
The Utility of Faecal Calprotectin, Lactoferrin and Other Faecal Biomarkers in Discriminating Endoscopic Activity in Crohn’s Disease: A Systematic Review and Meta-Analysis
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
2.5. Deviations from Protocol
3. Results
3.1. Study Characteristics
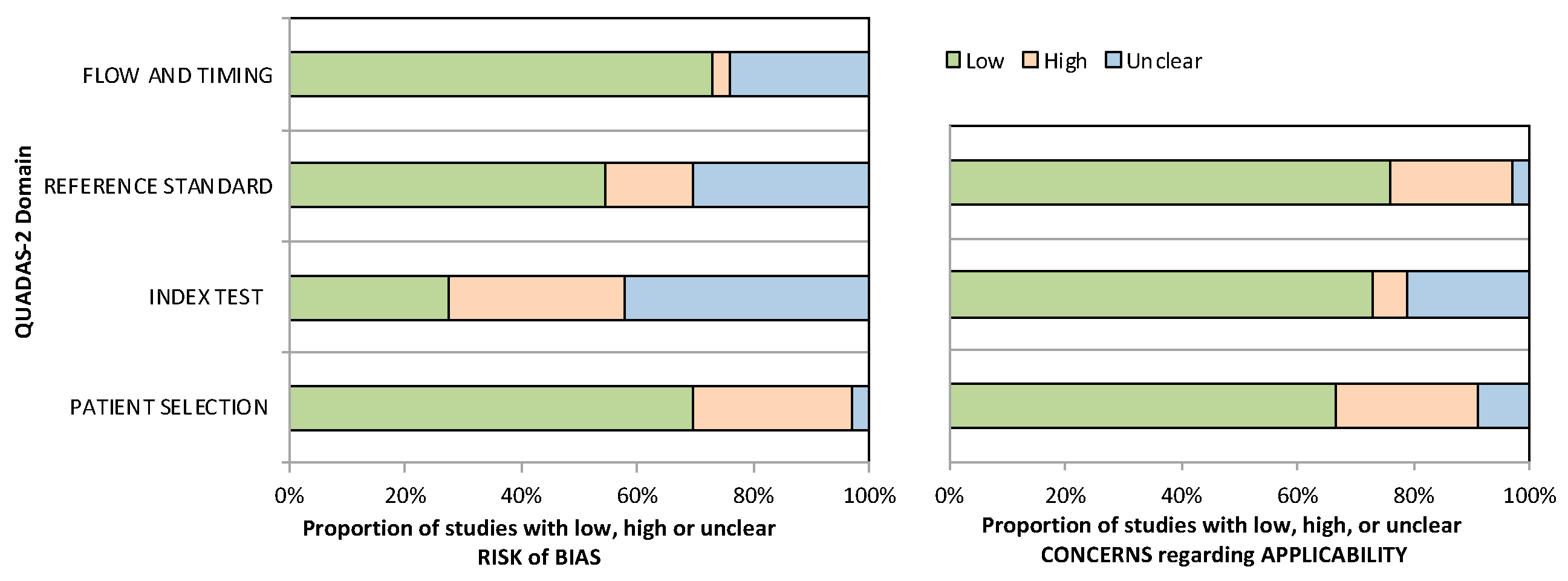
3.2. Study Quality
3.3. Faecal Calprotectin
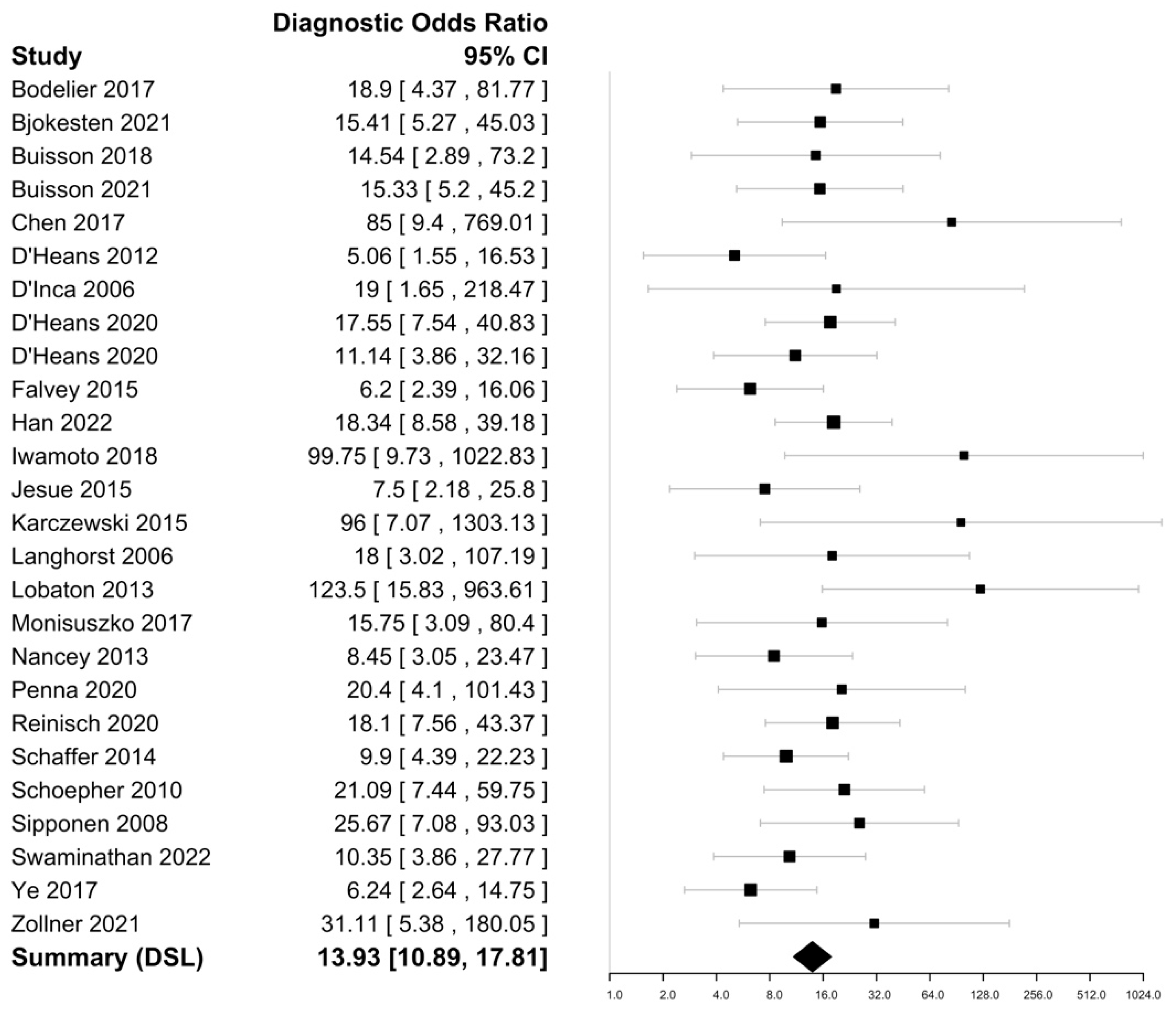
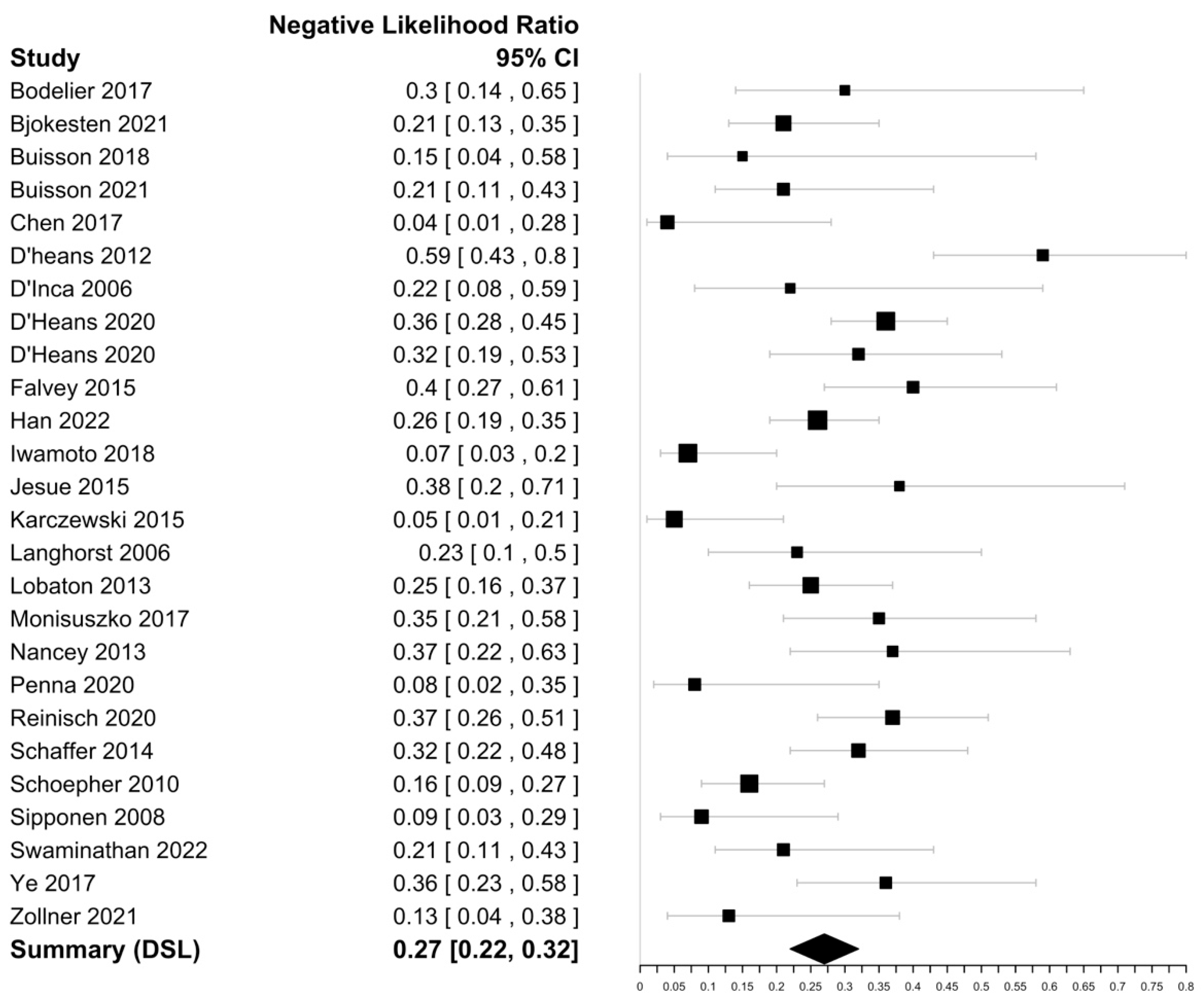
3.3.1. Detection of Endoscopic Activity
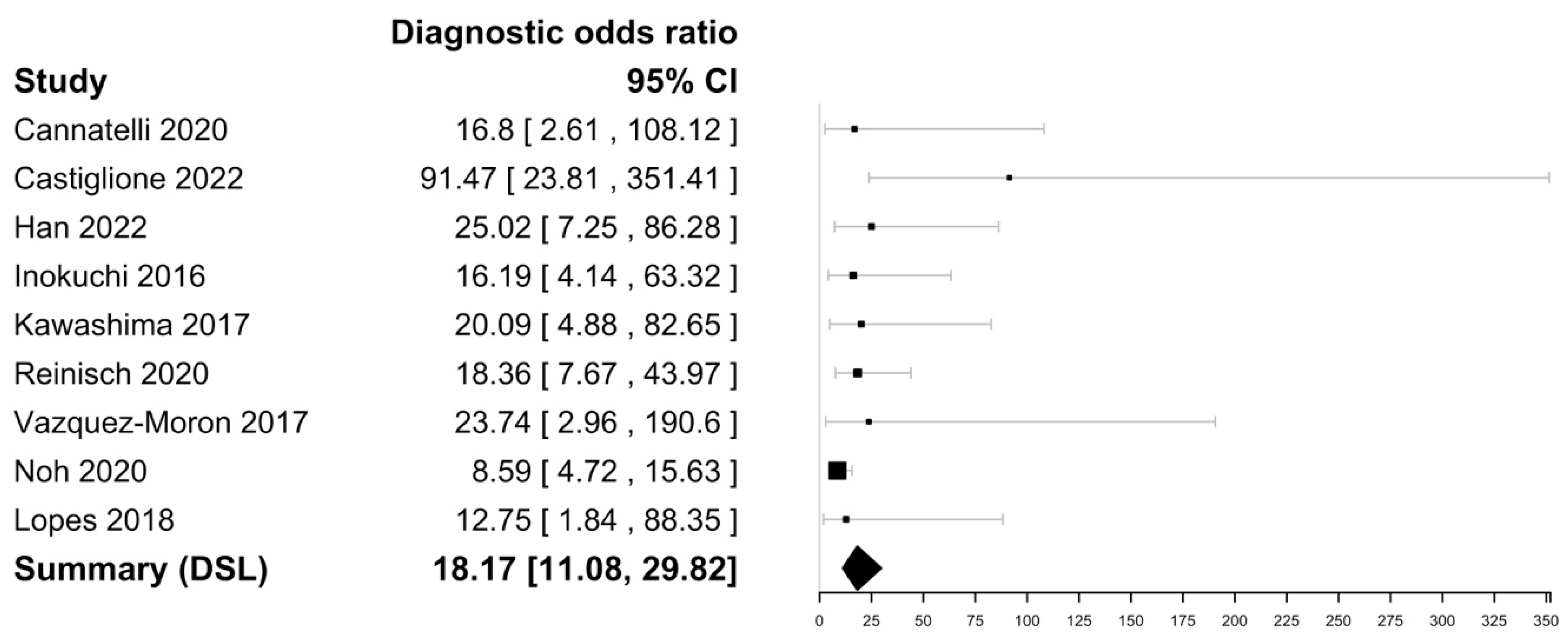
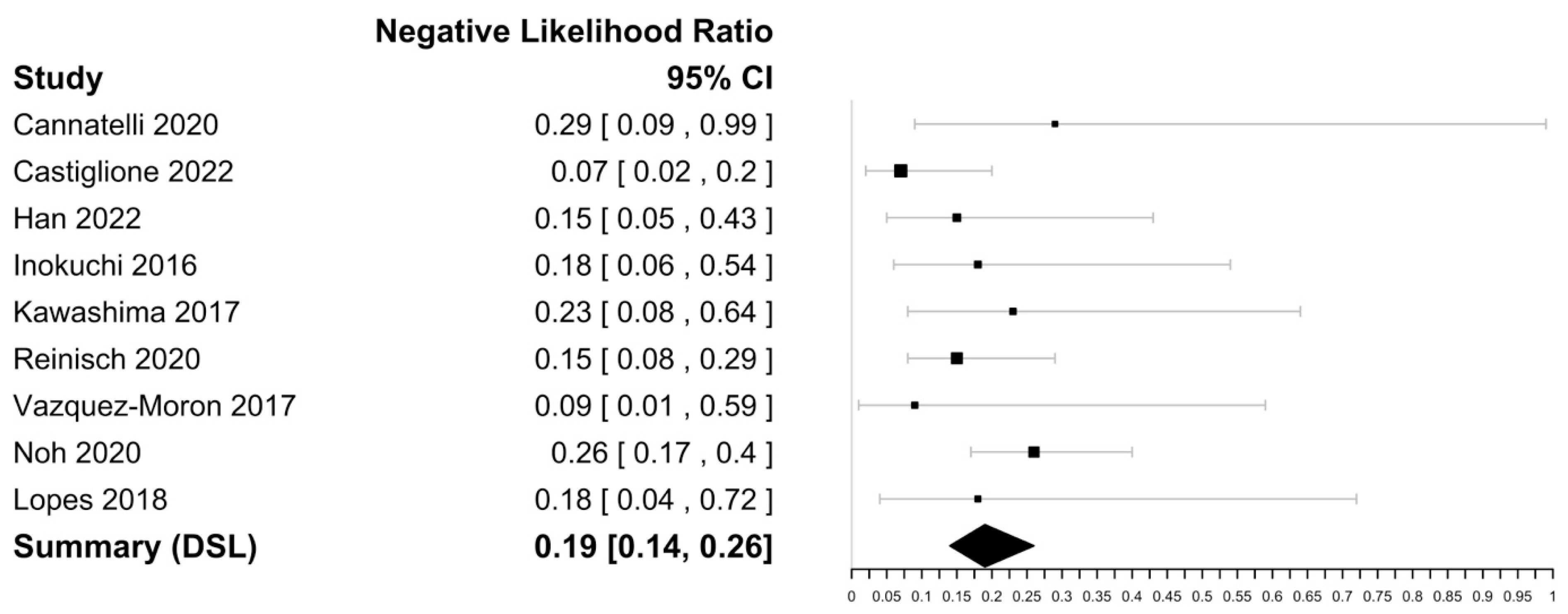
3.3.2. Prediction of Mucosal Healing
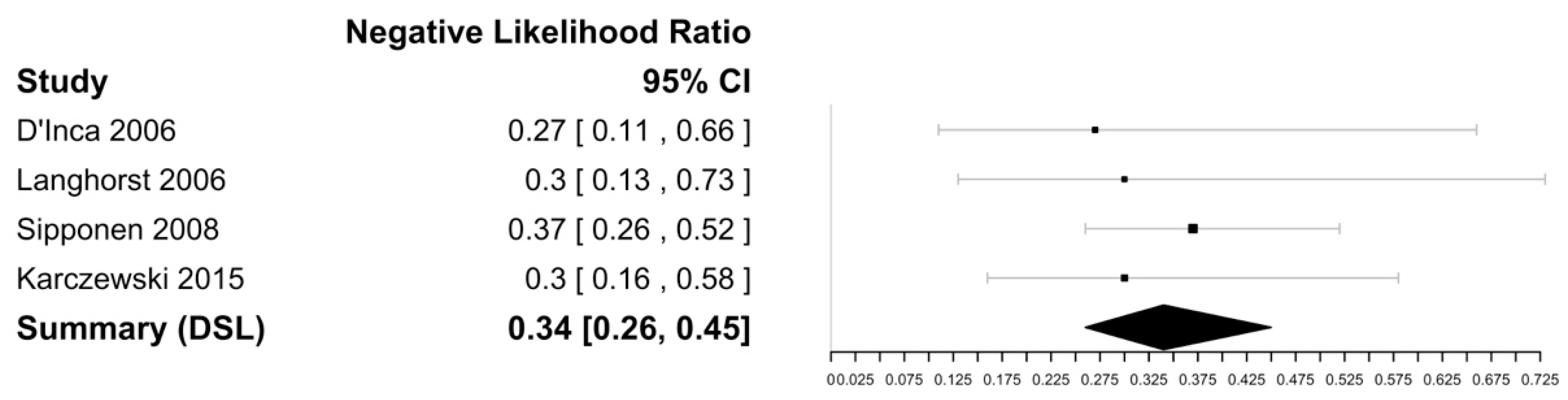
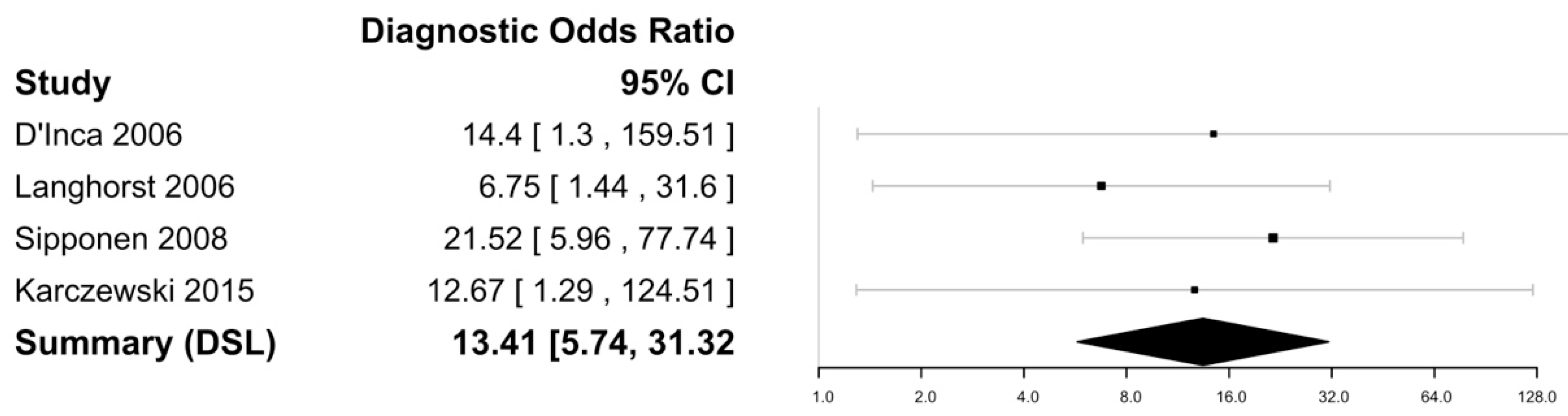
3.4. Faecal Lactoferrin
3.5. Other Biomarkers
- Faecal Lipocalin-2
- Faecal metalloprotease 9
- Neopterin
- Faecal myeloperoxidase
- Faecal chitinase 3-like 1
- PMN-e
- FIT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, M.; Christensen, H.S.; Bøgsted, M.; Colombel, J.F.; Jess, T.; Allin, K.H. The Rising Burden of Inflammatory Bowel Disease in Denmark Over Two Decades: A Nationwide Cohort Study. Gastroenterology 2022, 163, 1547–1554.e5. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Eun, C.S. Inflammatory bowel disease in Korea: Epidemiology and pathophysiology. Korean J. Intern. Med. 2022, 37, 885–894. [Google Scholar] [CrossRef] [PubMed]
