
The Microbiome and Metabolomic Profile of the Transplanted Intestine with Long-Term Function

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Patient Selection
- Long-term graft acceptance (Group A n = 23). Patients were at least five years beyond transplantation with normal intestinal allograft function, minimal immunosuppression requirement and no rejection episodes beyond the first 6 months after transplantation. These patients demonstrated normal histology on surveillance endoscopic biopsy.
- Short term graft acceptance (Group B n = 16). Patients within the first year after transplant with normal intestinal allograft function, restoration of intestinal continuity and no rejection episodes beyond the first six months. These patients demonstrated normal histology on surveillance endoscopic biopsy.
- Short term graft non-acceptance (Group C n = 4). Patients within the first year after transplantation demonstrated graft dysfunction resulting from an early rejection episode. In these patients, ongoing inflammatory changes and/or rejection were present on surveillance endoscopic biopsy of the allograft and were associated with the need for increased immunosuppression and resumption of parenteral nutritional or fluid supplementation.
2.2. Transplant Protocol
2.3. Post-Transplant Immunosuppression
2.4. Stool Sample Collection
2.5. Microbiome Analysis
2.6. Metabolite Extraction and Analysis
2.7. Clinical Outcomes
3. Results
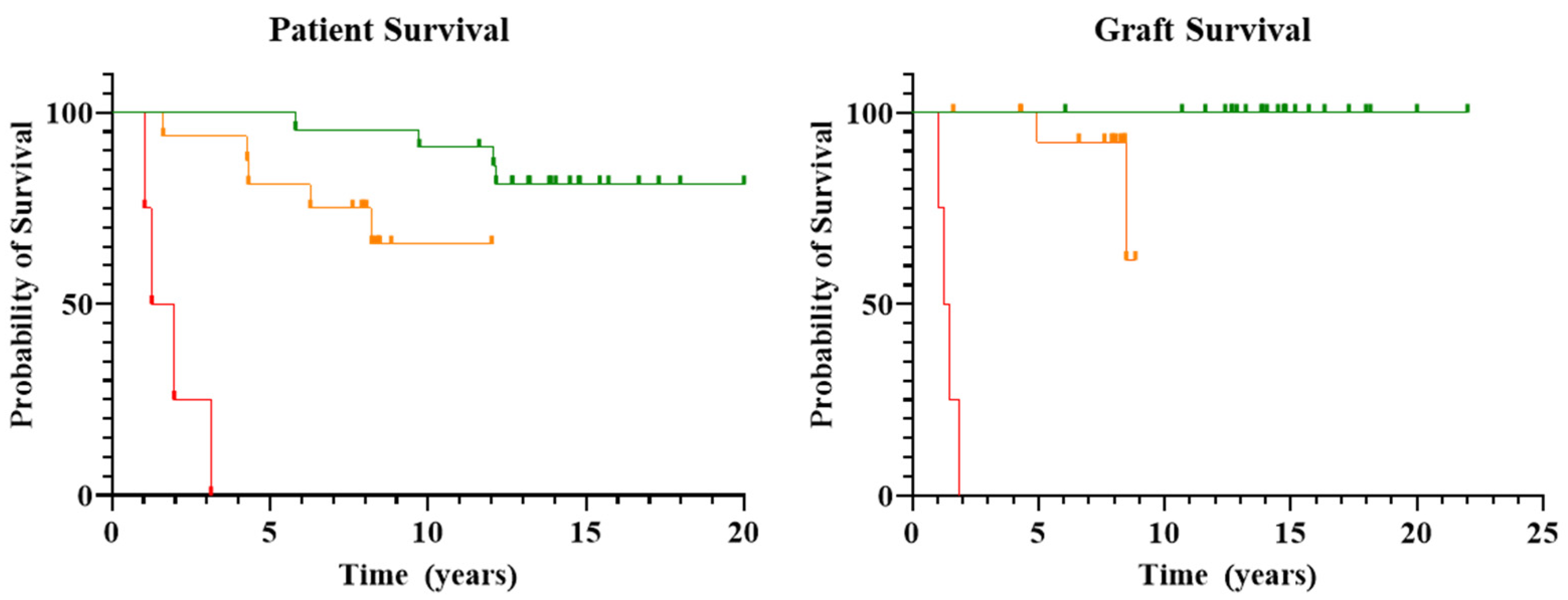
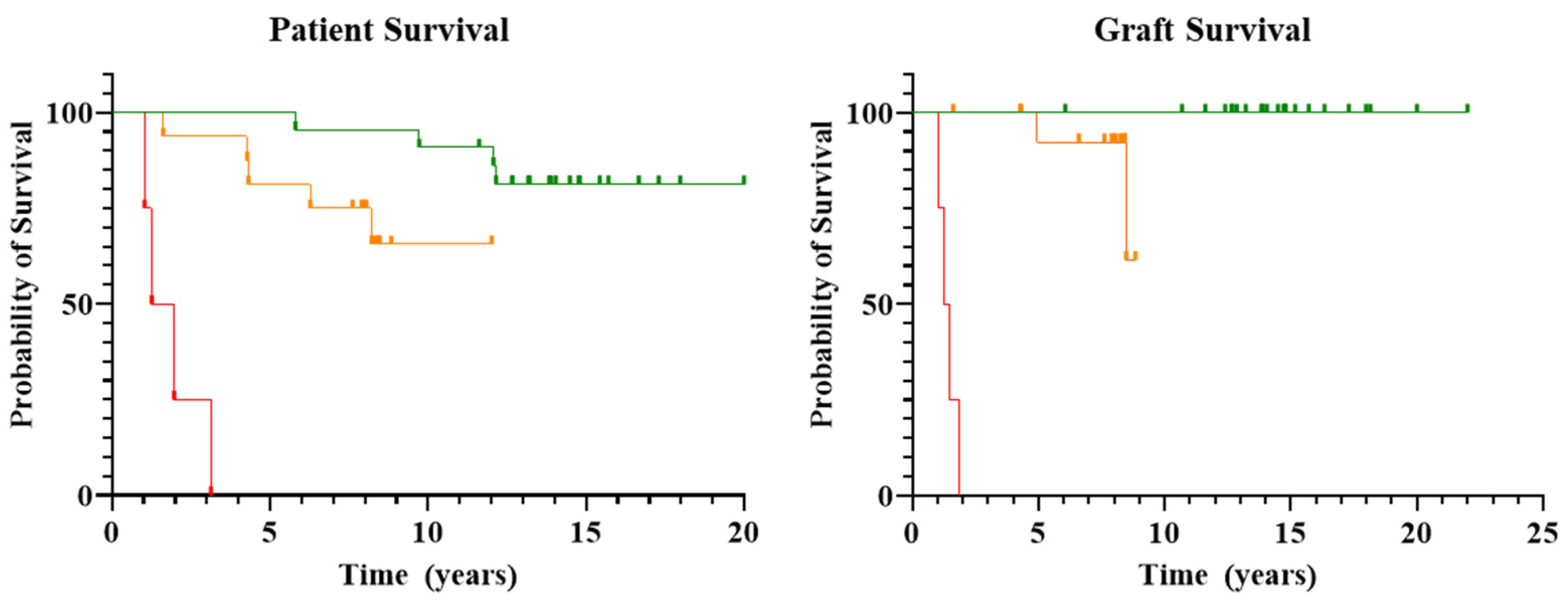
3.1. Patient and Graft Survival
3.2. Rejection Episodes and Systemic Infection
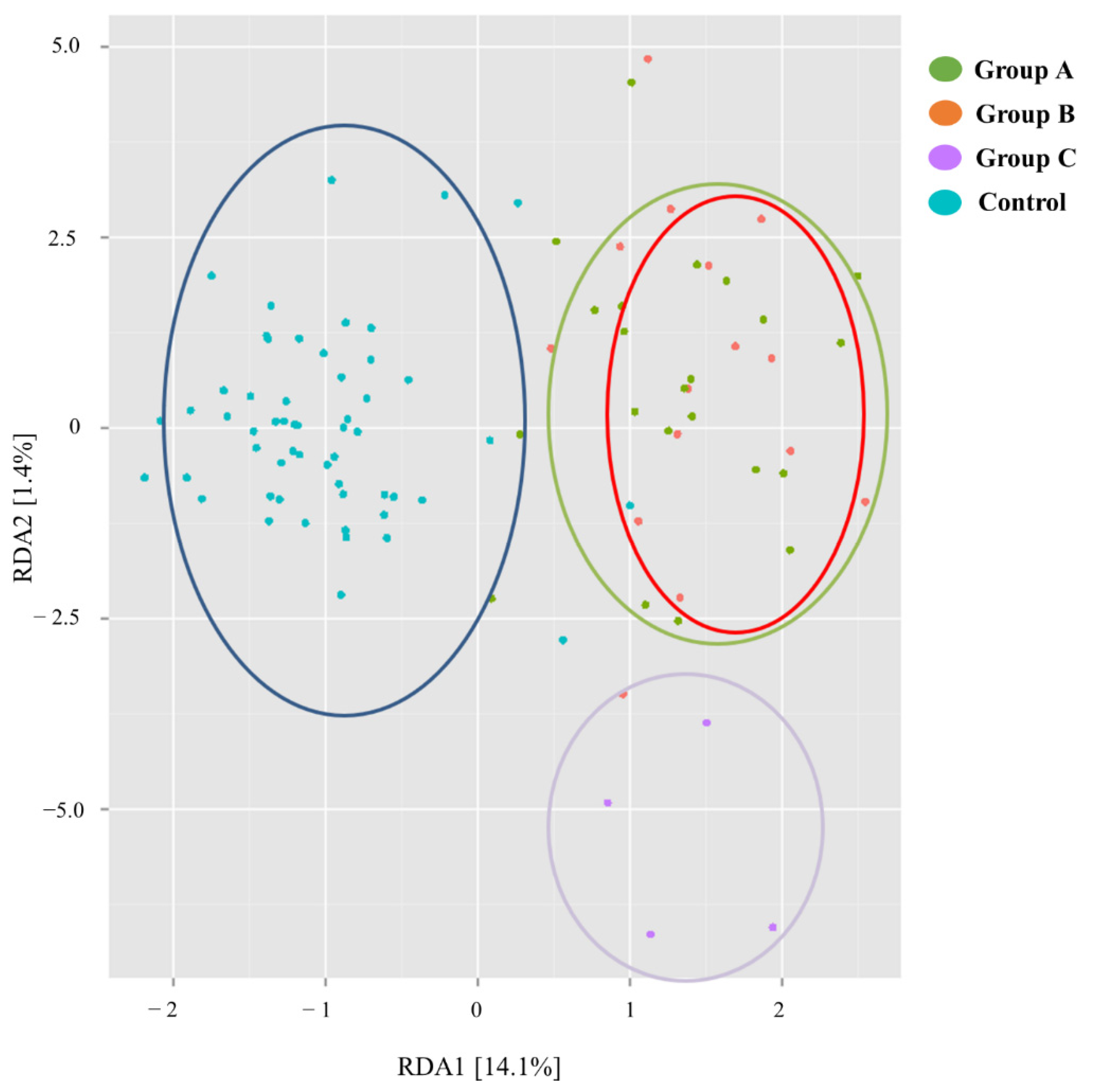
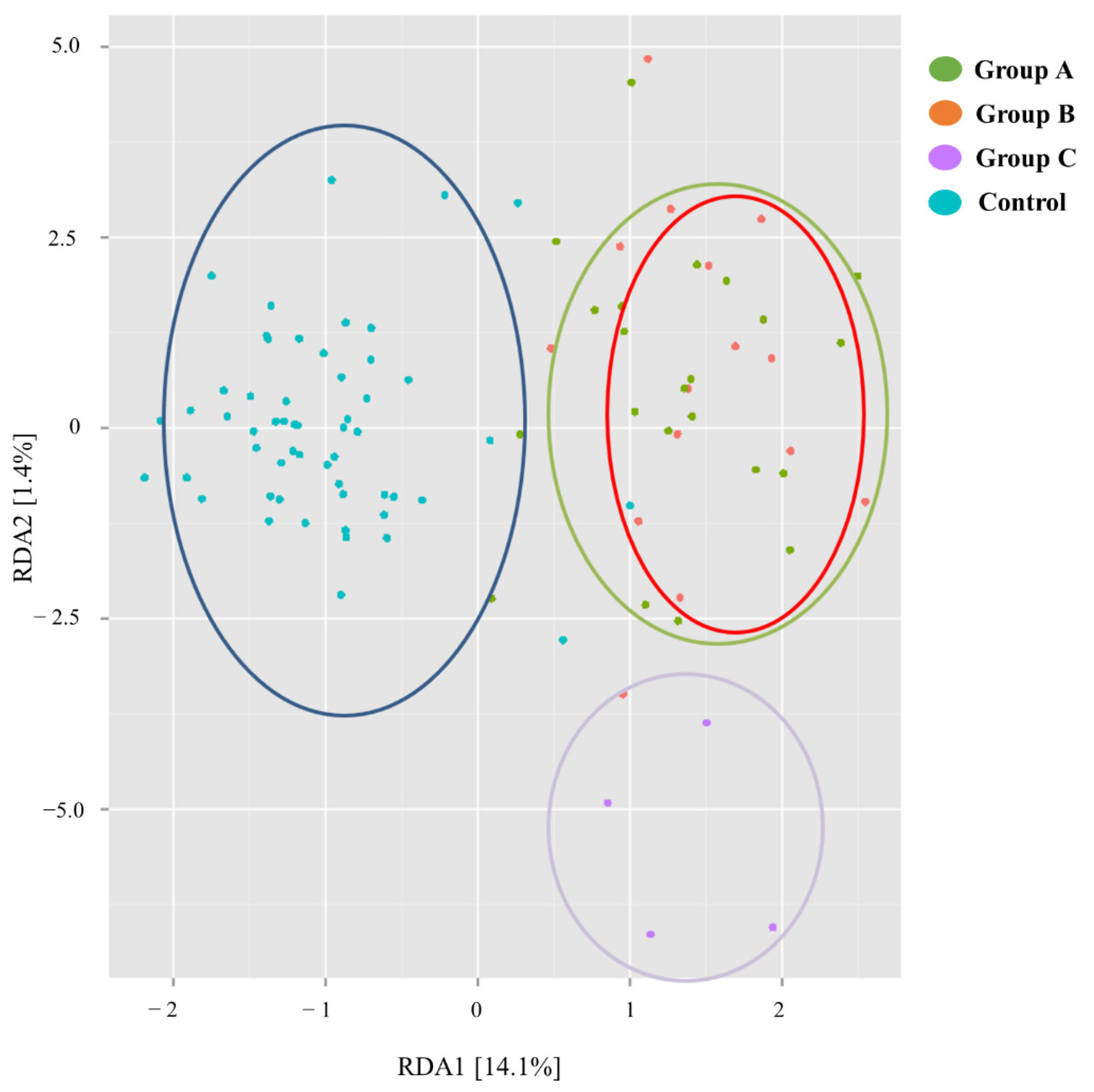
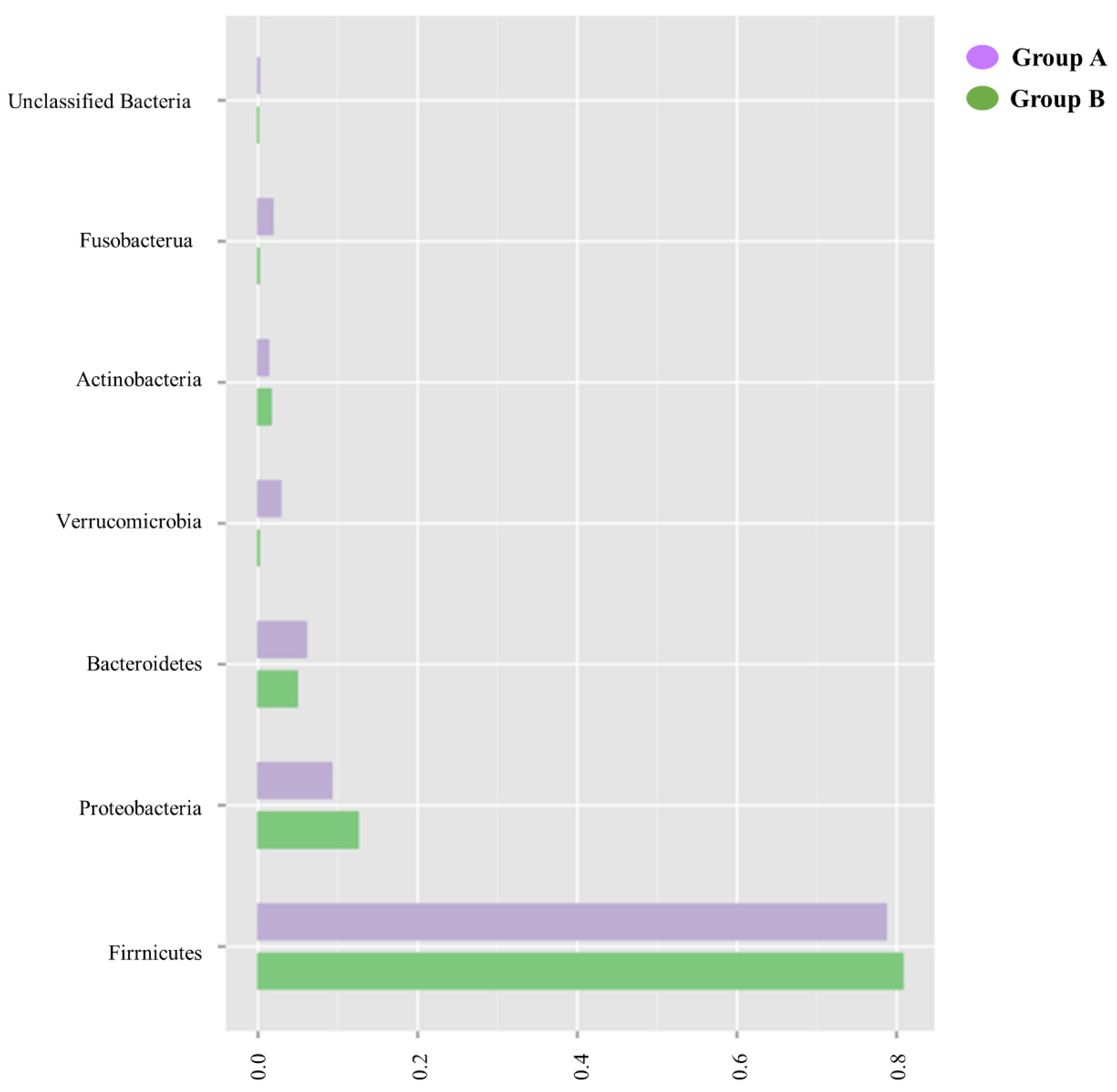
