
Blood Coagulation and Thrombotic Disorders following SARS-CoV-2 Infection and COVID-19 Vaccination
 , , ,
, , ,  , , , , , ,
, , , , , ,  ,
, 
Abstract
:1. Introduction
2. Search Strategy
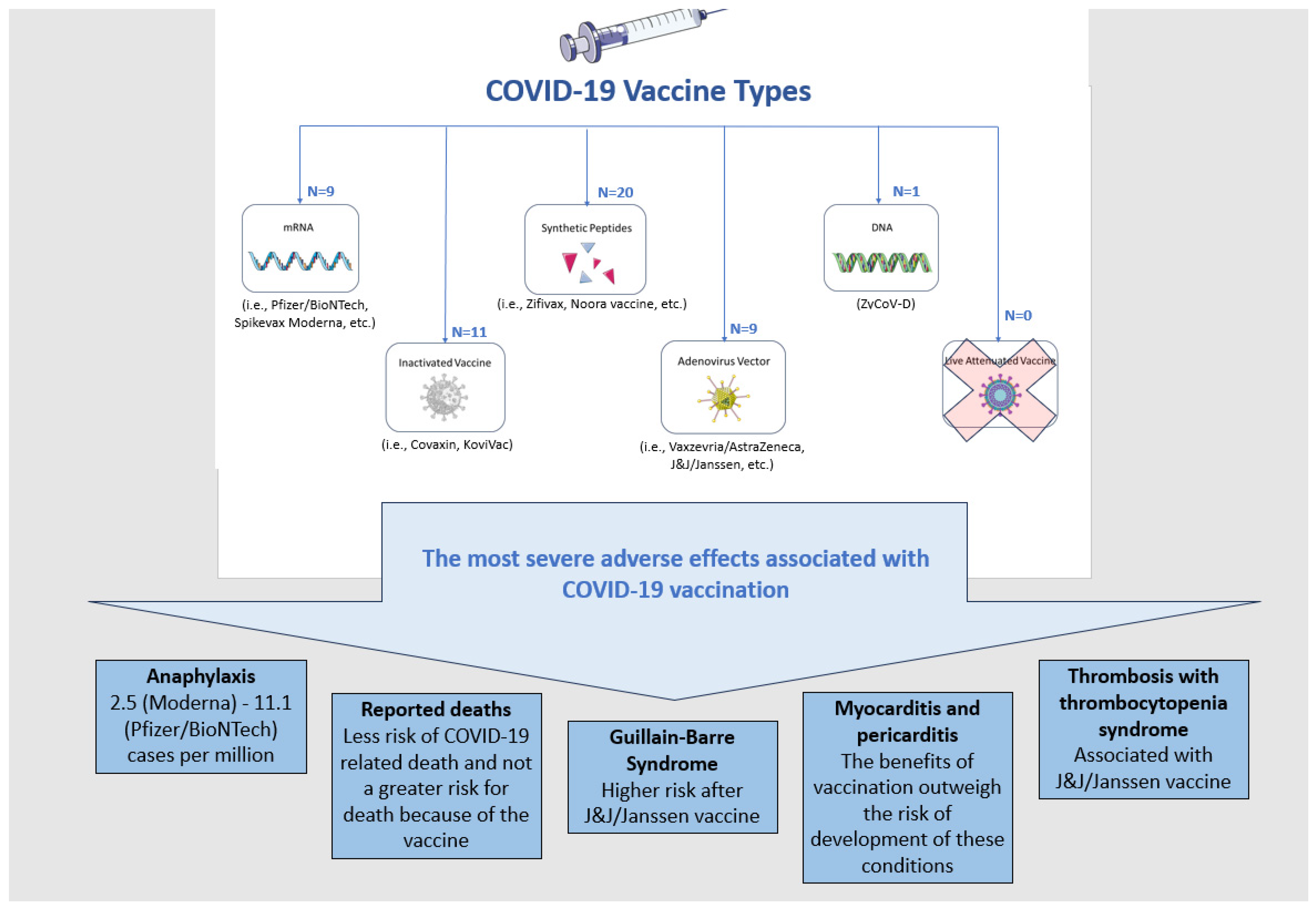
3. SARS-CoV-2 and COVID-19 Vaccines
4. Inherited Blood Coagulation Disorders and COVID-19 Vaccines
5. Congenital Coagulation and Thrombotic Disorders and COVID-19 Vaccines
6. Review of Acquired Coagulation and Thrombotic Disorders and Their Connection with COVID-19 Vaccines—Hypothesis and Therapeutic Interventions
7. Blood Coagulation and Thrombotic Disorders Related to COVID-19 Disease
8. Thrombotic and Bleeding Events following COVID-19 Vaccination: Hypothesis for Pathogenesis and Therapeutic Interventions
9. Summary of Reported Literature Cases of Ultrarare VITT Complications
10. Diagnostics of Coagulopathies following COVID-19 Vaccination through Imaging
11. Global Benefit/Risk Ratio of the Various Vaccination Types for Bleeding or Thrombotic Complications
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO COVID-19 Dashboard—Up to Date Data on Pandemic. WHO Heal Emerg Dashboard 2021. Available online: https://covid19.who.int/region/searo/country/id (accessed on 10 July 2023).
- Dhama, K.; Khan, S.; Tiwari, R.; Sircar, S.; Bhat, S.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Coronavirus Disease 2019-COVID-19. Clin. Microbiol. Rev. 2020, 33, e00028-20. [Google Scholar] [CrossRef]
- Sharun, K.; Tiwari, R.; Iqbal Yatoo, M.; Patel, S.K.; Natesan, S.; Dhama, J.; Malik, Y.S.; Harapan, H.; Singh, R.K.; Dhama, K. Antibody-based immunotherapeutics and use of convalescent plasma to counter COVID-19: Advances and prospects. Expert. Opin. Biol. Ther. 2020, 20, 1033–1046. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Sharun, K.; Dhama, K. COVID-19 Vaccine Diplomacy and Equitable Access to Vaccines Amid Ongoing Pandemic. Arch. Med. Res. 2021, 52, 761–763. [Google Scholar] [CrossRef]
- Knoll, M.D.; Wonodi, C. Oxford-AstraZeneca COVID-19 vaccine efficacy. Lancet 2021, 397, 72–74. [Google Scholar] [CrossRef]
- Gasparyan, A.Y.; Ayvazyan, L.; Blackmore, H.; Kitas, G.D. Writing a narrative biomedical review: Considerations for authors, peer reviewers, and editors. Rheumatol. Int. 2011, 31, 1409–1417. [Google Scholar] [CrossRef]
- COVID-10 Vaccine Tracker. Data Are Accurate as of 2 December 2022. Available online: https://covid19.trackvaccines.org/vaccines/approved/#vaccine-list (accessed on 15 August 2023).
- CDC Reported Adverse Events. Safety of COVID-19 Vaccines. 13 July 2023. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html (accessed on 15 August 2023).
- Graña, C.; Ghosn, L.; Evrenoglou, T.; Jarde, A.; Minozzi, S.; Bergman, H.; Buckley, B.S.; Probyn, K.; Villanueva, G.; Henschke, N.; et al. Efficacy and safety of COVID-19 vaccines. Cochrane Database Syst. Rev. 2022, 12, CD015477. [Google Scholar] [CrossRef] [PubMed]
- Graham, R.L.; Donaldson, E.F.; Baric, R.S. A decade after SARS: Strategies for controlling emerging coronaviruses. Nat. Rev. Microbiol. 2013, 11, 836–848. [Google Scholar] [CrossRef]
- Pardi, N.; Hogan, M.J.; Porter, F.W.; Weissman, D. mRNA vaccines–a new era in vaccinology. Nat. Rev. Drug Discov. 2018, 17, 261. [Google Scholar] [CrossRef]
- Pardi, N.; Tuyishime, S.; Muramatsu, H.; Kariko, K.; Mui, B.L.; Tam, Y.K.; Madden, T.D.; Hope, M.J.; Weissman, D. Expression kinetics of nucleoside-modified mRNA delivered in lipid nanoparticles to mice by various routes. J. Control Release 2015, 217, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Wrapp, D.; Wang, N.; Corbett, K.S.; Goldsmith, J.A.; Hsieh, C.-L.; Abiona, O.; Graham, B.S.; McLellan, J.S. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science 2020, 367, 1260–1263. [Google Scholar] [CrossRef] [PubMed]
- Karikó, K.; Muramatsu, H.; Welsh, F.A.; Ludwig, J.; Kato, H.; Akira, S.; Weissman, D. Incorporation of pseudouridine into mRNA yields superior nonimmunogenic vector with increased translational capacity and biological stability. Mol. Ther. 2008, 16, 1833–1840. [Google Scholar] [CrossRef] [PubMed]
- Corbett, K.S.; Edwards, D.; Leist, S.R.; Abiona, O.M.; Boyoglu-Barnum, S.; Gillespie, R.A.; Himansu, S.; Schäfer, A.; Ziwawo, C.T.; DiPiazza, A.T.; et al. SARS-Co-V-2 mRNA vaccine development enabled by prototype pathogen preparedness. Nature 2020, 586, 567–571. [Google Scholar] [CrossRef]
- Vaxzevria (Previously COVID-19 Vaccine Astra Zeneca): EPAR—Product Information, Vol. 2021. European Medicines Agency, 2021. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/vaxzevria (accessed on 15 August 2023).