- Argüelles-Arias, F.; Rodríguez-Oballe, J.; Duarte-Chang, C.; Castro-Laria, L.; García-Montes, J.M.; Caunedo-Álvarez, A.; Herrerías-Gutiérrez, J.M. Capsule endoscopy in the small bowel Crohn’s disease. Gastroenterol. Res. Pract. 2014, 2014, 529136. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Loftus, E.V.; Colombel, J.F.; Sandborn, W.J. Long-term complications, extraintestinal manifestations, and mortality in adult Crohn’s disease in population-based cohorts. Inflamm. Bowel Dis. 2011, 17, 471–478. [Google Scholar] [CrossRef]
- Cho, C.W.; You, M.W.; Oh, C.H.; Lee, C.K.; Moon, S.K. Long-term Disease Course of Crohn’s Disease: Changes in Disease Location, Phenotype, Activities, and Predictive Factors. Gut Liver 2022, 16, 157–170. [Google Scholar] [CrossRef]
- Adamina, M.; Bonovas, S.; Raine, T.; Spinelli, A.; Warusavitarne, J.; Armuzzi, A.; Bachmann, O.; Bager, P.; Biancone, L.; Bokemeyer, B.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Surgical Treatment. J. Crohn's Colitis 2020, 14, 155–168. [Google Scholar] [CrossRef]
