

A Bioactive Gelatin-Methacrylate Incorporating Magnesium Phosphate Cement for Bone Regeneration

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
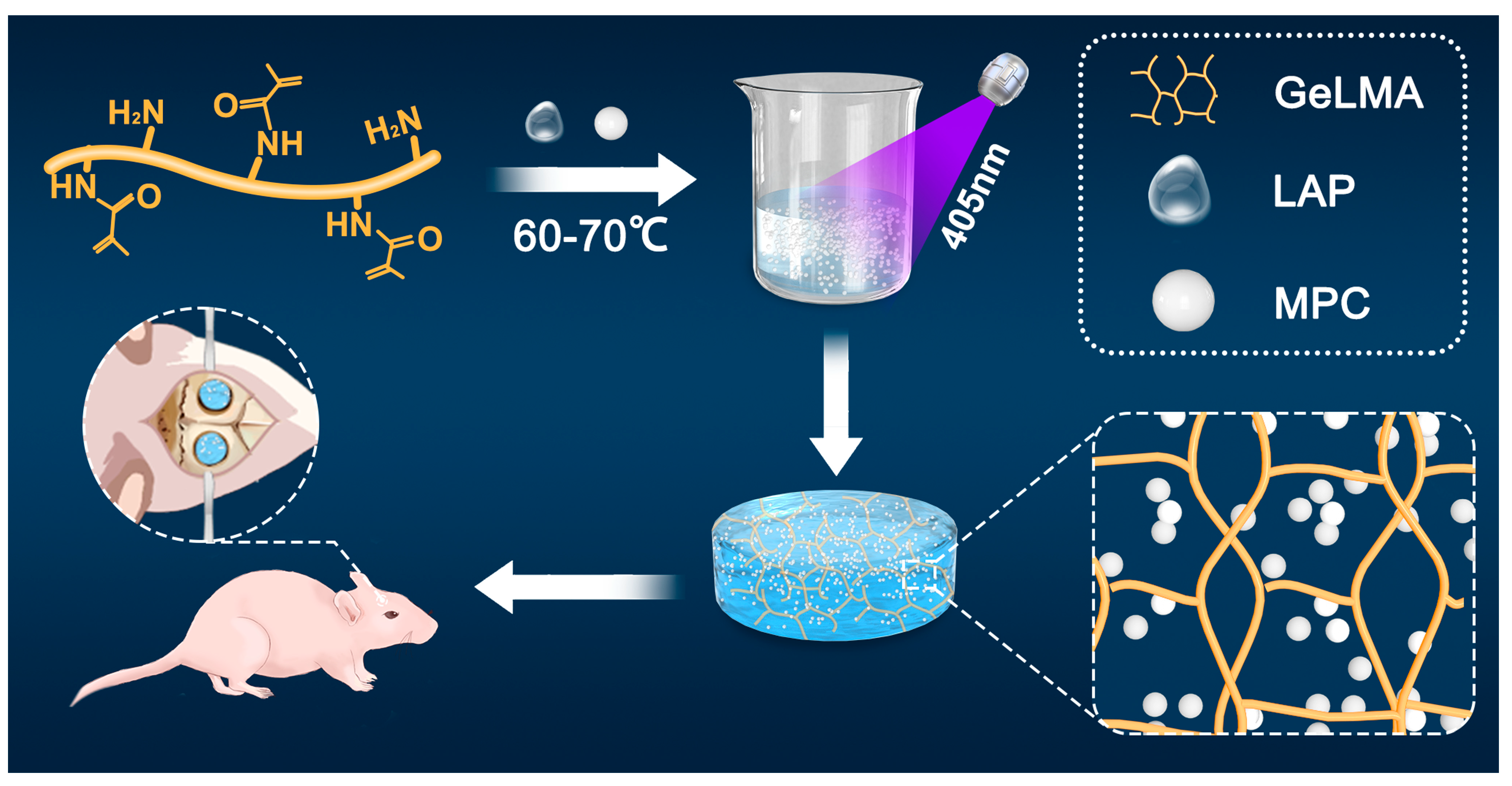
2.1. Preparation of GelMA/MPC Composites
2.2. Microstructure Analysis
2.3. X-ray Diffraction
2.4. Infrared Analysis
2.5. In Vitro Mechanical Analysis of GMPCs
2.6. In Vitro of Magnesium Ion Release Experiment
2.7. In Vitro of Cell Culture and Cell Viability Analysis
2.8. In Vivo Study
2.9. Microcomputed Tomography (Micro-CT) Analysis
2.10. Histological Analysis
2.11. Statistical Analysis
3. Results
3.1. Characterization of GelMA Hydrogels and GMPC
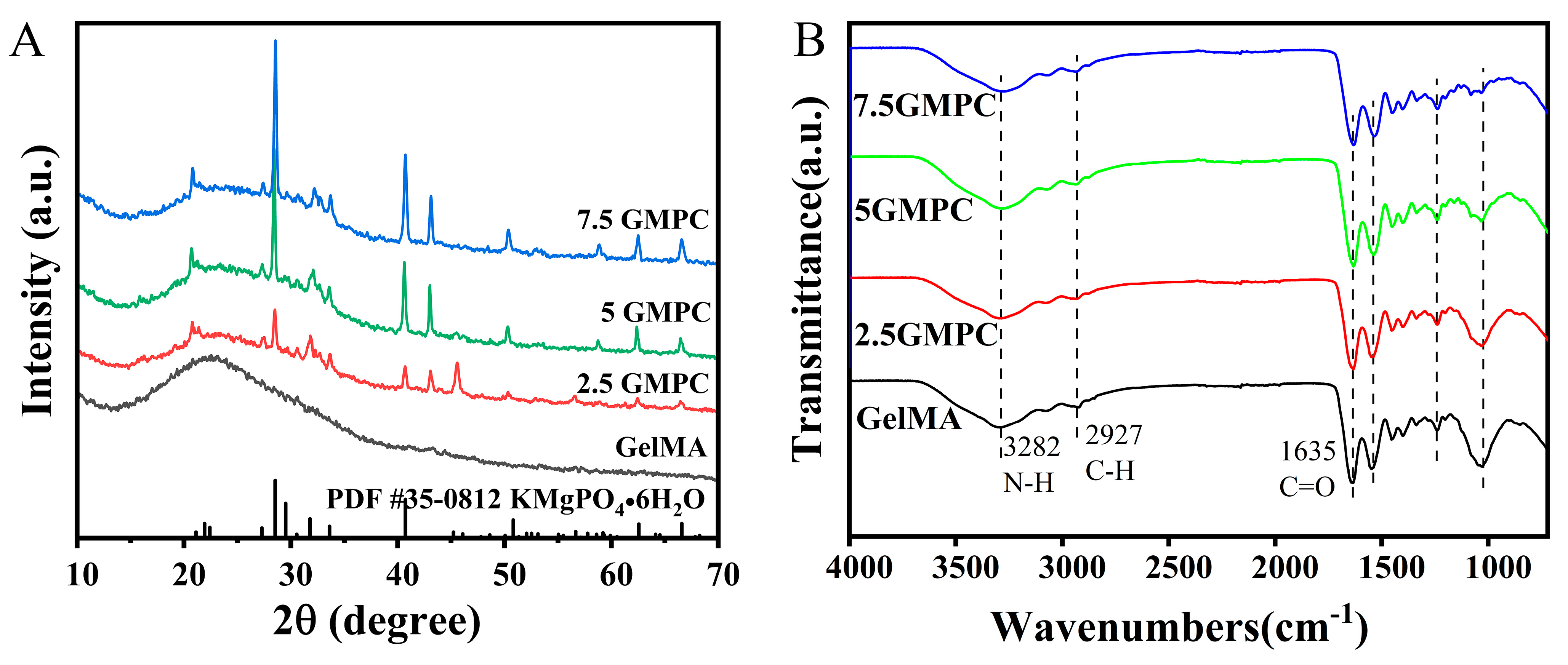
3.1.1. XRD and FTIR of GelMA and GMPC
3.1.2. Mechanical Properties and SEM of GelMA and GMPC
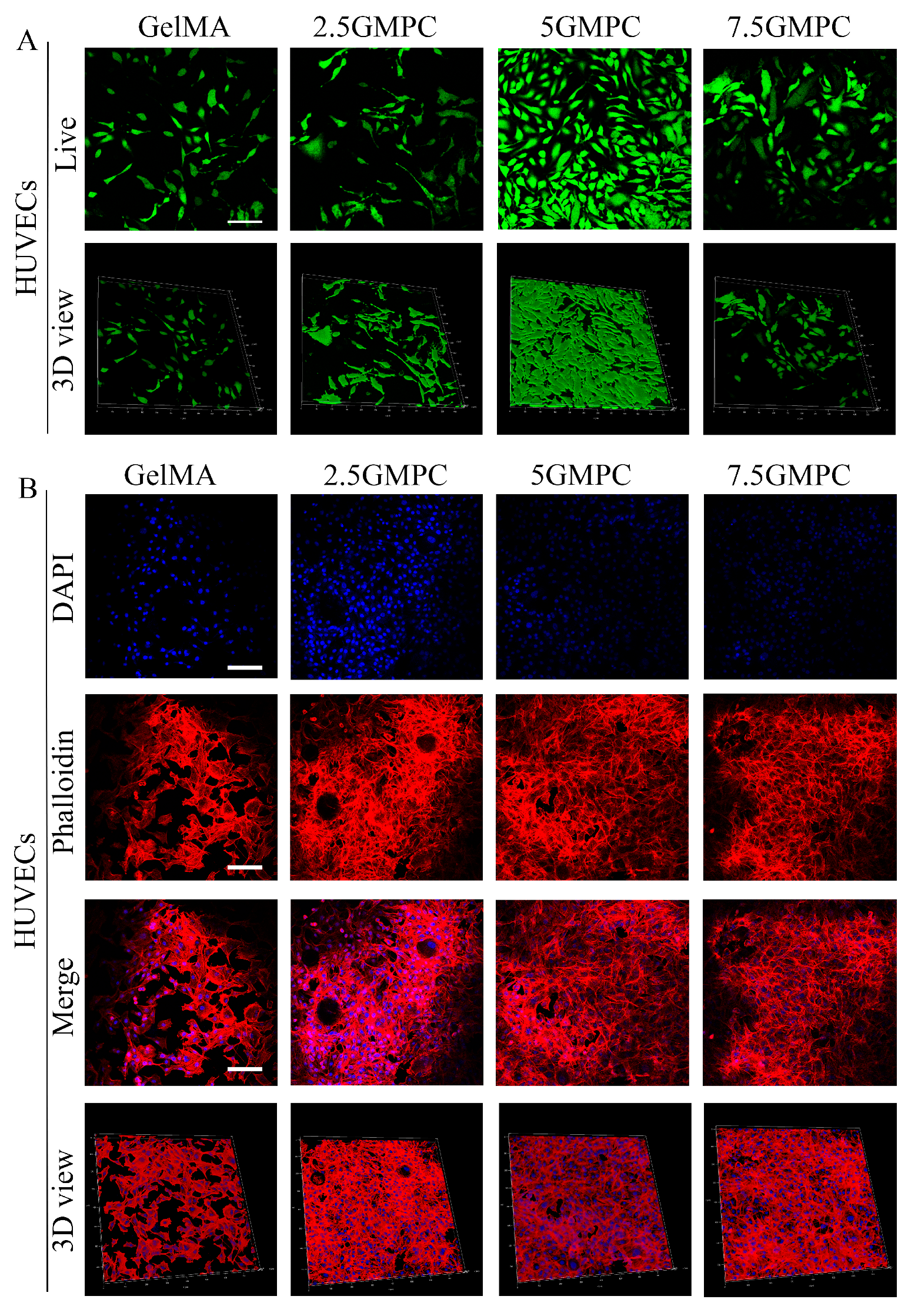
3.2. Cell Viability of HUVECs on the GelMA Hydrogels and GMPCs
3.3. Osteogenic Differentiation of MSCs on the GelMA and GMPC
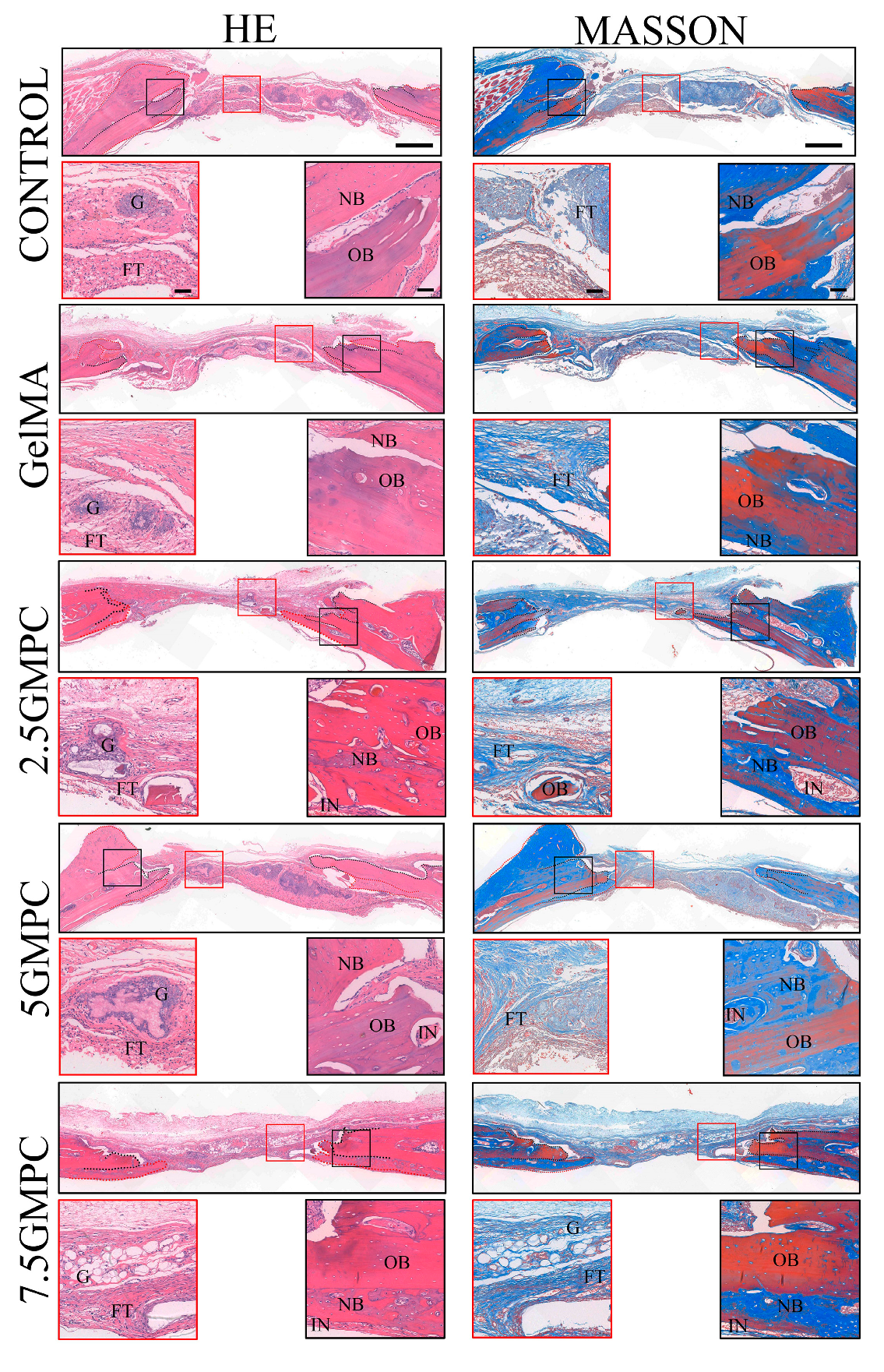
3.4. Bone Regeneration of GelMA and GMPCs in an Animal Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, S.; Chen, M.J.; Wu, X.H.; Lin, S.X.; Tao, C.; Cao, H.L.; Shao, Z.W.; Xiao, G.Z. Global, regional and national burden of low back pain 1990-2019: A systematic analysis of the Global Burden of Disease study 2019. J. Orthop. Transl. 2022, 32, 49–58. [Google Scholar] [CrossRef]
- Duda, G.N.; Geissler, S.; Checa, S.; Tsitsilonis, S.; Petersen, A.; Schmidt-Bleek, K. The decisive early phase of bone regeneration. Nat. Rev. Rheumatol. 2023, 19, 78–95. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Wairkar, S. Bone regeneration in osteoporosis: Opportunities and challenges. Drug Deliv. Transl. Res. 2023, 13, 419–432. [Google Scholar] [CrossRef] [PubMed]
