
Novel Biomarkers, Diagnostic and Therapeutic Approach in Rheumatoid Arthritis Interstitial Lung Disease—A Narrative Review


 ,
,
Abstract
1. Introduction
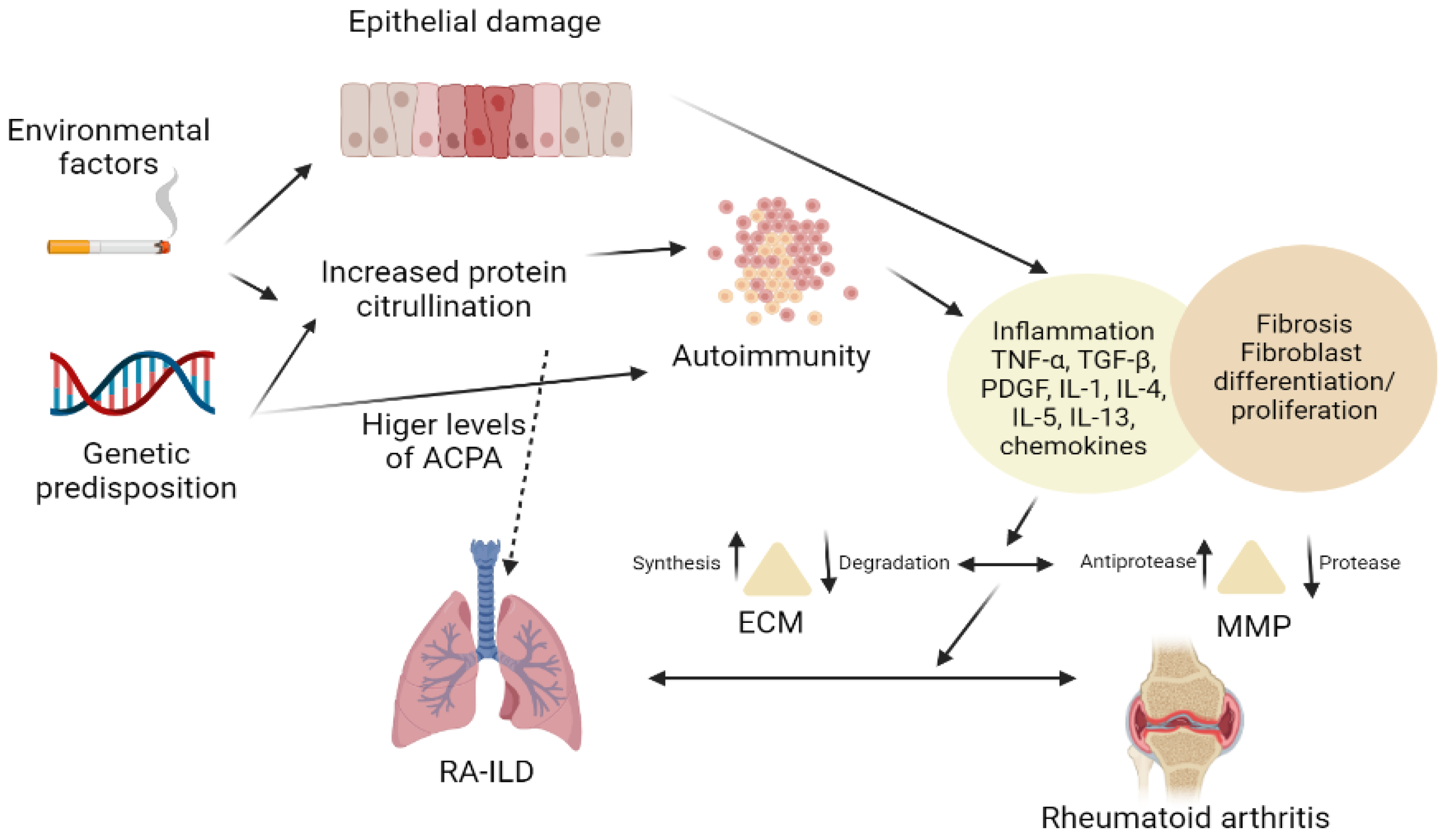
2. Pathogenesis
3. Biomarkers
3.1. Antibody Biomarkers
3.2. Genetic Biomarkers
3.3. Other Biomarkers
4. Similarities between RA-ILD and IPF
5. Diagnosis of RA-ILD
5.1. Clinical Presentation
5.2. Imaging
5.3. Phenotypes of RA-ILD
5.4. Pulmonary Function Tests
5.5. Bronchoalveolar Lavage
5.6. Histopathology
6. Treatment
6.1. Corticosteroids, Synthetic, Biological, and Targeted Therapy
6.2. Antifibrotic Therapy
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, S.; Kronzer, V.L.; Dellaripa, P.F.; Deane, K.D.; Bolster, M.B.; Nagaraja, V.; Khanna, D.; Doyle, T.J.; Sparks, J.A. Rheumatoid Arthritis–Associated Interstitial Lung Disease: Current Update on Prevalence, Risk Factors, and Pharmacologic Treatment. Curr. Treat. Options Rheumatol. 2020, 6, 337–353. [Google Scholar] [CrossRef] [PubMed]
- Marcucci, E.; Bartoloni, E.; Alunno, A.; Leone, M.C.; Cafaro, G.; Luccioli, F.; Valentini, V.; Valentini, E.; la Paglia, G.M.C.; Bonifacio, A.F.; et al. Extra-Articular Rheumatoid Arthritis. Reumatismo 2018, 70, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Marigliano, B.; Soriano, A.; Margiotta, D.; Vadacca, M.; Afeltra, A. Lung Involvement in Connective Tissue Diseases: A Comprehensive Review and a Focus on Rheumatoid Arthritis. Autoimmun. Rev. 2013, 12, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Cojocaru, M.; Cojocaru, I.M.; Silosi, I.; Vrabie, C.D.; Tanasescu, R. Extra-Articular Manifestations in Rheumatoid Arthritis. Maedica 2010, 5, 286. [Google Scholar] [CrossRef]
- Ha, Y.J.; Lee, Y.J.; Kang, E.H. Lung Involvements in Rheumatic Diseases: Update on the Epidemiology, Pathogenesis, Clinical Features, and Treatment. BioMed. Res. Int. 2018, 2018, 6930297. [Google Scholar] [CrossRef]
- Dai, Y.; Wang, W.; Yu, Y.; Hu, S. Rheumatoid Arthritis–Associated Interstitial Lung Disease: An Overview of Epidemiology, Pathogenesis and Management. Clin. Rheumatol. 2021, 40, 1211–1220. [Google Scholar] [CrossRef]
- Spagnolo, P.; Lee, J.S.; Sverzellati, N.; Rossi, G.; Cottin, V. The Lung in Rheumatoid Arthritis: Focus on Interstitial Lung Disease. Arthritis Rheumatol. 2018, 70, 1544–1554. [Google Scholar] [CrossRef]
- Azhar, M.; Muhammad, Q.; Halilu, F.; Woodford, M. Interstitial lung disease as the only manifestation of rheumatoid arthritis: Can lungs be the site of origin for rheumatoid arthritis-related inflammation? Chest 2021, 160, A2090. [Google Scholar] [CrossRef]
- Esposito, A.J.; Chu, S.G.; Madan, R.; Doyle, T.J.; Dellaripa, P.F. Thoracic Manifestations of Rheumatoid Arthritis. Clin. Chest Med. 2019, 40, 545–560. [Google Scholar] [CrossRef]
- Petrovská, N.; Prajzlerová, K.; Vencovský, J.; Šenolt, L.; Filková, M. The Pre-Clinical Phase of Rheumatoid Arthritis: From Risk Factors to Prevention of Arthritis. Autoimmun. Rev. 2021, 20, 102797. [Google Scholar] [CrossRef]
- Bongartz, T.; Cantaert, T.; Atkins, S.R.; Harle, P.; Myers, J.L.; Turesson, C.; Ryu, J.H.; Baeten, D.; Matteson, E.L. Citrullination in Extra-Articular Manifestations of Rheumatoid Arthritis. Rheumatology 2007, 46, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Darrah, E.; Andrade, F. Rheumatoid Arthritis and Citrullination. Curr. Opin. Rheumatol. 2018, 30, 72. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, A.; Luppi, F.; Cassone, G.; Vacchi, C.; Salvarani, C.; Sebastiani, M. Pathogenesis and Treatment of Idiopathic and Rheumatoid Arthritis-Related Interstitial Pneumonia. The Possible Lesson from COVID-19 Pneumonia. Expert Rev. Clin. Immunol. 2020, 16, 751–770. [Google Scholar] [CrossRef] [PubMed]
- Holers, V.M.; Demoruelle, M.K.; Kuhn, K.A.; Buckner, J.H.; Robinson, W.H.; Okamoto, Y.; Norris, J.M.; Deane, K.D. Rheumatoid Arthritis and the Mucosal Origins Hypothesis: Protection Turns to Destruction. Nat. Rev. Rheumatol. 2018, 14, 542–557. [Google Scholar] [CrossRef]
- Johnson, C. Recent Advances in the Pathogenesis, Prediction, and Management of Rheumatoid Arthritis-Associated Interstitial Lung Disease. Curr. Opin. Rheumatol. 2017, 29, 254–259. [Google Scholar] [CrossRef]
- Bendstrup, E.; Møller, J.; Kronborg-White, S.; Prior, T.S.; Hyldgaard, C. Interstitial Lung Disease in Rheumatoid Arthritis Remains a Challenge for Clinicians. J. Clin. Med. 2019, 8, 2038. [Google Scholar] [CrossRef]
- Khan, T.; Jose, R.J.; Renzoni, E.A.; Mouyis, M. A Closer Look at the Role of Anti-CCP Antibodies in the Pathogenesis of Rheumatoid Arthritis-Associated Interstitial Lung Disease and Bronchiectasis. Rheumatol. Ther. 2021, 8, 21. [Google Scholar]
- McDermott, G.C.; Doyle, T.J.; Sparks, J.A. Interstitial Lung Disease throughout the Rheumatoid Arthritis Disease Course. Curr. Opin. Rheumatol. 2021, 33, 284–291. [Google Scholar] [CrossRef]
