

Combination of Sarcopenia and Hypoalbuminemia Is a Poor Prognostic Factor in Surgically Treated Nonmetastatic Renal Cell Carcinoma


Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Data Collection and Variable Definitions
2.3. Assessment of Sarcopenia and Hypoalbuminemia
2.4. Statistical Analysis
3. Results
3.1. Patient and Disease Characteristics
3.2. The Optimal Thresholds for PMI
3.3. Association of Clinicopathological Parameters with Sarcopenia and Albumin
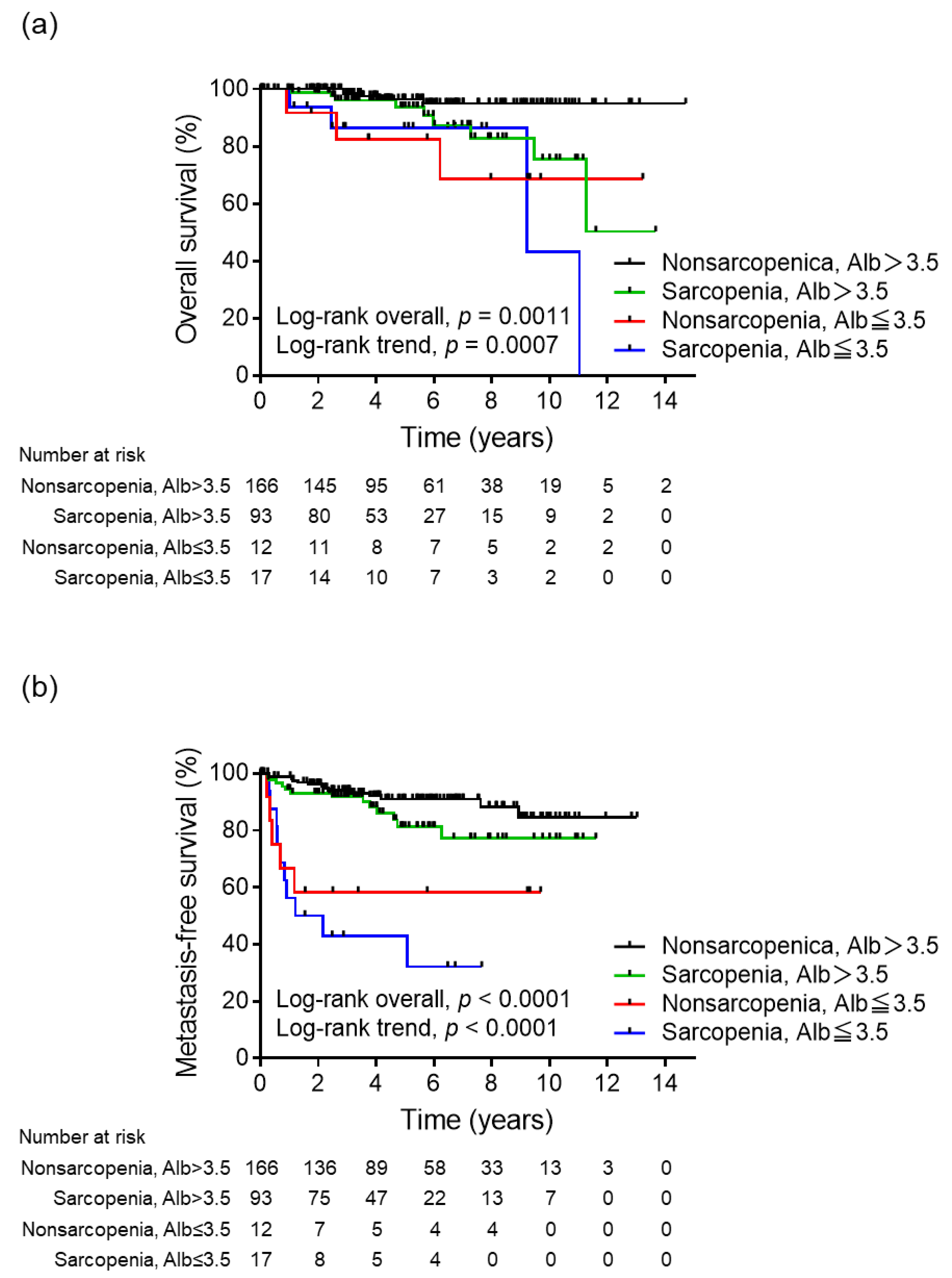
3.4. Survival Rates and Prognostic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klatte, T.; Rossi, S.H.; Stewart, G.D. Prognostic factors and prognostic models for renal cell carcinoma: A literature review. World J. Urol. 2018, 36, 1943–1952. [Google Scholar] [CrossRef] [PubMed]
- Parker, W.P.; Cheville, J.C.; Frank, I.; Zaid, H.B.; Lohse, C.M.; Boorjian, S.A.; Leibovich, B.C.; Thompson, R.H. Application of the Stage, Size, Grade, and Necrosis (SSIGN) Score for Clear Cell Renal Cell Carcinoma in Contemporary Patients. Eur. Urol. 2017, 71, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Wiedmer, P.; Jung, T.; Castro, J.P.; Pomatto, L.C.D.; Sun, P.Y.; Davies, K.J.A.; Grune, T. Sarcopenia—Molecular mechanisms and open questions. Ageing Res. Rev. 2021, 65, 101200. [Google Scholar] [CrossRef]
- Caan, B.J.; Meyerhardt, J.A.; Kroenke, C.H.; Alexeeff, S.; Xiao, J.; Weltzien, E.; Feliciano, E.C.; Castillo, A.L.; Quesenberry, C.P.; Kwan, M.L.; et al. Explaining the Obesity Paradox: The Association between Body Composition and Colorectal Cancer Survival (C-SCANS Study). Cancer Epidemiol. Biomark. Prev. 2017, 26, 1008–1015. [Google Scholar] [CrossRef]
- Prado, C.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: A population-based study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Joglekar, S.; Nau, P.N.; Mezhir, J.J. The impact of sarcopenia on survival and complications in surgical oncology: A review of the current literature. J. Surg. Oncol. 2015, 112, 503–509. [Google Scholar] [CrossRef]
- Shachar, S.S.; Williams, G.R.; Muss, H.B.; Nishijima, T.F. Prognostic value of sarcopenia in adults with solid tumours: A meta-analysis and systematic review. Eur. J. Cancer 2016, 57, 58–67. [Google Scholar] [CrossRef]
- Gupta, D.; Lis, C.G. Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature. Nutr. J. 2010, 9, 69. [Google Scholar] [CrossRef]