- Kolk, A.; Handschel, J.; Drescher, W.; Rothamel, D.; Kloss, F.; Blessmann, M.; Heiland, M.; Wolff, K.D.; Smeets, R. Current trends and future perspectives of bone substitute materials—From space holders to innovative biomaterials. J. Cranio-Maxillofac. Surg. 2012, 40, 706–718. [Google Scholar] [CrossRef]
- Yuan, Z.Y.; Wan, Z.; Gao, C.Y.; Wang, Y.; Huang, J.Y.; Cai, Q. Controlled magnesium ion delivery system for in situ bone tissue engineering. J. Control. Release 2022, 350, 360–376. [Google Scholar] [CrossRef]
- Zhang, L.Y.; Bi, Q.; Zhao, C.; Chen, J.Y.; Cai, M.H.; Chen, X.Y. Recent Advances in Biomaterials for the Treatment of Bone Defects. Organogenesis 2020, 16, 113–125. [Google Scholar] [CrossRef]
- Kantaros, A.; Ganetsos, T. From Static to Dynamic: Smart Materials Pioneering Additive Manufacturing in Regenerative Medicine. Int. J. Mol. Sci. 2023, 24, 15748. [Google Scholar] [CrossRef]
- Kantaros, A.; Piromalis, D. Fabricating Lattice Structures via 3D Printing: The Case of Porous Bio-Engineered Scaffolds. Appl. Mech. 2021, 2, 289–302. [Google Scholar] [CrossRef]
- Nabiyouni, M.; Brückner, T.; Zhou, H.; Gbureck, U.; Bhaduri, S.B. Magnesium-based bioceramics in orthopedic applications. Acta Biomater. 2018, 66, 23–43. [Google Scholar] [CrossRef]
- Sheikh, Z.; Najeeb, S.; Khurshid, Z.; Verma, V.; Rashid, H.; Glogauer, M. Biodegradable Materials for Bone Repair and Tissue Engineering Applications. Materials 2015, 8, 5744–5794. [Google Scholar] [CrossRef]
- Takagishi, Y.; Kawakami, T.; Hara, Y.; Shinkai, M.; Takezawa, T.; Nagamune, T. Bone-like tissue formation by three-dimensional culture of MG63 osteosarcoma cells in gelatin hydrogels using calcium-enriched medium. Tissue Eng. 2006, 12, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Heo, D.N.; Nah, H.R.; Lee, S.J.; Ko, W.K.; Lee, J.S.; Moon, H.J.; Bang, J.B.; Hwang, Y.S.; Reis, R.L.; et al. Injectable hydrogel composite containing modified gold nanoparticles: Implication in bone tissue regeneration. Int. J. Nanomed. 