
DDX3X Syndrome Behavioral Manifestations with Particular Emphasis on Psycho-Pathological Symptoms—A Review



Abstract
:
1. Introduction
2. Materials and Methods
2.1. Declaration and Protocol
2.2. Search Strategy
2.3. Research Protocols and Inclusion and Exclusion Criteria
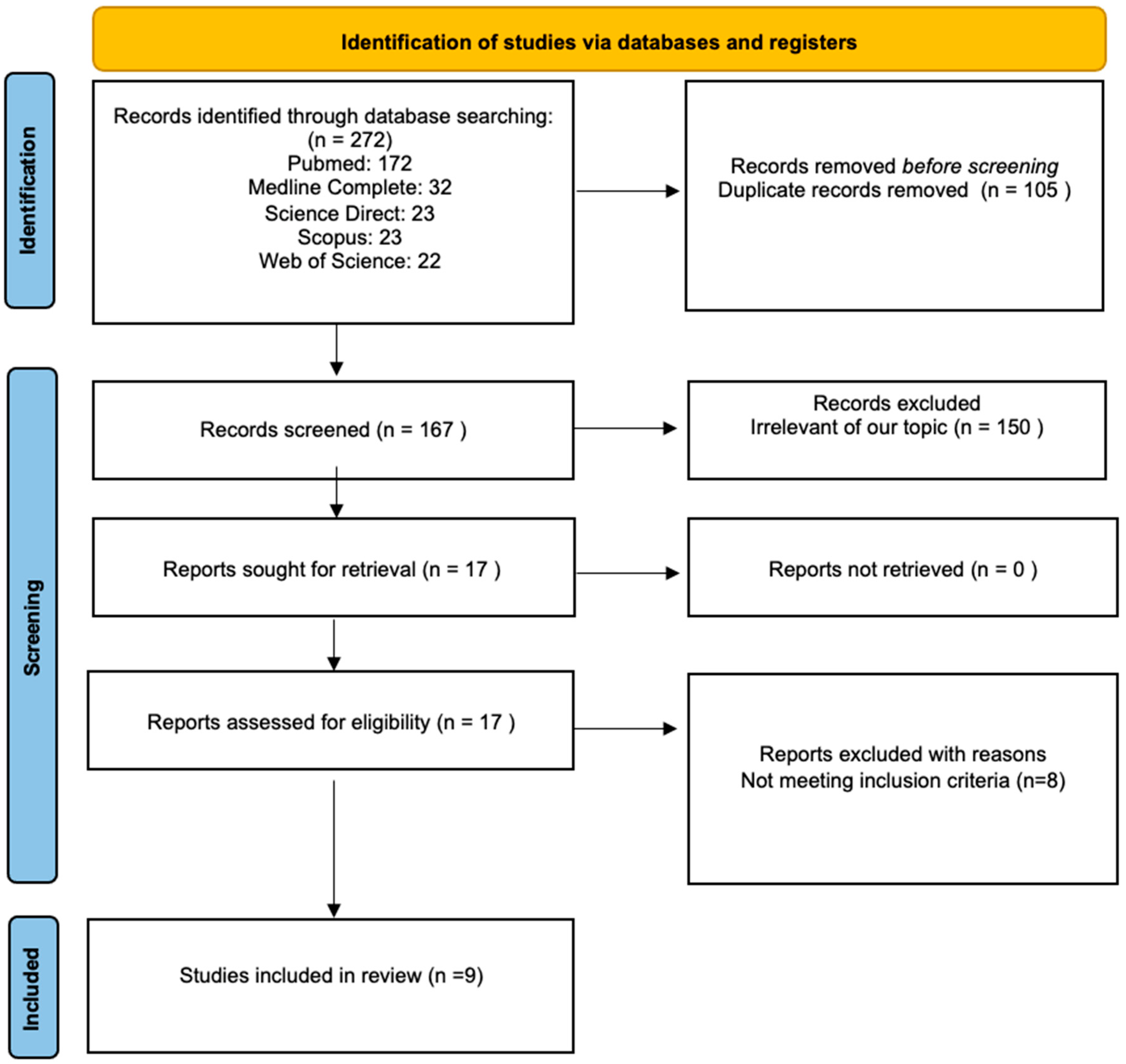
2.4. Study Selection
2.5. Data Extraction and Analysis
2.6. Data Synthesis
3. Results
3.1. Included Papers
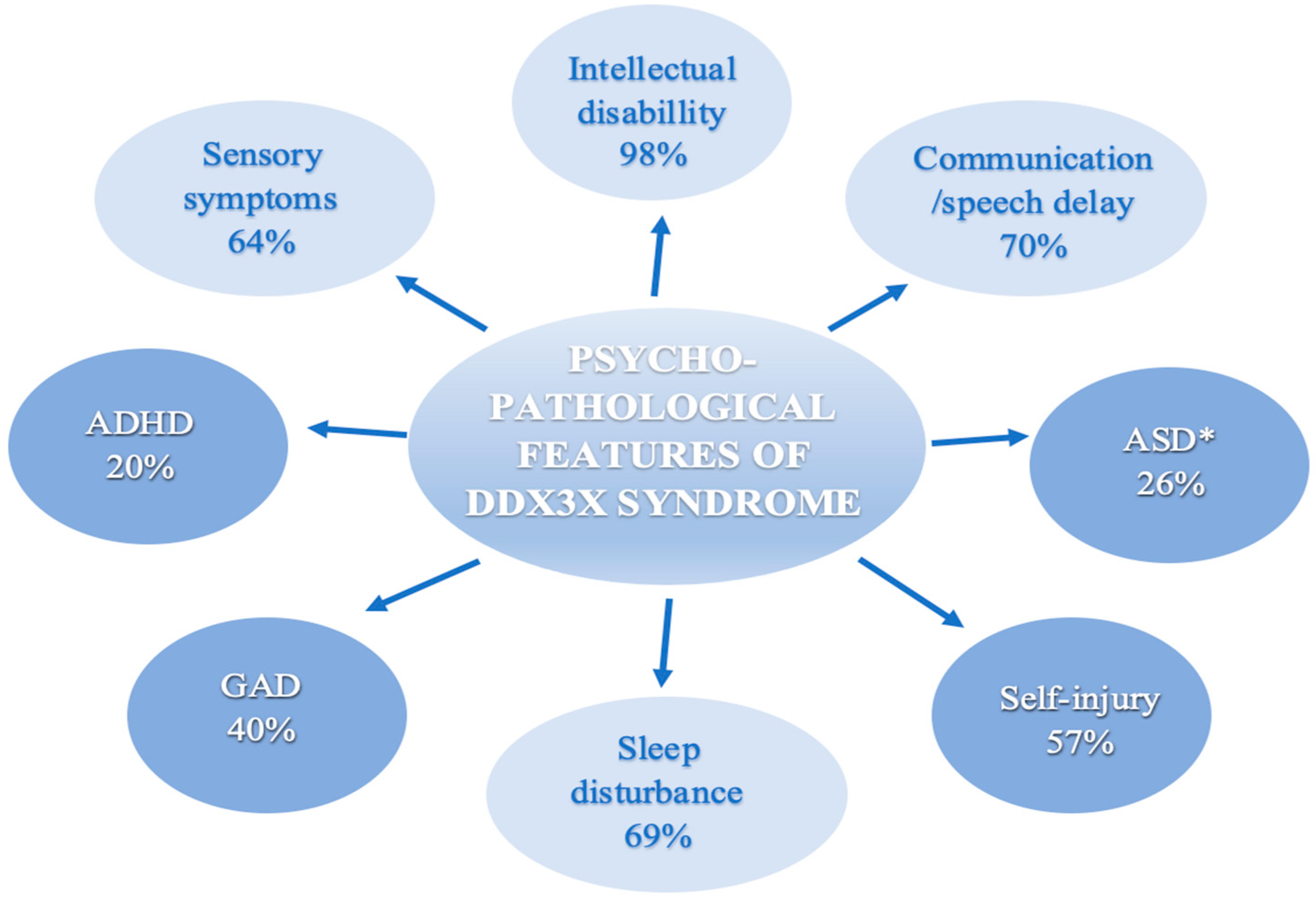
3.2. Results of Data Extraction

{kind=link}
{kind=link}
{kind=link}
| Number of Patients Tested in Different Research Groups/Centers | ||||||||
|---|---|---|---|---|---|---|---|---|
| Patients with Identified Behavior | Lennox [9] n= 107 | Snijders Blok [7] n= 38 | Wang [12] n= 28 | Mount Sinai * [15,24] n= 24 | Ng-Cordell [23] n= 23 | Dai [26] n= 23 | Beal [8] n= 6 | Stefaniak [19] n= 1 |
| 1.ID/DD | n = 106 | n = 38 (ID/DD) | n = 28 (ID/D) | n = 22 | n = 23 | n = 23 | n = 3 | X |
| 2. Communication / speech delay | n = 38 2a | n/a | n/a | n = 13 | n = 21 | n = 23 2b | n = 4 2c | 1 |
| 3. Autism spectrum disorder | n = 22 3a | n = 20 3b | n = 6 3c | n = 14 | n = 15 3d | n = 3 | n = 2 3e | 1 |
| 4. Attention deficit hyperactivity disorder | n = 16 3a | n/a | n/a | n = 9 | n/a | n/a | n/a | x |