- Meyer, C.P.; Rios-Diaz, A.J.; Dalela, D.; Ravi, P.; Sood, A.; Hanske, J.; Chun, F.K.H.; Kibel, A.S.; Lipsitz, S.R.; Sun, M.; et al. The association of hypoalbuminemia with early perioperative outcomes—A comprehensive assessment across 16 major procedures. Am. J. Surg. 2017, 214, 871–883. [Google Scholar] [CrossRef]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; O’Reilly, D.S.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. An inflammation-based prognostic score (mGPS) predicts cancer survival independent of tumour site: A Glasgow Inflammation Outcome Study. Br. J. Cancer 2011, 104, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; Fletcher, C.D.; O’Reilly, D.S.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. A comparison of inflammation-based prognostic scores in patients with cancer. A Glasgow Inflammation Outcome Study. Eur. J. Cancer 2011, 47, 2633–2641. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Zhang, G.L. C-reactive protein to albumin ratio predicts the outcome in renal cell carcinoma: A meta-analysis. PLoS ONE 2019, 14, e0224266. [Google Scholar] [CrossRef] [PubMed]
- Makino, T.; Izumi, K.; Iwamoto, H.; Kadomoto, S.; Kadono, Y.; Mizokami, A. Comparison of the Prognostic Value of Inflammatory and Nutritional Indices in Nonmetastatic Renal Cell Carcinoma. Biomedicines 2023, 11, 533. [Google Scholar] [CrossRef]
- Sun, D.W.; An, L.; Lv, G.Y. Albumin-fibrinogen ratio and fibrinogen-prealbumin ratio as promising prognostic markers for cancers: An updated meta-analysis. World J. Surg. Oncol. 2020, 18, 9. [Google Scholar] [CrossRef]
- Xia, Z.; Fu, X.; Yuan, X.; Li, J.; Wang, H.; Sun, J.; Wu, J.; Tang, L. Serum albumin to globulin ratio prior to treatment as a potential non-invasive prognostic indicator for urological cancers. Front. Nutr. 2022, 9, 1012181. [Google Scholar] [CrossRef]
- Kim, S.I.; Kim, S.J.; Kim, S.J.; Cho, D.S. Prognostic nutritional index and prognosis in renal cell carcinoma: A systematic review and meta-analysis. Urol. Oncol. 2021, 39, 623–630. [Google Scholar] [CrossRef]
- Ni, L.; Huang, J.; Ding, J.; Kou, J.; Shao, T.; Li, J.; Gao, L.; Zheng, W.; Wu, Z. Prognostic Nutritional Index Predicts Response and Prognosis in Cancer Patients Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Front. Nutr. 2022, 9, 823087. [Google Scholar] [CrossRef]
- Visser, M.; Kritchevsky, S.B.; Newman, A.B.; Goodpaster, B.H.; Tylavsky, F.A.; Nevitt, M.C.; Harris, T.B. Lower serum albumin concentration and change in muscle mass: The Health, Aging and Body Composition Study. Am. J. Clin. Nutr. 2005, 82, 531–537. [Google Scholar] [CrossRef]
- Hamaguchi, Y.; Kaido, T.; Okumura, S.; Kobayashi, A.; Hammad, A.; Tamai, Y.; Inagaki, N.; Uemoto, S. Proposal for new diagnostic criteria for low skeletal muscle mass based on computed tomography imaging in Asian adults. Nutrition 2016, 32, 1200–1205. [Google Scholar] [CrossRef]