2018, 13, 7019–7031. [Google Scholar] [CrossRef] [PubMed]
- Benton, J.A.; DeForest, C.A.; Vivekanandan, V.; Anseth, K.S. Photocrosslinking of Gelatin Macromers to Synthesize Porous Hydrogels That Promote Valvular Interstitial Cell Function. Tissue Eng. Part A 2009, 15, 3221–3230. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.K.; Lv, J.T.; Zhao, J.H.; Ling, G.X.; Zhang, P. A versatile GelMA composite hydrogel: Designing principles, delivery forms and biomedical applications. Eur. Polym. J. 2023, 197, 112370. [Google Scholar] [CrossRef]
- Gan, X.Q.; Li, C.; Sun, J.Y.; Zhang, X.D.; Zhou, M.; Deng, Y.; Xiao, A.Q. GelMA/κ-carrageenan double-network hydrogels with superior mechanics and biocompatibility. Rsc Adv. 2023, 13, 1558–1566. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.S.; Wang, Y.; Lai, J.H.; Tan, S.L.; Wang, M. Structure and Properties of Gelatin Methacryloyl (GelMA) Synthesized in Different Reaction Systems. Biomacromolecules 2023, 24, 2928–2941. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, A.S. Hydrogels for biomedical applications. Adv. Drug Deliv. Rev. 2012, 64, 18–23. [Google Scholar] [CrossRef]
- Lee, D.; Choi, E.J.; Lee, S.E.; Kang, K.L.; Moon, H.J.; Kim, H.J.; Youn, Y.H.; Heo, D.N.; Lee, S.J.; Nah, H.; et al. Injectable biodegradable gelatin-methacrylate/β-tricalcium phosphate composite for the repair of bone defects. Chem. Eng. J. 2019, 365, 30–39. [Google Scholar] [CrossRef]