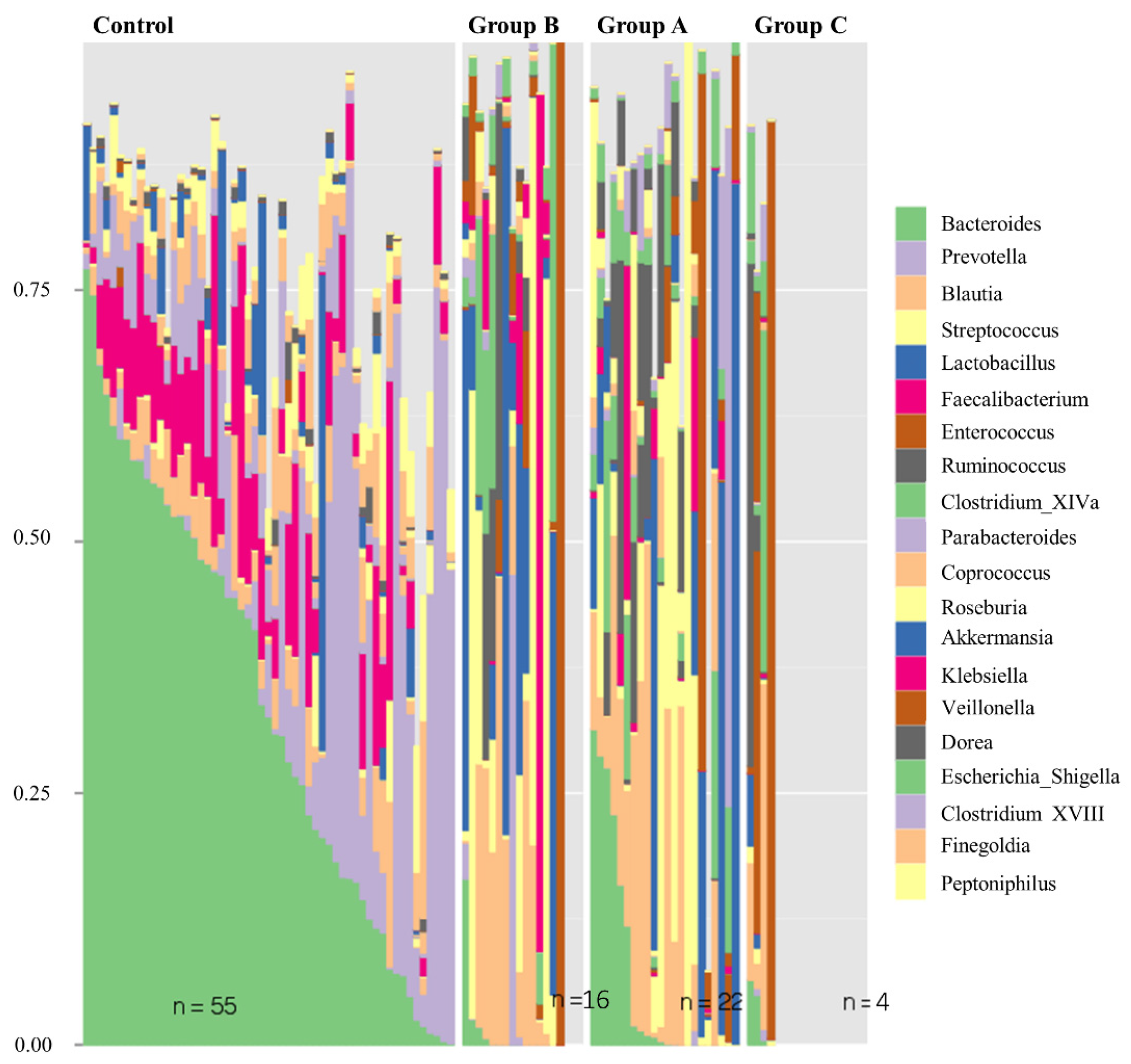
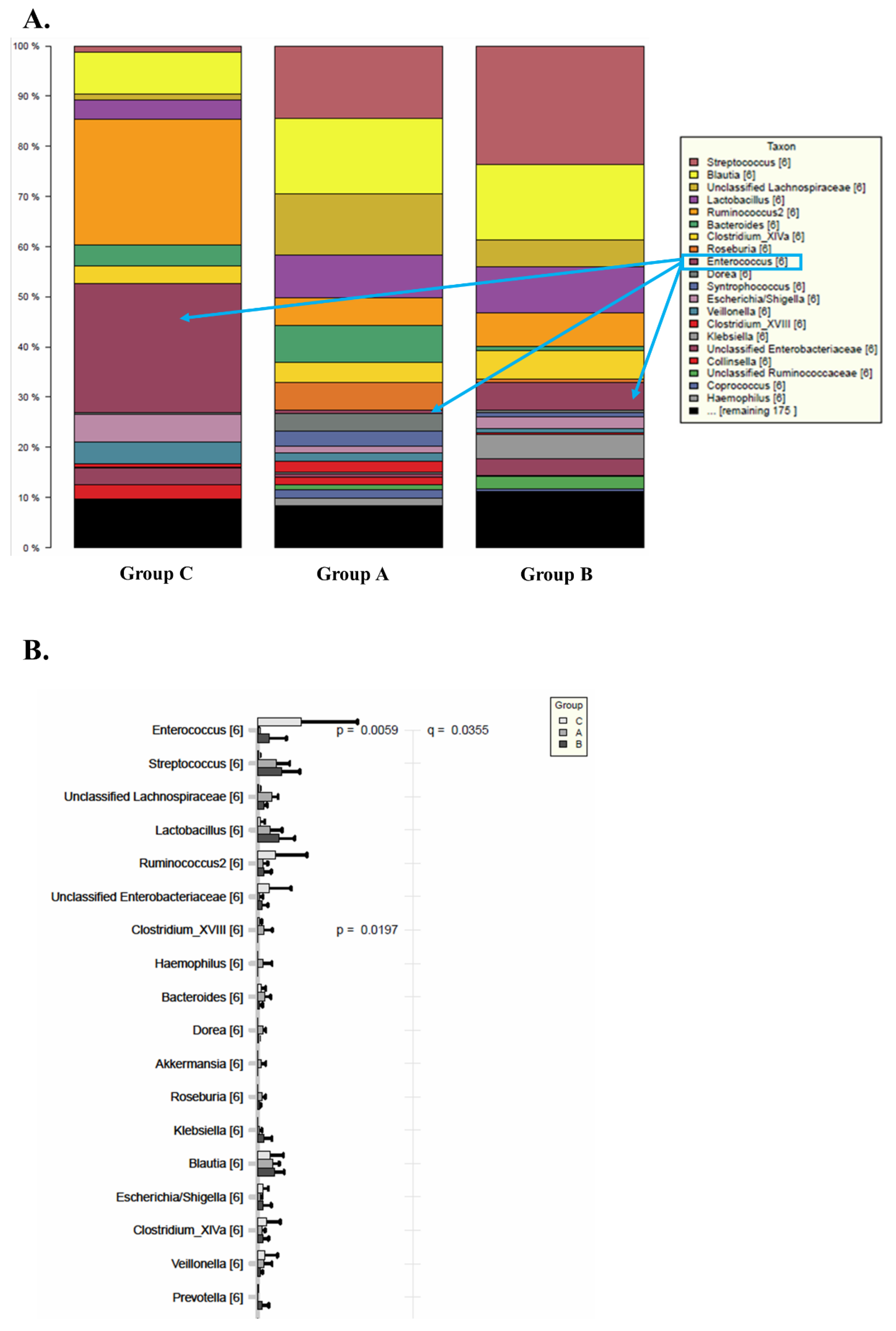
3.3. Fecal Microbiome
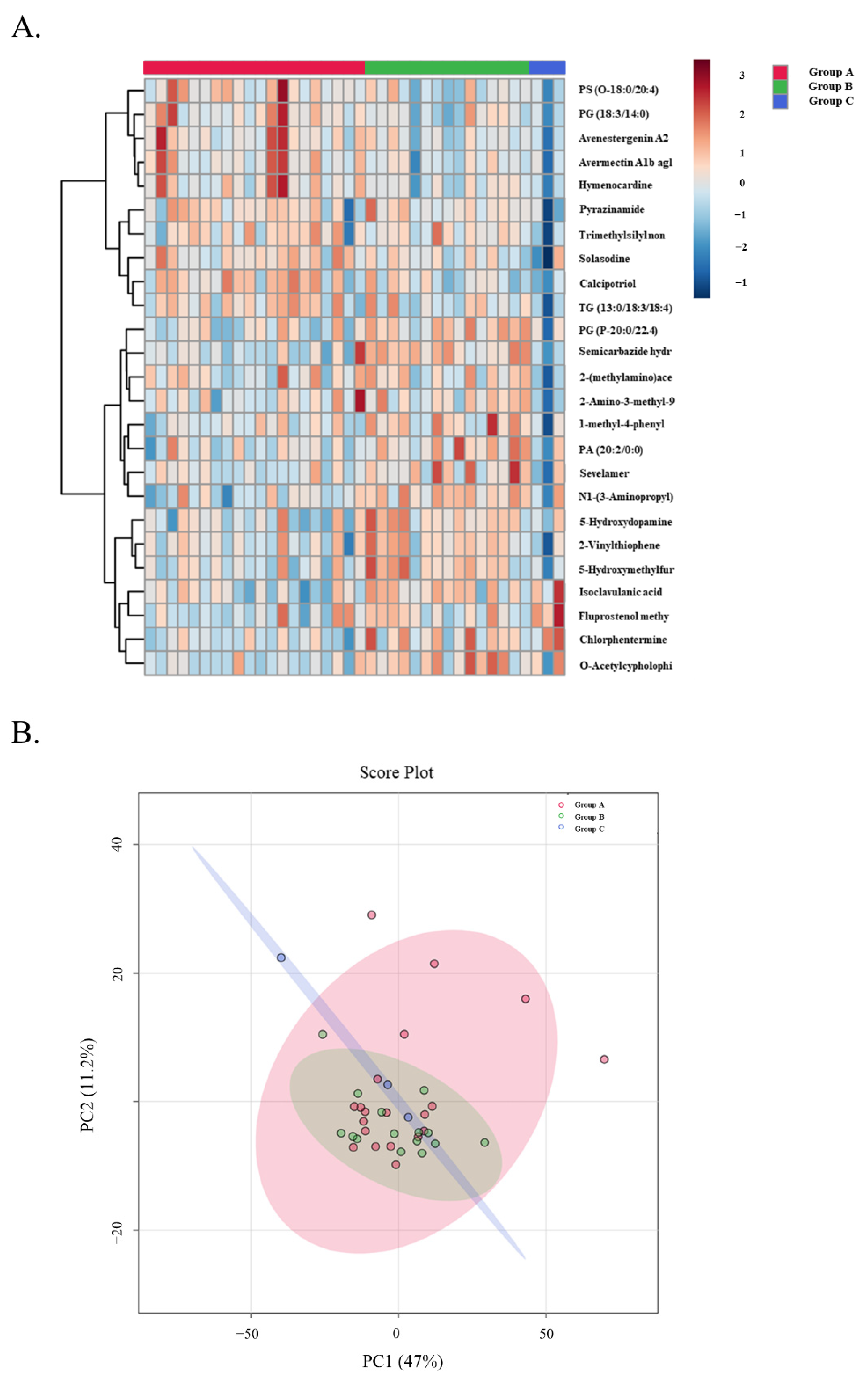
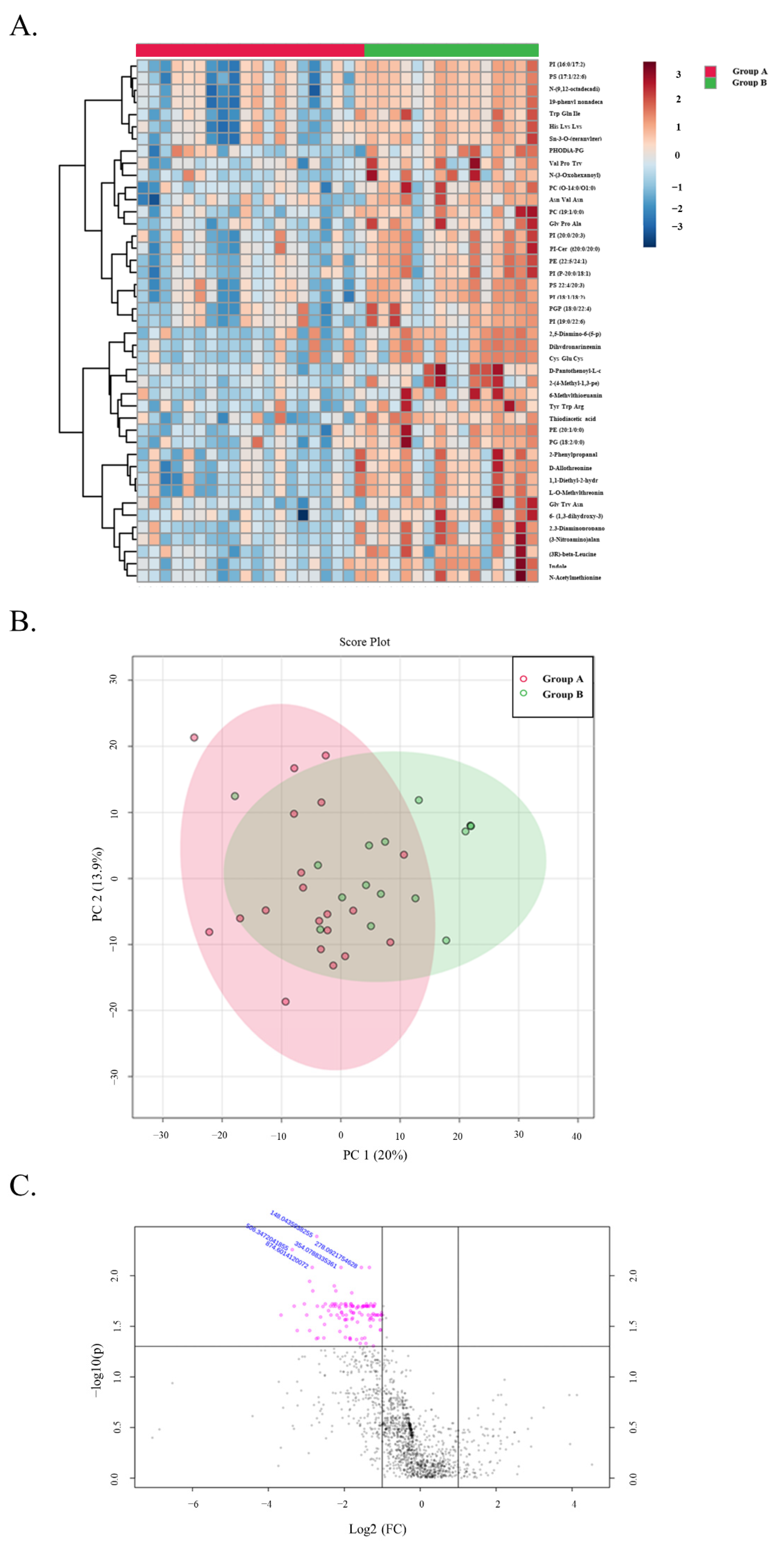
3.4. Metabolomic Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fishbein, T.M. Intestinal transplantation. N. Engl. J. Med. 2009, 361, 998–1008. [Google Scholar] [CrossRef]
- Garcia, J.; Selvaggi, G.; Tekin, A.; Vianna, R. Intestinal transplantation. Curr. Opin. Organ Transplant. 2021, 26, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Kroemer, A. Glimmers of hope for intestinal transplantation. Am. J. Transplant. 2020, 20, 2642–2643. [Google Scholar] [CrossRef]
- Abu-Elmagd, K.; Todo, S.; Tzakis, A.; Furukawa, H.; Bonet, H.; Mohamed, H.; Nour, B.; Reyes, J.; Green, M.; Manez, R.; et al. Intestinal transplantation and bacterial overgrowth in humans. Transplant. Proc. 1994, 26, 1684–1685. [Google Scholar]
- The NIH HMP Working Group; Peterson, J.; Garges, S.; Giovanni, M.; McInnes, P.; Wang, L.; Schloss, J.A.; Bonazzi, V.; McEwen, J.E.; Wetterstrand, K.A.; et al. The NIH Human Microbiome Project. Genome Res. 2009, 19, 2317–2323. [Google Scholar] [CrossRef]
- Gilbert, J.A.; Blaser, M.J.; Caporaso, J.G.; Jansson, J.K.; Lynch, S.V.; Knight, R. Current understanding of the human microbiome. Nat. Med. 2018, 24, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Hartman, A.L.; Lough, D.M.; Barupal, D.K.; Fiehn, O.; Fishbein, T.; Zasloff, M.; Eisen, J.A. Human gut microbiome adopts an alternative state following small bowel transplantation. Proc. Natl. Acad. Sci. USA 2009, 106, 17187–17192. [Google Scholar] [CrossRef] [PubMed]
- Girlanda, R.; Cheema, A.K.; Kaur, P.; Kwon, Y.; Li, A.; Guerra, J.; Matsumoto, C.S.; Zasloff, M.; Fishbein, T.M. Metabolomics of human intestinal transplant rejection. Am. J. Transplant. 2012, 12 (Suppl. 4), S18–S26. [Google Scholar] [CrossRef]