- Akobeng, A.K. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr. 2007, 96, 644–647. [Google Scholar] [CrossRef] [PubMed]
- Midenberg, E.; Higgins, M.I.; Schmeusser, B.N.; Patil, D.H.; Zaldumbide, J.; Martini, D.J.; Steele, S.; Williams, M.; Nabavizadeh, R.; Psutka, S.P.; et al. Prognostic Value of Sarcopenia and Albumin in the Surgical Management of Localized Renal Cell Carcinoma. Urol. Oncol. 2023, 41, 50.e19–50.e26. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Zargar-Shoshtari, K.; Caracciolo, J.T.; Fishman, M.; Poch, M.A.; Pow-Sang, J.; Sexton, W.J.; Spiess, P.E. Sarcopenia as a predictor of overall survival after cytoreductive nephrectomy for metastatic renal cell carcinoma. Urol. Oncol. 2015, 33, 339.e17–339.e23. [Google Scholar] [CrossRef] [PubMed]
- Psutka, S.P.; Boorjian, S.A.; Moynagh, M.R.; Schmit, G.D.; Costello, B.A.; Thompson, R.H.; Stewart-Merrill, S.B.; Lohse, C.M.; Cheville, J.C.; Leibovich, B.C.; et al. Decreased Skeletal Muscle Mass is Associated with an Increased Risk of Mortality after Radical Nephrectomy for Localized Renal Cell Cancer. J. Urol. 2016, 195, 270–276. [Google Scholar] [CrossRef]
- Fukushima, H.; Nakanishi, Y.; Kataoka, M.; Tobisu, K.; Koga, F. Prognostic Significance of Sarcopenia in Patients with Metastatic Renal Cell Carcinoma. J. Urol. 2016, 195, 26–32. [Google Scholar] [CrossRef]
- Mao, W.; Wang, K.; Zhang, H.; Lu, H.; Sun, S.; Tian, C.; Wu, Z.; Wu, J.; Xu, B.; Xu, H.; et al. Sarcopenia as a poor prognostic indicator for renal cell carcinoma patients undergoing nephrectomy in China: A multicenter study. Clin. Transl. Med. 2021, 11, e270. [Google Scholar] [CrossRef]
- Makino, T.; Izumi, K.; Iwamoto, H.; Kadomoto, S.; Kadono, Y.; Mizokami, A. Sarcopenia Is Associated with Aggressive Clinicopathological Outcomes and Is a Poor Prognostic Indicator for Non-metastatic Renal Cell Carcinoma. In Vivo 2023, 37, 1304–1311. [Google Scholar] [CrossRef]
- Li, S.; Wang, T.; Tong, G.; Li, X.; You, D.; Cong, M. Prognostic Impact of Sarcopenia on Clinical Outcomes in Malignancies Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 726257. [Google Scholar] [CrossRef]
- Higgins, M.I.; Martini, D.J.; Patil, D.H.; Nabavizadeh, R.; Steele, S.; Williams, M.; Joshi, S.S.; Narayan, V.M.; Sekhar, A.; Psutka, S.P.; et al. Sarcopenia and modified Glasgow Prognostic Score predict postsurgical outcomes in localized renal cell carcinoma. Cancer 2021, 127, 1974–1983. [Google Scholar] [CrossRef]