| 5. Generalized anxiety disorder | n/a | n/a | n/a | n = 1 | n = 16 | n/a | n/a | x |
| 6. Self-injury | n/a | n/a | n/a | n/a | n = 13 | n/a | n/a | x |
| 7. Sensory symptoms | n/a | n/a | n/a | n = 14 | n = 10 | n/a | n/a | n = 1 |
| 8. Sleep disturbance | n/a | n/a | n/a | n = 15 | n = 13 | n/a | n = 2 | n = 1 |
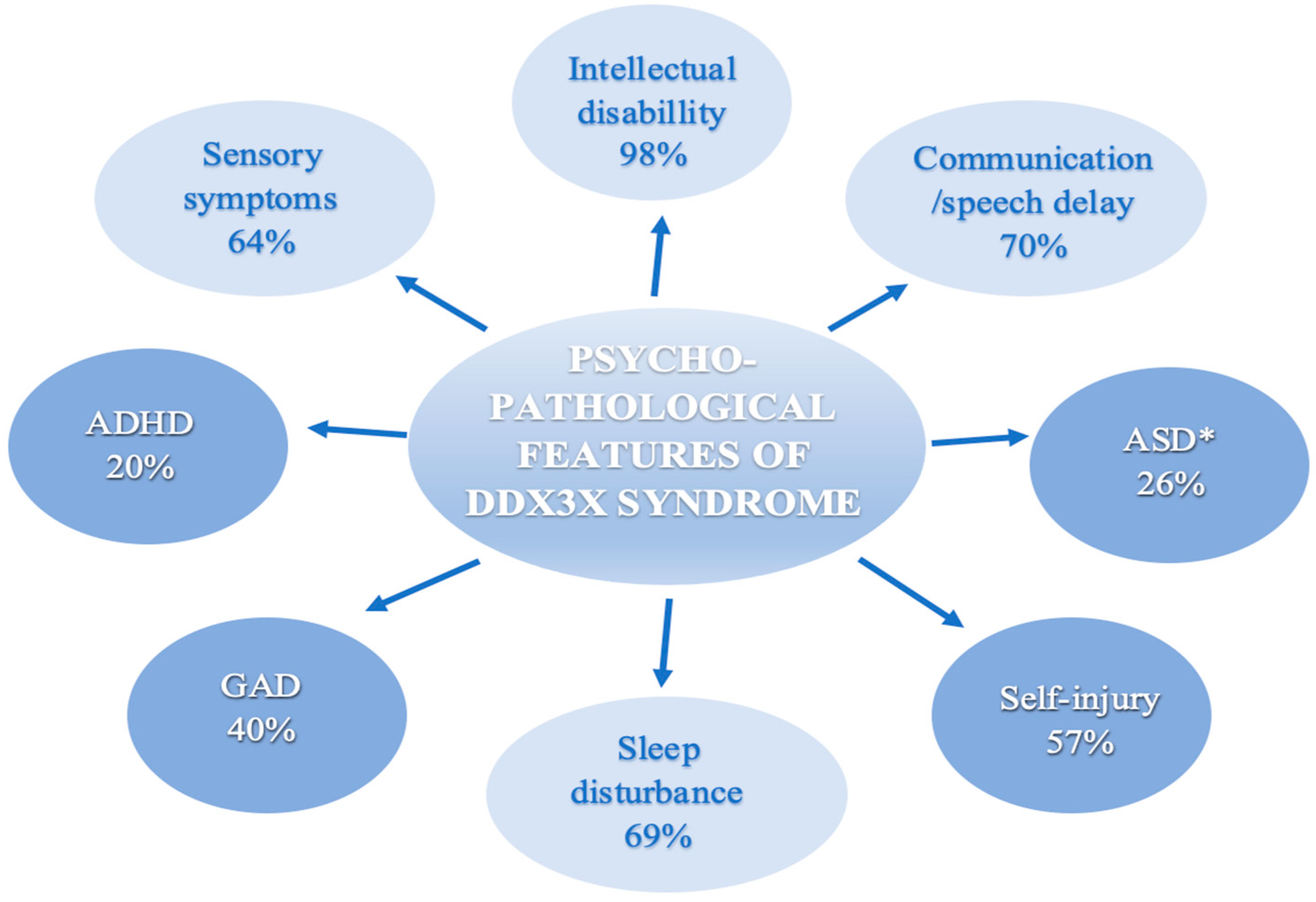
3.3. Intellectual Disability
3.4. Communication Delay
3.5. Autism Spectrum Disorder
3.6. Attention Deficit Hyperactivity Disorder
3.7. Abnormal Behavior
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AAC | Augmentative and Alternative Communication |
| ABA | Applied Behavioral Analysis |
| ADGRL1 | C-terminal phosphorylation of latrophilin-1 |
| ADHD | Attention Deficit and Hyperactivity Disorder |
| ADI-R | Autism Diagnostic Interview-Revised |
| ADOS-2 | Autism Diagnostic Observation Schedule-Second Edition |
| ASD | Autism Spectrum Disorder |
| CAS | Childhood Apraxia of Speech |
| CLN2 | Late-infantile neuronal ceroid lipofuscinosis type 2 |
| DBC | Developmental Behavior Checklist |
| DD | Developmental Delays |
| DDX3X | DEAD-Box Helicase 3 X-Linked |
| DDX3X | DDX3X Syndrome |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders |
| GAD | Generalized Anxiety Disorder |