- Pruijn, G.J.M. Citrullination and Carbamylation in the Pathophysiology of Rheumatoid Arthritis. Front. Immunol. 2015, 6, 192. [Google Scholar] [CrossRef]
- Cavagna, L.; Monti, S.; Grosso, V.; Boffini, N.; Scorletti, E.; Crepaldi, G.; Caporali, R. The Multifaceted Aspects of Interstitial Lung Disease in Rheumatoid Arthritis. BioMed Res. Int. 2013, 2013, 13. [Google Scholar] [CrossRef]
- Mizutani, S.; Nishio, J.; Kondo, K.; Motomura, K.; Yamada, Z.; Masuoka, S.; Yamada, S.; Muraoka, S.; Ishii, N.; Kuboi, Y.; et al. Treatment with an Anti-Cx3cl1 Antibody Suppresses M1 Macrophage Infiltration in Interstitial Lung Disease in Skg Mice. Pharmaceuticals 2021, 14, 474. [Google Scholar] [CrossRef] [PubMed]
- Kadura, S.; Raghu, G. Rheumatoid Arthritis-Interstitial Lung Disease: Manifestations and Current Concepts in Pathogenesis and Management. Eur. Respir. Rev. 2021, 30, 210011. [Google Scholar] [CrossRef] [PubMed]
- Kuwana, M.; Gil-Vila, A.; Selva-O’Callaghan, A. Role of Autoantibodies in the Diagnosis and Prognosis of Interstitial Lung Disease in Autoimmune Rheumatic Disorders. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X211032457. [Google Scholar] [CrossRef]
- Furukawa, H.; Oka, E.; Toma, S. Biomarkers for Rheumatoid Arthritis Associated Lung Disease. Clin. Rheumatol. Relat. Res. 2020, 32, 318–322. [Google Scholar] [CrossRef]
- Lucchino, B.; di Paolo, M.; Gioia, C.; Vomero, M.; Diacinti, D.; Mollica, C.; Alessandri, C.; Diacinti, D.; Palange, P.; di Franco, M. Identification of Subclinical Lung Involvement in ACPA-Positive Subjects through Functional Assessment and Serum Biomarkers. Int. J. Mol. Sci. 2020, 21, 5162. [Google Scholar] [CrossRef] [PubMed]
- Solomon, J.J.; Matson, S.; Kelmenson, L.B.; Chung, J.H.; Hobbs, S.B.; Rosas, I.O.; Dellaripa, P.F.; Doyle, T.J.; Poli, S.; Esposito, A.J.; et al. IgA Antibodies Directed Against Citrullinated Protein Antigens Are Elevated in Patients with Idiopathic Pulmonary Fibrosis. Chest 2020, 157, 1513–1521. [Google Scholar] [CrossRef] [PubMed]
- Tanguy, J.; Pommerolle, L.; Garrido, C.; Kolb, M.; Bonniaud, P.; Goirand, F.; Bellaye, P.S. Extracellular Heat Shock Proteins as Therapeutic Targets and Biomarkers in Fibrosing Interstitial Lung Diseases. Int. J. Mol. Sci. 2021, 22, 9316. [Google Scholar] [CrossRef] [PubMed]
- Samara, K.D.; Trachalaki, A.; Tsitoura, E.; Koutsopoulos, A.V.; Lagoudaki, E.D.; Lasithiotaki, I.; Margaritopoulos, G.; Pantelidis, P.; Bibaki, E.; Siafakas, N.M.; et al. Upregulation of Citrullination Pathway: From Autoimmune to Idiopathic Lung Fibrosis. Respir. Res. 2017, 18, 218. [Google Scholar] [CrossRef]
- Mohamed, A.; Enein, A.; Abdelsalam, N.; Balata, M.; Abdellatif, S.; Rizk, E.; Fathy, A. Utility of Anti-Carbamylated Protein Antibodies in the Diagnosis of Early Rheumatoid Arthritis. Indian J. Rheumatol. 2019, 14, 37. [Google Scholar] [CrossRef]
- Nakabo, S. Clinical and Etiological Meaning of Anti-Carbamylated Protein Antibodies in Rheumatoid Arthritis. Immunol. Med. 2018, 41, 147–153. [Google Scholar] [CrossRef]
- Wu, C.Y.; Yang, H.Y.; Luo, S.F.; Lai, J.H. From Rheumatoid Factor to Anti-Citrullinated Protein Antibodies and Anti-Carbamylated Protein Antibodies for Diagnosis and Prognosis Prediction in Patients with Rheumatoid Arthritis. Int. J. Mol. Sci. 2021, 22, 686. [Google Scholar] [CrossRef] [PubMed]
- Mikuls, T.R.; Edison, J.; Meeshaw, E.; Sayles, H.; England, B.R.; Duryee, M.J.; Hunter, C.D.; Kelmenson, L.B.; Kay Moss, L.; Feser, M.L.; et al. Autoantibodies to Malondialdehyde–Acetaldehyde Are Detected Prior to Rheumatoid Arthritis Diagnosis and After Other Disease Specific Autoantibodies. Arthritis Rheumatol. 2020, 72, 2025–2029. [Google Scholar] [CrossRef] [PubMed]
- Thiele, G.M.; Duryee, M.J.; Anderson, D.R.; Klassen, L.W.; Mohring, S.M.; Young, K.A.; Benissan-Messan, D.; Sayles, H.; Dusad, A.; Hunter, C.D.; et al. Malondialdehyde-Acetaldehyde Adducts and Anti-Malondialdehyde-Acetaldehyde Antibodies in Rheumatoid Arthritis. Arthritis Rheumatol. 2015, 67, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Brito, Y.; Glassberg, M.K.; Ascherman, D.P. Rheumatoid Arthritis-Associated Interstitial Lung Disease: Current Concepts. Curr. Rheumatol. Rep. 2017, 19, 79. [Google Scholar] [CrossRef]
- Furukawa, H.; Oka, S.; Higuchi, T.; Shimada, K.; Hashimoto, A.; Matsui, T.; Tohma, S. Biomarkers for Interstitial Lung Disease and Acute-Onset Diffuse Interstitial Lung Disease in Rheumatoid Arthritis. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1–12. [Google Scholar] [CrossRef]
- Oliveira, R.P.; Ribeiro, R.; Melo, L.; Grima, B.; Oliveira, S.; Alves, J.D. Connective Tissue Disease-Associated Interstitial Lung Disease. Pulmonology 2020, 28, 113–118. [Google Scholar] [CrossRef]
