






SARS-CoV-2 Infection in Venezuelan Pediatric Patients—A Single Center Prospective Observational Study

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
Characteristics of the Cohort
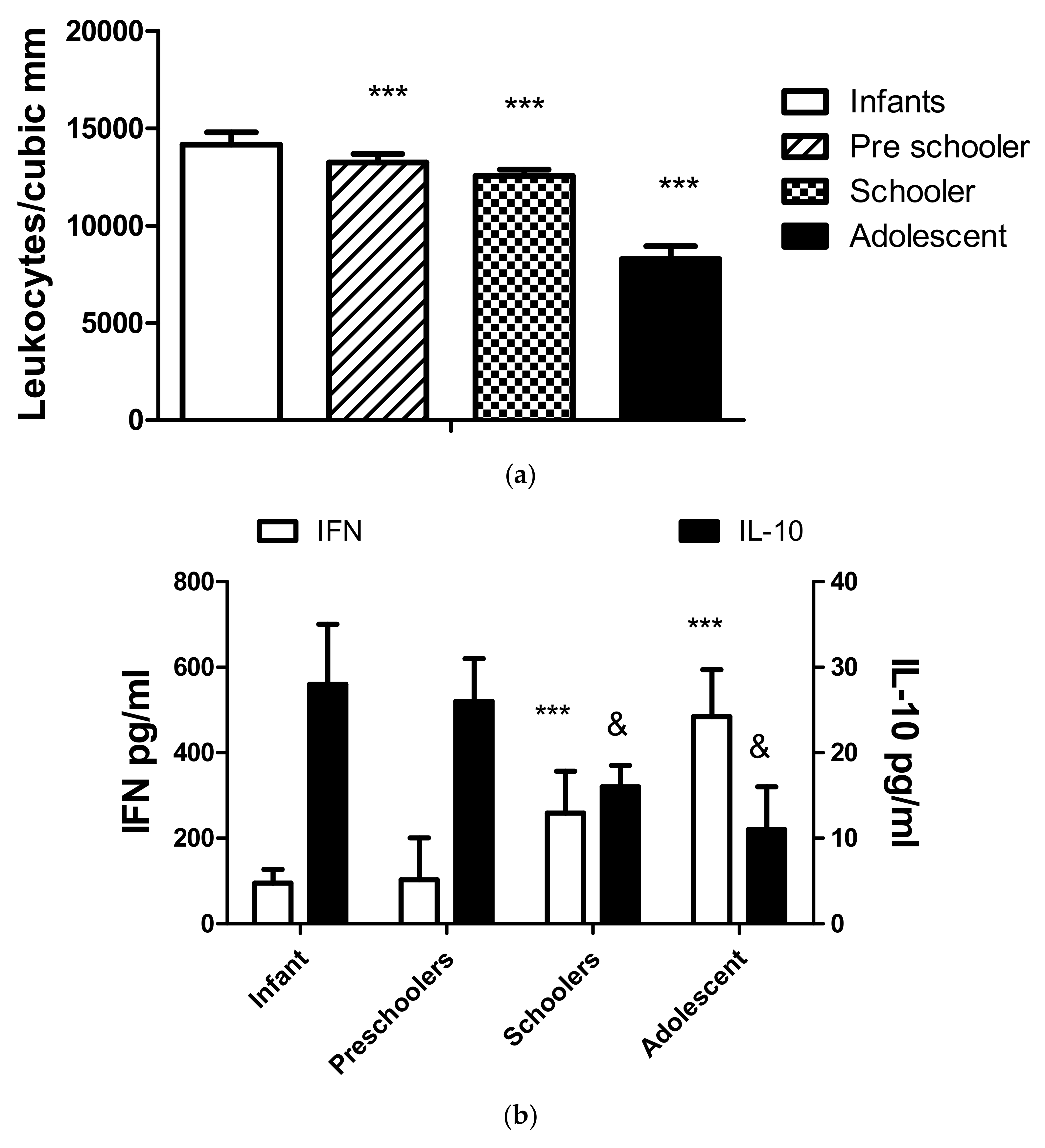
4. The Influence of Age on Lymphocyte Populations and Cytokine Values
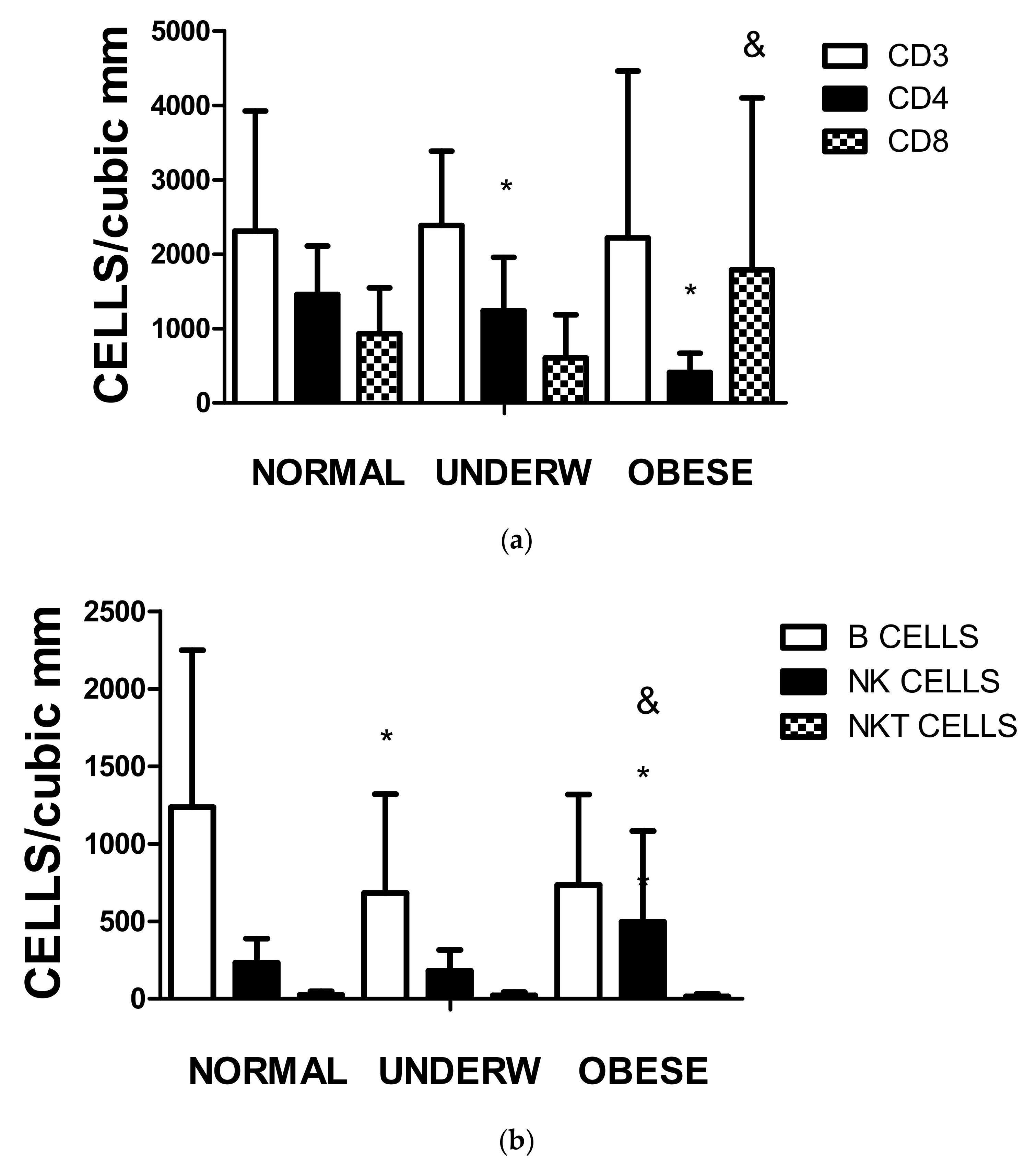
5. Nutritional Status and Lymphocyte Populations
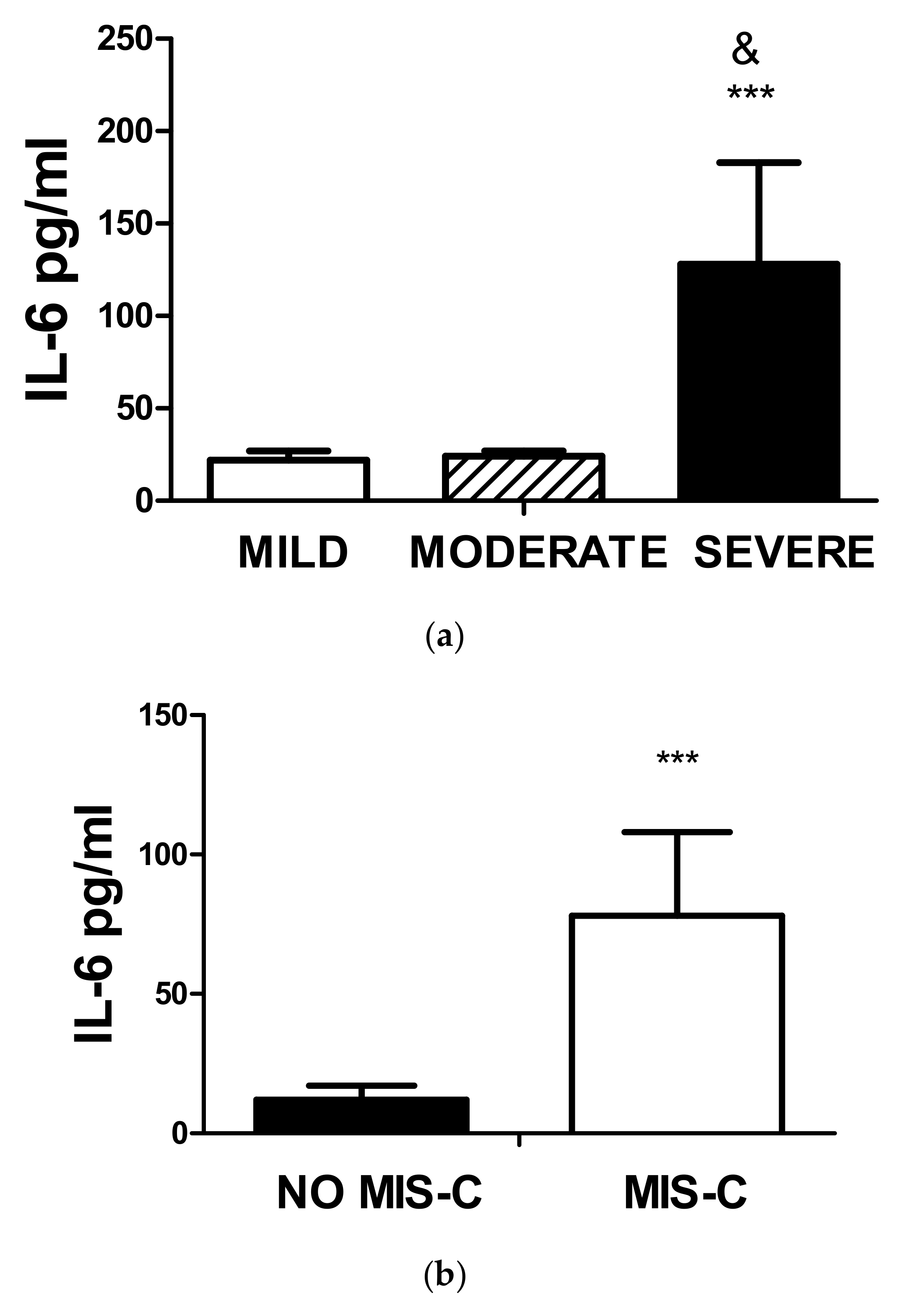
6. MIS-C, COVID-19 Severity, and IL-6 Concentrations
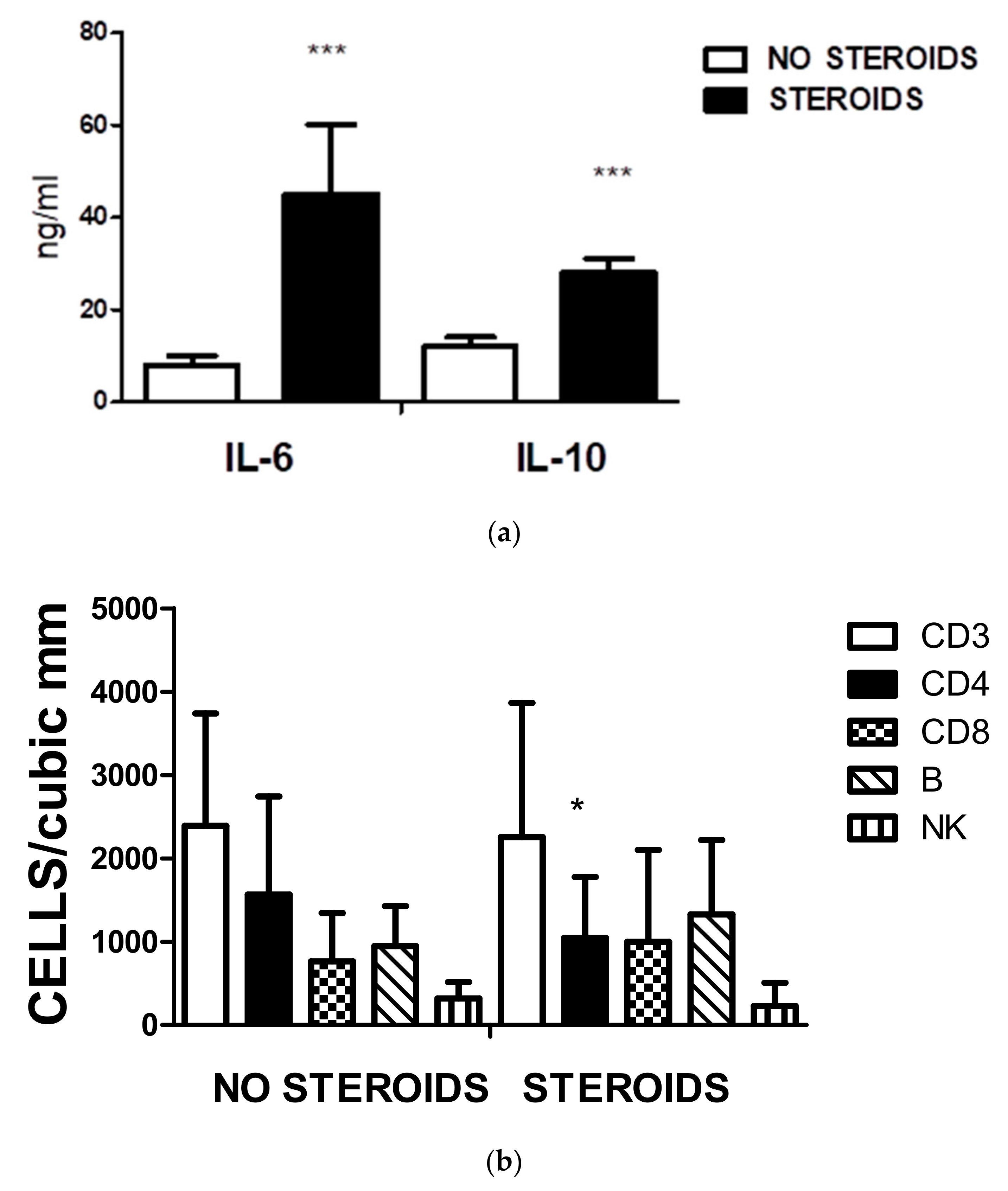
7. Steroid Use, Cytokine Concentration, and Lymphocyte Population
8. Discussion
9. Conclusions
10. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fung, T.S.; Liu, D.X. Human Coronavirus: Host-Pathogen Interaction. Annu. Rev. Microbiol. 2019, 73, 529–557. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Wong, G.W.K. SARS-CoV-2 Infection in Children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef] [PubMed]
- Consiglio, C.R.; Cotugno, N.; Sardh, F.; Pou, C.; Amodio, D.; Rodriguez, L.; Tan, Z.; Zicari, S.; Ruggiero, A.; Pascucci, G.R.; et al. The Immunology of Multisystem Inflammatory Syndrome in Children with COVID-19. Cell 2020, 183, 968–981.e7. [Google Scholar] [CrossRef]