| ID | Intellectual Disability |
| IDD | Intellectual and Developmental Disabilities |
| MHI | Medical History Interviews |
| NGS | Next Generation Sequencing |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RD | Rare Disease |
| RAC3 | Ras-related C3 botulinum toxin substrate 3 |
| RNNDs | Rare Neurodevelopmental Disorders |
| RSRC1 | Arginine/serine-rich coiled-coil 1 |
| SAND | Sensory Assessment for Neurodevelopmental Disorders |
| SI | Sensory Integration |
| SIBs | Self-injurious Behaviors |
| SSP | Short Sensory Profile |
| WES | Whole Exome Sequencing |
References
- Haendel, M.; Vasilevsky, N.; Unni, D. How many rare diseases are there? Nat. Rev. Drug Discov. 2020, 19, 77–78. [Google Scholar] [CrossRef] [PubMed]
- Nguengang Wakap, S.; Lambert, D.M.; Olry, A. Estimating cumulative point prevalence of rare diseases: Analysis of the Orphanet database. Eur. J. Hum. Genet. 2020, 28, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Mo, J.; Liang, H.; Su, C. DDX3X: Structure, physiologic functions and cancer. Mol. Cancer 2021, 20, 38. [Google Scholar] [CrossRef]
- Kellaris, G.; Khan, K.; Baig, S.M. A hypomorphic inherited pathogenic variant in DDX3X causes male intellectual disability with additional neurodevelopmental and neurodegenerative features. Hum. Genomics 2018, 12, 11. [Google Scholar] [CrossRef]