- Saad, M.N.; Mabrouk, M.S.; Eldeib, A.M.; Shaker, O.G. Identification of Rheumatoid Arthritis Biomarkers Based on Single Nucleotide Polymorphisms and Haplotype Blocks: A Systematic Review and Meta-Analysis. J. Adv. Res. 2016, 7, 1–16. [Google Scholar] [CrossRef]
- Deane, K.D.; Demoruelle, M.K.; Kelmenson, L.B.; Kuhn, K.A.; Norris, J.M.; Holers, V.M. Genetic and Environmental Risk Factors for Rheumatoid Arthritis. Best Pract. Res. Clin. Rheumatol. 2017, 31, 3–18. [Google Scholar] [CrossRef]
- Shirai, Y.; Honda, S.; Ikari, K.; Kanai, M.; Takeda, Y.; Kamatani, Y.; Morisaki, T.; Tanaka, E.; Kumanogoh, A.; Harigai, M.; et al. Association of the RPA3-UMAD1 Locus with Interstitial Lung Diseases Complicated with Rheumatoid Arthritis in Japanese. Ann. Rheum. Dis. 2020, 79, 1305–1309. [Google Scholar] [CrossRef]
- Jönsson, E.; Ljung, L.; Norrman, E.; Freyhult, E.; Lisbeth, L.; Dahlqvist, J.; Rantapää-Dahlqvist, S. Pulmonary Fibrosis in Relation to Genetic Loci in an Inception Cohort of Patients with Early Rheumatoid Arthritis from Northern Sweden. Rheumatology 2022, 61, 943–952. [Google Scholar] [CrossRef]
- Chen, J.; Doyle, T.J.; Liu, Y.; Aggarwal, R.; Wang, X.; Shi, Y.; Ge, S.X.; Huang, H.; Lin, Q.; Liu, W.; et al. Biomarkers of Rheumatoid Arthritis-Associated Interstitial Lung Disease. Arthritis Rheumatol. 2015, 67, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Moran-Moguel, M.C.; del Rio, S.P.; Mayorquin-Galvan, E.E.; Zavala-Cerna, M.G. Rheumatoid Arthritis and MiRNAs: A Critical Review through a Functional View. J. Immunol. Res. 2018, 2018, 2474529. [Google Scholar] [CrossRef] [PubMed]
- Konigsberg, I.R.; Borie, R.; Walts, A.D.; Cardwell, J.; Rojas, M.; Metzger, F.; Hauck, S.M.; Fingerlin, T.E.; Yang, I.V.; Schwartz, D.A. Molecular Signatures of Idiopathic Pulmonary Fibrosis. Am. J. Respir. Cell Mol. Biol. 2021, 65, 430–441. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Lee, E.Y.; Ha, Y.J.; Kang, E.H.; Lee, Y.J.; Song, Y.W. Serum Kl-6 Levels Reflect the Severity of Interstitial Lung Disease Associated with Connective Tissue Disease. Arthritis Res. Ther. 2019, 21, 58. [Google Scholar] [CrossRef]
- Amigues, I.; Ramadurai, D.; Swigris, J.J. Current Perspectives on Emerging Biomarkers for Rheumatoid Arthritis-Associated Interstitial Lung Disease. Open Access Rheumatol. Res. Rev. 2019, 11, 229. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, S.; Zheng, S.; Lin, J.; Hu, S.; Zhuang, J.; Lin, Q.; Xie, X.; Zheng, K.; Zhang, W.; et al. The Role of Lung Ultrasound B-Lines and Serum KL-6 in the Screening and Follow-up of Rheumatoid Arthritis Patients for an Identification of Interstitial Lung Disease: Review of the Literature, Proposal for a Preliminary Algorithm, and Clinical Application to Cases. Arthritis Res. Ther. 2021, 23, 212. [Google Scholar] [CrossRef]
- Ma, H.; Lu, J.; Song, Y.; Wang, H.; Yin, S. The Value of Serum Krebs von Den Lungen-6 as a Diagnostic Marker in Connective Tissue Disease Associated with Interstitial Lung Disease. BMC Pulm. Med. 2020, 20, 6. [Google Scholar] [CrossRef]
- Oguz, E.O.; Kucuksahin, O.; Turgay, M.; Yildizgoren, M.T.; Ates, A.; Demir, N.; Kumbasar, O.O.; Kinikli, G.; Duzgun, N. Association of Serum KL-6 Levels with Interstitial Lung Disease in Patients with Connective Tissue Disease: A Cross-Sectional Study. Clin. Rheumatol. 2016, 35, 663–666. [Google Scholar] [CrossRef]
- Doyle, T.J.; Patel, A.S.; Hatabu, H.; Nishino, M.; Wu, G.; Osorio, J.C.; Golzarri, M.F.; Traslosheros, A.; Chu, S.G.; Frits, M.L.; et al. Detection of Rheumatoid Arthritis-Interstitial Lung Disease Is Enhanced by Serum Biomarkers. Am. J. Respir. Crit. Care Med. 2015, 191, 1403–1412. [Google Scholar] [CrossRef]
- Mohan, C.; Assassi, S. Biomarkers in Rheumatic Diseases: How Can They Facilitate Diagnosis and Assessment of Disease Activity? BMJ 2015, 351, h5079. [Google Scholar] [CrossRef]
- Chen, Z.; Bozec, A.; Ramming, A.; Schett, G. Anti-Inflammatory and Immune-Regulatory Cytokines in Rheumatoid Arthritis. Nat. Rev. Rheumatol. 2019, 15, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Kass, D.J.; Nouraie, M.; Glassberg, M.K.; Ramreddy, N.; Fernandez, K.; Harlow, L.; Zhang, Y.; Chen, J.; Kerr, G.S.; Reimold, A.M.; et al. Comparative Profiling of Serum Protein Biomarkers in Rheumatoid Arthritis–Associated Interstitial Lung Disease and Idiopathic Pulmonary Fibrosis. Arthritis Rheumatol. 2020, 72, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Mahalanobish, S.; Saha, S.; Dutta, S.; Sil, P.C. Matrix Metalloproteinase: An Upcoming Therapeutic Approach for Idiopathic Pulmonary Fibrosis. Pharmacol. Res. 2020, 152, 104591. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Zhou, Y.; Chen, X.; Li, J. A Metaanalysis of the Increased Risk of Rheumatoid Arthritis-Related Pulmonary Disease as a Result of Serum Anticitrullinated Protein Antibody Positivity. J. Rheumatol. 2014, 41, 1282–1289. [Google Scholar] [CrossRef]
