
The Utility of Urodynamic Studies in Neuro-Urological Patients

Abstract
1. Introduction
2. Methods
3. Analysis
3.1. UDS Diagnostic Performance
3.1.1. UDS and NDO
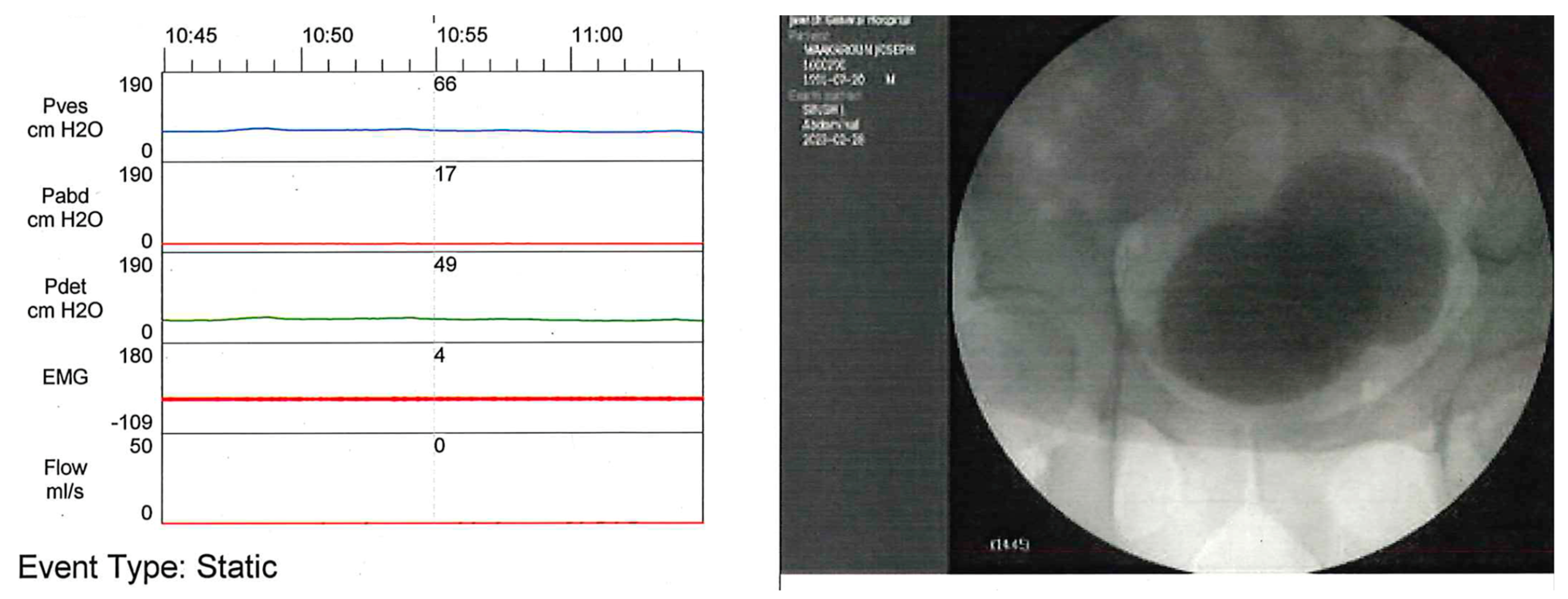
3.1.2. UDS and DSD
- Type 1 DSD presents a progressive increase in the external urinary sphincter (EUS) activity, with a peak at maximal detrusor contraction followed by a quick relaxation of the EUS as the detrusor pressure declines, allowing urination.
- Type 2 DSD shows clonic contractions of the EUS intermittently during the detrusor contraction, provoking intermittency of the urinary stream.
- Type 3 DSD is characterized by a continuous EUS contraction during the entire detrusor contraction, resulting in urinary obstruction or inability to urinate.