- Fishbein, T.; Novitskiy, G.; Mishra, L.; Matsumoto, C.; Kaufman, S.; Goyal, S.; Shetty, K.; Johnson, L.; Lu, A.; Wang, A.; et al. NOD2-expressing bone marrow-derived cells appear to regulate epithelial innate immunity of the transplanted human small intestine. Gut 2008, 57, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Kroemer, A.; Belyayev, L.; Khan, K.; Loh, K.; Kang, J.; Duttargi, A.; Dhani, H.; Sadat, M.; Aguirre, O.; Gusev, Y.; et al. Rejection of intestinal allotransplants is driven by memory T helper type 17 immunity and responds to infliximab. Am. J. Transplant. 2021, 21, 1238–1254. [Google Scholar] [CrossRef]
- Kroemer, A.; Cosentino, C.; Kaiser, J.; Matsumoto, C.S.; Fishbein, T.M. Intestinal Transplant Inflammation: The Third Inflammatory Bowel Disease. Curr. Gastroenterol. Rep. 2016, 18, 56. [Google Scholar] [CrossRef]
- Matsumoto, C.S.; Subramanian, S.; Fishbein, T.M. Adult Intestinal Transplantation. Gastroenterol. Clin. N. Am. 2018, 47, 341–354. [Google Scholar] [CrossRef]
- Matsumoto, C.S.; Kaufman, S.S.; Fishbein, T.M. Inclusion of the colon in intestinal transplantation. Curr. Opin. Organ Transplant. 2011, 16, 312–315. [Google Scholar] [CrossRef]
- Kaufman, S.S.; Hussan, E.; Kroemer, A.; Timofeeva, O.; Pasieka, H.B.; Guerra, J.F.; Yazigi, N.A.; Khan, K.M.; Ekong, U.D.; Subramanian, S.; et al. Graft Versus Host Disease After Intestinal Transplantation: A Single-center Experience. Transplant. Direct 2021, 7, e731. [Google Scholar] [CrossRef]
