
Hair Cortisol and Perceived Stress—Predictors for the Onset of Tics? A European Longitudinal Study on High-Risk Children

 , , , and
on behalf of the EMTICS Collaborative Group
, , , and
on behalf of the EMTICS Collaborative Group
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Procedure
2.3. Measures
2.4. Statistical Analyses
3. Results
3.1. Description and Characteristics of the Total Study Sample and Subsample Used for Analyses
3.2. Non-Linear Time Effects
3.3. Effects of Stress up to Twelve Months before the Onset of Tics on the Likelihood of Developing Tics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Cubo, E.; Trejo Gabriel y Galán, J.M.; Villaverde, V.A.; Sáez Velasco, S.; Delgado Benito, V.; Vicente Macarrón, J.; Guevara, J.C.; Louis, E.D.; Benito-León, J. Prevalence of Tics in Schoolchildren in Central Spain: A Population-Based Study. Pediatr. Neurol. 2011, 45, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Kurlan, R.; Como, P.G.; Miller, B.; Palumbo, D.; Deeley, C.; Andresen, E.M.; Eapen, S.; McDermott, M.P. The Behavioral Spectrum of Tic Disorders: A Community-Based Study. Neurology 2002, 59, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Snider, L.A.; Seligman, L.D.; Ketchen, B.R.; Levitt, S.J.; Bates, L.R.; Garvey, M.A.; Swedo, S.E. Tics and Problem Behaviors in Schoolchildren: Prevalence, Characterization, and Associations. Pediatrics 2002, 110, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Robertson, M.M.; Eapen, V.; Singer, H.S.; Martino, D.; Scharf, J.M.; Paschou, P.; Roessner, V.; Woods, D.W.; Hariz, M.; Mathews, C.A.; et al. Gilles de La Tourette Syndrome. Nat. Rev. Dis. Prim. 2017, 3, 16097. [Google Scholar] [CrossRef]
- Knight, T.; Steeves, T.; Day, L.; Lowerison, M.; Jette, N.; Pringsheim, T. Prevalence of Tic Disorders: A Systematic Review and Meta-Analysis. Pediatr. Neurol. 2012, 47, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Openneer, T.J.C.; Huyser, C.; Martino, D.; Schrag, A.; Group, E.C.; Hoekstra, P.J.; Dietrich, A. Clinical Precursors of Tics: An EMTICS Study. J. Child Psychol. Psychiatry 2022, 63, 305–314. [Google Scholar] [CrossRef]