3.1.3. UDS and DLPP
3.1.4. VUDS Contribution
3.2. UDS Treatment Assessment Performance
3.2.1. UDS and NDO
3.2.2. UDS and DSD
3.2.3. UDS and DLPP
3.3. UDS Prognostic Evaluation Performance
3.3.1. UDS and NDO and DSD
3.3.2. UDS and DLPP
3.3.3. VUDS
4. Discussion
4.1. Paucity of Data
4.2. Medico-Economic Impact
4.3. Risk of UDS
4.4. Surrogate to UDS
4.5. Consistency with International Guidelines
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BTX | Botox® |
| CIC | clean intermittent catheterization |
| DLPP | detrusor leak point pressure |
| DSD | detrusor-sphincter dyssynergia |
| EUS | external urinary sphincter |
| LUT | lower urinary tract |
| LUTS | lower urinary tract symptoms |
| MS | multiple sclerosis |
| NDO | neurogenic detrusor overactivity |
| NLUTD | neurogenic lower urinary tract dysfunction |
| PVR | post-voiding residual urine volume |
| SCI | spinal cord injury |
| UDS | urodynamic study |
| UUT | upper urinary tract |
| VUDS | video-urodynamic study |
| VUR | vesico-ureteral reflux |
References
- Nosseir, M.; Hinkel, A.; Pannek, J. Clinical usefulness of urodynamic assessment for maintenance of bladder function in patients with spinal cord injury. Neurourol. Urodyn. 2007, 26, 228–233. [Google Scholar] [CrossRef]
- Ginsberg, D.A.; Boone, T.B.; Cameron, A.P.; Gousse, A.; Kaufman, M.R.; Keays, E.; Kennelly, M.J.; Lemack, G.E.; Rovner, E.S.; Souter, L.H.; et al. The AUA/SUFU Guideline on Adult Neurogenic Lower Urinary Tract Dysfunction: Diagnosis and Evaluation. J. Urol. 2021, 206, 1097–1105. [Google Scholar] [CrossRef]
- Groen, J. Summary of European Association of Urology (EAU) Guidelines on Neuro-Urology. Eur. Urol. 2016, 69, 324–333. [Google Scholar] [CrossRef]
- Mangera, A.; Apostolidis, A.; Andersson, K.E.; Dasgupta, P.; Giannantoni, A.; Roehrborn, C.; Novara, G.; Chapple, C. An updated systematic review and statistical comparison of standardised mean outcomes for the use of botulinum toxin in the management of lower urinary tract disorders. Eur. Urol. 2014, 65, 981–990. [Google Scholar] [CrossRef]
- Winters, J.C.; Dmochowski, R.R.; Goldman, H.B.; Herndon, C.D.A.; Kobashi, K.C.; Kraus, S.R.; Lemack, G.E.; Nitti, V.W.; Rovner, E.S.; Wein, A.J.; et al. Urodynamic studies in adults: AUA/SUFU guideline. J. Urol. 2012, 188, 2464–2472. [Google Scholar] [CrossRef]
- Panicker, J.N.; de Sèze, M.; Fowler, C.J. Rehabilitation in practice: Neurogenic lower urinary tract dysfunction and its management. Clin. Rehabil. 2010, 24, 579–589. [Google Scholar] [CrossRef]
- Radley-Gardner, O.; Beale, H.; Zimmermann, R. (Eds.) Fundamental Texts on European Private Law; Hart Publishing: Oxford, UK, 2016; ISBN 978-1-78225-864-3. [Google Scholar]
- Gammie, A.; Clarkson, B.; Constantinou, C.; Damaser, M.; Drinnan, M.; Geleijnse, G.; Griffiths, D.; Rosier, P.; Schäfer, W.; Van Mastrigt, R.; et al. International Continence Society guidelines on urodynamic equipment performance. Neurourol. Urodyn. 2014, 33, 370–379. [Google Scholar] [CrossRef]
- Drake, M.J.; Doumouchtsis, S.K.; Hashim, H.; Gammie, A. Fundamentals of urodynamic practice, based on International Continence Society good urodynamic practices recommendations. Neurourol. Urodyn. 2018, 37, S50–S60. [Google Scholar] [CrossRef]