- Liu, Q.; Yang, J.; Chen, X.; Yang, J.; Zhao, X.; Huang, Y.; Lin, Y.; Pu, J. Prognostic significance of sarcopenia and systemic inflammation for patients with renal cell carcinoma following nephrectomy. Front. Oncol. 2022, 12, 1047515. [Google Scholar] [CrossRef]
- Morgan, T.M.; Tang, D.; Stratton, K.L.; Barocas, D.A.; Anderson, C.B.; Gregg, J.R.; Chang, S.S.; Cookson, M.S.; Herrell, S.D.; Smith, J.A., Jr.; et al. Preoperative nutritional status is an important predictor of survival in patients undergoing surgery for renal cell carcinoma. Eur. Urol. 2011, 59, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Heymsfield, S.B. Lean tissue imaging: A new era for nutritional assessment and intervention. JPEN J. Parenter. Enteral. Nutr. 2014, 38, 940–953. [Google Scholar] [CrossRef] [PubMed]
- Mantzorou, M.; Koutelidakis, A.; Theocharis, S.; Giaginis, C. Clinical Value of Nutritional Status in Cancer: What is its Impact and how it Affects Disease Progression and Prognosis? Nutr. Cancer 2017, 69, 1151–1176. [Google Scholar] [CrossRef] [PubMed]
- Yuxuan, L.; Junchao, L.; Wenya, L. The role of sarcopenia in treatment-related outcomes in patients with renal cell carcinoma: A systematic review and meta-analysis. Medicine 2022, 101, e31332. [Google Scholar] [CrossRef]
- Xia, L.; Zhao, R.; Wan, Q.; Wu, Y.; Zhou, Y.; Wang, Y.; Cui, Y.; Shen, X.; Wu, X. Sarcopenia and adverse health-related outcomes: An umbrella review of meta-analyses of observational studies. Cancer Med. 2020, 9, 7964–7978. [Google Scholar] [CrossRef]
- Caraceni, P.; Tufoni, M.; Bonavita, M.E. Clinical use of albumin. Blood Transfus. 2013, 11 (Suppl. S4), s18–s25. [Google Scholar] [CrossRef]
- Corcoran, A.T.; Kaffenberger, S.D.; Clark, P.E.; Walton, J.; Handorf, E.; Piotrowski, Z.; Tomaszewski, J.J.; Ginzburg, S.; Mehrazin, R.; Plimack, E.; et al. Hypoalbuminaemia is associated with mortality in patients undergoing cytoreductive nephrectomy. BJU Int. 2015, 116, 351–357. [Google Scholar] [CrossRef]
- Zhou, X.; Fu, G.; Zu, X.; Xu, Z.; Li, H.T.; D’Souza, A.; Tulpule, V.; Quinn, D.I.; Bhowmick, N.A.; Weisenberger, D.J.; et al. Albumin levels predict prognosis in advanced renal cell carcinoma treated with tyrosine kinase inhibitors: A systematic review and meta-analysis. Urol. Oncol. 2022, 40, 12.e13–12.e22. [Google Scholar] [CrossRef]
- Sun, K.; Chen, S.; Xu, J.; Li, G.; He, Y. The prognostic significance of the prognostic nutritional index in cancer: A systematic review and meta-analysis. J. Cancer Res. Clin. Oncol. 2014, 140, 1537–1549. [Google Scholar] [CrossRef]