- Bornstein, R.A.; Stefl, M.E.; Hammond, L. A Survey of Tourette Syndrome Patients and Their Families: The 1987 Ohio Tourette Survey. J. Neuropsychiatry Clin. Neurosci. 1990, 2, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Horesh, N.; Zimmerman, S.; Steinberg, T.; Yagan, H.; Apter, A. Is Onset of Tourette Syndrome Influenced by Life Events? J. Neural Transm. 2008, 115, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Rose, C.D.; Mariotti, P. Children Experienced New or Worsening Tic Issues When They Were Separated from Their Parents during the Italian COVID-19 Lockdown. Acta Paediatr. 2021, 110, 394–396. [Google Scholar] [CrossRef]
- Jones, H.F.; Han, V.X.; Patel, S.; Gloss, B.S.; Soler, N.; Ho, A.; Sharma, S.; Kothur, K.; Nosadini, M.; Wienholt, L.; et al. Maternal Autoimmunity and Inflammation Are Associated with Childhood Tics and Obsessive-Compulsive Disorder: Transcriptomic Data Show Common Enriched Innate Immune Pathways. Brain Behav. Immun. 2021, 94, 308–317. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: Berlin/Heidelberg, Germany, 1984; ISBN 9780826141927. [Google Scholar]
- Steudte-Schmiedgen, S.; Stalder, T.; Schönfeld, S.; Wittchen, H.-U.; Trautmann, S.; Alexander, N.; Miller, R.; Kirschbaum, C. Hair Cortisol Concentrations and Cortisol Stress Reactivity Predict PTSD Symptom Increase after Trauma Exposure during Military Deployment. Psychoneuroendocrinology 2015, 59, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Caparros-Gonzalez, R.A.; Romero-Gonzalez, B.; Strivens-Vilchez, H.; Gonzalez-Perez, R.; Martinez-Augustin, O.; Peralta-Ramirez, M.I. Hair Cortisol Levels, Psychological Stress and Psychopathological Symptoms as Predictors of Postpartum Depression. PLoS ONE 2017, 12, e0182817. [Google Scholar] [CrossRef]
- Ahrens, K.F.; Neumann, R.J.; von Werthern, N.M.; Kranz, T.M.; Kollmann, B.; Mattes, B.; Puhlmann, L.M.C.; Weichert, D.; Lutz, B.; Basten, U.; et al. Association of Polygenic Risk Scores and Hair Cortisol with Mental Health Trajectories during COVID Lockdown. Transl. Psychiatry 2022, 12, 396. [Google Scholar] [CrossRef] [PubMed]
- Frost, A.; Hagaman, A.; Baranov, V.; Chung, E.O.; Bhalotra, S.; Sikander, S.; Maselko, J. Non-Linear Associations between HPA Axis Activity during Infancy and Mental Health Difficulties during Early Childhood among Children in Rural Pakistan. Dev. Psychopathol. 2022. first view. [Google Scholar] [CrossRef]
