
Endovascular Intervention in Acute Ischemic Stroke: History and Evolution

 ,
,
Abstract
:1. Introduction
2. Evolution of Endovascular Therapy in Ischemic Stroke
2.1. History
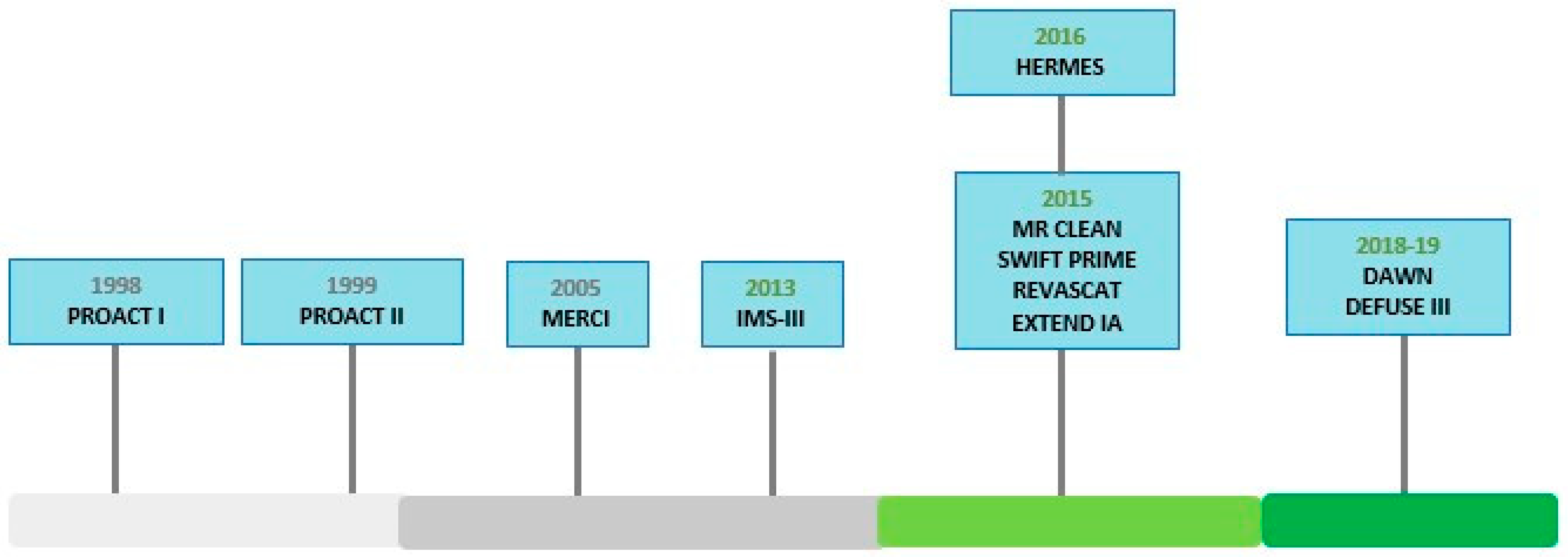
2.2. Early Clinical Trials
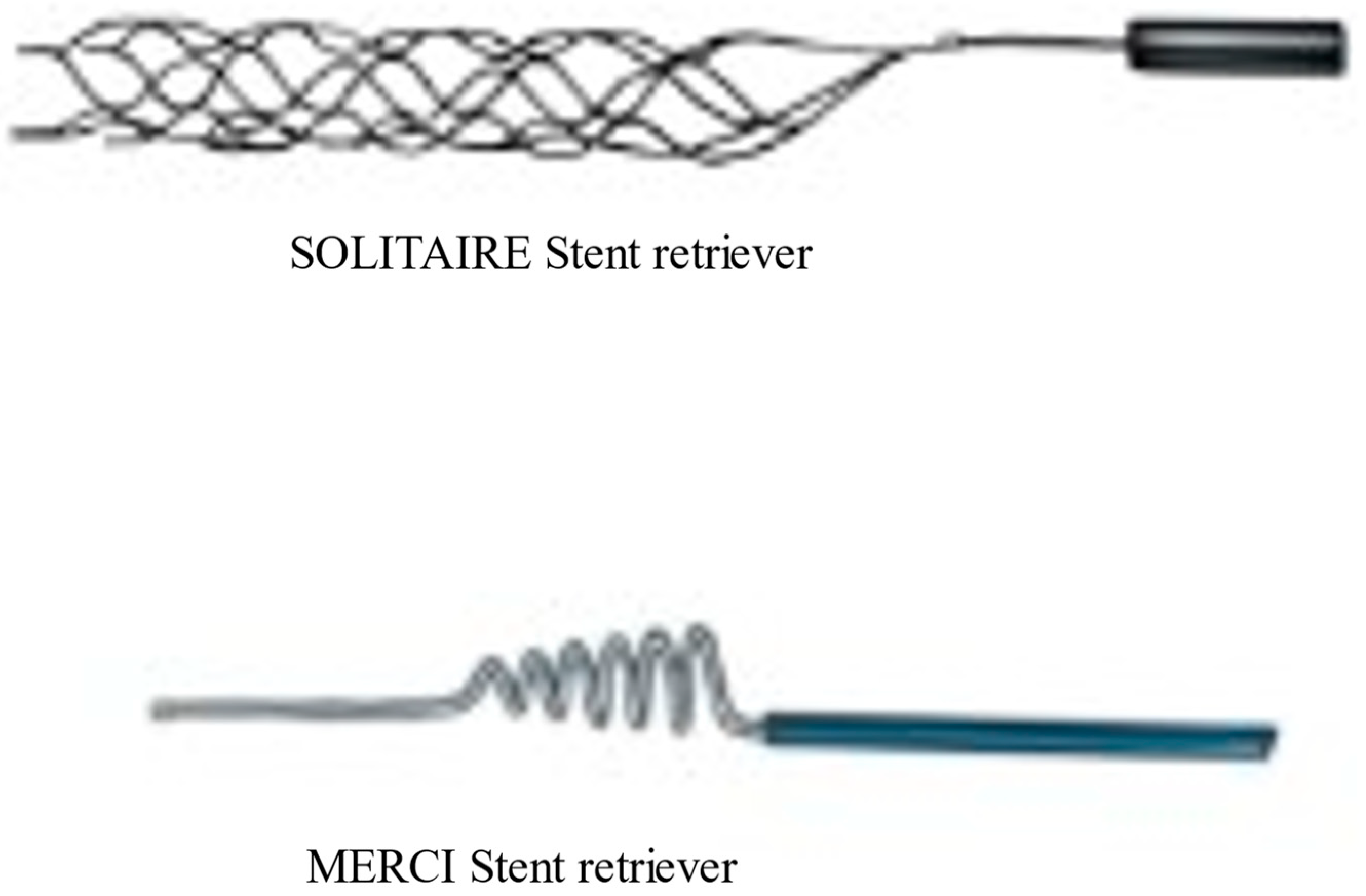
2.3. Second Generation Thrombectomy Devices
2.4. Modern Clinical Trials and Paradigm Shift
2.5. Evolution of the Concept of the Tissue Window and Late Window Trials
3. Conclusions
4. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 1 | PROACT: Prolyse in Acute Cerebral Thromboembolism |
| 2 | MERCI: Mechanical Embolus Removal in Cerebral Ischemia |
| 3 | MR RESCUE: Mechanical Retrieval and Recanalization of Stroke Clots Using Embolectomy |
| 4 | IMS-III: Interventional Management of Stroke-III |
| 5 | mRS: Modified Rankin Scale |
| 6 | SYNTHESIS: Systemic intravenous (IV) thrombolysis with Alteplase in acute ischemic stroke |
| 7 | MR CLEAN: Multicenter Randomized Clinical trial of Endovascular treatment for Acute ischemic stroke in the Netherlands |
| 8 | ESCAPE: Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times |
| 9 | SWIFT PRIME: Solitaire with the Intention for Thrombectomy as Primary Endovascular Treatment |
| 10 | REVASCAT: Randomized Trial of Revascularization with Solitaire FR Device versus Best Medical Therapy in the Treatment of Acute Stroke Due to Anterior Circulation Large Vessel Occlusion Presenting within Eight Hours of Symptom Onset |
| 11 | EXTEND IA: Extending the Time for Thrombolysis in Emergency Neurological Deficits—Intra-Arterial |
| 12 | HERMES: Highly Effective Reperfusion evaluated in Multiple Endovascular Stroke Trials |
| 13 | DAWN: DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo |
| 14 | DEFUSE: Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke |
References
- Johnson, W.; Onuma, O.; Owolabi, M.; Sachdev, S. Stroke: A global response is needed. Bull World Health Organ 2016, 94, 634. [Google Scholar] [CrossRef] [PubMed]