- Mahmoud, A.H.; Han, Y.Y.; Dal-Fabbro, R.; Daghrery, A.; Xu, J.P.; Kaigler, D.; Bhaduri, S.B.; Malda, J.; Bottino, M.C. Nanoscale β-TCP-Laden GelMA/PCL Composite Membrane for Guided Bone Regeneration. Acs Appl. Mater. Interfaces 2023, 15, 32121–32135. [Google Scholar] [CrossRef]
- Chen, W.C.; Zhou, H.Z.; Weir, M.D.; Bao, C.Y.; Xu, H.H.K. Umbilical cord stem cells released from alginate-fibrin microbeads inside macroporous and biofunctionalized calcium phosphate cement fir bone regeneration. Acta Biomater. 2012, 8, 2297–2306. [Google Scholar] [CrossRef]
- Shi, Y.B.; Yu, L.; Gong, C.T.; Li, W.; Zhao, Y.C.; Guo, W.C. A bioactive magnesium phosphate cement incorporating chondroitin sulfate for bone regeneration. Biomed. Mater. 2021, 16, 035034. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.C.; Zhang, T.F.; Hoff, B.; Suvarnapathaki, S.; Lantigua, D.; McCarthy, C.; Wu, B.; Camci-Unal, G. Mineralized Hydrogels Induce Bone Regeneration in Critical Size Cranial Defects. Adv. Healthc. Mater. 2021, 10, 2001101. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Gao, C.Y.; Ye, J.D.; Zhang, M. Synthesis and Characterization of a Novel Silver-Substituted Calcium Phosphate Cement. J. Mater. Sci. Technol. 2014, 30, 686–691. [Google Scholar] [CrossRef]
- Yu, Y.; Xu, C.; Dai, H.L. Preparation and characterization of a degradable magnesium phosphate bone cement. Regen. Biomater. 2016, 3, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Wen, J.Y.; Cai, D.L.; Gao, W.D.; He, R.Y.; Li, Y.L.; Zhou, Y.H.; Klein, T.; Xiao, L.; Xiao, Y. Osteoimmunomodulatory Nanoparticles for Bone Regeneration. Nanomaterials 2023, 13, 692. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, S.; Nakagaki, H.; Ishiguro, K.; Kondo, K.; Mukai, M.; Robinson, C.; Weatherell, J.A. Magnesium Distribution in Human Bone. Calcif. Tissue Int. 1994, 54, 34–37. [Google Scholar] [CrossRef] [PubMed]