- Ford, J.L.; Boch, S.J.; Browning, C.R. Hair Cortisol and Depressive Symptoms in Youth: An Investigation of Curvilinear Relationships. Psychoneuroendocrinology 2019, 109, 104376. [Google Scholar] [CrossRef] [PubMed]
- Corbett, B.A.; Mendoza, S.P.; Baym, C.L.; Bunge, S.A.; Levine, S. Examining Cortisol Rhythmicity and Responsivity to Stress in Children with Tourette Syndrome. Psychoneuroendocrinology 2008, 33, 810–820. [Google Scholar] [CrossRef]
- Chappell, P.; Riddle, M.; Anderson, G.; Scahill, L.; Hardin, M.; Walker, D.; Cohen, D.; Leckman, J. Enhanced Stress Responsivity of Tourette Syndrome Patients Undergoing Lumbar Puncture. Biol. Psychiatry 1994, 36, 35–43. [Google Scholar] [CrossRef]
- Chappell, P.; Leckman, J.; Goodman, W.; Bissette, G.; Pauls, D.; Anderson, G.; Riddle, M.; Scahill, L.; McDougle, C.; Cohen, D. Elevated Cerebrospinal Fluid Corticotropin-Releasing Ractor in Tourette’s Syndrome: Comparison to Obsessive Compulsive Disorder and Normal Controls. Biol. Psychiatry 1996, 39, 776–783. [Google Scholar] [CrossRef]
- Buse, J.; Rothe, J.; Uhlmann, A.; Bodmer, B.; Kirschbaum, C.; Hoekstra, P.J.; Dietrich, A.; Roessner, V.; Apter, A.; Baglioni, V.; et al. Hair Cortisol-a Stress Marker in Children and Adolescents with Chronic Tic Disorders? A Large European Cross-Sectional Study. Eur. Child Adolesc. Psychiatry 2021, 31, 771–779. [Google Scholar] [CrossRef]
- Browne, H.A.; Hansen, S.N.; Buxbaum, J.D.; Gair, S.L.; Nissen, J.B.; Nikolajsen, K.H.; Schendel, D.E.; Reichenberg, A.; Parner, E.T.; Grice, D.E. Familial Clustering of Tic Disorders and Obsessive-Compulsive Disorder. JAMA Psychiatry 2015, 72, 359–366. [Google Scholar] [CrossRef]
- Schrag, A.; Martino, D.; Apter, A.; Ball, J.; Bartolini, E.; Benaroya-Milshtein, N.; Buttiglione, M.; Cardona, F.; Creti, R.; Efstratiou, A.; et al. European Multicentre Tics in Children Studies (EMTICS): Protocol for Two Cohort Studies to Assess Risk Factors for Tic Onset and Exacerbation in Children and Adolescents. Eur. Child Adolesc. Psychiatry 2019, 28, 91–109. [Google Scholar] [CrossRef]
- Stalder, T.; Kirschbaum, C. Analysis of Cortisol in Hair—State of the Art and Future Directions. Brain Behav. Immun. 2012, 26, 1019–1029. [Google Scholar] [CrossRef]