- Peng, Q.; Liu, L.; Li, T.; Lei, C.; Wan, H. Prognostic impact of prognostic nutritional index on renal cell carcinoma: A meta-analysis of 7629 patients. PLoS ONE 2022, 17, e0265119. [Google Scholar] [CrossRef]
- Nascimento, W.; Ferrari, G.; Martins, C.B.; Rey-Lopez, J.P.; Izquierdo, M.; Lee, D.H.; Giovannucci, E.L.; Rezende, L.F.M. Muscle-strengthening activities and cancer incidence and mortality: A systematic review and meta-analysis of observational studies. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 69. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Thomson, C.A.; Sullivan, K.R.; Howe, C.L.; Kushi, L.H.; Caan, B.J.; Neuhouser, M.L.; Bandera, E.V.; Wang, Y.; Robien, K.; et al. American Cancer Society nutrition and physical activity guideline for cancer survivors. CA Cancer J. Clin. 2022, 72, 230–262. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; He, T.; Sun, S.; Wu, J.; Xu, B.; Mao, W.; Chen, M. Prognostic Significance of Pre- to Postoperative Dynamics of Sarcopenia for Patients with Renal Cell Carcinoma Undergoing Laparoscopic Nephrectomy. Front. Surg. 2022, 9, 871731. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suarez, V.J.; Redondo-Florez, L.; Rubio-Zarapuz, A.; Martinez-Guardado, I.; Navarro-Jimenez, E.; Tornero-Aguilera, J.F. Nutritional and Exercise Interventions in Cancer-Related Cachexia: An Extensive Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 4604. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | n (%) |
|---|---|
| Median age, yr (IQR) | 63 (55–71) |
| Sex | |
| Male | 208 (72.2) |
| Female | 80 (27.8) |
| Median BMI, kg/m2 (IQR) | 23.7 (21.7–26.4) |
| BMI ≥ 25 kg/m2 | 100 (34.7) |
| Median PMI, mm2/m2 (IQR) | 468.2 (352.9–571.7) |
| Male | 520.8 (440.5–619.0) |
| Female | 299.2 (249.2–374.8) |
| Sarcopenia | 110 (38.2) |
| KPS ≤ 90 | 17 (5.9) |
| Median CCI (IQR) | 2.0 (1.0–3.0) |
| CCI ≥ 3 | 121 (42.0) |
| Hypertension | 153 (53.1) |
| Diabetes | 54 (18.8) |
| Smoking status | 155 (53.8) |
| Median albumin concentration, g/dL (IQR) | 4.2 (3.9–4.5) |
| Hypoalbuminemia (≤3.5 g/dL) | 29 (10.1) |
| Median CRP level, mg/dL (IQR) | 0.1 (0.1–0.2) |
| Elevated CRP (≥0.3 mg/dL) | 62 (21.5) |
| Sarcopenia and albumin status | |
| Non-sarcopenia, albumin > 3.5 | 166 (57.6) |
| Sarcopenia, albumin > 3.5 | 93 (32.3) |
| Non-sarcopenia, albumin ≤ 3.5 | 12 (4.2) |
| Sarcopenia, albumin ≤ 3.5 | 17 (5.9) |
| Surgery type | |
| Radical nephrectomy | 145 (50.3) |
| Partial nephrectomy | 143 (49.7) |
| Histology | |
| Clear cell | 245 (85.1) |
| Non-clear cell | 43 (14.9) |
| Median tumor size, cm (IQR) | 2.9 (2.0–4.93) |
| Pathological T-stage | |
| ≤pT2 | 237 (82.3) |