- de Baaij, J.H.F.; Hoenderop, J.G.J.; Bindels, R.J.M. Magnesium in Man: Implications for Health and Disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, L.T.; Grynpas, M.D.; Rey, C.C.; Wu, Y.; Ackerman, J.L.; Glimcher, M.J. A comparison of the physical and chemical differences between cancellous and cortical bovine bone mineral at two ages. Calcif. Tissue Int. 2008, 83, 146–154. [Google Scholar] [CrossRef]
- Gelli, R.; Mati, L.; Ridi, F.; Baglioni, P. Tuning the properties of magnesium phosphate-based bone cements: Effect of powder to liquid ratio and aqueous solution concentration. Mater. Sci. Eng. C-Mater. Biol. Appl. 2019, 95, 248–255. [Google Scholar] [CrossRef]
- Kanter, B.; Vikman, A.; Brückner, T.; Schamel, M.; Gbureck, U.; Ignatius, A. Bone regeneration capacity of magnesium phosphate cements in a large animal model. Acta Biomater. 2018, 69, 352–361. [Google Scholar] [CrossRef]
- He, M.F.; Chen, L.; Yin, M.; Xu, S.X.; Liang, Z.Y. Review on magnesium and magnesium-based alloys as biomaterials for bone immobilization. J. Mater. Res. Technol. 2023, 23, 4396–4419. [Google Scholar] [CrossRef]
- Wang, S.; Xu, C.; Yu, S.C.; Wu, X.P.; Jie, Z.; Dai, H.L. Citric acid enhances the physical properties, cytocompatibility and osteogenesis of magnesium calcium phosphate cement. J. Mech. Behav. Biomed. Mater. 2019, 94, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Schlundt, C.; El Khassawna, T.; Serra, A.; Dienelt, A.; Wendler, S.; Schell, H.; van Rooijen, N.; Radbruch, A.; Lucius, R.; Hartmann, S.; et al. Macrophages in bone fracture healing: Their essential role in endochondral ossification. Bone 2018, 106, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Castaño, I.M.; Raftery, R.M.; Chen, G.; Cavanagh, B.; Quinn, B.; Duffy, G.R.; O’Brien, F.J.; Curtin, C.M. Rapid bone repair with the recruitment of CD206+M2-like macrophages using non-viral scaffold-mediated miR-133a inhibition of host cells. Acta Biomater. 2020, 109, 267–279. [Google Scholar] [CrossRef]