- Greinacher, A.; Selleng, K.; Palankar, R.; Wesche, J.; Handtke, S.; Wolff, M.; Aurich, K.; Lalk, M.; Methling, K.; Völker, U.; et al. Insights in ChAdOx1 nCoV-19 vaccine-induced immune thrombotic thrombocytopenia. Blood 2021, 138, 2256–2268. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Xia, S.; Liu, M.; Wang, C.; Xu, W.; Lan, Q.; Feng, S.; Qi, F.; Bao, L.; Du, L.; Liu, S.; et al. Inhibition of SARS-CoV-2 (previously 2019-nCoV) infection by a highly potent pan-coronavirus fusion inhibitor targeting its spike protein that harbors a high capacity to mediate membrane fusion. Cell Res. 2020, 30, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Zhong, G.; Zhang, J.; Shuai, L.; Chen, W. A single dose of an adenovirus-vectored vaccine provides protection against SARS-CoV-2 challenge. Nat. Commun. 2020, 11, 4081. [Google Scholar] [CrossRef]
- Logunov, D.Y.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Tukhvatulin, A.I.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S.; et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021, 397, 671–681. [Google Scholar] [CrossRef]
- Naygovzina, N.B.; Khabriev, R.U.; Krasheninnikov, A.E.; Matveev, A.V. The organizational aspects of security support of participants of clinical testing of vaccine “Gam-COVID-Vac”. Probl. Sotsialnoi Gig. Zdr. Istor. Med. 2021, 29, 5–13. (In Russian) [Google Scholar]
- Doroftei, B.; Ciobica, A.; Ilie, O.D.; Maftei, R.; Ilea, C. Mini-review discussing the reliability and efficiency of COVID-19 vaccines. Diagnostics 2021, 11, 579. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhang, Y.; Huang, B.; Deng, W.; Yang, X. Development of an inactivated vaccine candidate, BBIBP-CorV, with potent protection against SARS-CoV-2. Cell 2020, 182, 713–721.e9. [Google Scholar] [CrossRef] [PubMed]
- Al Kaabi, N.; Zhang, Y.; Xia, S.; Yang, Y.; Al Qahtani, M.M.; Abdulrazzaq, N.; Al Nusair, M.; Hassany, M.; Jawad, J.S.; Abdalla, J.; et al. Effect of 2 inactivated SARS-CoV-2 vaccines on symptomatic COVID-19 infection in adults: A randomized clinical trial. JAMA 2021, 326, 35–45. [Google Scholar] [CrossRef]
- Gao, Q.; Bao, L.; Mao, H.; Wang, L.; Xu, K.; Yang, M.; Li, Y.; Zhu, L.; Wang, N.; Lv, Z.; et al. Development of an inactivated vaccine candidate for SARS-CoV-2. Science 2020, 369, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Keech, C.; Albert, G.; Cho, I.; Robertson, A.; Reed, P.; Neal, S.; Plested, J.S.; Zhu, M.; Cloney-Clark, S.; Zhou, H.; et al. Phase 1-2 Trial of a SARS-CoV-2 Recombinant Spike Protein Nanoparticle Vaccine. N. Engl. J. Med. 2020, 383, 2320–2332. [Google Scholar] [CrossRef]
- Andrikovics, H.; Klein, I.; Bors, A.; Nemes, L.; Marosi, A.; Varadi, A.; Tordai, A. Analysis of large structural changes of the factor VIII gene, involving intron 1 and 22, in severe hemophilia A. Haematologica 2003, 88, 778–784. [Google Scholar]
- Rossaint, R.; Afshari, A.; Bouillon, B.; Cerny, V.; Cimpoesu, D.; Curry, N.; Duranteau, J.; Filipescu, D.; Grottke, O.; Grønlykke, L.; et al. The European guideline on management of major bleeding and coagulopathy following trauma: Sixth edition. Crit. Care 2023, 27, 80. [Google Scholar] [CrossRef]
- Salen, P.; Babiker, H.M. Hemophilia A. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470265/ (accessed on 15 August 2023).
- Konkle, B.A.; Nakaya Fletcher, S. Hemophilia A. In GeneReviews® [Internet]; Adam, M.P., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Angelini, D.; Konkle, B.A.; Sood, S.L. Aging among persons with hemophilia: Contemporary concerns. Semin. Hematol. 2016, 53, 35–39. [Google Scholar] [CrossRef]
- Mericliler, M.; Narayan, G. Outcomes of COVID-19 in Adult Males with Hemophilia A: A Propensity Score-Matched Analysis. Cureus 2022, 14, e30662. [Google Scholar] [CrossRef]
- Tiede, A.; Leise, H.; Horneff, S.; Oldenburg, J.; Halimeh, S.; Heller, C.; Königs, C.; Holstein, K.; Pfrepper, C. Safety of intramuscular COVID-19 vaccination in patients with haemophilia. Haemophilia 2022, 28, 687–693. [Google Scholar] [CrossRef]
- Velikov, T.; Keremidchiev, G.; Velikova, T. How to use Safely COVID-19 Vaccines in Patients on Anticoagulants or Antiaggregants. Int. J. Preven Cardio. 2021, 1, 32–33. [Google Scholar]
- Duminuco, A.; Calagna, M.; Markovic, U.; Esposito, B.; Grasso, S.; Riccobene, C.; Di Raimondo, F.; Giuffrida, G. Acquired hemophilia A following COVID-19 vaccination—The importance of prompt diagnosis: A case report. Transfus. Apher. Sci. 2023, 62, 103577. [Google Scholar] [CrossRef]
- Al Hennawi, H.; Al Masri, M.K.; Bakir, M.; Albarazi, M.; Jazaeri, F.; Almasri, T.N.; Shoura, S.J.; Barakeh, A.R.R.; Taftafa, A.; Khan, M.K.; et al. Acquired Hemophilia A Post-COVID-19 Vaccination: A Case Report and Review. Cureus 2022, 14, e21909. [Google Scholar] [CrossRef] [PubMed]
- Happaerts, M.; Vanassche, T. Acquired hemophilia following COVID-19 vaccination: Case report and review of literature. Res. Pract. Thromb. Haemost. 2022, 6, e12785. [Google Scholar] [CrossRef]
- Emna, B.; Kmira, Z.; Hajer, B.I.; Nadia, S.; Yossra, D.; Amina, B.; Yosra, B.Y.; Haifa, R.; Abderrahim, K. Acquired hemophilia A following COVID-19 vaccine: A case report. J. Med. Case Rep. 2023, 17, 125. [Google Scholar] [CrossRef] [PubMed]
- Ai Vuen, L.; Aun Su-Yin, E.; Naila Kori, A.; Shah, T.M. Case of acquired haemophilia a in Southeast Asia following COVID-19 vaccine. BMJ Case Rep. CP 2022, 15, e246922. [Google Scholar] [CrossRef]
- Hosoi, H.; Tane, M.; Kosako, H.; Ibe, M.; Takeyama, M.; Murata, S.; Mushino, T.; Sonoki, T. Acute-type acquired hemophilia A after COVID-19 mRNA vaccine administration: A new disease entity? J. Autoimmun. 2022, 133, 102915. [Google Scholar] [CrossRef]
- Radwi, M.; Farsi, S. A case report of acquired hemophilia following COVID-19 vaccine. J. Thromb. Haemost. 2021, 19, 1515–1518. [Google Scholar] [CrossRef]
- Goodeve, A.; James, P. von Willebrand Disease. In GeneReviews® [Internet]; Adam, M.P., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Michiels, J.J.; van Vliet, H.H.; Berneman, Z.; Gadisseur, A.; van der Planken, M.; Schroyens, W.; van der Velden, A.; Budde, U. Intravenous DDAVP and factor VIII-von Willebrand factor concentrate for the treatment and prophylaxis of bleedings in patients With von Willebrand disease type 1, 2 and 3. Clin. Appl. Thromb. Hemost. 2007, 13, 14–34. [Google Scholar] [CrossRef] [PubMed]
- Mei, Z.W.; van Wijk, X.M.R.; Pham, H.P.; Marin, M.J. Role of von Willebrand Factor in COVID-19 Associated Coagulopathy. J. Appl. Lab. Med. 2021, 6, 1305–1315. [Google Scholar] [CrossRef]
- NHF President and CEO Leonard Valentino, MD, Discusses the Role of von Willebrand Factor (VWF) in Severe Cases of COVID-19. Available online: https://www.hemophilia.org/news/covid-19-and-vwf (accessed on 15 August 2023).