- Dettenborn, L.; Tietze, A.; Kirschbaum, C.; Stalder, T. The Assessment of Cortisol in Human Hair: Associations with Sociodemographic Variables and Potential Confounders. Stress 2012, 15, 578–588. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Lee, E.-H. Review of the Psychometric Evidence of the Perceived Stress Scale. Asian Nurs. Res. 2012, 6, 121–127. [Google Scholar] [CrossRef]
- Findley, D.B.; Leckman, J.F.; Katsovich, L.; Lin, H.; Zhang, H.; Grantz, H.; Otka, J.; Lombroso, P.J.; King, R.A. Development of the Yale Children’s Global Stress Index (YCGSI) and Its Application in Children and Adolescents With Tourette’s Syndrome and Obsessive-Compulsive Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 450–457. [Google Scholar] [CrossRef]
- Benjamini, Y.; Yekutieli, D. The Control of the False Discovery Rate in Multiple Testing under Dependency. Ann. Stat. 2001, 29, 1165–1188. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013; ISBN 0-203-77158-3. [Google Scholar]
- Hastie, T.; Tibshirani, R.; Friedman, J.H.; Friedman, J.H. The Elements of Statistical Learning: Data Mining, Inference, and Prediction; Springer: New York, NY, USA, 2009; Volume 2. [Google Scholar]
- Wood, S.N. Fast Stable Restricted Maximum Likelihood and Marginal Likelihood Estimation of Semiparametric Generalized Linear Models. J. R. Stat. Soc. Ser. B (Stat. Methodol.) 2011, 73, 3–36. [Google Scholar] [CrossRef]
- Osborne, J. Improving Your Data Transformations: Applying the Box-Cox Transformation. Pract. Assess. Res. Eval. 2019, 15, 12. [Google Scholar] [CrossRef]
- Stalder, T.; Steudte-Schmiedgen, S.; Alexander, N.; Klucken, T.; Vater, A.; Wichmann, S.; Kirschbaum, C.; Miller, R. Stress-Related and Basic Determinants of Hair Cortisol in Humans: A Meta-Analysis. Psychoneuroendocrinology 2017, 77, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Holm, J.E.; Holroyd, K.A. The Daily Hassles Scale (Revised): Does It Measure Stress or Symptoms? Behav. Assess. 1992, 14, 465–482. [Google Scholar]
- Weckesser, L.J.; Dietz, F.; Schmidt, K.; Grass, J.; Kirschbaum, C.; Miller, R. The Psychometric Properties and Temporal Dynamics of Subjective Stress, Retrospectively Assessed by Different Informants and Questionnaires, and Hair Cortisol Concentrations. Sci. Rep. 2019, 9, 1098. [Google Scholar] [CrossRef]