| ≥pT3 | 51 (17.7) |
| Grade | |
| ≤G2 | 226 (78.5) |
| ≥G3 | 49 (17.0) |
| Unknown | 13 (4.5) |
| Lymphovascular invasion | |
| Yes | 138 (47.9) |
| No | 148 (51.4) |
| Unknown | 2 (0.7) |
| Sarcopenia and Albumin Status | ||||||
|---|---|---|---|---|---|---|
| Covariate | Level | Non-Sarcopenia, Albumin > 3.5 (n = 166) (%) | Sarcopenia, Albumin > 3.5 (n = 93) (%) | Non-Sarcopenia, Albumin ≤ 3.5 (n = 12) (%) | Sarcopenia, Albumin ≤ 3.5 (n = 17) (%) | p-Value |
| Age | ≥65 | 60 (36.1) | 58 (62.4) | 5 (41.7) | 9 (52.9) | <0.001 |
| Sex | Male | 103 (62.0) | 84 (90.3) | 6 (50.0) | 15 (88.2) | <0.001 |
| KPS | ≤90 | 6 (3.6) | 3 (3.2) | 4 (33.3) | 4 (23.5) | <0.001 |
| CCI | Median (IQR) | 2.0 (1.0–3.0) | 3.0 (2.0–4.0) | 2.0 (0.8–3.3) | 3.0 (2.0–3.0) | 0.009 |
| ≥3 | 57 (34.3) | 51 (54.8) | 4 (33.3) | 9 (52.9) | 0.002 | |
| BMI (kg/m2) | Median (IQR) | 24.3 (22.5–26.8) | 23.1 (21.4–24.9) | 25.8 (22.4–27.6) | 22.3 (20.5–23.3) | <0.001 |
| ≥25 | 67 (40.4) | 23 (24.7) | 7 (58.3) | 3 (17.6) | 0.009 | |
| CRP level (mg/dL) | Median (IQR) | 0.10 (0–0.20) | 0.10 (0.10–0.20) | 0.80 (0.10–5.33) | 3.00 (0.20–8.70) | <0.001 |
| ≥0.3 | 22 (13.3) | 21 (22.6) | 7 (58.3) | 12 (70.6) | <0.001 | |
| Tumor size (cm) | Median (IQR) | 2.7 (1.9–4.48) | 2.9 (2.0–4.50) | 5.05 (2.48–10.63) | 6.6 (2.5–8.8) | <0.001 |
| >4 | 44 (26.5) | 28 (30.1) | 8 (66.7) | 11 (64.7) | <0.001 | |
| Pathological T-stage | ≤pT2 | 147 (88.6) | 73 (78.5) | 7 (58.3) | 10 (58.8) | <0.001 |
| ≥pT3 | 19 (11.4) | 20 (21.5) | 5 (41.7) | 7 (41.2) | ||
| Grade | ≤G2 | 140 (84.3) | 74 (79.6) | 7 (58.3) | 5 (29.4) | <0.001 |
| ≥G3 | 16 (9.6) | 16 (17.2) | 5 (41.7) | 12 (70.6) | ||
| Unknown | 10 (6.0) | 3 (3.2) | 0 | 0 | ||
| Lymphovascular invasion | Yes | 73 (44.0) | 47 (50.5) | 5 (41.7) | 13 (76.5) | 0.072 |
| No | 92 (55.4) | 45 (48.4) | 7 (58.3) | 4 (23.5) | ||
| Unknown | 1 (0.6) | 1 (1.1) | 0 | 0 | ||
| Variables | Univariate | Multivariate | ||
|---|---|---|---|---|
| p-Value | p-Value | HR (95% CI) | ||
| Age | ≥65 vs. <65 | 0.053 | 0.017 | 0.43 (0.22–0.86) |
| Sex | Male vs. female | 0.151 | ||
| KPS | ≤90 vs. 100 | <0.001 | 0.047 | 2.46 (1.01–5.99) |
| CCI | ≥3 vs. <3 | 0.350 | ||
| BMI | ≥25 vs. <25 | 0.486 | ||
| Hypertension | Yes vs. no | 0.655 | ||
| Diabetes | Yes vs. no | 0.602 | ||
| Smoking | Yes vs. no | 0.943 | ||
| CRP level | ≥0.3 vs. <0.3 | <0.001 | 0.810 | 1.12 (0.45–2.80) |
| Tumor size | >4 cm vs. ≤4 cm | <0.001 | 0.001 | 4.79 (1.88–12.20) |
| Pathological T-stage | 3–4 vs. 1–2 | <0.001 | 0.835 | 1.10 (0.46–2.61) |
| Histologic type | Non-ccRCC vs. ccRCC | 0.485 | ||