- Bodmer, N.S.; Wirth, C.; Birkhäuser, V.; Sartori, A.M.; Leitner, L.; Averbeck, M.A.; de Wachter, S.; Finazzi Agro, E.; Gammie, A.; Goldman, H.B.; et al. Randomised Controlled Trials Assessing the Clinical Value of Urodynamic Studies: A Systematic Review and Meta-analysis. Eur. Urol. Open Sci. 2022, 44, 131–141. [Google Scholar] [CrossRef]
- Welk, B.; Schneider, M.P.; Thavaseelan, J.; Traini, L.R.; Curt, A.; Kessler, T.M. Early urological care of patients with spinal cord injury. World J. Urol. 2018, 36, 1537–1544. [Google Scholar] [CrossRef]
- Musco, S.; Padilla-Fernández, B.; Del Popolo, G.; Bonifazi, M.; Blok, B.F.M.; Groen, J.; ’t Hoen, L.; Pannek, J.; Bonzon, J.; Kessler, T.M.; et al. Value of urodynamic findings in predicting upper urinary tract damage in neuro-urological patients: A systematic review. Neurourol. Urodyn. 2018, 37, 1522–1540. [Google Scholar] [CrossRef]
- Veenboer, P.W.; Bosch, J.L.H.R.; Rosier, P.F.W.M.; Dik, P.; van Asbeck, F.W.A.; de Jong, T.P.V.M.; de Kort, L.M.O. Cross-sectional study of determinants of upper and lower urinary tract outcomes in adults with spinal dysraphism--new recommendations for urodynamic followup guidelines? J. Urol. 2014, 192, 477–482. [Google Scholar] [CrossRef]
- Shin, J.C.; Lee, Y.; Yang, H.; Kim, D.H. Clinical significance of urodynamic study parameters in maintenance of renal function in spinal cord injury patients. Ann. Rehabil. Med. 2014, 38, 353–359. [Google Scholar] [CrossRef]
- Ku, J.H.; Choi, W.J.; Lee, K.Y.; Jung, T.Y.; Lee, J.K.; Park, W.H.; Shim, H.B. Complications of the upper urinary tract in patients with spinal cord injury: A long-term follow-up study. Urol. Res. 2005, 33, 435–439. [Google Scholar] [CrossRef]
- Colli, E.; Artibani, W.; Goka, J.; Parazzini, F.; Wein, A.J. Are urodynamic tests useful tools for the initial conservative management of non-neurogenic urinary incontinence? A review of the literature. Eur. Urol. 2003, 43, 63–69. [Google Scholar] [CrossRef]
- De Muylder, X.; Claes, H.; Neven, P.; De Jaegher, K. Usefulness of urodynamic investigations in female incontinence. Eur. J. Obstet. Gynecol. Reprod. Biol. 1992, 44, 205–208. [Google Scholar] [CrossRef]
- Elmelund, M.; Klarskov, N.; Bagi, P.; Oturai, P.S.; Biering-Sørensen, F. Renal deterioration after spinal cord injury is associated with length of detrusor contractions during cystometry-A study with a median of 41 years follow-up. Neurourol. Urodyn. 2017, 36, 1607–1615. [Google Scholar] [CrossRef]
- Bywater, M.; Tornic, J.; Mehnert, U.; Kessler, T.M. Detrusor Acontractility after Acute Spinal Cord Injury-Myth or Reality? J. Urol. 2018, 199, 1565–1570. [Google Scholar] [CrossRef]
- Birkhäuser, V.; Liechti, M.D.; Anderson, C.E.; Bachmann, L.M.; Baumann, S.; Baumberger, M.; Birder, L.A.; Botter, S.M.; Büeler, S.; Cruz, C.D.; et al. TASCI-transcutaneous tibial nerve stimulation in patients with acute spinal cord injury to prevent neurogenic detrusor overactivity: Protocol for a nationwide, randomised, sham-controlled, double-blind clinical trial. BMJ Open 2020, 10, e039164. [Google Scholar] [CrossRef]
- Al-Ali, M.; Haddad, L. A 10 year review of the endoscopic treatment of 125 spinal cord injured patients with vesical outlet obstruction: Does bladder neck dyssynergia exist? Int. Med. Soc. Paraplegia 1996, 34, 34–38. [Google Scholar] [CrossRef]