- Konkle, B.A.; Nakaya Fletcher, S. Hemophilia B. In GeneReviews® [Internet]; Adam, M.P., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Pipe, S.W.; Kaczmarek, R.; Srivastava, A.; Pierce, G.F.; Makris, M.; Hermans, C.; Interim Guidance; Coagulation Products Safety, Supply and Access (CPSSA) Committee of the World Federation of Hemophilia. Management of COVID-19-associated coagulopathy in persons with haemophilia. Haemophilia 2021, 27, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Dautaj, A.; Krasi, G.; Bushati, V.; Precone, V.; Gheza, M.; Fioretti, F.; Sartori, M.; Costantini, A.; Benedetti, S.; Bertelli, M. Hereditary thrombophilia. Acta Biomed. 2019, 90, 44–46. [Google Scholar] [CrossRef] [PubMed]
- Thorelli, E.; Kaufman, R.J.; Dahlbäck, B. Cleavage of factor V at Arg 506 by activated protein C and the expression of anticoagulant activity of factor V. Blood 1999, 93, 2552–2558. [Google Scholar] [CrossRef]
- Padda, I.S.; Patel, P.; Citla Sridhar, D. Protein C and S. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK557814/ (accessed on 15 August 2023).
- Kate, M.K.; van der Meer, J. Protein S deficiency: A clinical perspective. Haemophilia 2008, 14, 1222–1228. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, M.O.; Rogers, H.J. Hypercoagulable states: An algorithmic approach to laboratory testing and update on monitoring of direct oral anticoagulants. Blood Res. 2014, 49, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Park, W.C.; Chang, J.H. Clinical Implications of Methylenetetrahydrofolate Reductase Mutations and Plasma Homocysteine Levels in Patients with Thromboembolic Occlusion. Vasc. Spec. Int. 2014, 30, 113–119. [Google Scholar] [CrossRef]
- Houghton, D.E.; Wysokinski, W.E.; Padrnos, L.J.; Shah, S.; Wysokinska, E.; Pruthi, R.; Ghorbanzadeh, A.; Ashrani, A.; Sridharan, M.; McBane, R.D.; et al. Venous thromboembolism after COVID-19 vaccination in patients with thrombophilia. Am. J. Hematol. 2023, 98, 566–570. [Google Scholar] [CrossRef]
- Elalamy, I.; Gerotziafas, G.; Alamowitch, S.; Laroche, J.P.; Van Dreden, P.; Ageno, W.; Beyer-Westendorf, J.; Cohen, A.T.; Jimenez, D.; Brenner, B.; et al. SARS-CoV-2 Vaccine and Thrombosis: An Expert Consensus on Vaccine-Induced Immune Thrombotic Thrombocytopenia. Thromb. Haemost. 2021, 121, 982–991. [Google Scholar] [CrossRef]
- De Lau, L.M.; Leebeek, F.W.; de Maat, M.P.; Koudstaal, P.J.; Dippel, D.W. A review of hereditary and acquired coagulation disorders in the aetiology of ischaemic stroke. Int. J. Stroke 2010, 5, 385–394. [Google Scholar] [CrossRef]
- Tripodi, A.; Mancuso, M.E.; Chantarangkul, V.; Clerici, M.; Bader, R.; Meroni, P.L.; Santagostino, E.; Mannucci, P.M. Lupus anticoagulants and their relationship with the inhibitors against coagulation factor VIII: Considerations on the differentiation between the 2 circulating anticoagulants. Clin. Chem. 2005, 51, 1883–1885. [Google Scholar] [CrossRef]
- Caldwell, S.H.; Hoffman, M.; Lisman, T.; Macik, B.G.; Northup, P.G.; Reddy, K.R.; Tripodi, A.; Sanyal, A.J.; Coagulation in Liver Disease Group. Coagulation disorders and hemostasis in liver disease: Pathophysiology and critical assessment of current management. Hepatology 2006, 44, 1039–1046. [Google Scholar] [CrossRef]
- Levi, M.; Toh, C.H.; Thachil, J.; Watson, H.G. Guidelines for the diagnosis and management of disseminated intravascular coagulation. British Committee for Standards in Haematology. Br. J. Haematol. 2009, 145, 24–33. [Google Scholar] [CrossRef]
- Aladdin, Y.; Algahtani, H.; Shirah, B. Vaccine-Induced Immune Thrombotic Thrombocytopenia with Disseminated Intravascular Coagulation and Death following the ChAdOx1 nCoV-19 Vaccine. J. Stroke Cerebrovasc. Dis. 2021, 30, 105938. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, V.; Caranci, F.; Negro, A.; Piscitelli, V.; Tuccillo, B.; Fasano, F.; Sirabella, G.; Marano, I.; Granata, V.; Grassi, R.; et al. A Rare Case of Cerebral Venous Thrombosis and Disseminated Intravascular Coagulation Temporally Associated to the COVID-19 Vaccine Administration. J. Pers. Med. 2021, 11, 285. [Google Scholar] [CrossRef] [PubMed]
- Bílková, S.; Hirmerová, J. Coagulopathy associated with COVID-19. Koagulopatie asociovaná s onemocněním COVID-19. Vnitr. Lek. 2020, 66, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Shaw, R.J.; Bradbury, C.; Abrams, S.T.; Wang, G.; Toh, C.H. COVID-19 and immunothrombosis: Emerging understanding and clinical management. Br. J. Haematol. 2021, 194, 518–529. [Google Scholar] [CrossRef]
- Ward, S.E.; Fogarty, H.; Karampini, E.; Lavin, M.; Schneppenheim, S.; Dittmer, R.; Morrin, H.; Glavey, S.; Ni Cheallaigh, C.; Bergin, C.; et al. ADAMTS13 regulation of VWF multimer distribution in severe COVID-19. J. Thromb. Haemost. 2021, 19, 1914–1921. [Google Scholar] [CrossRef]
- Flaumenhaft, R.; Enjyoji, K.; Schmaier, A.A. Vasculopathy in COVID-19. Blood 2022, 140, 222–235. [Google Scholar] [CrossRef]
- Whitworth, H.; Sartain, S.E.; Kumar, R.; Armstrong, K.; Ballester, L.; Betensky, M.; Cohen, C.T.; Diaz, R.; Diorio, C.; Goldenberg, N.A.; et al. Rate of thrombosis in children and adolescents hospitalized with COVID-19 or MIS-C. Blood 2021, 138, 190–198. [Google Scholar] [CrossRef]
- Riphagen, S.; Gomez, X.; Gonzalez-Martinez, C.; Wilkinson, N.; Theocharis, P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet 2020, 395, 1607–1608. [Google Scholar] [CrossRef] [PubMed]
- Lazova, S.; Gerenska, D.; Slabakova, Y.; Velikova, T. Immunological features of the multisystem inflammatory syndrome associated with SARS-CoV-2 in children. Am. J. Clin. Exp. Immunol. 2022, 11, 64–71. [Google Scholar]
- Lazova, S.; Dimitrova, Y.; Hristova, D.; Tzotcheva, I.; Velikova, T. Cellular, Antibody and Cytokine Pathways in Children with Acute SARS-CoV-2 Infection and MIS-C-Can We Match the Puzzle? Antibodies 2022, 11, 25. [Google Scholar] [CrossRef] [PubMed]
- Flaczyk, A.; Rosovsky, R.P.; Reed, C.T.; Bankhead-Kendall, B.K.; Bittner, E.A.; Chang, M.G. Comparison of published guidelines for management of coagulopathy and thrombosis in critically ill patients with COVID 19: Implications for clinical practice and future investigations. Crit. Care 2020, 24, 559. [Google Scholar] [CrossRef]
- Cuker, A.; Tseng, E.K.; Nieuwlaat, R.; Angchaisuksiri, P.; Blair, C.; Dane, K.; Davila, J.; DeSancho, M.T.; Diuguid, D.L.; Griffin, D.O.; et al. American Society of Hematology 2021 guidelines on the use of anticoagulation for thromboprophylaxis in patients with COVID-19. Blood Adv. 2021, 5, 872–888. [Google Scholar] [CrossRef]
- Klok, F.A.; Kruip, M.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: An updated analysis. Thromb. Res. 2020, 191, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety Efficacy of the BNT162b2 mRNACovid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Sadoff, J.; Le Gars, M.; Shukarev, G.; Heerwegh, D.; Truyers, C.; de Groot, A.M.; Stoop, J.; Tete, S.; Van Damme, W.; Leroux-Roels, I.; et al. Interim Results of a Phase 1-2a Trial of Ad26COV2SCovid-19 Vaccine. N. Engl. J. Med. 2021, 384, 1824–1835. [Google Scholar] [CrossRef]
- WHO Guidance for Clinical Case Management of Thrombosis with Thrombocytopenia Syndome (TTS) Following Vaccination to Prevent Coronavirus Disease (COVID-19). Available online: https://apps.who.int/iris/bitstream/handle/10665/342999/WHO-2019-nCoV-TTS-2021.1-eng.pdf?sequence=1&isAllowed=y (accessed on 7 July 2023).