- Bol, G.M.; Xie, M.; Raman, V. DDX3, a potential target for cancer treatment. Mol. Cancer 2015, 14, 188. [Google Scholar] [CrossRef] [PubMed]
- Schröder, M. Viruses and the human DEAD-box helicase DDX3: Inhibition or exploitation? Biochem. Soc. Trans. 2011, 39, 679–683. [Google Scholar] [CrossRef]
- Snijders Blok, L.; Madsen, E.; Juusola, J. Mutations in DDX3X Are a Common Cause of Unexplained Intellectual Disability with Gender-Specific Effects on Wnt Signaling. Am. J. Hum. Genet. 2015, 97, 343–352. [Google Scholar] [CrossRef]
- Beal, B.; Hayes, I.; McGaughran, J. Expansion of phenotype of DDX3X syndrome: Six new cases. Clin. Dysmorphol. 2019, 28, 169–174. [Google Scholar] [CrossRef]
- Lennox, A.L.; Hoye, M.L.; Jiang, R. Pathogenic DDX3X Mutations Impair RNA Metabolism and Neurogenesis during Fetal Cortical Development. Neuron 2020, 106, 404–420.e8. [Google Scholar] [CrossRef]
- Nicola, P.; Blackburn, P.R.; Rasmussen, K.J. De novo DDX3X missense variants in males appear viable and contribute to syndromic intellectual disability. Am. J. Med. Genet. Part A 2019, 179, 570–578. [Google Scholar] [CrossRef]