- Rossier, A.B.; Fam, B.A. 5-microtransducer catheter in evaluation of neurogenic bladder function. Urology 1986, 27, 371–378. [Google Scholar] [CrossRef]
- Bacsu, C.-D.; Chan, L.; Tse, V. Diagnosing detrusor sphincter dyssynergia in the neurological patient. BJU Int. 2012, 109 (Suppl. S3), 31–34. [Google Scholar] [CrossRef]
- Blaivas, J.G.; Sinha, H.P.; Zayed, A.A.; Labib, K.B. Detrusor-external sphincter dyssynergia: A detailed electromyographic study. J. Urol. 1981, 125, 545–548. [Google Scholar] [CrossRef]
- Weld, K.J.; Graney, M.J.; Dmochowski, R.R. Clinical significance of detrusor sphincter dyssynergia type in patients with post-traumatic spinal cord injury. Urology 2000, 56, 565–568. [Google Scholar] [CrossRef]
- D’Ancona, C.; Haylen, B.; Oelke, M.; Abranches-Monteiro, L.; Arnold, E.; Goldman, H.; Hamid, R.; Homma, Y.; Marcelissen, T.; Rademakers, K.; et al. The International Continence Society (ICS) report on the terminology for adult male lower urinary tract and pelvic floor symptoms and dysfunction. Neurourol. Urodyn. 2019, 38, 433–477. [Google Scholar] [CrossRef]
- Lose, G.; Griffiths, D.; Hosker, G.; Kulseng-Hanssen, S.; Perucchini, D.; Schäfer, W.; Thind, P.; Versi, E. Standardisation of urethral pressure measurement: Report from the Standardisation Sub-Committee of the International Continence Society. Neurourol. Urodyn. 2002, 21, 258–260. [Google Scholar] [CrossRef]
- Kurzrock, E.A.; Polse, S. Renal deterioration in myelodysplastic children: Urodynamic evaluation and clinical correlates. J. Urol. 1998, 159, 1657–1661. [Google Scholar] [CrossRef]
- Gerridzen, R.G.; Thijssen, A.M.; Dehoux, E. Risk factors for upper tract deterioration in chronic spinal cord injury patients. J. Urol. 1992, 147, 416–418. [Google Scholar] [CrossRef]
- Ozkan, B.; Demirkesen, O.; Durak, H.; Uygun, N.; Ismailoglu, V.; Cetinel, B. Which factors predict upper urinary tract deterioration in overactive neurogenic bladder dysfunction? Urology 2005, 66, 99–104. [Google Scholar] [CrossRef]
- Linsenmeyer, T.A.; Bagaria, S.P.; Gendron, B. The impact of urodynamic parameters on the upper tracts of spinal cord injured men who void reflexly. J. Spinal Cord Med. 1998, 21, 15–20. [Google Scholar] [CrossRef]
- Wyndaele, M.; Rosier, P.F.W.M. Basics of videourodynamics for adult patients with lower urinary tract dysfunction. Neurourol. Urodyn. 2018, 37, S61–S66. [Google Scholar] [CrossRef]
- Ginsberg, D. The epidemiology and pathophysiology of neurogenic bladder. Am. J. Manag. Care 2013, 19, s191–s196. [Google Scholar]
- Majumdar, A.; Latthe, P.; Toozs-Hobson, P. Urodynamics prior to treatment as an intervention: A pilot study. Neurourol. Urodyn. 2010, 29, 522–526. [Google Scholar] [CrossRef]
- Kopp Kallner, H.; Elmér, C.; Altman, D. Urodynamics as a Prognosticator of Mirabegron Treatment Outcomes. Gynecol. Obstet. Investig. 2019, 84, 472–476. [Google Scholar] [CrossRef]
- Abrams, P.; Kelleher, C.; Staskin, D.; Rechberger, T.; Kay, R.; Martina, R.; Newgreen, D.; Paireddy, A.; van Maanen, R.; Ridder, A. Combination treatment with mirabegron and solifenacin in patients with overactive bladder: Efficacy and safety results from a randomised, double-blind, dose-ranging, phase 2 study (Symphony). Eur. Urol. 2015, 67, 577–588. [Google Scholar] [CrossRef]