- Schultz, N.H.; Sørvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.-H.; Skattør, T.H.; Tjønnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2124–2130. [Google Scholar] [CrossRef]
- Scully, M.; Singh, D.; Lown, R.; Poles, A.; Solomon, T.; Levi, M.; Goldblatt, D.; Kotoucek, P.; Thomas, W.; Lester, W. Pathologic Antibodies to Platelet Factor 4 after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2202–2211. [Google Scholar] [CrossRef] [PubMed]
- Weller, S.C.; Porterfield, L.; Davis, J.; Wilkinson, G.S.; Chen, L.; Baillargeon, J. Incidence of venous thrombotic events and events of special interest in a retrospective cohort of commercially insured US patients. BMJ Open 2022, 12, e054669. [Google Scholar] [CrossRef] [PubMed]
- Palaiodimou, L.; Stefanou, M.I.; de Sousa, D.A.; Coutinho, J.M.; Papadopoulou, M.; Papaevangelou, V.; Vassilakopoulos, T.I.; Tsiodras, S.; Filippou, D.K.; Tsivgoulis, G. Cerebral venous sinus thrombosis in the setting of COVID-19 vaccination: A systematic review and meta-analysis. J. Neurol. 2022, 269, 3413–3419. [Google Scholar] [CrossRef]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Sharifian-Dorche, M.; Bahmanyar, M.; Sharifian-Dorche, A.; Mohammadi, P.; Nomovi, M.; Mowla, A. Vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis post COVID-19 vaccination; a systematic review. J. Neurol. Sci. 2021, 428, 117607. [Google Scholar] [CrossRef]
- Sarode, R.; Bandarenko, N.; Brecher, M.E.; Kiss, J.E.; Marques, M.B.; Szczepiorkowski, Z.M.; Winters, J.L. Thrombotic thrombocytopenic purpura: 2012 American Society for Apheresis (ASFA) consensus conference on classification, diagnosis, management, and future research. J. Clin. Apher. 2014, 29, 148–167. [Google Scholar] [CrossRef]
- Australian Government Department of Health Therapeutic Goods Administration. COVID-19 Vaccine Weekly Safety Report. Available online: https://www.tga.gov.au/news/covid-19-vaccine-safety-reports/covid-19-vaccine-weekly-safety-report-21-10-2021 (accessed on 15 August 2023).
- Therapeutic Goods Administration (TGA). Australian Government Department of Health; 2021 [citado 7 de Dezembro de 2021]. Available online: https://www.tga.gov.au/periodic/covid-19-vaccine-weekly-safety-report-14-10-2021 (accessed on 15 August 2023).
- Medicines & Healthcare Products, Regulatory Agency. Coronavirus Vaccine—Weekly Summary of Yellow Card Reporting [Internet]. GOV.UK. 2021 [citado 7 de Dezembro de 2021]. Available online: https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions/coronavirus-vaccine-summary-of-yellow-card-reporting (accessed on 15 August 2023).
- Hwang, J.; Park, S.H.; Lee, S.W.; Lee, S.B.; Lee, M.H.; Jeong, G.H.; Kim, M.S.; Kim, J.Y.; Koyanagi, A.; Jacob, L.; et al. Predictors of mortality in thrombotic thrombocytopenia after adenoviral COVID-19 vaccination: The FAPIC score. Eur. Heart J. 2021, 42, 4053–4063. [Google Scholar] [CrossRef]
- Thiele, T.; Weisser, K.; Schönborn, L.; Funk, M.B.; Weber, G.; Greinacher, A.; Keller-Stanislawski, B. Laboratory confirmed vaccine-induced immune thrombotic thrombocytopenia: Retrospective analysis of reported cases after vaccination with ChAdOx-1 nCoV-19 in Germany. Lancet Reg. Health Eur. 2022, 12, 100270. [Google Scholar] [CrossRef]
- Saluja, P.; Gautam, N.; Yadala, S.; Venkata, A.N. Thrombotic thrombocytopenic purpura (TTP) after COVID-19 vaccination: A systematic review of reported cases. Thromb. Res. 2022, 214, 115–121. [Google Scholar] [CrossRef]
- Tiede, A.; Sachs, U.J.; Czwalinna, A.; Werwitzke, S.; Bikker, R.; Krauss, J.K.; Donnerstag, F.; Weißenborn, K.; Höglinger, G.; Maasoumy, B.; et al. Pro-thrombotic immune thrombocytopenia after COVID-19 vaccination. Blood 2021, 138, 350–353. [Google Scholar] [CrossRef]
- Pottegård, A.; Lund, L.C.; Karlstad, Ø.; Dahl, J.; Andersen, M.; Hallas, J.; Lidegaard, Ø.; Tapia, G.; Gulseth, H.L.; Ruiz, P.L.; et al. Arterial events, venous thromboembolism, thrombocytopenia, and bleeding after vaccination with Oxford AstraZeneca ChAdOx1-S in Denmark and Norway: Population-based cohort study. BMJ 2021, 373, n1114. [Google Scholar] [CrossRef]
- Cari, L.; Fiore, P.; Naghavi Alhosseini, M.; Sava, G.; Nocentini, G. Blood clots and bleeding events following BNT162b2 and ChAdOx1 nCoV-19 vaccine: An analysis of European data. J. Autoimmun. 2021, 122, 102685. [Google Scholar] [CrossRef]
- Palaiodimou, L.; Stefanou, M.I.; Katsanos, A.H.; Aguiar de Sousa, D.; Coutinho, J.M.; Lagiou, P.; Michopoulos, I.; Naska, A.; Giannopoulos, S.; Vadikolias, K.; et al. Cerebral Venous Sinus Thrombosis and Thrombotic Events After Vector-Based COVID-19 Vaccines: A Systematic Review and Meta-analysis. Neurology 2021, 97, e2136–e2147. [Google Scholar] [CrossRef]
- Hafeez, M.U.; Ikram, M.; Shafiq, Z.; Sarfraz, A.; Sarfraz, Z.; Jaiswal, V.; Sarfraz, M.; Chérrez-Ojeda, I. COVID-19 vaccine-associated thrombosis with thrombocytopenia syndrome (TTS): A systematic review and post hoc analysis. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211048815. [Google Scholar] [CrossRef] [PubMed]
- Klein, N.P.; Lewis, N.; Goddard, K.; Fireman, B.; Zerbo, O.; Hanson, K.E.; Donahue, J.G.; Kharbanda, E.O.; Naleway, A.; Nelson, J.C.; et al. Surveillance for Adverse Events After COVID-19 mRNA Vaccination. JAMA 2021, 326, 1390–1399. [Google Scholar] [CrossRef] [PubMed]
- Mouta Nunes de Oliveira, P.; Mendes-de-Almeida, D.P.; Bertollo Gomes Porto, V.; Crespo Cordeiro, C.; Vitiello Teixeira, G.; Saraiva Pedro, R.; Roberto Gomes Takey, P.; Kegele Lignani, L.; Reis Xavier, J.; Cardoso Doria da Gama, V.; et al. Vaccine-induced immune thrombotic thrombocytopenia after COVID-19 vaccination: Description of a series of 39 cases in Brazil. Vaccine 2022, 40, 4788–4795. [Google Scholar] [CrossRef]
- Stam, J. Thrombosis of the cerebral veins and sinuses. N. Engl. J. Med. 2005, 352, 1791–1798. [Google Scholar] [CrossRef] [PubMed]
- Otite, F.O.; Patel, S.; Sharma, R.; Khandwala, P.; Desai, D.; Latorre, J.G.; Akano, E.O.; Anikpezie, N.; Izzy, S.; Malik, A.M.; et al. Trends in incidence and epidemiologic characteristics of cerebral venous thrombosis in the United States. Neurology 2020, 95, e2200–e2213. [Google Scholar] [CrossRef]
- Schulz, J.B.; Berlit, P.; Diener, H.C.; Gerloff, C.; Greinacher, A.; Klein, C.; Petzold, G.C.; Piccininni, M.; Poli, S.; Rohrig, R.; et al. COVID-19 Vaccine-Associated Cerebral Venous Thrombosis in Germany. Ann. Neurol. 2021, 90, 627–639. [Google Scholar] [CrossRef]
- European Medicines Agency. 29 March 2021 Update. COVID-19 Vaccine Safety Update VAXZEVRIA AstraZeneca AB. Available online: https://www.ema.europa.eu/en/search/search?search_api_views_fulltext=CVT+after+COVID-19+vaccination+administration (accessed on 12 July 2023).
