1.11 | 0.102 |
| History of stroke | 1.18 | 1.09–1.28 | <0.001 |
| Non-DM n = 15,367 | DM n = 7266 | p Value | |
|---|---|---|---|
| Major amputation rates all patients, n (%) | 4114 (39.0) | 2197 (45.3) | <0.001 |
| Major amputation rates PAD III, n (%) | 976 (29.9) | 319 (31.5) | 0.005 |
| Major amputation rates PAD IV, n (%) | 3138 (43.7) | 1878 (49.3) | <0.001 |
| Major amputation rates above-the-knee bypass PAD III, n (%) | 257 (22.4) | 83 (23.5) | 0.283 |
| Major amputation rates below-the-knee bypass PAD III, n (%) | 297 (29.9) | 90 (32.7) | 0.117 |
| Major amputation rates crural/pedal bypass PAD III, n (%) | 422 (39.8) | 146 (40.7) | 0.018 |
| Major amputation rates above-the-knee bypass PAD IV, n (%) | 715 (35.2) | 432 (40.7) | <0.001 |
| Major amputation rates below-the-knee bypass PAD IV, n (%) | 856 (41.1) | 463 (49.6) | 0.002 |
| Major amputation rates crural/pedal bypass PAD IV, n (%) | 1567 (52.4) | 983 (55.5) | 0.007 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Surmann, J.; Meyer, P.; Epple, J.; Schmitz-Rixen, T.; Böckler, D.; Grundmann, R.T., on behalf of the DIGG. Long-Term Outcome of Lower Extremity Bypass Surgery in Diabetic and Non-Diabetic Patients with Critical Limb-Threatening Ischaemia in Germany. Biomedicines 2024, 12, 38. https://doi.org/10.3390/biomedicines12010038
Surmann J, Meyer P, Epple J, Schmitz-Rixen T, Böckler D, Grundmann RT on behalf of the DIGG. Long-Term Outcome of Lower Extremity Bypass Surgery in Diabetic and Non-Diabetic Patients with Critical Limb-Threatening Ischaemia in Germany. Biomedicines. 2024; 12(1):38. https://doi.org/10.3390/biomedicines12010038
Chicago/Turabian StyleSurmann, Johanna, Philipp Meyer, Jasmin Epple, Thomas Schmitz-Rixen, Dittmar Böckler, and Reinhart T. Grundmann on behalf of the DIGG. 2024. "Long-Term Outcome of Lower Extremity Bypass Surgery in Diabetic and Non-Diabetic Patients with Critical Limb-Threatening Ischaemia in Germany" Biomedicines 12, no. 1: 38. https://doi.org/10.3390/biomedicines12010038
APA StyleSurmann, J., Meyer, P., Epple, J., Schmitz-Rixen, T., Böckler, D., & Grundmann, R. T., on behalf of the DIGG. (2024). Long-Term Outcome of Lower Extremity Bypass Surgery in Diabetic and Non-Diabetic Patients with Critical Limb-Threatening Ischaemia in Germany. Biomedicines, 12(1), 38. https://doi.org/10.3390/biomedicines12010038