- Amarenco, G.; Sutory, M.; Zachoval, R.; Agarwal, M.; Del Popolo, G.; Tretter, R.; Compion, G.; De Ridder, D. Solifenacin is effective and well tolerated in patients with neurogenic detrusor overactivity: Results from the double-blind, randomized, active- and placebo-controlled SONIC urodynamic study. Neurourol. Urodyn. 2017, 36, 414–421. [Google Scholar] [CrossRef]
- Hadiji, N.; Previnaire, J.G.; Benbouzid, R.; Robain, G.; Leblond, C.; Mieusset, R.; Enjalbert, M.; Soler, J.M. Are oxybutynin and trospium efficacious in the treatment of detrusor overactivity in spinal cord injury patients? Spinal Cord 2014, 52, 701–705. [Google Scholar] [CrossRef]
- Kasabian, N.G.; Bauer, S.B.; Dyro, F.M.; Colodny, A.H.; Mandell, J.; Retik, A.B. The prophylactic value of clean intermittent catheterization and anticholinergic medication in newborns and infants with myelodysplasia at risk of developing urinary tract deterioration. Am. J. Dis. Child. 1992, 146, 840–843. [Google Scholar] [CrossRef]
- Vainrib, M.; Reyblat, P.; Ginsberg, D.A. Differences in urodynamic study variables in adult patients with neurogenic bladder and myelomeningocele before and after augmentation enterocystoplasty. Neurourol. Urodyn. 2013, 32, 250–253. [Google Scholar] [CrossRef]
- Chen, H.; Xie, K.; Jiang, C. A single-blind randomized control trial of trigonal versus nontrigonal Botulinum toxin-A injections for patients with urinary incontinence and poor bladder compliance secondary to spinal cord injury. J. Spinal Cord Med. 2021, 44, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Aharony, S.; Przydacz, M.; Van Ba, O.L.; Corcos, J. Does asymptomatic bacteriuria increase the risk of adverse events or modify the efficacy of intradetrusor onabotulinumtoxinA injections? Neurourol. Urodyn. 2020, 39, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Kattan, M.W.; Boone, T.B. Bladder leak point pressure: The measure for sphincterotomy success in spinal cord injured patients with external detrusor-sphincter dyssynergia. J. Urol. 1998, 159, 493–496; discussion 496–497. [Google Scholar] [CrossRef] [PubMed]
- Schöps, T.-F.; Schneider, M.P.; Steffen, F.; Ineichen, B.V.; Mehnert, U.; Kessler, T.M. Neurogenic lower urinary tract dysfunction (NLUTD) in patients with spinal cord injury: Long-term urodynamic findings. BJU Int. 2015, 115 (Suppl. S6), 33–38. [Google Scholar] [CrossRef] [PubMed]
- Kozomara, M.; Birkhäuser, V.; Anderson, C.E.; Bywater, M.; Gross, O.; Kiss, S.; Knüpfer, S.C.; Koschorke, M.; Leitner, L.; Mehnert, U.; et al. Neurogenic Lower Urinary Tract Dysfunction in the First Year After Spinal Cord Injury: A Descriptive Study of Urodynamic Findings. J. Urol. 2023, 209, 225–232. [Google Scholar] [CrossRef]
- Tarcan, T.; Demirkesen, O.; Plata, M.; Castro-Diaz, D. ICS teaching module: Detrusor leak point pressures in patients with relevant neurological abnormalities. Neurourol. Urodyn. 2017, 36, 259–262. [Google Scholar] [CrossRef]
- Guerra, L.; Leonard, M.; Castagnetti, M. Best practice in the assessment of bladder function in infants. Ther. Adv. Urol. 2014, 6, 148–164. [Google Scholar] [CrossRef]
- Anding, R.; Rosier, P.; Smith, P.; Gammie, A.; Giarenis, I.; Rantell, A.; Thiruchelvam, N.; Arlandis, S.; Cardozo, L. When should video be added to conventional urodynamics in adults and is it justified by the evidence? ICI-RS 2014. Neurourol. Urodyn. 2016, 35, 324–329. [Google Scholar] [CrossRef]