- Rieder, F.; Latella, G.; Magro, F.; Yuksel, E.S.; Higgins, P.D.; Di Sabatino, A.; de Bruyn, J.R.; Rimola, J.; Brito, J.; Bettenworth, D.; et al. European Crohn’s and Colitis Organisation Topical Review on Prediction, Diagnosis and Management of Fibrostenosing Crohn’s Disease. J. Crohn's Colitis 2016, 10, 873–885. [Google Scholar] [CrossRef]
- Torres, J.; Bonovas, S.; Doherty, G.; Kucharzik, T.; Gisbert, J.P.; Raine, T.; Adamina, M.; Armuzzi, A.; Bachmann, O.; Bager, P.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. J. Crohn's Colitis 2020, 14, 4–22. [Google Scholar] [CrossRef]
- Kumar, A.; Cole, A.; Segal, J.; Smith, P.; Limdi, J.K. A review of the therapeutic management of Crohn’s disease. Therap. Adv. Gastroenterol. 2022, 15, 17562848221078456. [Google Scholar] [CrossRef]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Borralho Nunes, P.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J. Crohn's Colitis 2019, 13, 144–164. [Google Scholar] [CrossRef]
- Geyl, S.; Guillo, L.; Laurent, V.; D’Amico, F.; Danese, S.; Peyrin-Biroulet, L. Transmural healing as a therapeutic goal in Crohn’s disease: A systematic review. Lancet Gastroenterol. Hepatol. 