- Gillentine, M.A.; Wang, T.; Eichler, E.E. Estimating the Prevalence of De Novo Monogenic Neurodevelopmental Disorders from Large Cohort Studies. Biomedicines 2022, 10, 2865. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Posey, J.E.; Rosenfeld, J.A. Phenotypic expansion in DDX3X -a common cause of intellectual disability in females. Ann. Clin. Transl. Neurol. 2018, 5, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Deciphering Developmental Disorders Study. Large-scale discovery of novel genetic causes of developmental disorders. Nature 2015, 519, 223–228. [Google Scholar] [CrossRef]
- Deciphering Developmental Disorders Study. Prevalence and architecture of de novo mutations in developmental disorders. Nature 2017, 542, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Levy, T.; Siper, P.M.; Lerman, B. DDX3X Syndrome: Summary of Findings and Recommendations for Evaluation and Care. Pediatr. Neurol. 2022, 138, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Scala, M.; Torella, A.; Severino, M. Three de novo DDX3X variants associated with distinctive brain developmental abnormalities and brain tumor in intellectually disabled females. Eur. J. Hum. Genet. 2019, 27, 1254–1259. [Google Scholar] [CrossRef] [PubMed]
- DDX3X Foundation. Available online: http://ddx3x.org/ (accessed on 25 February 2023).