- Yu, S.C.; Liu, L.L.; Xu, C.; Dai, H.L. Magnesium phosphate based cement with improved setting, strength and cytocompatibility properties by adding Ca(H2PO4)2•H2O and citric acid. J. Mech. Behav. Biomed. Mater. 2019, 91, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Ding, Z.W.; Yan, D.W.; He, H.S.; Xi, W.J.; Hu, J.B.; Zhang, R.G.; Yan, Y.G.; Zhang, Q.Y. Double-network composites based on inorganic fillers reinforced dextran-based hydrogel with high strength. Carbohydr. Polym. 2022, 296, 119900. [Google Scholar] [CrossRef] [PubMed]
- Qiao, W.; Wong, K.H.M.; Shen, J.; Wang, W.; Wu, J.; Li, J.; Lin, Z.; Chen, Z.; Matinlinna, J.P.; Zheng, Y.; et al. TRPM7 kinase-mediated immunomodulation in macrophage plays a central role in magnesium ion-induced bone regeneration. Nat. Commun. 2021, 12, 2885. [Google Scholar] [CrossRef]
- Burguera, E.F.; Xu, H.H.K.; Weir, M.D. Injectable and rapid-setting calcium phosphate bone cement with dicalcium phosphate dihydrate. J. Biomed. Mater. Res. Part B-Appl. Biomater. 2006, 77B, 126–134. [Google Scholar] [CrossRef]
- Roseti, L.; Parisi, V.; Petretta, M.; Cavallo, C.; Desando, G.; Bartolotti, I.; Grigolo, B. Scaffolds for Bone Tissue Engineering: State of the art and new perspectives. Mater. Sci. Eng. C-Mater. Biol. Appl. 2017, 78, 1246–1262. [Google Scholar] [CrossRef]
- Zhao, C.Q.; Liu, W.Y.; Zhu, M.; Wu, C.T.; Zhu, Y.F. Bioceramic-based scaffolds with antibacterial function for bone tissue engineering: A review. Bioact. Mater. 2022, 18, 383–398. [Google Scholar] [CrossRef]