2021, 6, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Peyrin-Biroulet, L.; Sandborn, W.; Sands, B.E.; Reinisch, W.; Bemelman, W.; Bryant, R.V.; D’Haens, G.; Dotan, I.; Dubinsky, M.; Feagan, B.; et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): Determining Therapeutic Goals for Treat-to-Target. Am. J. Gastroenterol. 2015, 110, 1324–1338. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Ricciuto, A.; Lewis, A.; D’Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef]
- af Björkesten, C.G.; Nieminen, U.; Turunen, U.; Arkkila, P.; Sipponen, T.; Färkkilä, M. Surrogate markers and clinical indices, alone or combined, as indicators for endoscopic remission in anti-TNF-treated luminal Crohn’s disease. Scand. J. Gastroenterol. 2012, 47, 528–537. [Google Scholar] [CrossRef] [PubMed]
- Buisson, A.; Mak, W.Y.; Andersen, M.J.; Lei, D.; Pekow, J.; Cohen, R.D.; Kahn, S.A.; Pereira, B.; Rubin, D.T. Fecal Calprotectin Is Highly Effective to Detect Endoscopic Ulcerations in Crohn’s Disease Regardless of Disease Location. Inflamm. Bowel Dis. 2021, 27, 1008–1016. [Google Scholar] [CrossRef]
- Mohamed, G.; Bohra, A.; Segal, J. Sensitivity and Specificity of Stool Markers in Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. PROSPERO 2022 CRD42022354526. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022354526 (accessed on 13 April 2023).