- Collaborators, G.B.D.S. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Campbell, B.C.V.; De Silva, D.A.; Macleod, M.R.; Coutts, S.B.; Schwamm, L.H.; Davis, S.M.; Donnan, G.A. Ischaemic stroke. Nat Rev. Dis. Primers 2019, 5, 70. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Barber, P.A.; Zhang, J.; Demchuk, A.M.; Hill, M.D.; Buchan, A.M. Why are stroke patients excluded from TPA therapy? An analysis of patient eligibility. Neurology 2001, 56, 1015–1020. [Google Scholar] [CrossRef]
- Rabinstein, A.A. Update on Treatment of Acute Ischemic Stroke. Continuum (Minneap Minn) 2020, 26, 268–286. [Google Scholar] [CrossRef]
- Wang, D.; Wang, Y. Tissue window, not the time window, will guide acute stroke treatment. Stroke Vasc. Neurol. 2019, 4, 1–2. [Google Scholar] [CrossRef]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.; Mitchell, P.J.; Demchuk, A.M.; Davalos, A.; Majoie, C.B.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Artico, M.; Spoletini, M.; Fumagalli, L.; Biagioni, F.; Ryskalin, L.; Fornai, F.; Salvati, M.; Frati, A.; Pastore, F.S.; Taurone, S. Egas Moniz: 90 Years (1927–2017) from Cerebral Angiography. Front. Neuroanat. 2017, 11, 81. [Google Scholar] [CrossRef] [Green Version]
- Smith, W.S.; Furlan, A.J. Brief History of Endovascular Acute Ischemic Stroke Treatment. Stroke 2016, 47, e23–e26. [Google Scholar] [CrossRef] [Green Version]
- del Zoppo, G.J.; Higashida, R.T.; Furlan, A.J.; Pessin, M.S.; Rowley, H.A.; Gent, M. PROACT: A phase II randomized trial of recombinant pro-urokinase by direct arterial delivery in acute middle cerebral artery stroke. PROACT Investigators. Prolyse in Acute Cerebral Thromboembolism. Stroke 1998, 29, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyle, K.; Joundi, R.A.; Aviv, R.I. An historical and contemporary review of endovascular therapy for acute ischemic stroke. Neurovascular Imaging 2017, 3, 1. [Google Scholar] [CrossRef]
- Furlan, A.; Higashida, R.; Wechsler, L.; Gent, M.; Rowley, H.; Kase, C.; Pessin, M.; Ahuja, A.; Callahan, F.; Clark, W.M.; et al. Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study: A randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA 1999, 282, 2003–2011. [Google Scholar] [CrossRef]
- Smith, W.S.; Sung, G.; Saver, J.; Budzik, R.; Duckwiler, G.; Liebeskind, D.S.; Lutsep, H.L.; Rymer, M.M.; Higashida, R.T.; Starkman, S.; et al. Mechanical Thrombectomy for Acute Ischemic Stroke. Stroke 2008, 39, 1205–1212. [Google Scholar] [CrossRef] [Green Version]