- Linsenmeyer, T.A.; Linsenmeyer, M.A. Impact of annual urodynamic evaluations on guiding bladder management in individuals with spinal cord injuries. J. Spinal Cord Med. 2013, 36, 420–426. [Google Scholar] [CrossRef]
- Chao, R.; Mayo, M.E. Long-term urodynamic follow up in pediatric spinal cord injury. Paraplegia 1994, 32, 806–809. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Fattah, M.; Chapple, C.; Guerrero, K.; Dixon, S.; Cotterill, N.; Ward, K.; Hashim, H.; Monga, A.; Brown, K.; Drake, M.J.; et al. Female Urgency, Trial of Urodynamics as Routine Evaluation (FUTURE study): A superiority randomised clinical trial to evaluate the effectiveness and cost-effectiveness of invasive urodynamic investigations in management of women with refractory overactive bladder symptoms. Trials 2021, 22, 745. [Google Scholar] [CrossRef] [PubMed]
- Sinha, S. Follow-up urodynamics in patients with neurogenic bladder. Indian J. Urol. 2017, 33, 267. [Google Scholar] [CrossRef] [PubMed]
- Pannek, J.; Bartel, P.; Göcking, K.; Frotzler, A. Clinical usefulness of ultrasound assessment of detrusor wall thickness in patients with neurogenic lower urinary tract dysfunction due to spinal cord injury: Urodynamics made easy? World J. Urol. 2013, 31, 659–664. [Google Scholar] [CrossRef]
- Urinary Incontinence in Neurological Disease: Assessment and Management. Available online: https://www.nice.org.uk/guidance/cg148/resources/urinary-incontinence-in-neurological-disease-assessment-and-management-pdf-35109577553605 (accessed on 16 January 2023).
- Drake, M.J.; Apostolidis, A.; Cocci, A.; Emmanuel, A.; Gajewski, J.B.; Harrison, S.C.W.; Heesakkers, J.P.F.A.; Lemack, G.E.; Madersbacher, H.; Panicker, J.N.; et al. Neurogenic lower urinary tract dysfunction: Clinical management recommendations of the Neurologic Incontinence committee of the fifth International Consultation on Incontinence 2013. Neurourol. Urodyn. 2016, 35, 657–665. [Google Scholar] [CrossRef]
- Welk, B.; Liu, K.; Shariff, S.Z. The use of urologic investigations among patients with traumatic spinal cord injuries. Res. Rep. Urol. 2016, 8, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.S.; Greiman, A.; Casey, J.T.; Mukherjee, S.; Kielb, S.J. A snapshot of the adult spina bifida patient—High incidence of urologic procedures. Cent. Eur. J. Urol. 2016, 69, 72–77. [Google Scholar] [CrossRef]
- Veenboer, P.W.; Ruud Bosch, J.L.H.; de Kort, L.M.O. Assessment of bladder and kidney functioning in adult spina bifida patients by Dutch urologists: A survey. Neurourol. Urodyn. 2014, 33, 289–295. [Google Scholar] [CrossRef]
- Blok, B.F.M.; Karsenty, G.; Corcos, J. Urological surveillance and management of patients with neurogenic bladder: Results of a survey among practicing urologists in Canada. Can. J. Urol. 2006, 13, 3239–3243. [Google Scholar] [PubMed]
- Bycroft, J.; Hamid, R.; Bywater, H.; Patki, P.; Craggs, M.; Shah, J. Variation in urological practice amongst spinal injuries units in the UK and Eire. Neurourol. Urodyn. 2004, 23, 252–256; discussion 257. [Google Scholar] [CrossRef]
- Burki, J.R.; Omar, I.; Shah, P.J.R.; Hamid, R. Long-term urological management in spinal injury units in the U.K. and Eire: A follow-up study. Spinal Cord 2014, 52, 640–645. [Google Scholar] [CrossRef]