- Hu, L.; Xin, X.; Lin, S. A child with a novel DDX3X variant mimicking cerebral palsy: A case report. Ital. J. Pediatr. 2020, 46, 88. [Google Scholar] [CrossRef]
- Stefaniak, U.; Malak, R.; Mojs, E. Autistic-like Behaviors Associated with a Novel Non-Canonical Splice-Site DDX3X Variant: A Case Report of a Rare Clinical Syndrome. Brain Sci. 2022, 12, 390. [Google Scholar] [CrossRef]
- Schultze-Lutter, F.; Schmidt, S.J.; Theodoridou, A. Psychopathology-a Precision Tool in Need of Re-sharpening. Front. Psychiatry 2018, 9, 446. [Google Scholar] [CrossRef]
- Ormel, J.; Laceulle, O.M.; Jeronimus, B.F. Why personality and psychopathology are correlated: A developmental perspective is a first step but more is needed. Eur. J. Pers. 2014, 28, 396–398. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, TX, USA, 2013. [Google Scholar]
- Ng-Cordell, E.; Kolesnik-Taylor, A.; O’Brien, S. Social and emotional characteristics of girls and young women with DDX3X-associated intellectual disability: A descriptive and comparative study. J. Autism Dev. Disord. 2023, 53, 3208–3219. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Levy, T.; Guillory, S. Prospective and detailed behavioral phenotyping in DDX3X syndrome. Mol. Autism. 2021, 12, 36. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.; Yang, Z.; Guo, J. Expansion of Clinical and Genetic Spectrum of DDX3X Neurodevelopmental Disorder in 23 Chinese Patients. Front. Mol. Neurosci. 2022, 15, 793001. [Google Scholar] [CrossRef]
- Johnson-Kerner, B.; Snijders Blok, L.; Suit, L. DDX3X-Related Neurodevelopmental Disorder. In GeneReviews®; Adam, M.P., Fieldman, J., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Gripp, K.W., Amemiya, A., Eds.; University of Washington, Seattle: Seattle, WA, USA, 2020. [Google Scholar]
- Alharthi, A.; Alhazmi, S.; Alburae, N. The Human Gut Microbiome as a Potential Factor in Autism Spectrum Disorder. Int. J. Mol. Sci. 2022, 23, 1363. [Google Scholar] [CrossRef]
- Latrèche, K.; Kojovic, N.; Franchini, M. Attention to Face as a Predictor of Developmental Change and Treatment Outcome in Young Children with Autism Spectrum Disorder. Biomedicines 2021, 9, 942. [Google Scholar] [CrossRef]
- Hyman, S.L.; Levy, S.E.; Myers, S.M. Identification, Evaluation, and Management of Children with Autism Spectrum Disorder. Pediatrics 2020, 145, e20193447. [Google Scholar] [CrossRef]
- Singh, R.; Kisku, A.; Kungumaraj, H. Autism Spectrum Disorders: A Recent Update on Targeting Inflammatory Pathways with Natural Anti-Inflammatory Agents. Biomedicines 2023, 11, 115. [Google Scholar] [CrossRef]
- Ausderau, K.K.; Furlong, M.; Sideris, J. Sensory subtypes in children with autism spectrum disorder: Latent profile transition analysis using a national survey of sensory features. J. Child Psychol. Psychiatry 2014, 55, 935–944. [Google Scholar] [CrossRef]
- Gunderson, J.; Worthley, E.; Byiers, B. Self and caregiver report measurement of sensory features in autism spectrum disorder: A systematic review of psychometric properties. J. Neurodev. Disord. 2023, 15, 5. [Google Scholar] [CrossRef]
- Kirby, A.V.; Bilder, D.A.; Wiggins, L.D. Sensory features in autism: Findings from a large population-based surveillance system. Autism Res. 2022, 15, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Levit-Binnun, N.; Davidovitch, M.; Golland, Y. Sensory and motor secondary symptoms as indicators of brain vulnerability. J. Neurodev. Disord. 2013, 5, 26. [Google Scholar] [CrossRef] [PubMed]
- Hildebrand, M.S.; Jackson, V.E.; Scerri, T.S. Severe childhood speech disorder: Gene discovery highlights transcriptional dysregulation. Neurology 2020, 94, e2148–e2167. [Google Scholar] [CrossRef] [PubMed]