- Bose, A.; Henkes, H.; Alfke, K.; Reith, W.; Mayer, T.E.; Berlis, A.; Branca, V.; Sit, S.P. The Penumbra System: A mechanical device for the treatment of acute stroke due to thromboembolism. AJNR Am. J. Neuroradiol. 2008, 29, 1409–1413. [Google Scholar] [CrossRef] [Green Version]
- Castaño, C.; Serena, J.; Dávalos, A. Use of the New Solitaire (TM) AB Device for Mechanical Thrombectomy when Merci Clot Retriever Has Failed to Remove the Clot. A Case Report. Interv. Neuroradiol. 2009, 15, 209–214. [Google Scholar] [CrossRef]
- Saver, J.L.; Jahan, R.; Levy, E.I.; Jovin, T.G.; Baxter, B.; Nogueira, R.G.; Clark, W.; Budzik, R.; Zaidat, O.O. Solitaire flow restoration device versus the Merci Retriever in patients with acute ischaemic stroke (SWIFT): A randomised, parallel-group, non-inferiority trial. Lancet 2012, 380, 1241–1249. [Google Scholar] [CrossRef]
- Ciccone, A.; Valvassori, L.; Nichelatti, M.; Sgoifo, A.; Ponzio, M.; Sterzi, R.; Boccardi, E. Endovascular treatment for acute ischemic stroke. N. Engl. J. Med. 2013, 368, 904–913. [Google Scholar] [CrossRef] [Green Version]
- Broderick, J.P.; Palesch, Y.Y.; Demchuk, A.M.; Yeatts, S.D.; Khatri, P.; Hill, M.D.; Jauch, E.C.; Jovin, T.G.; Yan, B.; Silver, F.L.; et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N. Engl. J. Med. 2013, 368, 893–903. [Google Scholar] [CrossRef] [Green Version]
- Khatri, P.; Abruzzo, T.; Yeatts, S.D.; Nichols, C.; Broderick, J.P.; Tomsick, T.A. Good clinical outcome after ischemic stroke with successful revascularization is time-dependent. Neurology 2009, 73, 1066–1072. [Google Scholar] [CrossRef] [Green Version]
- Berkhemer, O.A.; Fransen, P.S.; Beumer, D.; van den Berg, L.A.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.; et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saver, J.L.; Goyal, M.; Bonafe, A.; Diener, H.C.; Levy, E.I.; Pereira, V.M.; Albers, G.W.; Cognard, C.; Cohen, D.J.; Hacke, W.; et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N. Engl. J. Med. 2015, 372, 2285–2295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina, C.A.; Chamorro, A.; Rovira, A.; de Miquel, A.; Serena, J.; Roman, L.S.; Jovin, T.G.; Davalos, A.; Cobo, E. REVASCAT: A randomized trial of revascularization with SOLITAIRE FR device vs. best medical therapy in the treatment of acute stroke due to anterior circulation large vessel occlusion presenting within eight-hours of symptom onset. Int. J. Stroke 2015, 10, 619–626. [Google Scholar] [CrossRef]