| Grade | ≥3 vs. <3 | <0.001 | 0.003 | 3.26 (1.48–7.17) |
| Lymphovascular invasion | Yes vs. no | <0.001 | 0.083 | 2.31 (0.90–5.97) |
| Sarcopenia + albumin status | Non-sarcopenia, albumin > 3.5 | — | — | 1 (ref.) |
| Sarcopenia, albumin > 3.5 | 0.124 | 0.102 | 1.94 (0.88–4.32) | |
| Non-sarcopenia, albumin ≤ 3.5 | <0.001 | 0.010 | 4.79 (1.44–15.89) | |
| Sarcopenia, albumin ≤ 3.5 | <0.001 | 0.041 | 2.96 (1.05–8.39) | |
| Variables | Univariate | Multivariate | ||
|---|---|---|---|---|
| p-Value | p-Value | HR (95% CI) | ||
| Age | ≥65 vs. <65 | 0.314 | ||
| Sex | Male vs. female | 0.302 | ||
| KPS | ≤90 vs. 100 | 0.082 | 0.116 | 2.77 (0.78–9.84) |
| CCI | ≥3 vs. <3 | 0.584 | ||
| BMI | ≥25 vs. <25 | 0.717 | ||
| Hypertension | Yes vs. no | 0.271 | ||
| Diabetes | Yes vs. no | 0.610 | ||
| Smoking | Yes vs. no | 0.276 | ||
| CRP level | ≥0.3 vs. <0.3 | 0.708 | ||
| Tumor size | >4 cm vs. ≤4 cm | 0.276 | ||
| Pathological T-stage | 3–4 vs. 1–2 | 0.366 | ||
| Histologic type | Non-ccRCC vs. ccRCC | 0.602 | ||
| Grade | ≥3 vs. <3 | 0.450 | ||
| Lymphovascular invasion | Yes vs. no | 0.082 | 0.238 | 1.74 (0.69–4.35) |
| Sarcopenia + albumin status | Non-sarcopenia, albumin > 3.5 | — | — | 1 (ref.) |
| Sarcopenia, albumin > 3.5 | 0.022 | 0.021 | 3.64 (1.21–10.90) | |
| Non-sarcopenia, albumin ≤ 3.5 | 0.012 | 0.016 | 5.87 (1.39–24.73) | |
| Sarcopenia, albumin ≤ 3.5 | 0.001 | 0.006 | 6.87 (1.75–26.94) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makino, T.; Izumi, K.; Iwamoto, H.; Kadomoto, S.; Mizokami, A. Combination of Sarcopenia and Hypoalbuminemia Is a Poor Prognostic Factor in Surgically Treated Nonmetastatic Renal Cell Carcinoma. Biomedicines 2023, 11, 1604. https://doi.org/10.3390/biomedicines11061604
Makino T, Izumi K, Iwamoto H, Kadomoto S, Mizokami A. Combination of Sarcopenia and Hypoalbuminemia Is a Poor Prognostic Factor in Surgically Treated Nonmetastatic Renal Cell Carcinoma. Biomedicines. 2023; 11(6):1604. https://doi.org/10.3390/biomedicines11061604
Chicago/Turabian StyleMakino, Tomoyuki, Kouji Izumi, Hiroaki Iwamoto, Suguru Kadomoto, and Atsushi Mizokami. 2023. "Combination of Sarcopenia and Hypoalbuminemia Is a Poor Prognostic Factor in Surgically Treated Nonmetastatic Renal Cell Carcinoma" Biomedicines 11, no. 6: 1604. https://doi.org/10.3390/biomedicines11061604
APA StyleMakino, T., Izumi, K., Iwamoto, H., Kadomoto, S., & Mizokami, A. (2023). Combination of Sarcopenia and Hypoalbuminemia Is a Poor Prognostic Factor in Surgically Treated Nonmetastatic Renal Cell Carcinoma. Biomedicines, 11(6), 1604. https://doi.org/10.3390/biomedicines11061604