
Analysis of Reproduction Number R0 of COVID-19 Using Current Health Expenditure as Gross Domestic Product Percentage (CHE/GDP) across Countries




Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials: The Variables
2.2. Methods
2.2.1. Exponential and ARIMA Model
2.2.2. Clustering Methodology
2.2.3. Linear and Polynomial Regression
2.2.4. Multivariate Ordinary Least Square Method
3. Results
3.1. Autocorrelation Slope
3.1.1. Parabolic and Cubic Regression
3.1.2. Quartic Regression
3.1.3. Sextic Regression
3.2. Exponential Model Slope
3.2.1. Developed and Developing Countries
3.2.2. Developed Countries
3.2.3. All Countries
3.3. ARIMA Model for First and Second Wave
3.3.1. First Wave ARIMA Model
3.3.2. ARIMA Model Forecast for First and Second Wave
3.4. Clustering of Countries from Epidemic and Economic Variables
3.5. Ordinary Least Square Method. The Multivariate Case
- The principal component analysis shows the importance of the CHE/GDP index in the first principal component (Figure 11a,c,d) and of the deterministic R0 (R0det) of the exponential phase of the first wave in the second principal component and of the second wave in third principal component (Figure 11e);
- The analysis of parallel coordinates for cluster centroids also shows the importance of the deterministic R0 in the discrimination of clusters (Figure 12);
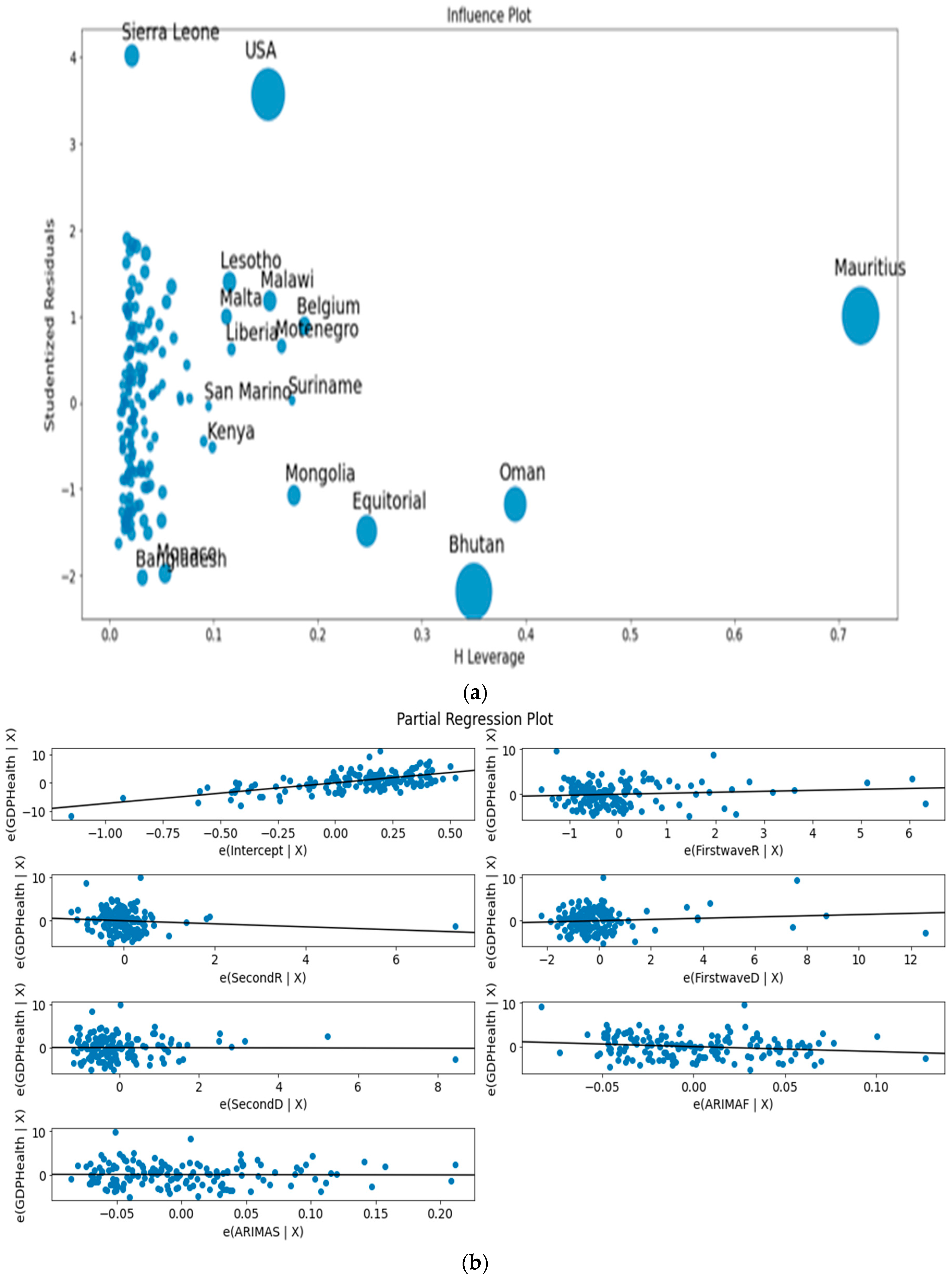
- The analysis of the residuals shows a good explanatory power of the first three principal components (60% of the total variance in Figure 11c, confirmed by the projections on the two first principal planes of Figure 11d,e), and a weak correlation of the principal components with these residuals (Figure 13a,b).
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ARIMAF | Opposite autocorrelation slope for first wave |
| ARIMAS | Opposite autocorrelation slope for second wave |
| SecondR | Maximum R0 for second wave from [3] |
| SecondD | Deterministic R0 for second wave from [2] |