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Glas, A.S.; Lijmer, J.G.; Prins, M.H.; Bonsel, G.J.; Bossuyt, P.M. The diagnostic odds ratio: A single indicator of test performance. J. Clin. Epidemiol. 2003, 56, 1129–1135. [Google Scholar] [CrossRef]
- Doebler, P. Comprehensive R Archive Network Mada: Meta-Analysis of Diagnostic Accuracy. Available online: https://cran.r-project.org/web/packages/mada/index.html (accessed on 13 April 2023).
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Deeks, J.J.; Macaskill, P.; Irwig, L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J. Clin. Epidemiol. 2005, 58, 882–893. [Google Scholar] [CrossRef] [PubMed]
- Han, W.; Wu, J.; Zhang, P.; Hu, N.; Mei, Q.; Hu, J. Fecal calprotectin predicts endoscopic activity and mucosal healing of small bowel Crohn’s disease evaluated by double-balloon endoscopy. Int. J. Color. Dis. 2022, 37, 1953–1961. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, F.; Matsuoka, K.; Motobayashi, M.; Takenaka, K.; Kuno, T.; Tanaka, K.; Tsukui, Y.; Kobayashi, S.; Yoshida, T.; Fujii, T.; et al. Prediction of disease activity of Crohn’s disease through fecal calprotectin evaluated by balloon-assisted endoscopy. J. Gastroenterol. Hepatol. 2018, 33, 1984–1989. [Google Scholar] [CrossRef] [PubMed]
- Bodelier, A.G.; Jonkers, D.; van den Heuvel, T.; de Boer, E.; Hameeteman, W.; Masclee, A.A.; Pierik, M.J. High Percentage of IBD Patients with Indefinite Fecal Calprotectin Levels: Additional Value of a Combination Score. Dig. Dis. Sci. 2017, 62, 465–472. [Google Scholar] [CrossRef]
- Buisson, A.; Vazeille, E.; Minet-Quinard, R.; Goutte, M.; Bouvier, D.; Goutorbe, F.; Pereira, B.; Barnich, N.; Bommelaer, G. Fecal Matrix Metalloprotease-9 and Lipocalin-2 as Biomarkers in Detecting Endoscopic Activity in Patients With Inflammatory Bowel Diseases. J. Clin. Gastroenterol. 2018, 52, e53–e62. [Google Scholar] [CrossRef]
- Chen, J.M.; Liu, T.; Gao, S.; Tong, X.D.; Deng, F.H.; Nie, B. Efficacy of noninvasive evaluations in monitoring inflammatory bowel disease activity: A prospective study in China. World J. Gastroenterol. 2017, 23, 8235–8247. [Google Scholar] [CrossRef]
- D’Haens, G.; Ferrante, M.; Vermeire, S.; Baert, F.; Noman, M.; Moortgat, L.; Geens, P.; Iwens, D.; Aerden, I.; Van Assche, G.; et al. Fecal calprotectin is a surrogate marker for endoscopic lesions in inflammatory bowel disease. Inflamm. Bowel Dis. 2012, 18, 2218–2224. [Google Scholar] [CrossRef]
- D’Haens, G.; Kelly, O.; Battat, R.; Silverberg, M.S.; Laharie, D.; Louis, E.; Savarino, E.; Bodini, G.; Yarur, A.; Boland, B.S.; et al. Development and Validation of a Test to Monitor Endoscopic Activity in Patients With Crohn’s Disease Based on Serum Levels of Proteins. Gastroenterology 2020, 158, 515–526.e10. [Google Scholar] [CrossRef]
- D’Incà, R.; Dal Pont, E.; Di Leo, V.; Ferronato, A.; Fries, W.; Vettorato, M.G.; Martines, D.; Sturniolo, G.C. Calprotectin and lactoferrin in the assessment of intestinal inflammation and organic disease. Int. J. Color. Dis. 2007, 22, 429–437. [Google Scholar] [CrossRef]
- Falvey, J.D.; Hoskin, T.; Meijer, B.; Ashcroft, A.; Walmsley, R.; Day, A.S.; Gearry, R.B. Disease activity assessment in IBD: Clinical indices and biomarkers fail to predict endoscopic remission. Inflamm. Bowel Dis. 2015, 21, 824–831. [Google Scholar] [CrossRef]
- Jusué, V.; Chaparro, M.; Gisbert, J.P. Accuracy of fecal calprotectin for the prediction of endoscopic activity in patients with inflammatory bowel disease. Dig. Liver Dis. 2018, 50, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Karczewski, J.; Swora-Cwynar, E.; Rzymski, P.; Poniedziałek, B.; Adamski, Z. Selected biologic markers of inflammation and activity of Crohn’s disease. Autoimmunity 2015, 48, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Langhorst, J.; Elsenbruch, S.; Koelzer, J.; Rueffer, A.; Michalsen, A.; Dobos, G.J. Noninvasive markers in the assessment of intestinal inflammation in inflammatory bowel diseases: Performance of fecal lactoferrin, calprotectin, and PMN-elastase, CRP, and clinical indices. Am. J. Gastroenterol. 2008, 103, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Lobatón, T.; López-García, A.; Rodríguez-Moranta, F.; Ruiz, A.; Rodríguez, L.; Guardiola, J. A new rapid test for fecal calprotectin predicts endoscopic remission and postoperative recurrence in Crohn’s disease. J. Crohn's Colitis 2013, 7, e641–e651. [Google Scholar] [CrossRef]