- Harlow, L.; Rosas, I.O.; Gochuico, B.R.; Mikuls, T.R.; Dellaripa, P.F.; Oddis, C.V.; Ascherman, D.P. Identification of Citrullinated Hsp90 Isoforms as Novel Autoantigens in Rheumatoid Arthritis-Associated Interstitial Lung Disease. Arthritis Rheum. 2013, 65, 869–879. [Google Scholar] [CrossRef]
- Giles, J.T.; Darrah, E.; Danoff, S.; Johnson, C.; Andrade, F.; Rosen, A.; Bathon, J.M. Association of Cross-Reactive Antibodies Targeting Peptidyl-Arginine Deiminase 3 and 4 with Rheumatoid Arthritis-Associated Interstitial Lung Disease. PLoS ONE 2014, 9, e98794. [Google Scholar] [CrossRef]
- Mori, S.; Koga, Y.; Sugimoto, M. Different Risk Factors between Interstitial Lung Disease and Airway Disease in Rheumatoid Arthritis. Respir. Med. 2012, 106, 1591–1599. [Google Scholar] [CrossRef]
- Li, H.; Li, L.; Liu, C.; Cheng, L.; Yan, S.; Chen, H.; Li, Y. Diagnostic Value of Anti-citrullinated A-enolase Peptide 1 Antibody in Patients with Rheumatoid Arthritis: A Systematic Review and Meta-analysis. Int. J. Rheum. Dis. 2021, 24, 633. [Google Scholar] [CrossRef]
- Castellanos-Moreira, R.; Rodríguez-García, S.C.; Gomara, M.J.; Ruiz-Esquide, V.; Cuervo, A.; Casafont-Solé, I.; Ramírez, J.; Holgado, S.; Gómez-Puerta, J.A.; Cañete, J.D.; et al. Anti-Carbamylated Proteins Antibody Repertoire in Rheumatoid Arthritis: Evidence of a New Autoantibody Linked to Interstitial Lung Disease. Ann. Rheum. Dis. 2020, 79, 587–594. [Google Scholar] [CrossRef]
- England, B.R.; Duryee, M.J.; Roul, P.; Mahajan, T.D.; Singh, N.; Poole, J.A.; Ascherman, D.P.; Caplan, L.; Demoruelle, M.K.; Deane, K.D.; et al. Malondialdehyde-Acetaldehyde Adducts and Antibody Responses in Rheumatoid Arthritis-Associated Interstitial Lung Disease. Arthritis Rheumatol. 2019, 71, 1483–1493. [Google Scholar] [CrossRef]
- Peljto, A.L.; Zhang, Y.; Fingerlin, T.E.; Shwu-Fan, M.; Garcia, J.G.N.; Richards, T.J.; Silveira, L.J.; Lindell, K.O.; Steele, M.P.; Loyd, J.E.; et al. Association between the MUC5B Promoter Polymorphism and Survival in Patients with Idiopathic Pulmonary Fibrosis. JAMA 2013, 309, 2232–2239. [Google Scholar] [CrossRef] [PubMed]
- Juge, P.A.; Borie, R.; Kannengiesser, C.; Gazal, S.; Revy, P.; Wemeau-Stervinou, L.; Debray, M.P.; Ottaviani, S.; Marchand-Adam, S.; Nathan, N.; et al. Shared Genetic Predisposition in Rheumatoid Arthritis-Interstitial Lung Disease and Familial Pulmonary Fibrosis. Eur. Respir. J. 2017, 49, 1602314. [Google Scholar] [CrossRef] [PubMed]
- Oka, S.; Furukawa, H.; Shimada, K.; Hashimoto, A.; Komiya, A.; Fukui, N.; Tsuchiya, N.; Tohma, S. Plasma MiRNA Expression Profiles in Rheumatoid Arthritis Associated Interstitial Lung Disease. BMC Musculoskelet. Disord. 2017, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Migita, K.; Nakamura, T.; Koga, T.; Eguchi, K. HLA-DRB1 Alleles and Rheumatoid Arthritis-Related Pulmonary Fibrosis. J. Rheumatol. 2010, 37, 205–207. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Deng, K.; Fan, Q.; Yang, Y.; Deng, X.; He, R.; Tan, Y.; Lan, Y.; Deng, X.; Pan, Y.; Wang, Y.; et al. Prognostic Roles of KL-6 in Disease Severity and Lung Injury in COVID-19 Patients: A Longitudinal Retrospective Analysis. J. Med. Virol. 2021, 93, 2505–2512. [Google Scholar] [CrossRef] [PubMed]
- Ko, U.W.; Cho, E.J.; Oh, H.B.; Koo, H.J.; Do, K.H.; Song, J.W. Serum Krebs von Den Lungen-6 Level Predicts Disease Progression in Interstitial Lung Disease. PLoS ONE 2020, 15, e0244114. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Xu, L.; Cheng, Q.; Nie, L.; Zhang, S.; Du, Y.; Xue, J. Increased Serum Soluble Programmed Death Ligand 1(SPD-L1) Is Associated with the Presence of Interstitial Lung Disease in Rheumatoid Arthritis: A Monocentric Cross-Sectional Study. Respir. Med. 2020, 166, 105948. [Google Scholar] [CrossRef]
- Matsuo, T.; Hashimoto, M.; Ito, I.; Kubo, T.; Uozumi, R.; Furu, M.; Ito, H.; Fujii, T.; Tanaka, M.; Terao, C.; et al. Interleukin-18 Is Associated with the Presence of Interstitial Lung Disease in Rheumatoid Arthritis: A Cross-Sectional Study. Scand. J. Rheumatol. 2019, 48, 87–94. [Google Scholar] [CrossRef]
- Hussein, M.S.; El-Barbary, A.M.; Nada, D.W.; Gaber, R.A.; Elkolaly, R.M.; Aboelhawa, M.A. Identification of Serum Interleukin-13 and Interleukin-13 Receptor Subunit Expressions: Rheumatoid Arthritis–Associated Interstitial Lung Disease. Int. J. Rheum. Dis. 2021, 24, 591–598. [Google Scholar] [CrossRef]
- Ohnishi, H.; Yokoyama, A.; Kondo, K.; Hamada, H.; Abe, M.; Nishimura, K.; Hiwada, K.; Kohno, N. Comparative Study of KL-6, Surfactant Protein-A, Surfactant Protein-D, and Monocyte Chemoattractant Protein-1 as Serum Markers for Interstitial Lung Diseases. Am. J. Respir. Crit. Care Med. 2002, 165, 378–381. [Google Scholar] [CrossRef]