- Zhou, Y.L.; Wu, C.T.; Chang, J. Bioceramics to regulate stem cells and their microenvironment for tissue regeneration. Mater. Today 2019, 24, 41–56. [Google Scholar] [CrossRef]
- Du, Z.Y.; Guo, L.Y.; Zheng, T.Y.; Cai, Q.; Yang, X.P. Formation of core-shell structured calcium silicate fiber via sol-gel electrospinning and controlled calcination. Ceram. Int. 2019, 45, 23975–23983. [Google Scholar] [CrossRef]
- Mendes, A.X.; Silva, S.M.; O’Connell, C.D.; Duchi, S.; Quigley, A.F.; Kapsa, R.M.I.; Moulton, S.E. Enhanced Electroactivity, Mechanical Properties, and Printability through the Addition of Graphene Oxide to Photo-Cross-linkable Gelatin Methacryloyl Hydrogel. Acs Biomater. Sci. Eng. 2021, 7, 2279–2295. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.S.; Um, Y.J.; Chai, J.K.; Cho, K.S.; Moon, I.S.; Choi, S.H.; Jung, U.W.; Lee, D.W.; Kim, C.K. A canine model for histometric evaluation of periodontal regeneration. Periodontol. 2000 2011, 56, 209–226. [Google Scholar] [CrossRef] [PubMed]
- Saris, N.E.L.; Mervaala, E.; Karppanen, H.; Khawaja, J.A.; Lewenstam, A. Magnesium—An update on physiological, clinical and analytical aspects. Clin. Chim. Acta 2000, 294, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.F.; Nightingale, C.H. Magnesium sulfate in eclampsia and pre-eclampsia pharmacokinetic principles. Clin. Pharmacokinet. 2000, 38, 305–314. [Google Scholar] [CrossRef]
- Zhou, H.; Liang, B.; Jiang, H.T.; Deng, Z.L.; Yu, K.X. Magnesium-based biomaterials as emerging agents for bone repair and regeneration: From mechanism to application. J. Magnes. Alloys 2021, 9, 779–804. [Google Scholar] [CrossRef]
- Amukarimi, S.; Mozafari, M. Biodegradable Magnesium Biomaterials-Road to the Clinic. Bioengineering 2022, 9, 107. [Google Scholar] [CrossRef]