- Zimmermann, P.; Curtis, N. Coronavirus Infections in Children Including COVID-19: An Overview of the Epidemiology, Clinical Features, Diagnosis, Treatment and Prevention Options in Children. Pediatr. Infect. Dis. J. 2020, 39, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Qiu, H.; Wu, J.; Hong, L.; Luo, Y.; Song, Q.; Chen, D. Clinical and epidemiological features of 36 children with coronavirus disease 2019 (COVID-19) in Zhejiang, China: An observational cohort study. Lancet Infect. Dis. 2020, 20, 689–696. [Google Scholar] [CrossRef]
- De Sanctis, J.B.; García, A.H.; Moreno, D.; Hajduch, M. Coronavirus infection: An immunologists’ perspective. Scand. J. Immunol. 2021, 93, e130432021. [Google Scholar] [CrossRef]
- Garmendia, J.V.; García, A.H.; De Sanctis, C.V.; Hajdúch, M.; De Sanctis, J.B. Autoimmunity and Immunodeficiency in Severe SARS-CoV-2 Infection and Prolonged COVID-19. Curr. Issues Mol. Biol. 2022, 45, 33–50. [Google Scholar] [CrossRef]
- Carsetti, R.; Quintarelli, C.; Quinti, I.; Piano Mortari, E.; Zumla, A.; Ippolito, G.; Locatelli, F. The immune system of children: The key to understanding SARS-CoV-2 susceptibility? Lancet Child Adolesc. Health. 2020, 4, 414–416. [Google Scholar] [CrossRef]
- Bunyavanich, S.; Do, A.; Vicencio, A. Nasal Gene Expression of Angiotensin-Converting Enzyme 2 in Children and Adults. JAMA 2020, 323, 2427–2429. [Google Scholar] [CrossRef]
- Hoste, L.; Van Paemel, R.; Haerynck, F. Multisystem inflammatory syndrome in children related to COVID-19: A systematic review. Eur. J. Pediatr. 2021, 180, 2019–2034. [Google Scholar] [CrossRef]
- Hosseini, P.; Fallahi, M.S.; Erabi, G.; Pakdin, M.; Zarezadeh, S.M.; Faridzadeh, A.; Entezari, S.; Ansari, A.; Poudineh, M.; Deravi, N. Multisystem Inflammatory Syndrome and Autoimmune Diseases Following COVID-19: Molecular Mechanisms and Therapeutic Opportunities. Front. Mol. Biosci. 2022, 9, 804109. [Google Scholar] [CrossRef] [PubMed]
- Kunal, S.; Ish, P.; Sakthivel, P.; Malhotra, N.; Gupta, K. The emerging threat of multisystem inflammatory syndrome in adults (MIS-A) in COVID-19: A systematic review. Heart Lung 2022, 54, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Panaro, S.; Cattalini, M. The