- Weiner, J.; Svetlicky, N.; Kang, J.; Sadat, M.; Khan, K.; Duttargi, A.; Stovroff, M.; Moturi, S.; Kara Balla, A.; Hyang Kwon, D.; et al. CD69+ resident memory T cells are associated with graft-versus-host disease in intestinal transplantation. Am. J. Transplant. 2021, 21, 1878–1892. [Google Scholar] [CrossRef]
- Rosas-Salazar, C.; Shilts, M.H.; Tovchigrechko, A.; Schobel, S.; Chappell, J.D.; Larkin, E.K.; Gebretsadik, T.; Halpin, R.A.; Nelson, K.E.; Moore, M.L.; et al. Nasopharyngeal Lactobacillus is associated with a reduced risk of childhood wheezing illnesses following acute respiratory syncytial virus infection in infancy. J. Allergy Clin. Immunol. 2018, 142, 1447–1456. [Google Scholar] [CrossRef]
- Rosas-Salazar, C.; Shilts, M.H.; Tovchigrechko, A.; Schobel, S.; Chappell, J.D.; Larkin, E.K.; Shankar, J.; Yooseph, S.; Nelson, K.E.; Halpin, R.A.; et al. Differences in the Nasopharyngeal Microbiome During Acute Respiratory Tract Infection with Human Rhinovirus and Respiratory Syncytial Virus in Infancy. J. Infect. Dis. 2016, 214, 1924–1928. [Google Scholar] [CrossRef]
- Shilts, M.H.; Rosas-Salazar, C.; Tovchigrechko, A.; Larkin, E.K.; Torralba, M.; Akopov, A.; Halpin, R.; Peebles, R.S.; Moore, M.L.; Anderson, L.J.; et al. Minimally Invasive Sampling Method Identifies Differences in Taxonomic Richness of Nasal Microbiomes in Young Infants Associated with Mode of Delivery. Microb. Ecol. 2016, 71, 233–242. [Google Scholar] [CrossRef]
- Rosas-Salazar, C.; Shilts, M.H.; Tovchigrechko, A.; Chappell, J.D.; Larkin, E.K.; Nelson, K.E.; Moore, M.L.; Anderson, L.J.; Das, S.R.; Hartert, T.V. Nasopharyngeal Microbiome in Respiratory Syncytial Virus Resembles Profile Associated with Increased Childhood Asthma Risk. Am. J. Respir. Crit. Care Med. 2016, 193, 1180–1183. [Google Scholar] [CrossRef]