- Moniuszko, A.; Głuszek, S.; Rydzewska, G. Rapid fecal calprotectin test for prediction of mucosal inflammation in ulcerative colitis and Crohn disease: A prospective cohort study. Pol. Arch. Intern. Med. 2017, 127, 312–318. [Google Scholar] [CrossRef]
- Nancey, S.; Boschetti, G.; Moussata, D.; Cotte, E.; Peyras, J.; Cuerq, C.; Haybrard, J.; Charlois, A.L.; Mialon, A.; Chauvenet, M.; et al. Neopterin is a novel reliable fecal marker as accurate as calprotectin for predicting endoscopic disease activity in patients with inflammatory bowel diseases. Inflamm. Bowel Dis. 2013, 19, 1043–1052. [Google Scholar] [CrossRef]
- Penna, F.G.C.; Rosa, R.M.; Pereira, F.H.; Cunha, P.F.S.; Sousa, S.C.S.; Ferrari, T.C.A.; Cara, C.; Ferrari, M.L.A. Combined evaluation of fecal calprotectin and C-reactive protein as a therapeutic target in the management of patients with Crohn’s disease. Gastroenterol. Hepatol. 2021, 44, 87–95. [Google Scholar] [CrossRef]
- Reinisch, W.; Panaccione, R.; Bossuyt, P.; Baert, F.; Armuzzi, A.; Hébuterne, X.; Travis, S.; Danese, S.; Sandborn, W.J.; Schreiber, S.; et al. Association of Biomarker Cutoffs and Endoscopic Outcomes in Crohn’s Disease: A Post Hoc Analysis From the CALM Study. Inflamm. Bowel Dis. 2020, 26, 1562–1571. [Google Scholar] [CrossRef]
- Schaffer, T.; Schoepfer, A.M.; Seibold, F.; Swiss IBD Cohort Study Group. Serum ficolin-2 correlates worse than fecal calprotectin and CRP with endoscopic Crohn’s disease activity. J. Crohns Colitis 2014, 8, 1125–1132. [Google Scholar] [CrossRef]
- Schoepfer, A.M.; Beglinger, C.; Straumann, A.; Trummler, M.; Vavricka, S.R.; Bruegger, L.E.; Seibold, F. Fecal calprotectin correlates more closely with the Simple Endoscopic Score for Crohn’s disease (SES-CD) than CRP, blood leukocytes, and the CDAI. Am. J. Gastroenterol. 2010, 105, 162–169. [Google Scholar] [CrossRef]
- Sipponen, T.; Savilahti, E.; Kolho, K.L.; Nuutinen, H.; Turunen, U.; Färkkilä, M. Crohn’s disease activity assessed by fecal calprotectin and lactoferrin: Correlation with Crohn’s disease activity index and endoscopic findings. Inflamm. Bowel Dis. 2008, 14, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Swaminathan, A.; Borichevsky, G.M.; Edwards, T.S.; Hirschfeld, E.; Mules, T.C.; Frampton, C.M.A.; Day, A.S.; Hampton, M.B.; Kettle, A.J.; Gearry, R.B. Faecal Myeloperoxidase as a Biomarker of Endoscopic Activity in Inflammatory Bowel Disease. J. Crohn's Colitis 2022, 16, 1862–1873. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Cheng, W.; Chen, B.Q.; Lan, X.; Wang, S.D.; Wu, X.C.; Huang, W.; Wang, F.Y. Levels of Faecal Calprotectin and Magnetic Resonance Enterocolonography Correlate with Severity of Small Bowel Crohn’s Disease: A Retrospective Cohort Study. Sci. Rep. 2017, 7, 1970. [Google Scholar] [CrossRef] [PubMed]
- Zollner, A.; Schmiderer, A.; Reider, S.J.; Oberhuber, G.; Pfister, A.; Texler, B.; Watschinger, C.; Koch, R.; Effenberger, M.; Raine, T.; et al. Faecal Biomarkers in Inflammatory Bowel Diseases: Calprotectin Versus Lipocalin-2-a Comparative Study. J. Crohn's Colitis 2021, 15, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Vázquez Morón, J.M.; Pallarés Manrique, H.; Machancoses, F.H.; Ramos Lora, M.; Ruiz Frutos, C. Accurate cut-offs for predicting endoscopic activity and mucosal healing in Crohn’s disease with fecal calprotectin. Rev. Esp. Enferm. Dig. 2017, 109, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Inokuchi, T.; Kato, J.; Hiraoka, S.; Takashima, S.; Nakarai, A.; Takei, D.; Sugihara, Y.; Takahara, M.; Kawano, S.; Harada, K.; et al. Fecal Immunochemical Test Versus Fecal Calprotectin for Prediction of Mucosal Healing in Crohn’s Disease. Inflamm. Bowel Dis. 2016, 22, 1078–1085. [Google Scholar] [CrossRef]
- Kawashima, K.; Ishihara, S.; Yuki, T.; Fukuba, N.; Sonoyama, H.; Kazumori, H.; Yamashita, N.; Tada, Y.; Kusunoki, R.; Oka, A.; et al. Fecal Calprotectin More Accurately Predicts Endoscopic Remission of Crohn’s Disease than Serological Biomarkers Evaluated Using Balloon-assisted Enteroscopy. Inflamm. Bowel Dis. 2017, 23, 2027–2034. [Google Scholar] [CrossRef]
- Lopes, S.; Andrade, P.; Afonso, J.; Cunha, R.; Rodrigues-Pinto, E.; Ramos, I.; Macedo, G.; Magro, F. Monitoring Crohn’s disease activity: Endoscopy, fecal markers and computed tomography enterography. Therap. Adv. Gastroenterol. 2018, 11, 1756284818769075. [Google Scholar] [CrossRef]