- Denys, P.; Soler, J.-M.; Fatton, B.; Rischmann, P.; Yelnik, A.; Aegerter, P.; Saidji-Domingo, N.-Y.; Chartier-Kastler, E. Highlighting differences in the management of neurogenic bladder existing between urologists and physiatrists: A survey conducted among 383 specialists. La Presse Médicale 2012, 41, e599–e608. [Google Scholar] [CrossRef]


{kind=link}
| Documents or Guidelines | Organization, Version | Recommendations | Level of Evidence/Grade of Recommendations | References |
|---|---|---|---|---|
| The AUA/SUFU Guideline on Adult Neurogenic Lower Urinary Tract Dysfunction: Diagnosis and Evaluation | American Urological Association, 2021 | UDS, with or without fluoroscopy (VUDS), is recommended at initial evaluation of patients with unknown risk NLUTD and in the follow-up of those thought to be at moderate and high risk if change in signs and symptoms, new complications (autonomic dysreflexia, UTI, stones), UUT or renal function deterioration. | Moderate Recommendation; Evidence Level: Grade C | [2] |
| EAU Guidelines on Neuro-Urology | European Association of Urology, 2022 | UDS investigation is the only method that can objectively assess the (dys-) function of the LUT. | 2a | EAU Guidelines, 2022. |
| VUDS is the optimum procedure for urodynamic investigation in neuro-urological disorders. | 4 | |||
| Perform urodynamic investigation as a mandatory baseline diagnostic intervention in high-risk patients at regular intervals. | Strong recommendation | |||
| Urinary incontinence in neurological disease: assessment and management | National Institute for Health and Care Excellence, 2012 | Do not offer UDS routinely to people at low risk of renal complications (most MS patients). | [54] | |
| Offer VUDS to people at high risk of renal complications (spina bifida, SCI or anorectal abnormalities). | ||||
| Offer UDS before performing surgical treatments for NLUTD. | ||||
| Neurogenic Lower Urinary Tract Dysfunction: Clinical Management Recommendations | Fifth International Consultation on Incontinence 2013 (Published 2016) | UDS should selectively be employed to supplement clinical assessment in determining management in NLUTD | [55] | |
| UDS should be used to gauge potential impact on a renal function as a consequence of NLUTD. | ||||
| Patients on CIC and bladder storage treatment often require long-term UDS and upper tract monitoring | A | |||
| Patients with stress incontinence in association with NLUTD require VUDS to evaluate both bladder and sphincter function | C |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perrin, A.; Corcos, J. The Utility of Urodynamic Studies in Neuro-Urological Patients. Biomedicines 2023, 11, 1134. https://doi.org/10.3390/biomedicines11041134
Perrin A, Corcos J. The Utility of Urodynamic Studies in Neuro-Urological Patients. Biomedicines. 2023; 11(4):1134. https://doi.org/10.3390/biomedicines11041134
Chicago/Turabian StylePerrin, Andry, and Jacques Corcos. 2023. "The Utility of Urodynamic Studies in Neuro-Urological Patients" Biomedicines 11, no. 4: 1134. https://doi.org/10.3390/biomedicines11041134
APA StylePerrin, A., & Corcos, J. (2023). The Utility of Urodynamic Studies in Neuro-Urological Patients. Biomedicines, 11(4), 1134. https://doi.org/10.3390/biomedicines11041134