- European Medicines Agency. COVID-19 Vaccine Janssen: EMA Finds Possible Link to Very Rare Cases of Unusual Blood Clots with Low Blood Platelets. 20 April 2021. Available online: https://www.ema.europa.eu/en/news/covid-19-vaccine-janssen-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood (accessed on 12 July 2023).
- See, I.; Su, J.R.; Lale, A.; Woo, E.J.; Guh, A.Y.; Shimabukuro, T.T.; Streiff, M.B.; Rao, A.K.; Wheeler, A.P.; Beavers, S.F.; et al. US Case Reports of Cerebral Venous Sinus Thrombosis with Thrombocytopenia After Ad26.COV2.S Vaccination, March 2 to April 21, 2021. JAMA 2021, 325, 2448–2456. [Google Scholar] [CrossRef]
- Franchini, M.; Testa, S.; Pezzo, M.; Glingani, C.; Caruso, B.; Terenziani, I.; Pognani, C.; Bellometti, S.A.; Castelli, G. Cerebral venous thrombosis and thrombocytopenia post-COVID-19 vaccination. Thromb. Res. 2021, 202, 182–183. [Google Scholar] [CrossRef]
- Franchini, M.; Liumbruno, G.M. Pezzo MCOVID-19 vaccine-associated immune thrombosis thrombocytopenia (VITT): Diagnostic therapeutic recommendations for a new syndrome. Eur. J. Haematol. 2021, 107, 173–180. [Google Scholar] [CrossRef]
- Rizk, J.G.; Gupta, A.; Sardar, P.; Henry, B.M.; Lewin, J.C.; Lippi, G.; Lavie, C.J. Clinical Characteristics and Pharmacological Management of COVID-19 Vaccine–Induced Immune Thrombotic Thrombocytopenia with Cerebral Venous Sinus Thrombosis. JAMA Cardiol. 2021, 6, 1451. [Google Scholar] [CrossRef]
- Sørvoll, I.H.; Horvei, K.D.; Ernstsen, S.L.; Lægreid, I.J.; Lund, S.; Grønli, R.H.; Olsen, M.K.; Jacobsen, H.K.; Eriksson, A.; Halstensen, A.M.; et al. An observational study to identify the prevalence of thrombocytopenia and anti-PF4/polyanion antibodies in Norwegian health care workers after COVID-19 vaccination. J. Thromb. Haemost. 2021, 19, 1813–1818. [Google Scholar] [CrossRef]
- Maramattom, B.V.; Moidu, F.M.; Varikkottil, S.; Syed, A.A. Cerebral venous sinus thrombosis after ChAdOx1 vaccination: The first case of definite thrombosis with thrombocytopenia syndrome from India. BMJ Case Rep. 2021, 14, e246455. [Google Scholar] [CrossRef]
- Hekmat, A.S.; Javanmardi, K. Possible Risk of Thrombotic Events following Oxford-AstraZeneca COVID-19 Vaccination in Women Receiving Estrogen. BioMed Res. Int. 2021, 2021, 7702863. [Google Scholar]
- Allas, G.D.O.; Arizala, J.D.R.; Manalo, R.V.M. COVID-19 Adenoviral Vaccine-Induced Immune Thrombotic Thrombocytopenia (VITT), COVID-19-Related Thrombosis, and the Thrombotic Thrombocytopenic Syndromes. Hematol. Rep. 2022, 14, 358–372. [Google Scholar] [CrossRef]
- Wolf, M.E.; Luz, B.; Niehaus, L.; Bhogal, P.; Bäzner, H.; Henkes, H. Thrombocytopenia and Intracranial Venous Sinus Thrombosis after “COVID-19 Vaccine AstraZeneca” Exposure. J. Clin. Med. 2021, 10, 1599. [Google Scholar] [CrossRef]
- Mehta, P.R.; Mangion, S.A.; Benger, M.; Stanton, B.R.; Czuprynska, J.; Arya, R.; Sztriha, L.K. Cerebral venous sinus thrombosis and thrombocytopenia after COVID-19 vaccination—A report of two UK cases. Brain Behav. Immun. 2021, 95, 514–517. [Google Scholar] [CrossRef]
- Guan, C.-Y.; Tsai, S.-H.; Fan, J.-S.; Lin, Y.-K.; Kao, C.-C. A rare case of a middle-age Asian male with cerebral venous thrombosis after COVID-19 AstraZeneca vaccination. Am. J. Emerg. Med. 2021, 51, 427.e3–427.e4. [Google Scholar]
- Panovska-Stavridis, I. A rare case of superior ophthalmic vein thrombosis and thrombocytopenia following ChAdOx1 nCoV-19 vaccine against SARS-CoV-2. Mediterr. J. Hematol. Infect. Dis. 2021, 13, e2021048. [Google Scholar] [CrossRef] [PubMed]
- Walter, U.; Fuchs, M.; Grossmann, A.; Walter, M.; Thiele, T.; Storch, A.; Wittstock, M. Adenovirus-Vectored COVID-19 Vaccine–Induced Immune Thrombosis of Carotid Artery. Neurology 2021, 97, 716–719. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.; Ko, C.-A.; Sung, Y.-F.; Chen, Y.-C.; Lee, J.-T.; Lin, Y.-Q.; Lin, Y.-K. Cerebral Venous Sinus Thrombosis, Pulmonary Embolism, and Thrombocytopenia After COVID-19 Vaccination in a Taiwanese Man: A Case Report and Literature Review. Front. Neurol. 2021, 12, 738329. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Huang, L.-Y.; Chen, Y.-L.; Chan, J.-S.; Chiang, W.-F.; Lin, C.-Y.; Chen, M.-H.; Shyu, H.-Y.; Hsiao, P.-J. ChAdOx1 COVID-19 vaccine-induced thrombocytopenia syndrome. QJM Int. J. Med. 2021, 114, 733–734. [Google Scholar] [CrossRef]
- Strobel, D.; Haberkamp, S.; Zundler, S. Portal Vein Thrombosis due to Vaccine-Induced Immune Thrombotic Thrombocytopenia (VITT) after COVID Vaccination with ChAdOx1 nCoV-19. Ultraschall Med.-Eur. J. Ultrasound 2021, 42, 551–552. [Google Scholar] [CrossRef]
- Fousse, M.; Schub, D.; Merzou, F.; Fassbender, K.; Sester, M.; Kettner, M.; Lochner, P.; Schmidt, T.; Júnior, J.R.G. Case report: Cerebral sinus vein thrombosis in two patients with AstraZeneca SARS-CoV-2 vaccination. J. Neurol. 2021, 269, 583–586. [Google Scholar] [CrossRef]
- Ceschia, N.; Scheggi, V.; Gori, A.M.; Rogolino, A.A.; Cesari, F.; Giusti, B.; Cipollini, F.; Marchionni, N.; Alterini, B.; Marcucci, R. Diffuse pro-thrombotic syndrome after ChAdOx1 nCoV-19 vaccine administration: A case report. J. Med. Case Rep. 2021, 15, 496. [Google Scholar] [CrossRef]
- Chiang, C.-Y.; Chen, C.-Y.; Yu, W.-L.; Kan, W.-C.; Feng, Y.-H. Myocardial Infarction and Azygos Vein Thrombosis After ChAdOx1 nCoV-19 Vaccination in a Hemodialysis Patient. Cureus 2021, 13, 18390. [Google Scholar] [CrossRef]