- Noh, S.M.; Oh, E.H.; Park, S.H.; Lee, J.B.; Kim, J.Y.; Park, J.C.; Kim, J.; Ham, N.S.; Hwang, S.W.; Yang, D.H.; et al. Association of Faecal Calprotectin Level and Combined Endoscopic and Radiological Healing in Patients With Crohn’s Disease Receiving Anti-tumour Necrosis Factor Therapy. J. Crohn's Colitis 2020, 14, 1231–1240. [Google Scholar] [CrossRef]
- Buisson, A.; Vazeille, E.; Minet-Quinard, R.; Goutte, M.; Bouvier, D.; Goutorbe, F.; Pereira, B.; Barnich, N.; Bommelaer, G. Faecal chitinase 3-like 1 is a reliable marker as accurate as faecal calprotectin in detecting endoscopic activity in adult patients with inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2016, 43, 1069–1079. [Google Scholar] [CrossRef] [PubMed]
- Cannatelli, R.; Bazarova, A.; Zardo, D.; Nardone, O.M.; Shivaji, U.; Smith, S.C.L.; Gkoutos, G.; Ricci, C.; Gui, X.S.; Ghosh, S.; et al. Fecal Calprotectin Thresholds to Predict Endoscopic Remission Using Advanced Optical Enhancement Techniques and Histological Remission in IBD Patients. Inflamm. Bowel Dis. 2021, 27, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Castiglione, F.; Imperatore, N.; Testa, A.; de Sire, R.; Nardone, O.M.; Ricciolino, S.; Di Luna, I.; Patturelli, M.; Villani, G.D.; Olmo, O.; et al. Exploring the concept of deep remission in Crohn’s disease: Correlation between transmural healing and biomarkers. Therap. Adv. Gastroenterol. 2022, 15, 17562848221110643. [Google Scholar] [CrossRef] [PubMed]
- Rokkas, T.; Portincasa, P.; Koutroubakis, I.E. Fecal calprotectin in assessing inflammatory bowel disease endoscopic activity: A diagnostic accuracy meta-analysis. J. Gastrointestin. Liver Dis. 2018, 27, 299–306. [Google Scholar] [CrossRef] [PubMed]
- 56 Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Name, Year) | Nation of Origin | CD Patients (n=) | Definition of Endoscopic Activity (Inactive/Active) | Optimal FC Cut-off | Sensitivity (95% CI) | Specificity (95% CI) |
|---|---|---|---|---|---|---|
| Björkesten 2021 [15] | Finland | 126 | SES-CD ≤ 2/SES-CD > 2 | 94 µg/g | 84% (76–90) | 74% (54–87) |
| Bodelier 2017 [26] | Netherlands | 50 | SES-CD ≤ 3/SES-CD > 3 | 250 µg/g | 74% (51–88) | 87% (71–95) |
| Buisson 2021 [16] | France | 83 | Absence of ulcers/ presence of ulcers | 250 µg/g | 84% (70–91) | 74% (58–85) |
| Buisson 2018 [27] | France | 54 | Absence of ulcers/presence of ulcers | 250 µg/g | 91% (73–98) | 58% (41–73) |
| Chen 2017 [28] | China | 56 | SES-CD ≤ 2/SES-CD > 2 | 250 µg/g | 97% (85–99) | 71% (50–86) |
| D’Haens 2012 [29] | Netherlands | 87 | Absence of ulcers/presence of ulcers | 250 µg/g | 52% (40–63) | 83% (63–93) |
| D’Haens 2020 * [30] | Netherlands | 247 81 | SES-CD ≤ 2/SES-CD > 2 SES-CD ≤ 2/SES-CD > 2 | 250 µg/g 50 µg/g | 68% (61–75) 75% (61–85) | 88% (78–94) 78% (62–89) |
| D’Inca 2006 [31] | Italy | 31 | SES-CD ≤ 3/SES-CD > 3 | 80 µg/g | 83% (63–93) | 80% (38–96) |
| Falvey 2015 [32] | New Zealand | 108 | SES-CD ≤ 2/SES-CD > 2 | 125 µg/g | 71% (60–80) | 71% (53–84) |
| Han 2022 [24] | China | 254 | pSES-CD = 0/pSES-CD ≥ 1 | 156 µg/g | 78% (72–83) | 83% (72–90) |
| Iwamoto 2018 [25] | Japan | 69 | eSES-CD = 0/eSES-CD ≥ 1 | 92 mg/kg | 93% (84–97) | 88% (53–91) |
| Jesue 2018 [33] | Spain | 52 | SES-CD = 0/SES-CD ≥ 1 | 54 µg/g | 71% (53–84) | 75% (55–88) |
| Karczewski 2015 [34] | Poland | 55 | CDEIS < 3/CDEIS ≥ 3 | 76 µg/g | 96% (87–99) | 80% (38–96) |
| Langhorst 2006 [35] | Germany | 43 | Authors’ score | 48 µg/mL | 82% (66–91) | 80% (49–94) |
| Lobaton 2013 [36] | Spain | 115 | CDEIS < 3/CDEIS ≥ 3 | 274 µg/g | 76% (65–84) | 98% (87–99) |
| Monisuszko 2017 [37] | Poland | 57 | SES-CD ≤ 3/SES-CD > 3 | 238.5 µg/g | 69% (53–81) | 88% (64–97) |
| Nancey 2013 [38] | France | 78 | SES-CD ≤ 2/SES-CD > 2 | 250 µg/g | 71% (55–82) | 77% (62–87) |
| Penna 2020 [39] | Italy | 80 | SES-CD ≤ 2/SES-CD > 2 | 155 µg/g | 96% (87–99%) | 45% (28–63) |
| Reinisch 2020 [40] | Austria | 156 | CDEIS ≤ 3/CDEIS > 3 | 250 µg/g | 67% (56–76) | 90% (81–95) |
| Schaffer 2014 [41] | Switzerland | 136 | SES-CD ≤ 3/SES-CD > 3 | 250 µg/g | 75% (65–83%) | 76% (63–86) |
| Schoepher 2010 [42] | Switzerland | 122 | SES-CD ≤ 3/SES-CD > 3 | 70 µg/g | 89% (81–93) | 72% (53–86) |
| Sipponen 2008 [43] | Finland | 116 | CDEIS ≤ 3/CDEIS > 3 | 200 µg/g | 94% (84–98) | 61% (48–73) |
| Swaminathan 2022 [44] | New Zealand | 100 | SES-CD ≤ 2/SES-CD > 2 | 58 µg/g | 87% (76–93) | 61% (45–74) |