- Fu, Q.; Bai, Y.; Liu, Y.; Zhou, J.; Zheng, Y. The Serum Level and Significance of Lysyl Oxidase-like 2 in Patients with Rheumatoid Arthritis-Associated Interstitial Lung Disease. Clin. Rheumatol. 2018, 37, 193–198. [Google Scholar] [CrossRef] [PubMed]
- De Lauretis, A.; Veeraraghavan, S.; Renzoni, E. Connective Tissue Disease-Associated Interstitial Lung Disease: How Does It Differ from IPF? How Should the Clinical Approach Differ? Chronic Respir. Dis. 2011, 8, 53–82. [Google Scholar] [CrossRef] [PubMed]
- Paulin, F.; Doyle, T.J.; Fletcher, E.A.; Ascherman, D.P.; Rosas, I.O. Rheumatoid Arthritis-Associated Interstitial Lung Disease and Idiopathic Pulmonary Fibrosis: Shared Mechanistic and Phenotypic Traits Suggest Overlapping Disease Mechanisms. Rev. Investig. Clin. 2015, 67, 280–286. [Google Scholar]
- Matson, S.; Lee, J.; Eickelberg, O. Two Sides of the Same Coin? A Review of the Similarities and Differences between Idiopathic Pulmonary Fibrosis and Rheumatoid Arthritis-Associated Interstitial Lung Disease. Eur. Respir. J. 2021, 57, 2002533. [Google Scholar] [CrossRef] [PubMed]
- Perry, E.; Kelly, C.; Eggleton, P.; de Soyza, A.; Hutchinson, D. The Lung in ACPA-Positive Rheumatoid Arthritis: An Initiating Site of Injury? Rheumatology 2014, 53, 1940–1950. [Google Scholar] [CrossRef] [PubMed]
- Tirelli, C.; Morandi, V.; Valentini, A.; La Carrubba, C.; Dore, R.; Zanframundo, G.; Morbini, P.; Grignaschi, S.; Franconeri, A.; Oggionni, T.; et al. Multidisciplinary Approach in the Early Detection of Undiagnosed Connective Tissue Diseases in Patients with Interstitial Lung Disease: A Retrospective Cohort Study. Front. Med. 2020, 7, 11. [Google Scholar] [CrossRef]
- Fischer, A.; du Bois, R. Interstitial Lung Disease in Connective Tissue Disorders. Lancet 2012, 380, 689–698. [Google Scholar] [CrossRef]
- Oldham, J.M.; Adegunsoye, A.; Valenzi, E.; Lee, C.; Witt, L.; Chen, L.; Husain, A.N.; Montner, S.; Chung, J.H.; Cottin, V.; et al. Characterisation of Patients with Interstitial Pneumonia with Autoimmune Features. Eur. Respir. J. 2016, 47, 1767. [Google Scholar] [CrossRef]
- Zamora-Legoff, J.A.; Krause, M.L.; Crowson, C.S.; Ryu, J.H.; Matteson, E.L. Patterns of Interstitial Lung Disease and Mortality in Rheumatoid Arthritis. Rheumatology 2017, 56, 344–350. [Google Scholar] [CrossRef]
- Yunt, Z.X.; Chung, J.H.; Hobbs, S.; Fernandez-Perez, E.R.; Olson, A.L.; Huie, T.J.; Keith, R.C.; Janssen, W.J.; Goldstein, B.L.; Lynch, D.A.; et al. High Resolution Computed Tomography Pattern of Usual Interstitial Pneumonia in Rheumatoid Arthritis-Associated Interstitial Lung Disease: Relationship to Survival. Respir. Med. 2017, 126, 100–104. [Google Scholar] [CrossRef]
- Salaffi, F.; Carotti, M.; di Carlo, M.; Tardella, M.; Giovagnoni, A.; Adamek, M. High-Resolution Computed Tomography of the Lung in Patients with Rheumatoid Arthritis: Prevalence of Interstitial Lung Disease Involvement and Determinants of Abnormalities. Medicine 2019, 98, e17088. [Google Scholar] [CrossRef] [PubMed]
- Lan, S.; Huayang, D.; Ruxuan, C.; Xin, S.; Wei, S.; Zhengyu, J. Chest High-Resolution Computed Tomography Imaging Features of Lung Involvement in Rheumatoid Arthritis. Acta Acad. Med. Sin. 2020, 42, 202–208. [Google Scholar] [CrossRef]
- Huang, S.; Doyle, T.J.; Hammer, M.M.; Byrne, S.C.; Huang, W.; Marshall, A.A.; Iannaccone, C.K.; Huang, J.; Feathers, V.; Weinblatt, M.E.; et al. Rheumatoid Arthritis-Related Lung Disease Detected on Clinical Chest Computed Tomography Imaging: Prevalence, Risk Factors, and Impact on Mortality. Semin. Arthritis Rheum. 2020, 50, 1216–1225. [Google Scholar] [CrossRef] [PubMed]
- Balbir-Gurman, A.; Guralnik, L.; Yigla, M.; Braun-Moscovici, Y.; Hardak, E. Imaging Aspects of Interstitial Lung Disease in Patients with Rheumatoid Arthritis: Literature Review. Autoimmun. Rev. 2018, 17, 87–93. [Google Scholar] [CrossRef]
- Gautam, M.; Masood, M.J.; Arooj, S.; Mahmud, M.-H.; Mukhtar, M.U. Rheumatoid Arthritis Related Interstitial Lung Disease: Patterns of High-Resolution Computed Tomography. Cureus 2020, 12, e6875. [Google Scholar] [CrossRef]
- Zamora-Legoff, J.A.; Krause, M.L.; Crowson, C.S.; Ryu, J.H.; Matteson, E.L. Progressive Decline of Lung Function in Rheumatoid Arthritis–Associated Interstitial Lung Disease. Arthritis Rheumatol. 2017, 69, 542–549. [Google Scholar] [CrossRef]
- Robles-Pérez, A.; Luburich, P.; Bolivar, S.; Dorca, J.; Nolla, J.M.; Molina-Molina, M.; Narváez, J. A Prospective Study of Lung Disease in a Cohort of Early Rheumatoid Arthritis Patients. Sci. Rep. 2020, 10, 15640. [Google Scholar] [CrossRef]
- Hyldgaard, C.; Hilberg, O.; Pedersen, A.B.; Ulrichsen, S.P.; Løkke, A.; Bendstrup, E.; Ellingsen, T. A Population-Based Cohort Study of Rheumatoid Arthritis-Associated Interstitial Lung Disease: Comorbidity and Mortality. Ann. Rheum. Dis. 2017, 76, 1700–1706. [Google Scholar] [CrossRef]