Spectrum of Manifestations of Severe Acute Respiratory Syndrome-Coronavirus 2 (SARS-CoV2) Infection in Children: What We Can Learn from Multisystem Inflammatory Syndrome in Children (MIS-C). Front. Med. 2021, 8, 747190. [Google Scholar] [CrossRef] [PubMed]
- Whitworth, H.; Sartain, S.E.; Kumar, R.; Armstrong, K.; Ballester, L.; Betensky, M.; Cohen, C.T.; Diaz, R.; Diorio, C.; Goldenberg, N.A.; et al. Rate of thrombosis in children and adolescents hospitalised with COVID-19 or MIS-C. Blood 2021, 138, 190–198. [Google Scholar] [CrossRef] [PubMed]
- James, P.T.; Ali, Z.; Armitage, A.E.; Bonell, A.; Cerami, C.; Drakesmith, H.; Prentice, A.M. The Role of Nutrition in COVID-19 Susceptibility and Severity of Disease: A Systematic Review. J. Nutr. 2021, 151, 1854–1878. [Google Scholar] [CrossRef] [PubMed]
- Venezuelan Ministry of Health Epidemiological Bulletin 8 April 2021–8 December 2022 (Ministerio del Poder Popular para la Salud COVID-19 Boletín Nacional. 8 de abril 2021 y 8 de Diciembre 2022). Available online: https://covid19.patria.org.ve/estadisticas-venezuela/ (accessed on 24 March 2023).