- Eskind, C.C.; Shilts, M.H.; Shaver, C.M.; Das, S.R.; Satyanarayana, G. The respiratory microbiome after lung transplantation: Reflection or driver of respiratory disease? Am. J. Transplant. 2021, 21, 2333–2340. [Google Scholar] [CrossRef]
- Lee, J.R.; Muthukumar, T.; Dadhania, D.; Toussaint, N.C.; Ling, L.; Pamer, E.; Suthanthiran, M. Gut microbial community structure and complications after kidney transplantation: A pilot study. Transplantation 2014, 98, 697–705. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.R.; Magruder, M.; Zhang, L.; Westblade, L.F.; Satlin, M.J.; Robertson, A.; Edusei, E.; Crawford, C.; Ling, L.; Taur, Y.; et al. Gut microbiota dysbiosis and diarrhea in kidney transplant recipients. Am. J. Transplant. 2019, 19, 488–500. [Google Scholar] [CrossRef]
- Doycheva, I.; Leise, M.D.; Watt, K.D. The Intestinal Microbiome and the Liver Transplant Recipient: What We Know and What We Need to Know. Transplantation 2016, 100, 61–68. [Google Scholar] [CrossRef]
- Kriss, M.; Verna, E.C.; Rosen, H.R.; Lozupone, C.A. Functional Microbiomics in Liver Transplantation: Identifying Novel Targets for Improving Allograft Outcomes. Transplantation 2019, 103, 668–678. [Google Scholar] [CrossRef]
- Lu, H.F.; Ren, Z.G.; Li, A.; Zhang, H.; Xu, S.Y.; Jiang, J.W.; Zhou, L.; Ling, Q.; Wang, B.H.; Cui, G.Y.; et al. Fecal Microbiome Data Distinguish Liver Recipients with Normal and Abnormal Liver Function from Healthy Controls. Front. Microbiol. 2019, 10, 1518. [Google Scholar] [CrossRef]
- Oh, P.L.; Martinez, I.; Sun, Y.; Walter, J.; Peterson, D.A.; Mercer, D.F. Characterization of the ileal microbiota in rejecting and nonrejecting recipients of small bowel transplants. Am. J. Transplant. 2012, 12, 753–762. [Google Scholar] [CrossRef]