- Kim, E.J.; Collard, H.R.; King, T.E. Rheumatoid Arthritis-Associated Interstitial Lung Disease: The Relevance of Histopathologic and Radiographic Pattern. Chest 2009, 136, 1397–1405. [Google Scholar] [CrossRef]
- Manfredi, A.; Cassone, G.; Luppi, F.; Atienza-Mateo, B.; Cavazza, A.; Sverzellati, N.; González-Gay, M.A.; Salvarani, C.; Sebastiani, M. Rheumatoid Arthritis Related Interstitial Lung Disease. Expert. Rev. Clin. Immunol. 2021, 17, 485–497. [Google Scholar] [CrossRef]
- Kelly, C.; Saravanan, V. Treatment Strategies for a Rheumatoid Arthritis Patient with Interstitial Lung Disease. Expert Opin. Pharmacother. 2008, 9, 3221–3230. [Google Scholar] [CrossRef] [PubMed]
- Vij, R.; Strek, M.E. Diagnosis and Treatment of Connective Tissue Disease-Associated Interstitial Lung Disease. Chest 2013, 143, 814–824. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, K.; Kelly, C. Treatment of Rheumatoid Arthritis-Associated Interstitial Lung Disease: A Perspective Review. Ther. Adv. Musculoskelet. Dis. 2015, 7, 247–267. [Google Scholar] [CrossRef] [PubMed]
- Song, L.N.; Kong, X.D.; Wang, H.J.; bin Zhan, L. Establishment of a Rat Adjuvant Arthritis-Interstitial Lung Disease Model. Biomed. Res. Int. 2016, 2016, 2970783. [Google Scholar] [CrossRef]
- Juge, P.A.; Lee, J.S.; Lau, J.; Kawano-Dourado, L.; Serrano, J.R.; Sebastiani, M.; Koduri, G.; Matteson, E.; Bonfiglioli, K.; Sawamura, M.; et al. Methotrexate and Rheumatoid Arthritis Associated Interstitial Lung Disease. Eur. Respir. J. 2021, 57, 2000337. [Google Scholar] [CrossRef]
- Kiely, P.; Busby, A.D.; Nikiphorou, E.; Sullivan, K.; Walsh, D.A.; Creamer, P.; Dixey, J.; Young, A. Is Incident Rheumatoid Arthritis Interstitial Lung Disease Associated with Methotrexate Treatment? Results from a Multivariate Analysis in the ERAS and ERAN Inception Cohorts. BMJ Open 2019, 9, e028466. [Google Scholar] [CrossRef]
- Md Yusof, M.Y.; Kabia, A.; Darby, M.; Lettieri, G.; Beirne, P.; Vital, E.M.; Dass, S.; Emery, P. Effect of Rituximab on the Progression of Rheumatoid Arthritis–Related Interstitial Lung Disease: 10 Years’ Experience at a Single Centre. Rheumatology 2017, 56, 1348. [Google Scholar] [CrossRef]
- Bonniaud, P.; Georges, M.; Favrolt, N.; Camus, P. Drug-Induced Interstitial Lung Disease. Eur. Respir. J. 2022, 64, 951–956. [Google Scholar] [CrossRef]
- Fernández-Díaz, C.; Castañeda, S.; Melero-González, R.B.; Ortiz-Sanjuán, F.; Juan-Mas, A.; Carrasco-Cubero, C.; Casafont-Solé, I.; Olivé, A.; Rodríguez-Muguruza, S.; Almodóvar-González, R.; et al. Abatacept in Interstitial Lung Disease Associated with Rheumatoid Arthritis: National Multicenter Study of 263 Patients. Rheumatology 2020, 59, 3906–3916. [Google Scholar] [CrossRef]
- Mena-Vázquez, N.; Redondo-Rodríguez, R.; Rojas-Gimenez, M.; Romero-Barco, C.M.; Manrique-Arija, S.; Ortega-Castro, R.; Hidalgo Conde, A.; Arnedo Díez de Los Ríos, R.; Cabrera César, E.; Espildora, F.; et al. Efficacy and Safety of Rituximab in Autoimmune Disease-Associated Interstitial Lung Disease: A Prospective Cohort Study. J. Clin. Med. 2022, 11, 927. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, D.; Wang, L.; Wang, S.; Roden, A.C.; Zhao, H.; Li, X.; Prakash, X.Y.S.; Matteson, E.L.; Tschumperlin, D.J.; et al. Profibrotic Effect of IL-17A and Elevated IL-17RA in Idiopathic Pulmonary Fibrosis and Rheumatoid Arthritis-Associated Lung Disease Support a Direct Role for IL-17A/IL-17RA in Human Fibrotic Interstitial Lung Disease. Am. J. Physiol. Lung Cell. Mol. Physiol. 2019, 316, L487–L497. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Wang, X.; Ye, S. Tofacitinib in Amyopathic Dermatomyositis–Associated Interstitial Lung Disease. N. Engl. J. Med. 2019, 381, 291–293. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandro, M.; Perillo, F.; Metella Refini, R.; Bergantini, L.; Bellisai, F.; Selvi, E.; Cameli, P.; Manganelli, S.; Conticini, E.; Cantarini, L.; et al. Efficacy of Baricitinib in Treating Rheumatoid Arthritis: Modulatory Effects on Fibrotic and Inflammatory Biomarkers in a Real-Life Setting. Int. Immunopharmacol. 2020, 86, 106748. [Google Scholar] [CrossRef] [PubMed]
- Silva-Carmona, M.; Vogel, T.P.; Marchal, S.; Guesmi, M.; Jean-Christophe, D.; Leroy, S.; Fabre, A.; Barlogis, V.; Forbes, L.R.; Giovannini-Chami, L. Successful Treatment of Interstitial Lung Disease in STAT3 Gain-of-Function Using JAK Inhibitors. Am. J. Respir. Crit. Care Med. 2020, 202, 893–897. [Google Scholar] [CrossRef]
- Balci, S.; Ekinci, R.M.K.; de Jesus, A.A.; Goldbach-Mansky, R.; Yilmaz, M. Baricitinib Experience on STING-Associated Vasculopathy with Onset in Infancy: A Representative Case from Turkey. Clin. Immunol. 2020, 212, 108273. [Google Scholar] [CrossRef]