- Hair, J.F., Jr.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis, 5th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 1998. [Google Scholar]
- Holodick, N.E.; Rodríguez-Zhurbenko, N.; Hernández, A.M. Defining Natural Antibodies. Front. Immunol. 2017, 8, 872. [Google Scholar] [CrossRef]
- Capolunghi, F.; Rosado, M.M.; Sinibaldi, M.; Aranburu, A.; Carsetti, R. Why do we need IgM memory B cells? Immunol. Lett. 2013, 152, 114–120. [Google Scholar] [CrossRef]
- Cui, X.; Zhao, Z.; Zhang, T.; Guo, W.; Guo, W.; Zheng, J.; Cai, C. A systematic review and meta-analysis of children with Coronavirus Disease 2019 (COVID-19). J. Med. Virol. 2021, 93, 1057–1069. [Google Scholar] [CrossRef]
- Pierce, C.A.; Preston-Hurlburt, P.; Dai, Y.; Aschner, C.B.; Cheshenko, N.; Galen, B.; Herold, B.C. Immune responses to SARS-CoV-2 infection in hospitalised pediatric and adult patients. Sci. Transl. Med. 2020, 12, eabd5487. [Google Scholar] [CrossRef]
- Rehman, S.; Majeed, T.; Azam Ansari, M.; Ali, U.; Sabit, H.; Al-Suhaimi, E.A. Current Scenario of COVID-19 in Pediatric Age Group and Physiology of Immune and Thymus response. Saudi J. Biol. Sci. 2020, 27, 2567–2573. [Google Scholar] [CrossRef]
- Abrams, E.M.; Sinha, I.; Fernandes, R.M.; Hawcutt, D.B. Pediatric asthma and COVID-19: The known, the unknown, and the controversial. Pediatr. Pulmonol. 2020, 55, 3573–3578. [Google Scholar] [CrossRef] [PubMed]
- Adir, Y.; Saliba, W.; Beurnier, A.; Humbert, M. Asthma and COVID-19: An update. Eur. Respir. Rev. 2021, 30, 210152. [Google Scholar] [CrossRef] [PubMed]
- Rytter, M.J.; Kolte, L.; Briend, A.; Friis, H.; Christensen, V.B. The immune system in children with malnutrition—A systematic review. PLoS ONE 2014, 9, e105017. [Google Scholar] [CrossRef] [PubMed]