- Martino, D.; Dale, R.C.; Gilbert, D.L.; Giovannoni, G.; Leckman, J.F. Immunopathogenic Mechanisms in Tourette Syndrome: A Critical Review. Mov. Disord. 2009, 24, 1267–1279. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; Xu, P.; Zhu, W.; Chen, Z.; Tao, X.; Liu, J.; Xue, Z.; Zhu, T.; Jiang, P. Changes of Cytokines in Children With Tic Disorder. Front. Neurol. 2022, 12, 800189. [Google Scholar] [CrossRef] [PubMed]
- Yeon, S.; Lee, J.H.; Kang, D.; Bae, H.; Lee, K.Y.; Jin, S.; Kim, J.R.; Jung, Y.W.; Park, T.W. A Cytokine Study of Pediatric Tourette’s Disorder without Obsessive Compulsive Disorder. Psychiatry Res. 2017, 247, 90–96. [Google Scholar] [CrossRef]
- Leckman, J.F.; Katsovich, L.; Kawikova, I.; Lin, H.; Zhang, H.; Krönig, H.; Morshed, S.; Parveen, S.; Grantz, H.; Lombroso, P.J.; et al. Increased Serum Levels of Interleukin-12 and Tumor Necrosis Factor-Alpha in Tourette’s Syndrome. Biol. Psychiatry 2005, 57, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Lemos, J.C.; Wanat, M.J.; Smith, J.S.; Reyes, B.A.S.; Hollon, N.G.; Van Bockstaele, E.J.; Chavkin, C.; Phillips, P.E.M. Severe Stress Switches CRF Action in the Nucleus Accumbens from Appetitive to Aversive. Nature 2012, 490, 402–406. [Google Scholar] [CrossRef]
- Payer, D.; Williams, B.; Mansouri, E.; Stevanovski, S.; Nakajima, S.; Le Foll, B.; Kish, S.; Houle, S.; Mizrahi, R.; George, S.R.; et al. Corticotropin-Releasing Hormone and Dopamine Release in Healthy Individuals. Psychoneuroendocrinology 2017, 76, 192–196. [Google Scholar] [CrossRef]
- Ganos, C.; Roessner, V.; Münchau, A. The Functional Anatomy of Gilles de La Tourette Syndrome. Neurosci. Biobehav. Rev. 2013, 37, 1050–1062. [Google Scholar] [CrossRef] [PubMed]
- Buse, J.; Kirschbaum, C.; Leckman, J.F.; Münchau, A.; Roessner, V. The Modulating Role of Stress in the Onset and Course of Tourette’s Syndrome: A Review. Behav. Modif. 2014, 38, 184–216. [Google Scholar] [CrossRef]
- Hsu, C.-J.; Wong, L.-C.; Lee, W.-T. Immunological Dysfunction in Tourette Syndrome and Related Disorders. Int. J. Mol. Sci. 2021, 22, 853. [Google Scholar] [CrossRef]
- Cox, J.H.; Seri, S.; Cavanna, A.E. Sensory Aspects of Tourette Syndrome. Neurosci. Biobehav. Rev. 2018, 88, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Belluscio, B.A.; Jin, L.; Watters, V.; Lee, T.H.; Hallett, M. Sensory Sensitivity to External Stimuli in Tourette Syndrome Patients. Mov. Disord. 2011, 26, 2538–2543. [Google Scholar] [CrossRef] [PubMed]