- Hocking, J.; Chunilal, S.D.; Chen, V.M.; Brighton, T.; Nguyen, J.; Tan, J.; Ting, S.B.; Tran, H. The first known case of vaccine-induced thrombotic thrombocytopenia in Australia. Med. J. Aust. 2021, 215, 19. [Google Scholar] [CrossRef]
- Garnier, M.; Curado, A.; Billoir, P.; Barbay, V.; Demeyere, M.; Dacher, J.-N. Imaging of Oxford/AstraZeneca® COVID-19 vaccine-induced immune thrombotic thrombocytopenia. Diagn. Interv. Imaging 2021, 102, 649–650. [Google Scholar] [CrossRef] [PubMed]
- McKeigue, P.M.; Burgul, R.; Bishop, J.; Robertson, C.; McMenamin, J.; O’Leary, M.; McAllister, D.A.; Colhoun, H.M. Association of cerebral venous thrombosis with recent COVID-19 vaccination: Case-crossover study using ascertainment through neuroimaging in Scotland. BMC Infect. Dis. 2021, 21, 1275. [Google Scholar] [CrossRef]
- Muir, K.-L.; Kallam, A.; Koepsell, S.A.; Gundabolu, K. Thrombotic Thrombocytopenia after Ad26.COV2.S Vaccination. N. Engl. J. Med. 2021, 384, 1964–1965. [Google Scholar] [CrossRef]
- Parums, D.V. Editorial: SARS-CoV-2 mRNA Vaccines and the Possible Mechanism of Vaccine-Induced Immune Thrombotic Thrombocytopenia (VITT). Med. Sci. Monit. 2021, 27, e932899. [Google Scholar] [CrossRef] [PubMed]
- Malik, B.; Kalantary, A.; Rikabi, K.; Kunadi, A. Pulmonary embolism, transient ischaemic attack and thrombocytopenia after the Johnson & Johnson COVID-19 vaccine. BMJ Case Rep. 2021, 14, e243975. [Google Scholar] [PubMed]
- Kennedy, V.E.; Wong, C.C.; Hong, J.M.; Peng, T.A.; Brondfield, S.; Reilly, L.M.; Cornett, P.; Leavitt, A.D. VITT following Ad26.COV2.S vaccination presenting without radiographically demonstrable thrombosis. Blood Adv. 2021, 5, 4662–4665. [Google Scholar] [CrossRef]
- Curcio, R.; Gandolfo, V.; Alcidi, R.; Giacomino, L.; Campanella, T.; Casarola, G.; Rossi, R.; Chiatti, L.; D’Abbondanza, M.; Commissari, R.; et al. Vaccine-induced massive pulmonary embolism and thrombocytopenia following a single dose of Janssen Ad26.COV2.S vaccination. Int. J. Infect. Dis. 2022, 116, 154–156. [Google Scholar] [CrossRef]
- Carli, G.; Nichele, I.; Ruggeri, M.; Barra, S.; Tosetto, A. Deep vein thrombosis (DVT) occurring shortly after the second dose of mRNA SARS-CoV-2 vaccine. Intern. Emerg. Med. 2021, 16, 803–804. [Google Scholar] [CrossRef] [PubMed]
- Meo, S.A.; Bukhari, I.A.; Akram, J.; Meo, A.S.; Klonoff, D.C. COVID-19 vaccines: Comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and Moderna Vaccines. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1663–1669. [Google Scholar] [PubMed]
- Zakaria, Z.; Sapiai, N.A.; Ghani, A.R.I. Cerebral venous sinus thrombosis 2 weeks after the first dose of mRNA SARS-CoV-2 vaccine. Acta Neurochir. 2021, 163, 2359–2362. [Google Scholar] [CrossRef] [PubMed]
- Dias, L.; Soares-Dos-Reis, R.; Meira, J.; Ferrão, D.; Soares, P.R.; Pastor, A.; Gama, G.; Fonseca, L.; Fagundes, V.; Carvalho, M. Cerebral Venous Thrombosis after BNT162b2 mRNA SARS-CoV-2 vaccine. J. Stroke Cerebrovasc. Dis. 2021, 30, 105906. [Google Scholar] [CrossRef]
- Yamaguchi, Y.; Kimihira, L.; Nagasawa, H.; Seo, K.; Wada, M. Cerebral Venous Sinus Thrombosis After BNT162b2 mRNA COVID-19 Vaccination. Cureus 2021, 13, 18775. [Google Scholar] [CrossRef]
- Al-Maqbali, J.S.; Al Rasbi, S.; Kashoub, M.S.; Al Hinaai, A.M.; Farhan, H.; Al Rawahi, B.; Al Alawi, A.M. A 59-Year-Old Woman with Extensive Deep Vein Thrombosis and Pulmonary Thromboembolism 7 Days Following a First Dose of the Pfizer-BioNTech BNT162b2 mRNA COVID-19 Vaccine. Am. J. Case Rep. 2021, 22, e932946. [Google Scholar] [CrossRef]
- Andraska, E.A.; Kulkarni, R.; Chaudhary, M.; Sachdev, U. Three cases of acute venous thromboembolism in females after vaccination for coronavirus disease 2019. J. Vasc. Surg. Venous Lymphat. Disord. 2021, 10, 14–17. [Google Scholar] [CrossRef]
- Okada, Y.; Sakai, R.; Sato-Fitoussi, M.; Nodera, M.; Yoshinaga, S.; Shibata, A.; Kurasawa, T.; Kondo, T.; Amano, K. Potential Triggers for Thrombocytopenia and/or Hemorrhage by the BNT162b2 Vaccine, Pfizer-BioNTech. Front. Med. 2021, 8, 751598. [Google Scholar] [CrossRef]
- Finsterer, J.; Nics, S. Venous sinus thrombosis after the second jab of an mRNA-based SARS-CoV-2 vaccine. Brain Hemorrhages 2021, 3, 36–38. [Google Scholar] [CrossRef]
- Bhan, C.; Bheesham, N.; Shakuntulla, F.; Sharma, M.; Sun, C.; Weinstein, M. An unusual presentation of acute deep vein thrombosis after the Moderna COVID-19 vaccine—A case report. Ann. Transl. Med. 2021, 9, 1605. [Google Scholar] [CrossRef] [PubMed]
- Krzywicka, K.; Heldner, M.R.; Sanchez van Kammen, M.; van Haaps, T.; Hiltunen, S.; Silvis, S.M.; Levi, M.; Kremer Hovinga, J.A.; Jood, K.; Lindgren, E.; et al. Post-SARS-CoV-2-vaccination cerebral venous sinus thrombosis: An analysis of cases notified to the European Medicines Agency. Eur. J. Neurol. 2021, 28, 3656–3662. [Google Scholar] [CrossRef]
- Tobaiqy, M.; Elkout, H.; MacLure, K. Analysis of Thrombotic Adverse Reactions of COVID-19 AstraZeneca Vaccine Reported to EudraVigilance Database. Vaccines 2021, 9, 393. [Google Scholar] [CrossRef] [PubMed]
- Cari, L.; Alhosseini, M.N.; Fiore, P.; Pierno, S.; Pacor, S.; Bergamo, A.; Sava, G.; Nocentini, G. Cardiovascular, neurological, and pulmonary events following vaccination with the BNT162b2, ChAdOx1 nCoV-19, and Ad26.COV2.S vaccines: An analysis of European data. J. Autoimmun. 2021, 125, 102742. [Google Scholar] [CrossRef] [PubMed]