| FirstwaveR | Maximum R0 for first wave from [3] |
| FirstwaveD | Deterministic R0 for first wave from [2] |
| CHE/GDP | Current health expenditure as gross domestic product percentage [1] |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Countries | First Wave | Second Wave | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. | Country Name | Exponential Slope | Auto-Correlation Slope | Exponential Slope | Auto-Correlation Slope | GDP Health 2018 | ||||
| 1 | AFGHANISTAN | 1.78 | 0.65 | 0.1070 | −0.025 | 0.79 | 0.04 | 0.0017 | −0.097 | 9.40 |
| 2 | ALGERIA | 2.19 | 1.25 | 0.1594 | −0.040 | 0.86 | 0.91 | 0.0316 | −0.100 | 6.22 |
| 3 | ARUBA | - | 5.46 | - | - | - | 1.10 | 0.0172 | −0.112 | - |
| 4 | ANDORRA | - | 1.36 | −0.0313 | −0.121 | - | 0.12 | −0.0067 | −0.155 | 6.71 |
| 5 | ANGOLA | 2.06 | 0.63 | 0.0100 | −0.095 | 1.13 | 1.70 | −0.0135 | −0.057 | 2.55 |
| 6 | ANTIGUA | 4.23 | 1.92 | - | - | 3.30 | 2.13 | 0.0051 | −0.177 | 5.23 |
| 7 | ALBANIA | 1.61 | 0.96 | 0.0091 | −0.138 | 0.99 | 0.66 | 0.0058 | −0.085 | 5.26 |
| 8 | ARGENTINA | 2.06 | 0.73 | 0.1485 | −0.060 | 1.19 | 0.36 | 0.0427 | −0.240 | 9.62 |
| 9 | ARMENIA | 1.51 | 4.43 | 0.0809 | −0.050 | 0.80 | 0.86 | 0.0570 | −0.090 | 10.03 |
| 10 | AUSTRALIA | 2.45 | 2.79 | 0.1832 | −0.054 | 1.11 | 1.50 | 0.0037 | −0.136 | 9.28 |
| 11 | AUSTRIA | 2.93 | 1.17 | 0.2825 | −0.053 | 1.05 | 2.08 | 0.0034 | −0.053 | 10.33 |
| 12 | AZERBAIJAN | 2.11 | 1.16 | 0.1422 | −0.071 | 0.63 | 0.37 | 0.0676 | −0.130 | 3.51 |
| 13 | BAHAMAS | 6.33 | 0.57 | - | - | 1.48 | 1.22 | −0.0250 | −0.077 | 6.25 |
| 14 | BAHRAIN | 1.81 | 1.10 | 0.1884 | −0.079 | 1.24 | 1.14 | 0.0012 | −0.053 | 4.13 |
| 15 | BANGLADESH | 3.67 | 1.04 | 0.0799 | −0.033 | 0.92 | 0.99 | −0.0086 | −0.046 | 2.34 |
| 16 | BARBADOS | 4.63 | 1.86 | - | - | 1.99 | 1.14 | 0.0378 | −0.109 | 6.56 |
| 17 | BELARUS | 3.15 | 1.57 | 0.0043 | −0.060 | 1.02 | 1.07 | 0.0159 | −0.026 | 5.64 |
| 18 | BELGIUM | 8.28 | 0.43 | 0.1963 | −0.047 | 0.88 | 2.23 | −0.0182 | −0.063 | 10.32 |