- Trofin, F.; Nastase, E.V.; Vâță, A.; Iancu, L.S.; Luncă, C.; Buzilă, E.R.; Vlad, M.A.; Dorneanu, O.S. The Immune, Inflammatory and Hematological Response in COVID-19 Patients, According to the Severity of the Disease. Microorganisms 2023, 11, 319. [Google Scholar] [CrossRef]
- Morhart, P.; Kehl, S.; Schuh, W.; Hermes, K.; Meltendorf, S.; Neubert, A.; Schneider, M.; Brunner-Weinzierl, M.; Schneider, H. Age-related Differences in Immune Reactions to SARS-CoV-2 Spike and Nucleocapsid Antigens. In Vivo 2023, 37, 70–78. [Google Scholar] [CrossRef]
- Barrera, G.J.; Sánchez, G. Cytokine modulation (IL-6, IL-8, IL-10) by human breast milk lipids on intestinal epithelial cells (Caco-2). J. Matern.-Fetal Neonatal Med. 2015, 29, 2504–2511. [Google Scholar] [CrossRef]
- Fiocchi, A.; Schünemann, H.J.; Brozek, J.; Restani, P.; Beyer, K.; Troncone, R.; Martelli, A.; Terracciano, L.; Bahna, S.L.; Rancé, F.; et al. Diagnosis and Rationale for Action against Cow’s Milk Allergy (DRACMA): A summary report. J. Allergy Clin. Immunol. 2010, 126, 11191128.e12. [Google Scholar] [CrossRef]
- Patel, V.K.; Shirbhate, E.; Patel, P.; Veerasamy, R.; Sharma, P.C.; Rajak, H. Corticosteroids for treatment of COVID-19: Effect, evidence, expectation and extent. Beni-Suef Univ. J. Basic Appl. Sci. 2021, 10, 78. [Google Scholar] [CrossRef]
- Avcu, G.; Arslan, A.; Arslan, S.Y.; Sahbudak Bal, Z.; Turan, C.; Ersayoglu, I.; Cebeci, K.; Kurugol, Z.; Ozkinay, F. Misdiagnosis of the multisystemic inflammatory syndrome in children: A diagnostic challenge. J. Paediatr. Child Health 2023, 54, 667–672. [Google Scholar] [CrossRef]