- Bartman, C.; Chong, A.S.; Alegre, M.L. The influence of the microbiota on the immune response to transplantation. Curr. Opin. Organ Transplant. 2015, 20, 1–7. [Google Scholar] [CrossRef]
- Nellore, A.; Fishman, J.A. The Microbiome, Systemic Immune Function, and Allotransplantation. Clin. Microbiol. Rev. 2016, 29, 191–199. [Google Scholar] [CrossRef]
- Zaza, G.; Dalla Gassa, A.; Felis, G.; Granata, S.; Torriani, S.; Lupo, A. Impact of maintenance immunosuppressive therapy on the fecal microbiome of renal transplant recipients: Comparison between an everolimus- and a standard tacrolimus-based regimen. PLoS ONE 2017, 12, e0178228. [Google Scholar] [CrossRef]
- Prideaux, L.; Kang, S.; Wagner, J.; Buckley, M.; Mahar, J.E.; De Cruz, P.; Wen, Z.; Chen, L.; Xia, B.; van Langenberg, D.R.; et al. Impact of ethnicity, geography, and disease on the microbiota in health and inflammatory bowel disease. Inflamm. Bowel Dis. 2013, 19, 2906–2918. [Google Scholar] [CrossRef]
- Peled, J.U.; Gomes, A.L.C.; Devlin, S.M.; Littmann, E.R.; Taur, Y.; Sung, A.D.; Weber, D.; Hashimoto, D.; Slingerland, A.E.; Slingerland, J.B.; et al. Microbiota as Predictor of Mortality in Allogeneic Hematopoietic-Cell Transplantation. N. Engl. J. Med. 2020, 382, 822–834. [Google Scholar] [CrossRef] [PubMed]
- Kusakabe, S.; Fukushima, K.; Yokota, T.; Hino, A.; Fujita, J.; Motooka, D.; Nakamura, S.; Shibayama, H.; Kanakura, Y. Enterococcus: A Predictor of Ravaged Microbiota and Poor Prognosis after Allogeneic Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2020, 26, 1028–1033. [Google Scholar] [CrossRef] [PubMed]
- Ubeda, C.; Taur, Y.; Jenq, R.R.; Equinda, M.J.; Son, T.; Samstein, M.; Viale, A.; Socci, N.D.; van den Brink, M.R.; Kamboj, M.; et al. Vancomycin-resistant Enterococcus domination of intestinal microbiota is enabled by antibiotic treatment in mice and precedes bloodstream invasion in humans. J. Clin. Investig. 2010, 120, 4332–4341. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A n = 23 | Group B n = 16 | Group C n = 4 | p-Value | |