| 19 | BELIZE | 3.74 | 0.99 | - | - | 1.34 | 0.51 | −0.0004 | −0.140 | 5.69 |
| 20 | BENIN | 2.16 | 0.85 | 0.0226 | −0.133 | 1.55 | 0.85 | 0.0020 | −0.125 | 2.49 |
| 21 | BHUTAN | 2.10 | 15.00 | 0.0021 | −0.118 | 2.49 | 1.08 | 0.0126 | −0.099 | 3.06 |
| 22 | BOLIVIA | 1.46 | 2.17 | 0.0647 | −0.045 | 1.45 | 1.61 | 0.0152 | −0.087 | 6.30 |
| 23 | BOSNIA | 1.70 | 0.09 | 0.0088 | −0.110 | 0.97 | 1.56 | −0.0118 | −0.106 | 8.90 |
| 24 | BOTSWANA | 3.76 | 28.47 | - | - | 1.43 | 28.43 | 0.0030 | −0.186 | 5.85 |
| 25 | BRAZIL | 3.10 | 0.77 | 0.0389 | −0.048 | 0.92 | 0.46 | 0.0092 | −0.188 | 9.51 |
| 26 | BRUNEI | 5.00 | 1.08 | −0.0165 | −0.120 | 3.66 | 1.00 | - | - | 2.41 |
| 27 | BULGARIA | 1.97 | 5.06 | 0.0178 | −0.087 | 0.78 | 0.75 | 0.0049 | −0.110 | 7.35 |
| 28 | BURKINA FASO | 2.44 | 1.08 | −0.0227 | −0.123 | 1.18 | 0.94 | 0.0360 | −0.058 | 5.63 |
| 29 | BURUNDI | 2.80 | 1.33 | - | - | 1.69 | 2.18 | 0.0226 | −0.063 | 7.74 |
| 30 | CABO VERDE | 1.54 | 0.82 | 0.0247 | −0.091 | 1.71 | 0.19 | −0.0064 | −0.110 | 5.36 |
| 31 | CAMBODIA | 5.55 | 0.34 | −0.0129 | −0.129 | 3.12 | 0.27 | 0.0010 | −0.158 | 6.03 |
| 32 | CAMEROON | 2.56 | 2.17 | 0.0338 | −0.123 | 1.64 | 2.48 | 0.0085 | −0.207 | - |
| 33 | CANADA | 2.95 | 1.10 | 0.2432 | −0.029 | 1.05 | 0.44 | 0.0153 | −0.047 | 10.79 |
| 34 | CAR | 2.45 | 1.66 | −0.0130 | −0.096 | 4.99 | 0.33 | - | - | 10.99 |
| 35 | CHAD | 2.43 | 1.19 | −0.0108 | −0.114 | 1.44 | 0.77 | 0.0222 | −0.050 | 4.10 |
| 36 | CHILE | 2.42 | 1.00 | 0.1906 | −0.034 | 1.16 | 1.64 | 0.0586 | −0.090 | 9.14 |
| 37 | CHINA | 2.05 | 1.10 | −0.0602 | −0.088 | 1.07 | 0.87 | 0.0137 | −0.068 | 5.35 |
| 38 | COLUMBIA | 1.86 | 1.00 | 0.0384 | −0.040 | 0.99 | 1.47 | 0.0061 | −0.126 | 7.64 |
| 39 | COMOROS | 1.93 | 3.75 | −0.0094 | −0.153 | 1.58 | 1.65 | 0.0397 | −0.076 | 4.59 |
| 40 | CONGO DEM | 1.48 | 0.03 | 0.0384 | −0.052 | 1.10 | 0.88 | 0.0252 | −0.089 | 3.30 |
| 41 | CONGO REP | 2.39 | 0.92 | 0.0294 | −0.152 | 1.43 | 0.39 | 0.0064 | −0.118 | 2.14 |