- Sachdeva, M.; Agarwal, A.; Sra, H.K.; Rana, M.; Pradhan, P.; Singh, M.; Saini, S.; Singh, M. Multisystem Inflammatory Syndrome Associated With COVID-19 in Children (MIS-C): A Systematic Review of Studies from India. Indian Pediatr. 2022, 59, 563–569. [Google Scholar] [CrossRef]
- Vasichkina, E.; Alekseeva, D.; Kudryavtsev, I.; Glushkova, A.; Starshinova, A.Y.; Malkova, A.; Kudlay, D.; Starshinova, A. COVID-19 Heart Lesions in Children: Clinical, Diagnostic and Immunological Changes. Int. J. Mol. Sci. 2023, 24, 1147. [Google Scholar] [CrossRef] [PubMed]
- Khoo, W.H.; Jackson, K.; Phetsouphanh, C.; Zaunders, J.J.; Alquicira-Hernandez, J.; Yazar, S.; Ruiz-Diaz, S.; Singh, M.; Dhenni, R.; Kyaw, W.; et al. Tracking the clonal dynamics of SARS-CoV-2-specific T cells in children and adults with mild/asymptomatic COVID-19. Clin. Immunol. 2023, 246, 109209. [Google Scholar] [CrossRef] [PubMed]
- Mayora, S.; Zabaleta-Lanz, M.; Martínez, W.; Toro, F.; De Sanctis, J.B.; García, A. Lymphocyte subpopulations in Venezuelan patients infected with SARS CoV-2. Gac. Méd. Caracas 2020, 128 (Suppl. S1), S74–S78. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n | % |
|---|---|---|
| Sex | ||
| Male | 34 | 47.2 |
| Female | 38 | 52.8 |
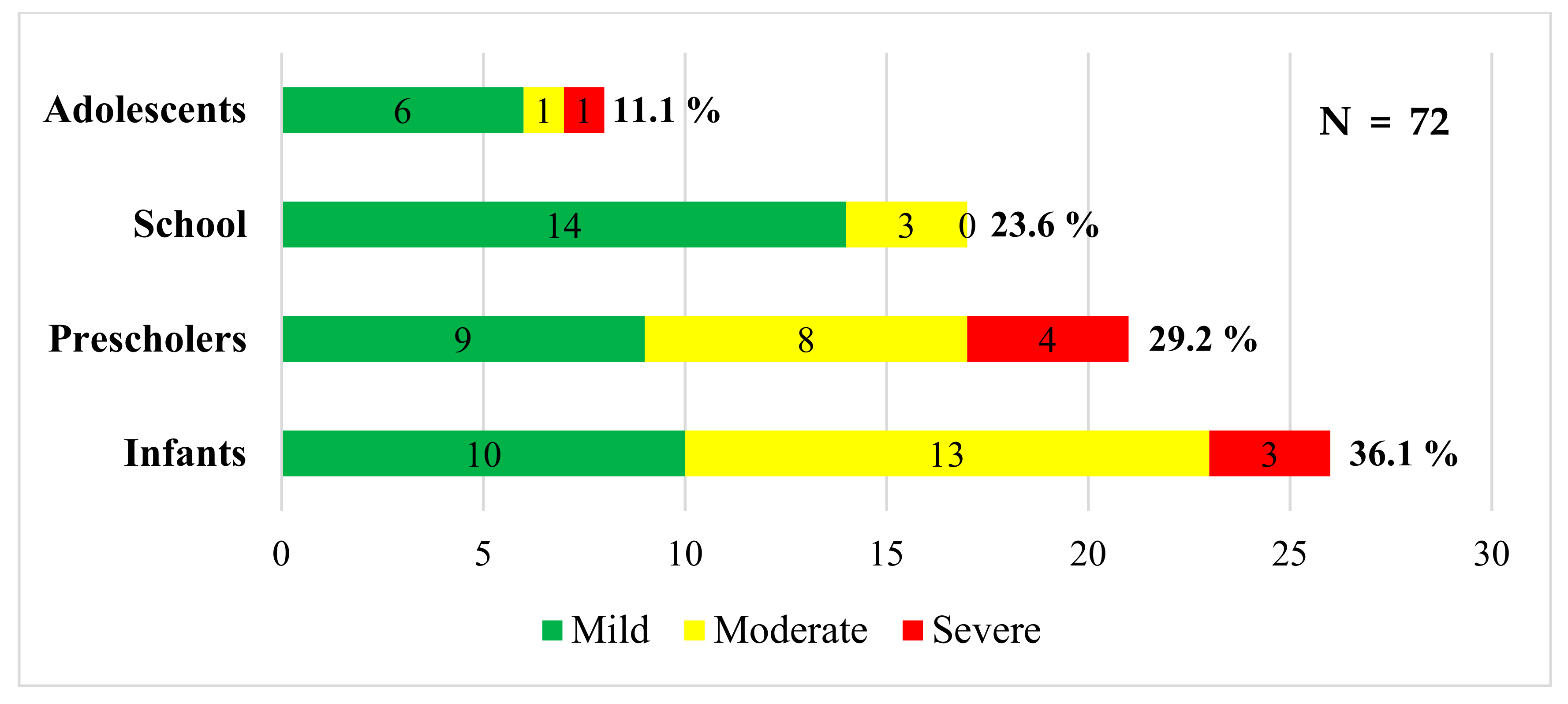
| Age group | ||
| Infant | 26 | 36.1 |
| Preschooler | 21 | 29.2 |
| School-age | 17 | 23.6 |
| Adolescent | 8 | 11.1 |
| COVID-19 severeness | ||
| Mild | 38 | 52.8 |
| Moderate | 26 | 36.1 |
| Severe | 8 | 11.1 |
| Nutrition Diagnosis | ||
| Malnutrition | 25 | 34.7 |
| Normal | 44 | 61.1 |
| Overweight–obese | 3 | 4.2 |
| Comorbidities | ||
| Yes | 20 | 27.8 |
| No | 52 | 72.2 |
| Complications | ||
| No | 43 | 59.7 |
| Bacterial coinfection | 6 | 8.3 |
| Viral coinfection | 1 | 1.4 |
| MIS-C | 22 | 30.6 |