|---|---|---|---|---|
| Age at Transplantation (years) | p = 0.611 | |||
| Adults | ||||
| Median (range) | 42 (19–66) | 47 (21–62) | 37 (24–53) | |
| Pediatric | ||||
| Median (range) | 2 (1–15) | 2 (1–3) | - | |
| Patient Sex [n (%)] | ||||
| Male | 15 (65%) | 8 (50%) | 1 (25%) | p = 0.275 |
| Female | 8 (35%) | 8 (50%) | 3 (75%) | p = 0.691 |
| Cause of Intestinal Failure [n (%)] | p = 0.286 | |||
| Short Gut Syndrome | 20 (87%) | 11 (69%) | 3 (75%) | |
| Gastroschisis | 1 (5%) | - | - | |
| Jejunal Atresia | 2 (10%) | - | - | |
| Mesenteric Thrombosis | 3 (14%) | 3 (27%) | 1 (33.3%) | |
| Necrotizing Enterocolitis | 2 (10%) | - | - | |
| Radiation Enteritis | - | - | 1 (33.3%) | |
| Surgical Complication | 5 (22%) | 5 (45%) | - | |
| Trauma | 2 (10%) | 1 (9%) | - | |
| Tumor | 1 (5%) | 1 (9%) | - | |
| Volvulus | 4 (19%) | 1 (9%) | 1 (33.3%) | |
| Dysmotility | 3 (13%) | 5 (31%) | 1 (25%) | |
| Hirsprung’s Disease | - | 1 (20%) | - | |
| Pseudo-obstruction | 3 (100%) | 4 (80%) | 1 (100%) | |
| Graft Type [n (%)] | ||||
| Small Intestine | 12 (52%) | 3 (20%) | 1 (25%) | p = 0.074 |
| Small Intestine + Colon | 3 (13%) | 7 (44%) | 3 (75%) * | p = 0.015 |
| Multivisceral Transplant ** | 8 (35%) | 4 (25%) | - | p = 0.340 |
| Modified Multvisceral Transplant *** | - | 2 (13%) | - | p = 0.170 |
| Group A [n (%)] n = 23 | Group B [n (%)] n = 16 | Group C [n (%)] n = 4 | p-Value | |
|---|---|---|---|---|
| Acute Rejection | 7 (30%) | 4 (25%) | 4 (100%) | p = 0.015 |
| Mild | 3 (43%) | 2 (50%) | 0 | |