- Abbattista, M.; Martinelli, I.; Peyvandi, F. Comparison of adverse drug reactions among four COVID-19 vaccines in Europe using the EudraVigilance database: Thrombosis at unusual sites. J. Thromb. Haemost. 2021, 19, 2554–2558. [Google Scholar] [CrossRef] [PubMed]
- Hippisley-Cox, J.; Patone, M.; Mei, X.W.; Saatci, D.; Dixon, S.; Khunti, K.; Zaccardi, F.; Watkinson, P.; Shankar-Hari, M.; Doidge, J.; et al. Risk of thrombocytopenia and thromboembolism after COVID-19 vaccination and SARS-CoV-2 positive testing: Self-controlled case series study. BMJ 2021, 374, n1931. [Google Scholar] [CrossRef]
- Gras-Champel, V.; Liabeuf, S.; Baud, M.; Albucher, J.-F.; Benkebil, M.; Boulay, C.; Bron, A.; El Kaddissi, A.; Gautier, S.; Geeraerts, T.; et al. Atypical thrombosis associated with VaxZevria® (AstraZeneca) vaccine: Data from the French Network of Regional Pharmacovigilance Centres. Therapie 2021, 76, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.J.; Stowe, J.; Ramsay, M.E.; Miller, E. Risk of venous thrombotic events and thrombocytopenia in sequential time periods after ChAdOx1 and BNT162b2 COVID-19 vaccines: A national cohort study in England. Lancet Reg. Health-Eur. 2021, 13, 100260. [Google Scholar] [CrossRef] [PubMed]
- Shay, D.K.; Gee, J.; Su, J.R.; Myers, T.R.; Marquez, P.; Liu, R. Safety monitoring of the Janssen (Johnson & Johnson) COVID-19 Vaccine—United States, March–April 2021. MMWR 2021, 70, 680–684. [Google Scholar] [PubMed]
- Smadja, D.M.; Yue, Q.-Y.; Chocron, R.; Sanchez, O.; Louet, A.L.-L. Vaccination against COVID-19: Insight from arterial and venous thrombosis occurrence using data from VigiBase. Eur. Respir. J. 2021, 58, 2100956. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.-J.; Cines, D.B.; Gernsheimer, T.; Kessler, C.; Michel, M.; Tarantino, M.D.; Semple, J.W.; Arnold, D.M.; Godeau, B.; Lambert, M.P.; et al. Thrombocytopenia following Pfizer and Moderna SARS-CoV-2 vaccination. Am. J. Hematol. 2021, 96, 534–537. [Google Scholar] [CrossRef]
- Guetl, K.; Raggam, R.B.; Gary, T. Thrombotic Complications after COVID-19 Vaccination: Diagnosis and Treatment Options. Biomedicines 2022, 10, 1246. [Google Scholar] [CrossRef]
- Markus, A.F.; Strauss, V.Y.; Burn, E.; Li, X.; Delmestri, A.; Reich, C.; Yin, C.; Mayer, M.A.; Ramírez-Anguita, J.M.; Marti, E.; et al. Characterising the treatment of thromboembolic events after COVID-19 vaccination in 4 European countries and the US: An international network cohort study. Front. Pharmacol. 2023, 14, 1118203. [Google Scholar] [CrossRef]
- Wills, A.; Swallow, G.; Kirkman, M.A.; Rajan, K.; Subramanian, G. Arterial and venous thrombotic stroke after ChAdOx1 nCoV-19 vaccine. Clin. Med. 2022, 22, 184–186. [Google Scholar] [CrossRef]
- Berlot, G.; Tomasini, A.; La Fata, C.; Pintacuda, S.; Rigutti, S.; Falanga, A. Widespread Arterial Thrombosis after ChAdOx1 nCov-19 Vaccination. Case Rep. Crit. Care 2022, 2022, 6804456. [Google Scholar] [CrossRef]
- Yeo, S.; Kim, H.; Lee, J.; Yi, J.; Chung, Y.R. Retinal vascular occlusions in COVID-19 infection and vaccination: A literature review. Graefe’s Arch. Clin. Exp. Ophthalmol. 2023, 261, 1793–1808. [Google Scholar] [CrossRef]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk factors and disease profile of post-vaccination SARS-CoV-2 infection in UK users of the COVID Symptom Study app: A prospective, community-based, nested, case-control study. Lancet Infect. Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Timing and Spacing of Immunobiologics. General Best Practice Guidelines for Immunization. Vaccine Recommendations Guidelines of the ACIP. Available online: https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/timing.html (accessed on 2 September 2023).
- Wang, C.A.; Yeh, J.S.; Hong, C.Y. Repeated Coronary Artery Thrombosis after mRNA-1273 COVID-19 Vaccination. Acta Cardiol. Sin. 2022, 38, 793–795. [Google Scholar] [CrossRef]
- Alsmady, M.M.; Al-Qaryouti, R.A.; Sultan, N.G.; Khrais, O.I.; Khrais, H. Upper Limb Ischemia Due to Arterial Thrombosis after COVID-19 Vaccination. Case Rep. Med. 2022, 2022, 4819131. [Google Scholar] [CrossRef] [PubMed]
- Hansen, K.L.; Carlsen, J.F. New Trends in Vascular Imaging. Diagnostics 2021, 11, 112. [Google Scholar] [CrossRef]
- Peycheva, M.V.; Chervenkov, L.; Harizanova, Z.; Ahmed-Popova, F.; Zahariev, Z.I. Ultrasound fusion imaging system in neurology practice. Folia Medica 2022, 64, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Tang, C. Novel study and applications of CT angiography derived fractional flow reserve in China. Zhonghua Yi Xue Za Zhi 2022, 102, 2563–2566. (In Chinese) [Google Scholar] [CrossRef]
- Cademartiri, F.; Casolo, G.; Clemente, A.; Seitun, S.; Mantini, C.; Bossone, E.; Saba, L.; Sverzellati, N.; Nistri, S.; Punzo, B.; et al. Coronary CT angiography: A guide to examination, interpretation, and clinical indications. Expert. Rev. Cardiovasc. Ther. 2021, 19, 413–425. [Google Scholar] [CrossRef]
- Evrev, D.; Sekulovski, M.; Gulinac, M.; Dobrev, H.; Velikova, T.; Hadjidekov, G. Retroperitoneal and abdominal bleeding in anticoagulated COVID-19 hospitalized patients: Case series and brief literature review. World J. Clin. Cases. 2023, 11, 1528–1548. [Google Scholar] [CrossRef]
- De Leucio, A.; De Jesus, O. MR Angiogram. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK558984/ (accessed on 10 July 2023).