- Bader-Meunier, B.; Hadchouel, A.; Berteloot, L.; Polivka, L.; Béziat, V.; Casanova, J.L.; Lévy, R. Effectiveness and Safety of Ruxolitinib for the Treatment of Refractory Systemic Idiopathic Juvenile Arthritis like Associated with Interstitial Lung Disease: A Case Report. Ann. Rheum. Dis. 2022, 81, E20. [Google Scholar] [CrossRef]
- Makino, S. Progressive Fibrosing Interstitial Lung Diseases: A New Concept and Indication of Nintedanib. Mod. Rheumatol. 2021, 31, 13–19. [Google Scholar] [CrossRef]
- Miura, Y.; Ohkubo, H.; Niimi, A.; Kanazawa, S. Suppression of Epithelial Abnormalities by Nintedanib in Induced-Rheumatoid Arthritis-Associated Interstitial Lung Disease Mouse Model. ERJ Open Res. 2021, 7, 00345. [Google Scholar] [CrossRef]
- Wollin, L.; Distler, J.H.W.; Redente, E.F.; Riches, D.W.H.; Stowasser, S.; Schlenker-Herceg, R.; Maher, T.M.; Kolb, M. Potential of Nintedanib in Treatment of Progressive Fibrosing Interstitial Lung Diseases. Eur. Respir. J. 2019, 54, 1900161. [Google Scholar] [CrossRef]
- Wells, A.U.; Flaherty, K.R.; Brown, K.K.; Inoue, Y.; Devaraj, A.; Richeldi, L.; Moua, T.; Crestani, B.; Wuyts, W.A.; Stowasser, S.; et al. Nintedanib in Patients with Progressive Fibrosing Interstitial Lung Diseases-Subgroup Analyses by Interstitial Lung Disease Diagnosis in the INBUILD Trial: A Randomised, Double-Blind, Placebo-Controlled, Parallel-Group Trial. Lancet Respir. Med. 2020, 8, 453–460. [Google Scholar] [CrossRef]
- Behr, J.; Prasse, A.; Kreuter, M.; Johow, J.; Rabe, K.F.; Bonella, F.; Bonnet, R.; Grohe, C.; Held, M.; Wilkens, H.; et al. Pirfenidone in Patients with Progressive Fibrotic Interstitial Lung Diseases Other than Idiopathic Pulmonary Fibrosis (RELIEF): A Double-Blind, Randomised, Placebo-Controlled, Phase 2b Trial. Lancet Respir. Med. 2021, 9, 476–486. [Google Scholar] [CrossRef]
- Behr, J.; Neuser, P.; Prasse, A.; Kreuter, M.; Rabe, K.; Schade-Brittinger, C.; Wagner, J.; Günther, A. Exploring Efficacy and Safety of Oral Pirfenidone for Progressive, Non-IPF Lung Fibrosis (RELIEF)—A Randomized, Double-Blind, Placebo-Controlled, Parallel Group, Multi-Center, Phase II Trial. BMC Pulm. Med. 2017, 17, 122. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Category | Biomarkers | Value | Evidence |
|---|---|---|---|
| Autoantibodies | ACPA | Diagnosis | High specificity—high titers associated with higher incidence of RA-ILD [54] |
| Anticitrullinated HSP90 | Diagnosis | Relatively high specificty and sensitivity [55] | |
| PAD | Severity | No utility for diagnosis—possible link to disease severity [56] | |
| Rheumatoid factor | Diagnosis | Low specificity—high titers associated with higher incidence of RA-ILD [57] | |
| Anti-CEP1 | Diagnosis | More specific for synovial disease [58] | |
| Anti-CarP | Diagnosis | Relatively high specificity [59] | |
| Anti-MAA | Diagnosis | Not specific for RA-ILD—also found in RA without ILD [60] | |
| Genetic biomarkers | MUC5B gene | Diagnosis | Highly suggestive, specifically in those with UIP pattern [61,62] |
| microRNAs (has-miR-214-5p, has-miR-7-5p) | Diagnosis | High specificity, lower sensitivity—higher levels in patients with RA-ILD, not RA without ILD [63] | |
| HLA haplotypes (HLA-DR2, HLA-DQB1*04, *06, HLA-DR4, HLA-DRB1*14:06, HLA-DRB1*16:02-DQB1*05:02) | Diagnosis | Relatively low frequencies in RA-ILD [64] | |
| Other biomarkers | KL-6 | Severity | Highly suggestive for severity on HRCT [65,66] |
| MMP-7 | Diagnosis | Suggestive for fibrotic ILD—elevated in patients with ILD, not RA without ILD [41] | |
| CXCL10 | Diagnosis | Elevated in patients with ILD, not RA without ILD [49] | |
| sPD-L1 | Predictive | Relatively high specificity, lower sensitivity [67] | |
| IL-18 | Diagnosis | Relatively high sensitivity and specificity [68] | |
| IL-13 | Severity | Higher levels in RA-ILD, not RA without ILD [69] | |
| SP-D | Diagnosis | High specificity, lower sensitivity—influenced by bacterial lung infections [70] | |
| LOLX2 | Diagnosis | High specificity for diagnosis [71] |
| Clinical Study | Type | Primary Outcome | Secondary Outcome | Biomarkers | Status/Results |
|---|---|---|---|---|---|
| Soluble Programmed Death 1 (sPD1) is a Diagnostic Biomarker of ILD in Patients With Rheumatoid Arthritis Disease NCT05105230 Year: 2021 | Observational, Retrospective, Case-control, NP—66 | Evaluation of the levels of serum (sPD1) in RA patients and its association with ILD | Detection of subclinical RA-ILD for early diagnosis and management of this extra-articular manifestation | sPD1 | Not yet recruiting |
| Deciphering Rheumatoid Arthritis -associated Interstitial Lung Disease Pathogenesis 2 (TRANSLATE2) Year: 2020 | Observational, Prospective, Case-control, NP—500 | Identification of genetic factors involved in RA-ILD using whole exome sequencing (WES). | Identification of genetic factors implicated in RA-ILD using genome wide association study. Description of RA-ILD natural history by a 5 years annual follow up of RA-ILD patients. Description of the effect of disease modifying Anti Rheumatic Drugs (DMARDs) on ILD course and mortality. | Genetic | Recruiting |