- Buse, J.; Beste, C.; Herrmann, E.; Roessner, V. Neural Correlates of Altered Sensorimotor Gating in Boys with Tourette Syndrome: A Combined EMG/FMRI Study. World J. Biol. Psychiatry 2016, 17, 187–197. [Google Scholar] [CrossRef]
- Reese, H.E.; Vallejo, Z.; Rasmussen, J.; Crowe, K.; Rosenfield, E.; Wilhelm, S. Mindfulness-Based Stress Reduction for Tourette Syndrome and Chronic Tic Disorder: A Pilot Study. J. Psychosom. Res. 2015, 78, 293–298. [Google Scholar] [CrossRef] [PubMed]



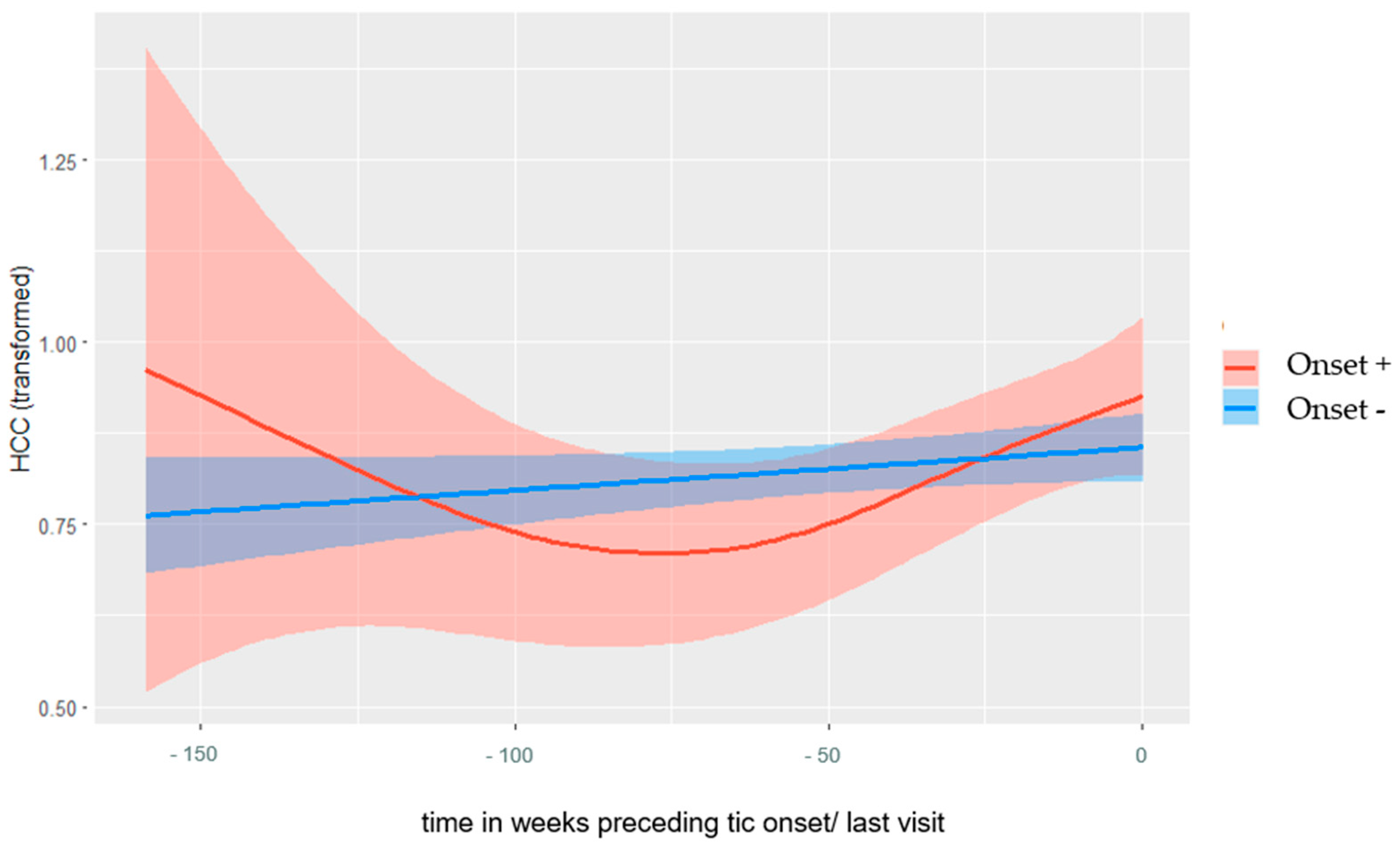{kind=link}
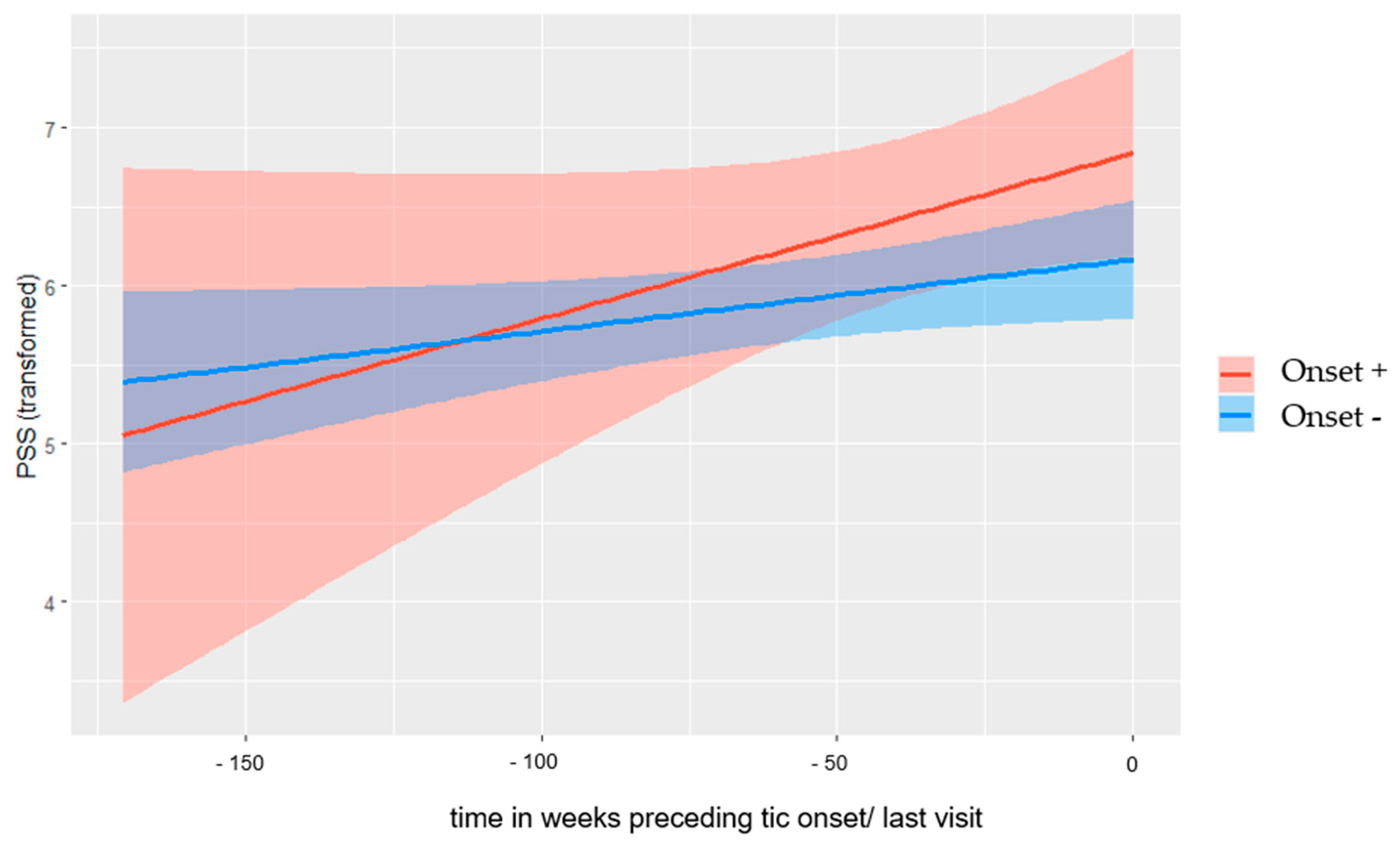{kind=link}
| Onset+ | Onset− | Test Statistic | p-Value | Effect Size | |
|---|---|---|---|---|---|
| Children included in the present study | |||||
| n | 54 | 177 | |||
| Sex, male, n (%) | 33 (61%) | 67 (38%) | X2 (1) = 9.12 | p = 0.003 | φ = 0.19 |
| Highest education parents, Md | 5 | 5 | X2 (4) = 1.92 | p = 0.75 | V = 0.09 |
| ADHD (DSM-IV-TR), n (%) | 6 (11%) | 13 (7%) | X2 (1) = 0.63 | p = 0.43 | φ = 0.05 |
| Age, M (SD) | 6.61 (1.83) | 6.69 (2.16) | t (229) = −0.25 | p = 0.80 | d = 0.04 |
| Study duration in weeks, M (SD) | 51.41 (40.10) | 84.68 (53.07) | t (114.88) = −4.92 | p < 0.001 | d = −0.66 |
| Sample used for binary logistic regression | |||||
| n | 13 | 59 | |||
| Sex, male, n (%) | 8 (62%) | 17 (29%) | X2 (1) = 5.03 | p = 0.03 | φ = 0.26 |
| Highest education parents, Md | 4 | 4 | X2 (4) = 0.15 | p = 0.99 | V = 0.05 |
| ADHD (DSM-IV-TR), n (%) | 0 (0%) | 7 (12%) | X2 (1) = 1.71 | p = 0.19 | φ = 0.15 |
| Age, M (SD) | 6.94 (1.89) | 7.27 (2.32) | t (70) = −0.48 | p = 0.63 | d = 0.15 |
| Weeks between T1 and T2, M (SD) Range | 17.24 (2.05) 14–20 | 17.02 (1.87) 12–22 | t (70) = 0.37 | p = 0.72 | d = 0.11 |
| Weeks between T2 and T3, M (SD) Range | 14.15 (4.47) 6–20 | 16.63 (2.06) 10–23 | t (13.14) = −1.95 | p = 0.07 | d = −0.93 |
| Onset+ n = 13 | Onset− n = 59 | Test Statistic | p-Value | Effect Size | |
|---|---|---|---|---|---|
| T1 | |||||
| Description of the visit and time range | Second last visit before tic onset with valid hair sample and PSS-10 (visit occurred 6–9 months before onset) | Baseline visit with a valid hair sample | |||
| HCC, M (SD) 1 | 4.93 (5.22) | 2.94 (3.84) | t (70) = 1.43 | p = 0.16 | d = 0.44 |