- Campbell, B.C.; Mitchell, P.J.; Kleinig, T.J.; Dewey, H.M.; Churilov, L.; Yassi, N.; Yan, B.; Dowling, R.J.; Parsons, M.W.; Oxley, T.J.; et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N. Engl. J. Med. 2015, 372, 1009–1018. [Google Scholar] [CrossRef] [Green Version]
- Barber, P.A.; Demchuk, A.M.; Zhang, J.; Buchan, A.M. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet 2000, 355, 1670–1674. [Google Scholar] [CrossRef]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef]
- Albers, G.W.; Marks, M.P.; Kemp, S.; Christensen, S.; Tsai, J.P.; Ortega-Gutierrez, S.; McTaggart, R.A.; Torbey, M.T.; Kim-Tenser, M.; Leslie-Mazwi, T.; et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N. Engl. J. Med. 2018, 378, 708–718. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [CrossRef]
- Turc, G.; Bhogal, P.; Fischer, U.; Khatri, P.; Lobotesis, K.; Mazighi, M.; Schellinger, P.D.; Toni, D.; de Vries, J.; White, P.; et al. European Stroke Organisation (ESO)—European Society for Minimally Invasive Neurological Therapy (ESMINT) Guidelines on Mechanical Thrombectomy in Acute Ischemic Stroke. J. Neurointerv. Surg. 2019, 4, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Langezaal, L.C.M.; van der Hoeven, E.; Mont’Alverne, F.J.A.; de Carvalho, J.J.F.; Lima, F.O.; Dippel, D.W.J.; van der Lugt, A.; Lo, R.T.H.; Boiten, J.; Lycklama À Nijeholt, G.J.; et al. Endovascular Therapy for Stroke Due to Basilar-Artery Occlusion. N. Engl. J. Med. 2021, 384, 1910–1920. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TRIAL | Inclusion Criteria | Number of Patients | Mean/Median Age | Median NIHSS | IV tPA | Re Perfusion | sICH | mRS Less than 2 at 90 Days | limitation | Mortality 90 Days |
|---|---|---|---|---|---|---|---|---|---|---|
| MR CLEAN | NIHSS > 2, occlusion of vessel imaging | 500 I: 233 C:267 | I:65.8 C65.7 | I: 17 C: 18 | I: 87.1 C:90.6 | 58.7 | I 7.7 C6.4 | I 32.6 C 19.1 | No perfusion imaging. Low reperfusion rate | I:18.9 C:18.4 At 30 days |