| Treatment received | ||
| No steroids | 30 | 41.7 |
| Dexamethasone | 30 | 41.7 |
| Hydrocortisone | 5 | 6.9 |
| Methylprednisolone | 4 | 5.6 |
| Dexamethasone + immunoglobulin | 3 | 4.2 |
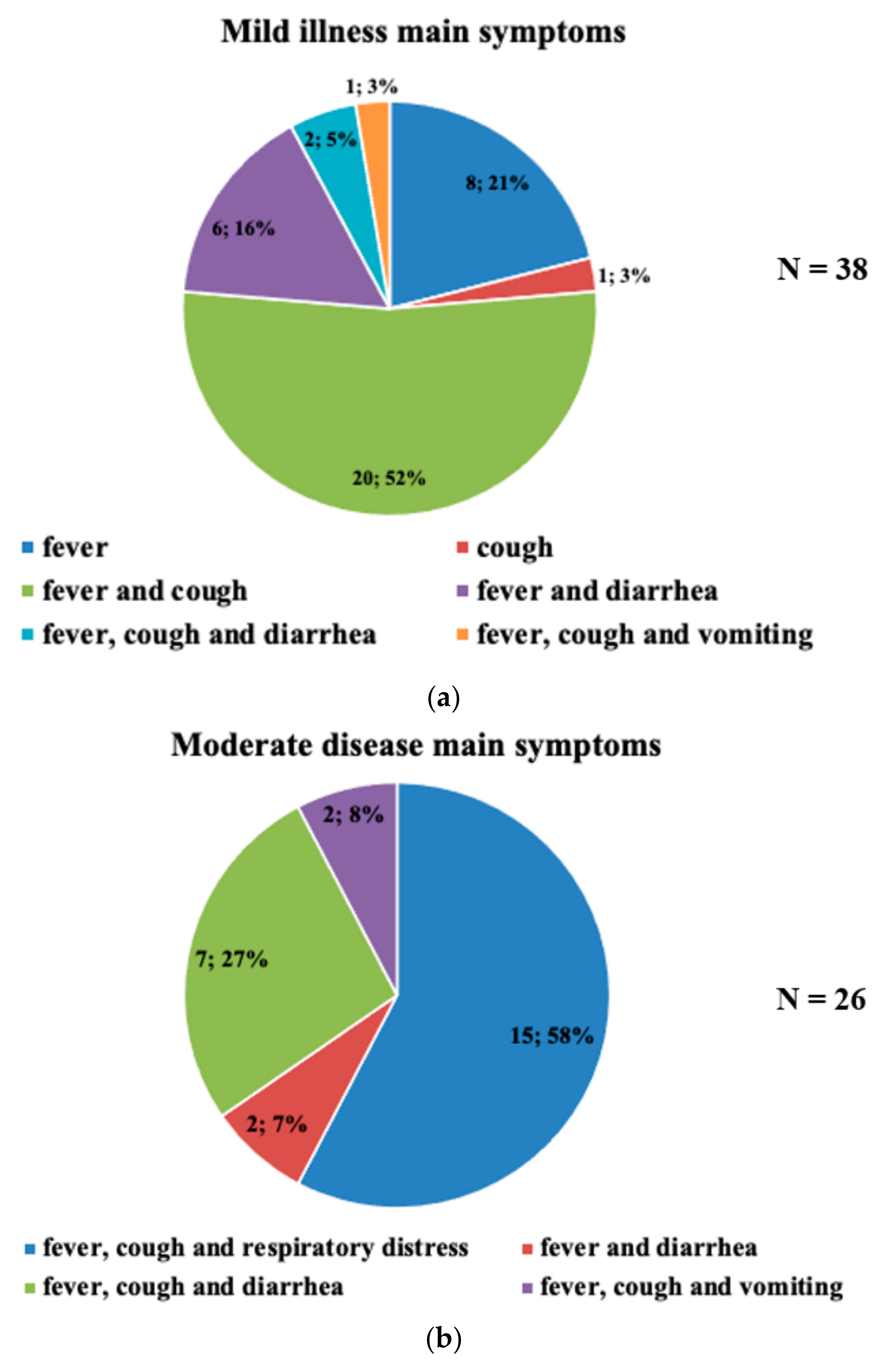
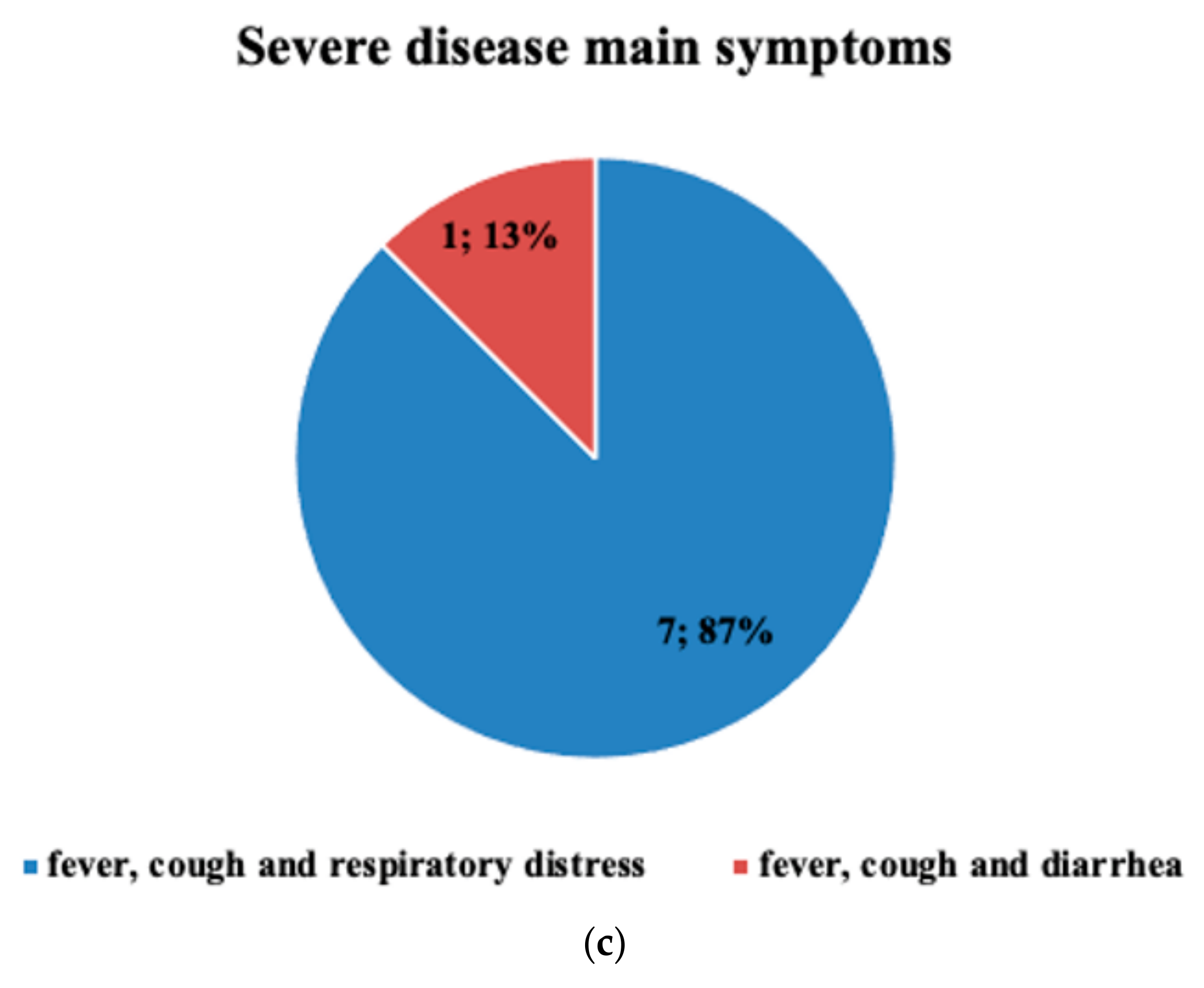
| Symptoms | ||
| Fever | 66 | 91.6 |
| Cough | 56 | 77.7 |
| Diarrhea | 38 | 52.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crespo, F.I.; Mayora, S.J.; De Sanctis, J.B.; Martínez, W.Y.; Zabaleta-Lanz, M.E.; Toro, F.I.; Deibis, L.H.; García, A.H. SARS-CoV-2 Infection in Venezuelan Pediatric Patients—A Single Center Prospective Observational Study. Biomedicines 2023, 11, 1409. https://doi.org/10.3390/biomedicines11051409
Crespo FI, Mayora SJ, De Sanctis JB, Martínez WY, Zabaleta-Lanz ME, Toro FI, Deibis LH, García AH. SARS-CoV-2 Infection in Venezuelan Pediatric Patients—A Single Center Prospective Observational Study. Biomedicines. 2023; 11(5):1409. https://doi.org/10.3390/biomedicines11051409
Chicago/Turabian StyleCrespo, Francis Isamarg, Soriuska José Mayora, Juan Bautista De Sanctis, Wendy Yaqueline Martínez, Mercedes Elizabeth Zabaleta-Lanz, Félix Isidro Toro, Leopoldo Humberto Deibis, and Alexis Hipólito García. 2023. "SARS-CoV-2 Infection in Venezuelan Pediatric Patients—A Single Center Prospective Observational Study" Biomedicines 11, no. 5: 1409. https://doi.org/10.3390/biomedicines11051409
APA StyleCrespo, F. I., Mayora, S. J., De Sanctis, J. B., Martínez, W. Y., Zabaleta-Lanz, M. E., Toro, F. I., Deibis, L. H., & García, A. H. (2023). SARS-CoV-2 Infection in Venezuelan Pediatric Patients—A Single Center Prospective Observational Study. Biomedicines, 11(5), 1409. https://doi.org/10.3390/biomedicines11051409