| 42 | COSTA RICA | 1.51 | 0.50 | 0.0142 | −0.110 | 1.08 | 1.26 | −0.0022 | −0.209 | 7.56 |
| 43 | COTE D’VOIRE | 1.47 | 1.18 | 0.0309 | −0.080 | 1.35 | 2.09 | 0.0253 | −0.078 | 4.19 |
| 44 | CROTIA | 3.95 | 0.75 | −0.0042 | −0.069 | 0.72 | 0.57 | −0.0115 | −0.106 | 6.83 |
| 45 | CUBA | 2.23 | 0.48 | 0.0706 | −0.063 | 1.30 | 0.78 | 0.0517 | −0.040 | 11.19 |
| 46 | CURACAO | - | 0.50 | - | - | - | 4.19 | −0.0060 | −0.074 | - |
| 47 | CYPRUS | 2.21 | 0.69 | −0.0056 | −0.131 | 1.30 | 0.45 | 0.0273 | −0.089 | 6.77 |
| 48 | CZECH | 2.40 | 0.16 | 0.2570 | −0.067 | 1.22 | 0.88 | 0.0474 | −0.197 | 7.65 |
| 49 | DENMARK | 1.60 | 0.80 | −0.0024 | −0.087 | 0.90 | 0.64 | 0.0092 | −0.048 | 10.07 |
| 50 | DJIBOUTI | 2.73 | 0.17 | 0.0144 | −0.094 | 1.47 | 0.36 | −0.0045 | −0.169 | 2.32 |
| 51 | DOMINICAN | 2.09 | 1.02 | 0.0309 | −0.088 | 1.10 | 1.57 | 0.0151 | −0.081 | 5.73 |
| 52 | DOMINICA | - | 7.75 | - | - | - | 0.67 | - | - | 6.59 |
| 53 | ECUADOR | 2.22 | 1.46 | 0.0157 | −0.140 | 1.18 | 1.14 | −0.0045 | −0.175 | 8.14 |
| 54 | EGYPT | 1.69 | 0.84 | 0.0527 | −0.042 | 1.33 | 0.51 | 0.0243 | −0.023 | 4.95 |
| 55 | EL SALVADOR | 1.58 | 1.70 | 0.0783 | −0.052 | 1.29 | 0.66 | 0.0535 | −0.113 | 7.11 |
| 56 | EQUATORIAL G. | 10.0 | 0.38 | 0.0454 | −0.190 | 2.41 | 1.48 | 0.0142 | −0.177 | 3.00 |
| 57 | ERITREA | 2.57 | 1.18 | 0.0083 | −0.216 | 0.74 | 0.80 | 0.0222 | −0.146 | 4.09 |
| 58 | ESTONIA | 2.10 | 0.87 | −0.0254 | −0.116 | 1.03 | 3.04 | 0.0279 | −0.099 | 6.69 |
| 59 | ESWATINI | 2.08 | 0.94 | 0.0317 | −0.071 | 1.34 | 0.71 | 0.0412 | −0.034 | 6.54 |
| 60 | ETHIOPIA | 2.42 | 0.80 | 0.1259 | −0.054 | 1.11 | 1.24 | −0.0041 | −0.136 | 3.30 |
| 61 | FIJI | - | 2.00 | - | - | 0.50 | - | - | 3.42 | |
| 62 | FINLAND | 1.66 | 1.14 | −0.0030 | −0.093 | 1.04 | 2.41 | −0.0010 | −0.119 | 9.04 |
| 63 | FRANCE | 2.68 | 1.17 | 0.2898 | −0.110 | 1.00 | 2.17 | −0.0096 | −0.081 | 11.26 |
| 64 | GABON | 1.83 | 0.97 | 0.0404 | −0.077 | 1.44 | 0.19 | 0.0187 | −0.143 | 2.75 |