| PSS-10, M (SD) 1 | 11.38 (7.14) | 10.38 (6.56) | t (70) = 0.45 | p = 0.66 | d = 0.14 |
| T2 | |||||
| Description of the visit and time range | Last visit before tic onset with valid hair sample and PSS-10 (visit occurred 2–5 months before onset) | First follow-up visit with a valid hair sample | |||
| HCC, M (SD) 1 | 5.62 (5.48) | 2.26 (1.94) | t (70) = 2.63 | p = 0.01 2 | d = 0.81 |
| PSS-10, M (SD) 1 | 11.23 (6.62) | 10.70 (7.98) | t (70) = 0.32 | p = 0.75 | d = 0.10 |
| T3 | |||||
| Description of the visit and time range | At onset with valid hair sample and PSS-10 | Second follow-up visit with a valid hair sample | |||
| HCC, M (SD) 1 | 3.31 (2.71) | 2.61 (3.24) | t (70) = 1.16 | p = 0.25 | d = 0.36 |
| PSS-10, M (SD) 1 | 11.23 (6.62) | 10.70 (7.98) | t (70) = 0.67 | p = 0.51 | d = 0.20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rothe, J.; Buse, J.; Uhlmann, A.; Bodmer, B.; Kirschbaum, C.; Hoekstra, P.J.; Dietrich, A.; Roessner, V., on behalf of the EMTICS Collaborative Group. Hair Cortisol and Perceived Stress—Predictors for the Onset of Tics? A European Longitudinal Study on High-Risk Children. Biomedicines 2023, 11, 1561. https://doi.org/10.3390/biomedicines11061561
Rothe J, Buse J, Uhlmann A, Bodmer B, Kirschbaum C, Hoekstra PJ, Dietrich A, Roessner V on behalf of the EMTICS Collaborative Group. Hair Cortisol and Perceived Stress—Predictors for the Onset of Tics? A European Longitudinal Study on High-Risk Children. Biomedicines. 2023; 11(6):1561. https://doi.org/10.3390/biomedicines11061561
Chicago/Turabian StyleRothe, Josefine, Judith Buse, Anne Uhlmann, Benjamin Bodmer, Clemens Kirschbaum, Pieter J. Hoekstra, Andrea Dietrich, and Veit Roessner on behalf of the EMTICS Collaborative Group. 2023. "Hair Cortisol and Perceived Stress—Predictors for the Onset of Tics? A European Longitudinal Study on High-Risk Children" Biomedicines 11, no. 6: 1561. https://doi.org/10.3390/biomedicines11061561
APA StyleRothe, J., Buse, J., Uhlmann, A., Bodmer, B., Kirschbaum, C., Hoekstra, P. J., Dietrich, A., & Roessner, V., on behalf of the EMTICS Collaborative Group. (2023). Hair Cortisol and Perceived Stress—Predictors for the Onset of Tics? A European Longitudinal Study on High-Risk Children. Biomedicines, 11(6), 1561. https://doi.org/10.3390/biomedicines11061561