| Ye 2017 [45] | China | 109 | SES-CD ≤ 2/SES-CD > 2 | 213 µg/g | 76% (65–84) | 66% (51–79) |
| Zollner 2021 [46] | Austria | 72 | SES-CD ≤ 2/SES-CD > 2 | 78 µg/g | 90% (75–97) | 77% (50–92) |
| Study (Name, Year) | Nation of Origin | Definition of Endoscopic Mucosal Healing | Optimal FC Cut-off | Sensitivity (95% CI) | Specificity (95% CI) |
|---|---|---|---|---|---|
| Cannatelli 2021 [53] | Italy | SES-CD ≤ 2 | 96 mcg/g | 75% (41–93%) | 85% (69–93) |
| Castiglione 2022 [54] | Italy | SES-CD ≤ 2 | 94 µg/g | 94% (84–98) | 85% (74–92) |
| Han 2022 [24] | China | pSES-CD = 0 | 117.48 µg/g | 89% (72–86) | 76% (70–81) |
| Inokuchi 2016 [48] | Japan | SES-CD = 0 | 180 µg/g | 87% (68–95) | 71% (57–82) |
| Kawashima 2017 [49] | Japan | SES-CD ≤ 2 | 162.2 µg/g | 81% (57–93) | 82% (71–90) |
| Lopes 2018 [50] | Spain | SES = CD = 0 | 100 µg/g | 89% (69–97) | 60% (31–83) |
| Noh 2018 [51] | Korea | No ulcers and/or inflammation | 234 µg/g | 84% (76–90) | 62% (54–69) |
| Reinisch 2020 [40] | Austria | CDEIS ≤ 3 | 250 µg/g | 90% (81–95) | 67% (56–77) |
| Vazquez-Moron 2017 [47] | Spain | SES-CD ≤ 2 | 71 µg/g | 95% (78–99) | 53% (39–66) |
| Study (Name, Year) | Nation of Origin | CD Patients (n=) | Definition of Endoscopic Activity | Optimal FL Cut-off | Sensitivity (95% CI) | Specificity (95% CI) |
|---|---|---|---|---|---|---|
| D’Inca 2006 [31] | Italy | 31 | SES-CD ≤ 3/SES-CD > 3 | 0.007 optical density | 77% (57–89) | 80% (38–96) |
| Karczewski 2015 [34] | Poland | 55 | CDEIS ≤ 2/CDEIS > 2 | 25 µg/g | 75% (62–85) | 80% (38–96) |
| Langhorst 2006 [35] | Germany | 43 | Authors score | 7.1 µg/mL | 81% (65–91) | 59% (32–82) |
| Sipponen 2008 [43] | Finland | 116 | CDEIS ≤ 3/CDEIS > 3 | 10 µg/g | 66% (54–76) | 91% (77–96) |
| Study (Name, Year) | Nation of Origin | Number of CD Patients | Definition of Endoscopic Activity | Faecal Biomarker | Optimal Faecal Biomarker Cut-off | Sensitivity (95% CI) | Specificity (95% CI) |
|---|---|---|---|---|---|---|---|
| Buisson 2016 [52] | France | 54 | Absence of ulcers/Presence of ulcers | Faecal chitinase 3-like 1 | 15 ng/g | 100% (84–100) | 64% (41–80) |
| Buisson 2018 [27] | France | 54 | Absence of ulcers/Presence of ulcers Absence of ulcers/Presence of ulcers | FCLN-2 Faecal metalloprotease 9 | 6700 ng/g 350 ng/g | 86% (64–97) 90% (64–97) | 45% (24–68) 64% (41–80) |
| Iwamoto 2018 [25] | Japan | 69 | eSES-CD = 0/eSES-CD ≥ 1 | FIT | 13 ng/mL | 73% (95% CI na) | 71% (95% CI na) |
| Langhorst 2006 [35] | Germany | 43 | Authors score | PMN-e | 0.062 µg/mL | 82% (65–93) | 70% (35–93) |
| Nancey 2013 [38] | France | 78 | SES-CD ≤ 2/SES-CD > 2 | Neopterin | 200 pmol/g | 74% (57–87) | 73% (56–85) |
| Swaminathan 2022 [44] | New Zealand | 100 | SES-CD ≤ 2/SES-CD > 2 | Faecal Myeloperoxidase | 10.25 µg/g | 63% (50–75) | 68% (51–83) |
| Zollner 2021 [46] | Austria | 72 | SES-CD ≤ 2/SES-CD > 2 | FLCN-2 | 0.56 µg/g | 91% (74–98) | 77% (46–95) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bohra, A.; Mohamed, G.; Vasudevan, A.; Lewis, D.; Van Langenberg, D.R.; Segal, J.P. The Utility of Faecal Calprotectin, Lactoferrin and Other Faecal Biomarkers in Discriminating Endoscopic Activity in Crohn’s Disease: A Systematic Review and Meta-Analysis. Biomedicines 2023, 11, 1408. https://doi.org/10.3390/biomedicines11051408
Bohra A, Mohamed G, Vasudevan A, Lewis D, Van Langenberg DR, Segal JP. The Utility of Faecal Calprotectin, Lactoferrin and Other Faecal Biomarkers in Discriminating Endoscopic Activity in Crohn’s Disease: A Systematic Review and Meta-Analysis. Biomedicines. 2023; 11(5):1408. https://doi.org/10.3390/biomedicines11051408
Chicago/Turabian StyleBohra, Anuj, Ghada Mohamed, Abhinav Vasudevan, Diana Lewis, Daniel R. Van Langenberg, and Jonathan P. Segal. 2023. "The Utility of Faecal Calprotectin, Lactoferrin and Other Faecal Biomarkers in Discriminating Endoscopic Activity in Crohn’s Disease: A Systematic Review and Meta-Analysis" Biomedicines 11, no. 5: 1408. https://doi.org/10.3390/biomedicines11051408
APA StyleBohra, A., Mohamed, G., Vasudevan, A., Lewis, D., Van Langenberg, D. R., & Segal, J. P. (2023). The Utility of Faecal Calprotectin, Lactoferrin and Other Faecal Biomarkers in Discriminating Endoscopic Activity in Crohn’s Disease: A Systematic Review and Meta-Analysis. Biomedicines, 11(5), 1408. https://doi.org/10.3390/biomedicines11051408