- Wang, J.; Witte, F.; Xi, T.; Zheng, Y.; Yang, K.; Yang, Y.; Zhao, D.; Meng, J.; Li, Y.; Li, W.; et al. Recommendation for modifying current cytotoxicity testing standards for biodegradable magnesium-based materials. Acta Biomater. 2015, 21, 237–249. [Google Scholar] [CrossRef]
- Laubach, M.; Hildebrand, F.; Suresh, S.; Wagels, M.; Kobbe, P.; Gilbert, F.; Kneser, U.; Holzapfel, B.M.; Hutmacher, D.W. The Concept of Scaffold-Guided Bone Regeneration for the Treatment of Long Bone Defects: Current Clinical Application and Future Perspective. J. Funct. Biomater. 2023, 14, 341. [Google Scholar] [CrossRef]
- Loi, F.; Córdova, L.A.; Pajarinen, J.; Lin, T.H.; Yao, Z.Y.; Goodman, S.B. Inflammation, fracture and bone repair. Bone 2016, 86, 119–130. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Gong, C.; Wang, X.; Wei, Z.; Guo, W. A Bioactive Gelatin-Methacrylate Incorporating Magnesium Phosphate Cement for Bone Regeneration. Biomedicines 2024, 12, 228. https://doi.org/10.3390/biomedicines12010228
Zhang X, Gong C, Wang X, Wei Z, Guo W. A Bioactive Gelatin-Methacrylate Incorporating Magnesium Phosphate Cement for Bone Regeneration. Biomedicines. 2024; 12(1):228. https://doi.org/10.3390/biomedicines12010228
Chicago/Turabian StyleZhang, Xiping, Changtian Gong, Xingyu Wang, Zhun Wei, and Weichun Guo. 2024. "A Bioactive Gelatin-Methacrylate Incorporating Magnesium Phosphate Cement for Bone Regeneration" Biomedicines 12, no. 1: 228. https://doi.org/10.3390/biomedicines12010228
APA StyleZhang, X., Gong, C., Wang, X., Wei, Z., & Guo, W. (2024). A Bioactive Gelatin-Methacrylate Incorporating Magnesium Phosphate Cement for Bone Regeneration. Biomedicines, 12(1), 228. https://doi.org/10.3390/biomedicines12010228