- Dikow, N.; Granzow, M.; Graul-Neumann, L.M.; Karch, S.; Hinderhofer, K.; Paramasivam, N.; Behl, L.-J.; Kaufmann, L.; Fischer, C.; Evers, C.; et al. DDX3X mutations in two girls with a phenotype overlapping Toriello-Carey syndrome. Am. J. Med. Genet. Prat A 2017, 173, 1369–1373. [Google Scholar] [CrossRef] [PubMed]
- Scala, M.; Mojarrad, M.; Riazuddin, S. RSRC1 loss-of-function variants cause mild to moderate autosomal recessive intellectual disability. Brain 2020, 143, e31. [Google Scholar] [CrossRef] [PubMed]
- Scala, M.; Nishikawa, M.; Ito, H. Variant-specific changes in RAC3 function disrupt corticogenesis in neurodevelopmental phenotypes. Brain 2022, 145, 3308–3327. [Google Scholar] [CrossRef]
- Vitobello, A.; Mazel, B.; Lelianova, V. ADGRL1 haploinsufficiency causes a variable spectrum of neurodevelopmental disorders in humans and alters synaptic activity and behavior in a mouse model. Am. J. Hum. Genet. 2022, 109, 1436–1457. [Google Scholar] [CrossRef]
- Amadori, E.; Scala, M.; Cereda, G. Targeted re-sequencing for early diagnosis of genetic causes of childhood epilepsy: The Italian experience from the ‘beyond epilepsy’ project. Ital. J. Pediatr. 2020, 46, 92. [Google Scholar] [CrossRef]

| Study | Design | Year of Publication | Patient Age | Objective |
|---|---|---|---|---|
| Snijders et al., 2015 [7]. | Cohort study | 2015 | 1–33 years | Presentation of 37 unique deleterious de novo mutations in the DDX3X gene identified by whole exome sequencing. |
| Wang et al., 2018 [12]. | Cohort study | 2018 | 1–47 years | Description of DNA variants and phenotypes associated with DDX3X disorders. |
| Beal et al., 2019 [8]. | Cohort study | 2019 | 3–15 years | Characterization of the genotypic—phenotypic spectrum associated with heterogeneous DDX3X syndrome. |
| Lennox et al., 2020 [9]. | Cohort study | 2020 | 1–24 years | Elucidation of mechanisms by which pathogenic DDX3X variants disrupt brain development. |
| Tang et al., 2021 [24]. | Research | 2021 | 3–16 years | Expanding the knowledge of the neurobehavioral phenotype of the DDX3X syndrome in the first prospective study. |
| Ng- Cordell et al., 2021 [23]. | Cohort study | 2021 | 3–22 years | Comparison of social and emotional characteristics in patients with DDX3X variants to individuals with other monogenic causes of ID. |
| Stefaniak et al., 2022 [19]. | Case report | 2022 | 7 years | Introduction to symptoms of the musculoskeletal system and sensory integration processing disorders in the DDX3X syndrome. |
| Dai et al., 2022 [26]. | Cohort study | 2022 | 1–6 years | Identification of the clinical and genetic features of the DDX3X syndrome in Chinese patients. |
| Levy et al., 2023 [15]. | Cohort study | 2023 | 3–16 years | Presentation of clinical knowledge about the DDX3X syndrome and recommendations for clinical assessments. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefaniak, U.; Malak, R.; Kaczmarek, A.; Samborski, W.; Mojs, E. DDX3X Syndrome Behavioral Manifestations with Particular Emphasis on Psycho-Pathological Symptoms—A Review. Biomedicines 2023, 11, 3046. https://doi.org/10.3390/biomedicines11113046
Stefaniak U, Malak R, Kaczmarek A, Samborski W, Mojs E. DDX3X Syndrome Behavioral Manifestations with Particular Emphasis on Psycho-Pathological Symptoms—A Review. Biomedicines. 2023; 11(11):3046. https://doi.org/10.3390/biomedicines11113046
Chicago/Turabian StyleStefaniak, Urszula, Roksana Malak, Ada Kaczmarek, Włodzimierz Samborski, and Ewa Mojs. 2023. "DDX3X Syndrome Behavioral Manifestations with Particular Emphasis on Psycho-Pathological Symptoms—A Review" Biomedicines 11, no. 11: 3046. https://doi.org/10.3390/biomedicines11113046
APA StyleStefaniak, U., Malak, R., Kaczmarek, A., Samborski, W., & Mojs, E. (2023). DDX3X Syndrome Behavioral Manifestations with Particular Emphasis on Psycho-Pathological Symptoms—A Review. Biomedicines, 11(11), 3046. https://doi.org/10.3390/biomedicines11113046