- Cau, R.; Mantini, C.; Monti, L.; Mannelli, L.; Di Dedda, E.; Mahammedi, A.; Nicola, R.; Roubil, J.; Suri, J.S.; Cerrone, G.; et al. Role of imaging in rare COVID-19 vaccine multiorgan complications. Insights Imaging 2022, 13, 44. [Google Scholar] [CrossRef]
- Kim, E.-J.; Yoo, S.-J. Pulmonary Embolism after Vaccination with the COVID-19 Vaccine (Pfizer, BNT162b2): A Case Report. Vaccines 2023, 11, 1075. [Google Scholar] [CrossRef]
- Issakov, G.; Tzur, Y.; Friedman, T.; Tzur, T. Abnormal Uterine Bleeding Among COVID-19 Vaccinated and Recovered Women: A National Survey. Reprod. Sci. 2023, 30, 713–721. [Google Scholar] [CrossRef]
- Ljung, R.; Xu, Y.; Sundström, A.; Leach, S.; Hallberg, E.; Bygdell, M.; Larsson, M.; Arthurson, V.; Gisslén, M.; Gedeborg, R.; et al. Association between SARS-CoV-2 vaccination and healthcare contacts for menstrual disturbance and bleeding in women before and after menopause: Nationwide, register-based cohort study. BMJ 2023, 381, e074778. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19: Unusual blood clots are “very rare side effect” of Janssen vaccine, says EMA. BMJ 2021, 373, n1046. [Google Scholar] [CrossRef] [PubMed]
- Hernández, A.F.; Calina, D.; Poulas, K.; Docea, A.O.; Tsatsakis, A.M. Safety of COVID-19 vaccines administered in the EU: Should we be concerned? Toxicol. Rep. 2021, 8, 871–879. [Google Scholar] [CrossRef]
- MacIntyre, C.R.; Veness, B.; Berger, D.; Hamad, N.; Bari, N. Thrombosis with Thrombocytopenia Syndrome (TTS) following AstraZeneca ChAdOx1 nCoV-19 (AZD1222) COVID-19 vaccination—A risk–benefit analysis for people <60 years in Australia. Vaccine 2021, 39, 4784–4787. [Google Scholar] [CrossRef]
- Dyer, O. COVID-19: EMA defends AstraZeneca vaccine as Germany and Canada halt rollouts. BMJ 2021, 373, n883. [Google Scholar] [CrossRef] [PubMed]
- Rosenblum, H.G.; Hadler, S.C.; Moulia, D. Use of COVID-19 vaccines after reports of adverse events among adult recipients of Janssen (Johnson & Johnson) and mRNA COVID-19 Vaccines (Pfizer-BioNTech and Moderna): Update from the Advisory Committee on Immunization Practices—United States, July 2021. MMWR 2021, 70, 1094–1099. [Google Scholar]
- Oliver, S.E.; Wallace, M.; See, I.; Mbaeyi, S.; Godfrey, M.; Hadler, S.C.; Jatlaoui, T.C.; Twentyman, E.; Hughes, M.M.; Rao, A.K.; et al. Use of the Janssen (Johnson & Johnson) COVID-19 Vaccine: Updated Interim Recommendations from the Advisory Committee on Immunization Practices—United States, December 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 90–95. [Google Scholar] [CrossRef]
- Kantarcioglu, B.; Patel, K.; Lewis, J.; Iqbal, O.; Siddiqui, F.; Jabeen, N.; Laddu, A.R.; Carter, C.A.; Fareed, J. Public Perceptions of Current COVID-19 Vaccinations. Results of a Pilot Survey. Clin. Appl. Thromb. 2021, 27. [Google Scholar] [CrossRef] [PubMed]
- Vasilev, G.; Kabakchieva, P.; Miteva, D.; Batselova, H.; Velikova, T. Effectiveness and safety of COVID-19 vaccines in patients with diabetes as a factor for vaccine hesitancy. World J. Diabetes. 2022, 13, 738–751. [Google Scholar] [CrossRef] [PubMed]
- Sen, P.; Naveen, R.; Houshmand, N.; Moghadam Kia, S.; Joshi, M.; Saha, S.; Jagtap, K.; Agarwal, V.; Nune, A.; Nikiphorou, E.; et al. Vaccine hesitancy decreases, long term concerns remain in myositis, rheumatic disease patients: A comparative analysis of the COVAD surveys. Rheumatology 2023, kead057, Epub ahead of print. [Google Scholar] [CrossRef]
- McMurry, R.; Lenehan, P.; Awasthi, S.; Silvert, E.; Puranik, A.; Pawlowski, C.; Venkatakrishnan, A.; Anand, P.; Agarwal, V.; O’Horo, J.C.; et al. Real-time analysis of a mass vaccination effort confirms the safety of FDA-authorized mRNA COVID-19 vaccines. Med 2021, 2, 965–978. [Google Scholar] [CrossRef] [PubMed]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNACovid-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Bikdeli, B.; Chatterjee, S.; Arora, S.; Monreal, M.; Jimenez, D.; Krumholz, H.M.; Goldhaber, S.Z.; Elkind, M.S.; Piazza, G. Cerebral Venous Sinus Thrombosis in the U.S. Population, After Adenovirus-Based SARS-CoV-2 Vaccination, and After COVID-19. J. Am. Coll. Cardiol. 2021, 78, 408–411. [Google Scholar] [CrossRef]
- Huh, K.; Na, Y.; Kim, Y.-E.; Radnaabaatar, M.; Peck, K.R.; Jung, J. Predicted and Observed Incidence of Thromboembolic Events among Koreans Vaccinated with ChAdOx1 nCoV-19 Vaccine. J. Korean Med. Sci. 2021, 36, e197. [Google Scholar] [CrossRef]
- Soliman, D.S.; Al Battah, A.; Al Faridi, D.; Ibrahim, F. Acquired Hemophilia A Developed Post COVID-19 Vaccine: An Extremely Rare Complication. J. Med. Cases. 2022, 13, 1–4. [Google Scholar] [CrossRef]
- Nowak, K.M.; Carpinteiro, A.; Szalai, C.; Saner, F.H. Acquired Hemophilia A: A Permanent Challenge for All Physicians. Medicines 2022, 9, 21. [Google Scholar] [CrossRef]
- Abrignani, M.G.; Murrone, A.; De Luca, L.; Roncon, L.; Di Lenarda, A.; Valente, S.; Caldarola, P.; Riccio, C.; Oliva, F.; Gulizia, M.M.; et al. COVID-19, Vaccines, and Thrombotic Events: A Narrative Review. J. Clin. Med. 2022, 11, 948. [Google Scholar] [CrossRef]
- Angeli, F.; Spanevello, A.; Reboldi, G.; Visca, D. Verdecchia PSARS-CoV-2 vaccines: Lights shadows. Eur. J. Intern. Med. 2021, 88, 1–8. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Type of Study | Vaccine | Number of Participants | Standardized Morbidity Ratio for Any Thrombocytopenia/Coagulation Disorders | Mortality | Authors |
|---|---|---|---|---|---|
| Population-based | Viral vectored | 281,264 | 1.52 (0.97 to 2.25) | NR | Pottegård et al. [95] |
| European database | Viral vectored and m-RNA | NR | Viral vectored vaccine recipients 2.5 (2.3–2.7)mRNA vaccine recipients 1.9 (1.6–2.2) | 0.4 and 4.8 deaths/1 million doses for mRNA and viral vector recipients, respectively | Cari et al. [96] |
| Systematic review | Viral vectored | 4552 participants (12 studies) | OR 13.8; 95% CI 2.0–97.3 | Approximately 1/3 were deceased | Palaiodimou et al. [97] |
| Systematic review | Viral vectored and m-RNA | 69 participants (59 studies) | 63 out of 69 (91.3%) occurred after the viral vector vaccine | 24 deceased | Hafeez et al. [98] |
| Surveillance | m-RNA | 10,162,227 (8 participating US health plans) | Excess cases in risk interval 1.0 (−4.6 to 1.4) per million doses | NR | Klein et al. [99] |
| Systematic review | Viral vectored and m-RNA | 49 participants (12 studies) | NR | 39% deceased | Sharifian-Dorche et al. [86] |
| Case series | Viral vectored and m-RNA | 11 patients | NR | 6 deceased | Greinacher et al. [85] |
| Case series | Viral vectored | 39 cases | NR | 51% deceased | Mouta Nunes de Oliveira et al. [100] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sekulovski, M.; Mileva, N.; Vasilev, G.V.; Miteva, D.; Gulinac, M.; Peshevska-Sekulovska, M.; Chervenkov, L.; Batselova, H.; Vasilev, G.H.; Tomov, L.; et al. Blood Coagulation and Thrombotic Disorders following SARS-CoV-2 Infection and COVID-19 Vaccination. Biomedicines 2023, 11, 2813. https://doi.org/10.3390/biomedicines11102813
Sekulovski M, Mileva N, Vasilev GV, Miteva D, Gulinac M, Peshevska-Sekulovska M, Chervenkov L, Batselova H, Vasilev GH, Tomov L, et al. Blood Coagulation and Thrombotic Disorders following SARS-CoV-2 Infection and COVID-19 Vaccination. Biomedicines. 2023; 11(10):2813. https://doi.org/10.3390/biomedicines11102813
Chicago/Turabian StyleSekulovski, Metodija, Niya Mileva, Georgi Vasilev Vasilev, Dimitrina Miteva, Milena Gulinac, Monika Peshevska-Sekulovska, Lyubomir Chervenkov, Hristiana Batselova, Georgi Hristov Vasilev, Latchezar Tomov, and et al. 2023. "Blood Coagulation and Thrombotic Disorders following SARS-CoV-2 Infection and COVID-19 Vaccination" Biomedicines 11, no. 10: 2813. https://doi.org/10.3390/biomedicines11102813
APA StyleSekulovski, M., Mileva, N., Vasilev, G. V., Miteva, D., Gulinac, M., Peshevska-Sekulovska, M., Chervenkov, L., Batselova, H., Vasilev, G. H., Tomov, L., Lazova, S., Vassilev, D., & Velikova, T. (2023). Blood Coagulation and Thrombotic Disorders following SARS-CoV-2 Infection and COVID-19 Vaccination. Biomedicines, 11(10), 2813. https://doi.org/10.3390/biomedicines11102813