| 65 | GAMBIA | 3.21 | 0.83 | −0.0026 | −0.094 | 2.29 | 0.37 | 0.0145 | −0.099 | 3.09 |
| 66 | GEORGIA | 2.19 | 1.23 | 0.2536 | −0.136 | 0.76 | 0.79 | 0.0293 | −0.057 | 7.11 |
| 67 | GERMANY | 2.84 | 0.73 | 0.2624 | −0.050 | 0.98 | 0.79 | 0.0050 | −0.195 | 11.43 |
| 68 | GHANA | 1.85 | 1.48 | 0.0463 | −0.099 | 1.09 | 0.62 | 0.0118 | −0.117 | 3.45 |
| 69 | GREECE | 1.72 | 0.71 | −0.0189 | −0.091 | 1.05 | 0.71 | −0.0111 | −0.069 | 7.72 |
| 70 | GRENADA | 5.78 | 14.00 | - | - | 1.08 | 0.10 | 0.0106 | −0.167 | 4.46 |
| 71 | GUADELOUPE | - | 1.35 | −0.0131 | −0.130 | - | 1.35 | −0.0084 | −0.137 | - |
| 72 | GUATEMALA | 1.67 | 0.25 | 0.0880 | −0.044 | 1.08 | 0.27 | 0.1109 | −0.197 | 5.71 |
| 73 | GUIANA FRENCH | - | 0.88 | 0.0391 | −0.102 | - | 0.43 | 0.0238 | −0.124 | - |
| 74 | GUINEA | 1.50 | 0.46 | 0.0097 | −0.111 | 1.36 | 1.68 | −0.0108 | −0.126 | 3.93 |
| 75 | GUINEA BISSAU | 3.56 | 1.14 | 0.0230 | −0.145 | 4.66 | 4.20 | - | - | 7.00 |
| 76 | GUYANA | 2.49 | 2.38 | 0.0005 | −0.152 | 1.54 | 4.23 | −0.0021 | −0.163 | 5.94 |
| 77 | HAITI | 2.32 | 0.60 | 0.0565 | −0.047 | 1.66 | 0.61 | 0.0217 | −0.082 | 7.69 |
| 78 | HONDURAS | 1.96 | 0.57 | 0.0532 | −0.086 | 1.59 | 1.64 | 0.0016 | −0.141 | 7.05 |
| 79 | HONGKONG | - | 0.04 | −0.0003 | −0.060 | - | 0.24 | 0.0285 | −0.041 | - |
| 80 | HUNGARY | 2.25 | 0.90 | 0.0018 | −0.093 | 0.77 | 1.93 | −0.0081 | −0.088 | 6.70 |
| 81 | ICELAND | 2.89 | 2.28 | −0.0261 | −0.056 | 1.86 | 0.66 | −0.0174 | −0.079 | 8.47 |
| 82 | INDIA | 2.43 | 0.98 | 0.0331 | −0.050 | 0.91 | 0.96 | −0.0151 | −0.048 | 3.54 |
| 83 | INDONESIA | 2.04 | 0.95 | 0.0391 | −0.071 | 1.07 | 0.99 | 0.0127 | −0.051 | 2.87 |
| 84 | IRAN | 3.61 | 1.04 | 0.2641 | −0.063 | 1.00 | 0.90 | 0.0438 | −0.140 | 8.66 |
| 85 | IRAQ | 1.81 | 0.77 | 0.1184 | −0.084 | 0.96 | 0.96 | 0.0410 | −0.150 | - |
| 86 | IRELAND | 2.63 | 2.16 | −0.0021 | −0.058 | 1.45 | 1.12 | 0.0188 | −0.057 | 6.93 |
| 87 | ISRAEL | 2.86 | 0.21 | −0.0047 | −0.049 | 1.33 | 1.16 | 0.0339 | −0.037 | 7.52 |