| Rheumatoid Arthritis Patients at Risk for Interstitial Lung Disease (RAPID) NCT03297775 Year: 2017 | Observational, Prospective, Cohort, NP—750 | Presence or absence of ILD on HRCT imaging. The study is designed to evaluate individuals affected by RA and explore associated lung disease so that the investigators can better understand the clinical phenotype and genetic and molecular endotypes of this disease. | Multiple biomarkers (genetic, serum, sputum) | Recruiting | |
| Lysophosphatidic Acid (LPA)/Autotaxin (ATX) Axis in Rheumatoid Lung Disease (LYSLUNG) NCT04284735 Year:2020 | Interventional, Non-randomized NP—40 | ATX and LPA levels in sputum from RA patients with ILD in comparison with sputum from RA patients without ILD | Correlation between ATX and LPA levels and severity of RA-ILD estimated by tomodensitometry | LPA/ATX | Recruiting |
| Rheumatoid Arthritis-Associated Interstitial Lung Disease: Characterization of Lung Disease Progression (BERTHA) NCT04136223 Year: 2019 | Observational, Prospective, Cohort NP—100 | Interstitial Lung Disease progression—FVC | Interstitial Lung Disease progression—imaging, death, FVC dichotomous variable | Genetic | Recruiting |
| Factors of ILD in Newly Diagnosed Rheumatoid Arthritis (FIND-RA) NCT04002765 Year: 2019 | Interventional, Single group assignment NP—300 | Presence of an interstitial lung disease | Proportion of different ILD subtypes Proportion of patients with a non-ILD lung involvement of RA rs35705950 variant of the MUC5B promoter Anti-CCP antibodies Relevant exposure | rs35705950 variant of the MUC5B promoter anti-CCP antibodies | Recruiting |
| Effects of Tofacitinib vs. Methotrexate on Clinical and Molecular Disease Activity Markers in Joints and Lungs in Early Rheumatoid Arthritis (PULMORA)—A Randomized, Controlled, Open-label, Assessor-blinded, Phase IV Trial NCT04311567 Year: 2020 | Interventional, Randomized, Parallel assignment NP—48 | Change in total interstitial disease score of pulmonary abnormalities by HRCT | Change in extent of parenchymal lung disease by HRCT pattern Change in Forced Vital Capacity (FVC) Change in Diffusion Capacity of Carbon Monoxide (DLCO) Change in walking distance (meters) Change in blood oxygen saturation (SpO2) after 6 min walking Patient reported outcome of breathing and airway symptoms | Exploratory sub-study: Gene expression of bulk tissue and sorted cells of synovial biopsies and broncho-alveolar lavage samples by RNA sequencing. Levels of cytokines (IL-1β, IFN-α2, IFN-γ, TNF-α, IL-6, IL-8 (CXCL8), IL-10, IL-12p70, IL-17A, IL-18, IL-23, and IL-33), chemokines (CCL2, CCL3, CCL4, CCL5, CCL11, CCL17, CCL20, CXCL1, CXCL5, CXCL8, CXCL9, CXCL10, CXCL11) and growth factors (GM-CSF, PDGF and TGFbeta1) of synovial fluid, blood and broncho-alveolar lavage will be determined by bead-based immunoassay. | Recruiting |
| Change in Serum and Sputum Biomarkers Over Time in the Development of Rheumatoid Arthritis-associated Lung Disease NCT03616158 Year: 2019 | Observational, NP—340 | Define which patients with RA (or pre-RA) are at greatest risk for developing RA-related lung disease (LD) | Multiple biomarkers (genetic, serum, sputum) | Recruiting |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Florescu, A.; Gherghina, F.L.; Mușetescu, A.E.; Pădureanu, V.; Roșu, A.; Florescu, M.M.; Criveanu, C.; Florescu, L.-M.; Bobircă, A. Novel Biomarkers, Diagnostic and Therapeutic Approach in Rheumatoid Arthritis Interstitial Lung Disease—A Narrative Review. Biomedicines 2022, 10, 1367. https://doi.org/10.3390/biomedicines10061367
Florescu A, Gherghina FL, Mușetescu AE, Pădureanu V, Roșu A, Florescu MM, Criveanu C, Florescu L-M, Bobircă A. Novel Biomarkers, Diagnostic and Therapeutic Approach in Rheumatoid Arthritis Interstitial Lung Disease—A Narrative Review. Biomedicines. 2022; 10(6):1367. https://doi.org/10.3390/biomedicines10061367
Chicago/Turabian StyleFlorescu, Alesandra, Florin Liviu Gherghina, Anca Emanuela Mușetescu, Vlad Pădureanu, Anca Roșu, Mirela Marinela Florescu, Cristina Criveanu, Lucian-Mihai Florescu, and Anca Bobircă. 2022. "Novel Biomarkers, Diagnostic and Therapeutic Approach in Rheumatoid Arthritis Interstitial Lung Disease—A Narrative Review" Biomedicines 10, no. 6: 1367. https://doi.org/10.3390/biomedicines10061367
APA StyleFlorescu, A., Gherghina, F. L., Mușetescu, A. E., Pădureanu, V., Roșu, A., Florescu, M. M., Criveanu, C., Florescu, L.-M., & Bobircă, A. (2022). Novel Biomarkers, Diagnostic and Therapeutic Approach in Rheumatoid Arthritis Interstitial Lung Disease—A Narrative Review. Biomedicines, 10(6), 1367. https://doi.org/10.3390/biomedicines10061367