| Moderate | 3 (43%) | 2 (50%) | 3 (75%) | |
| Severe | 1 (14%) | 0 | 1 (25%) | |
| Median time from transplant to rejection (days) | 20 | 21 | 164 | p = 0.122 |
| Bacteremia Episodes | ||||
| Enterococcus faecium | 0 | 0 | 1 (25%) | p = 0.007 |
| Vancomycin Resistant Enterococcus | 0 | 1 (6%) | 1 (25%) | p = 0.099 |
| Other | 2 (9%) | 8 (50%) | 3 (75%) | p = 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Girlanda, R.; Liggett, J.R.; Jayatilake, M.; Kroemer, A.; Guerra, J.F.; Hawksworth, J.S.; Radkani, P.; Matsumoto, C.S.; Zasloff, M.; Fishbein, T.M. The Microbiome and Metabolomic Profile of the Transplanted Intestine with Long-Term Function. Biomedicines 2022, 10, 2079. https://doi.org/10.3390/biomedicines10092079
Girlanda R, Liggett JR, Jayatilake M, Kroemer A, Guerra JF, Hawksworth JS, Radkani P, Matsumoto CS, Zasloff M, Fishbein TM. The Microbiome and Metabolomic Profile of the Transplanted Intestine with Long-Term Function. Biomedicines. 2022; 10(9):2079. https://doi.org/10.3390/biomedicines10092079
Chicago/Turabian StyleGirlanda, Raffaelle, Jedson R. Liggett, Meth Jayatilake, Alexander Kroemer, Juan Francisco Guerra, Jason Solomon Hawksworth, Pejman Radkani, Cal S. Matsumoto, Michael Zasloff, and Thomas M. Fishbein. 2022. "The Microbiome and Metabolomic Profile of the Transplanted Intestine with Long-Term Function" Biomedicines 10, no. 9: 2079. https://doi.org/10.3390/biomedicines10092079
APA StyleGirlanda, R., Liggett, J. R., Jayatilake, M., Kroemer, A., Guerra, J. F., Hawksworth, J. S., Radkani, P., Matsumoto, C. S., Zasloff, M., & Fishbein, T. M. (2022). The Microbiome and Metabolomic Profile of the Transplanted Intestine with Long-Term Function. Biomedicines, 10(9), 2079. https://doi.org/10.3390/biomedicines10092079