| ESCAPE | NIHSS > 5, ASPECT > 6, collateral assessment, stent retriever in 84% | 315 I 165 C150 | I 71 C 70 | I 16 C 17 | I 72.7 C 78.7 | 72.4% | I 3.6 C2.7 | I 53 C29.3 | No perfusion imaging | I: 10.4 at 90 days C 19% |
| EXTEND IA | Age > 18 y Collateral assesment, perfusion imaging | 70 I 35 C 35 | I 78.6 C 70.2 | I 17 C 13 | I 100 C 100 | 86% | I 0 C 6 | I 71 C 40 | Small sample size | I 9% C 20% |
| SWIFT PRIME | NIHSS 8–29 ASPECT > 6 Perfusion imaging | 196 I 98 C 98 | I 65 C 66.3 | I 17 C 17 | I 100 C 100 | 83% | I 0 C 3 | I 16 C 35 | All patients received IVT | I 9 C12 |
| REVASCAT | NIHSS > 6 ASPECT > 6 AGE 18–85 years | 206 I 103 C 103 | I 65.7 C 67.2 | I 17 C 17 | I 68 C 77 | 65.6% | I 4.9 C1.9 | I 43.7 C28.2 | Low reperfusion rate | I: 18.4% C:15.5% |
| DAWN | NIHSS > 10 Core and clinical mismatch Up to 24 h | 206 I 107 C 99 | I 69.4 C 70.7 | I 17 C 17 | I 5 C 13 | 84% | I 6 C 3 | I 49 C 13 | Severe stroke, Difference in baseline variables | I 19 C 18 |
| DIFFUSE 3 | Perfusion with mismatch 6–16 | 182 I 92 C 90 | I 70 C 71 | I 16 C 16 | I 11 C 9 | 76% | I 7% C 4% | I 45% C 17% | Patient papulation is older. | I 14% C 26% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ansari, J.; Triay, R.; Kandregula, S.; Adeeb, N.; Cuellar, H.; Sharma, P. Endovascular Intervention in Acute Ischemic Stroke: History and Evolution. Biomedicines 2022, 10, 418. https://doi.org/10.3390/biomedicines10020418
Ansari J, Triay R, Kandregula S, Adeeb N, Cuellar H, Sharma P. Endovascular Intervention in Acute Ischemic Stroke: History and Evolution. Biomedicines. 2022; 10(2):418. https://doi.org/10.3390/biomedicines10020418
Chicago/Turabian StyleAnsari, Junaid, Rachel Triay, Sandeep Kandregula, Nimer Adeeb, Hugo Cuellar, and Pankaj Sharma. 2022. "Endovascular Intervention in Acute Ischemic Stroke: History and Evolution" Biomedicines 10, no. 2: 418. https://doi.org/10.3390/biomedicines10020418
APA StyleAnsari, J., Triay, R., Kandregula, S., Adeeb, N., Cuellar, H., & Sharma, P. (2022). Endovascular Intervention in Acute Ischemic Stroke: History and Evolution. Biomedicines, 10(2), 418. https://doi.org/10.3390/biomedicines10020418