| 88 | ITALY | 2.99 | 1.04 | 0.2475 | −0.040 | 1.06 | 3.69 | −0.0057 | −0.072 | 8.67 |
| 89 | JAMAICA | 2.43 | 0.43 | −0.0031 | −0.089 | 1.22 | 2.47 | 0.0034 | −0.174 | 6.06 |
| 90 | JAPAN | 1.91 | 1.02 | 0.0872 | −0.055 | 1.21 | 1.16 | 0.0260 | −0.052 | 10.95 |
| 91 | JORDAN | 2.16 | 2.53 | −0.0006 | −0.155 | 0.93 | 0.93 | −0.0138 | −0.053 | 7.79 |
| 92 | KAZAKHSTAN | 2.85 | 0.60 | 0.0856 | −0.064 | 1.05 | 2.06 | 0.0933 | −0.210 | 2.92 |
| 93 | KENYA | 1.57 | 1.14 | 0.0413 | −0.067 | 1.26 | 1.18 | −0.0237 | −0.310 | 5.17 |
| 94 | KOREA REP. | 6.06 | 1.00 | 0.1664 | −0.076 | 0.90 | 1.04 | 0.0585 | −0.090 | 7.56 |
| 95 | KOSOVO | 1.90 | 1.02 | - | - | 0.82 | 0.99 | - | - | - |
| 96 | KUWAIT | 2.25 | 0.88 | 0.0687 | −0.031 | 1.27 | 1.10 | −0.0094 | −0.038 | 5.00 |
| 97 | KYRGYZSTAN | 2.27 | 0.17 | 0.0671 | −0.091 | 0.86 | 1.05 | 0.0271 | −0.200 | 6.53 |
| 98 | LAO PDR | - | 0.50 | - | - | - | 0.15 | - | - | 2.25 |
| 99 | LATVIA | 2.32 | 0.74 | −0.0179 | −0.087 | 1.10 | 0.50 | 0.0224 | −0.136 | 6.19 |
| 100 | LEBANON | 1.91 | 1.03 | 0.2286 | −0.112 | 1.27 | 0.90 | 0.0757 | −0.180 | 8.35 |
| 101 | LESOTHO | 1.99 | 7.08 | 0.0053 | −0.206 | 1.36 | 1.42 | 0.0398 | −0.087 | 9.28 |
| 102 | LIBERIA | 1.76 | 0.31 | 0.0151 | −0.114 | 3.08 | 4.56 | 0.0046 | −0.159 | 6.74 |
| 103 | LIBYA | 3.12 | 0.96 | 0.0493 | −0.047 | 1.09 | 0.79 | −0.0059 | −0.099 | - |
| 104 | LITHUANIA | 1.63 | 0.83 | 0.0394 | −0.096 | 0.98 | 2.49 | 0.0554 | −0.230 | 6.57 |
| 105 | LUXEMBOURG | 1.99 | 0.24 | −0.0401 | −0.061 | 0.83 | 1.48 | −0.0174 | −0.105 | 5.29 |
| 106 | MACAO | - | 0.29 | −0.0019 | −0.190 | - | - | - | - | |
| 107 | MADAGASCAR | 2.48 | 0.94 | 0.0377 | −0.057 | 1.54 | 0.75 | 0.0060 | −0.211 | 4.79 |
| 108 | MALAWI | 3.55 | 1.12 | 0.0478 | −0.088 | 1.66 | 6.46 | 0.0583 | −0.087 | 9.33 |
| 109 | MALAYSIA | 2.86 | 1.25 | 0.1042 | −0.101 | 1.15 | 1.30 | 0.0794 | −0.260 | 3.76 |
| 110 | MALDIVES | 1.96 | 0.83 | 0.0031 | −0.154 | 1.41 | 1.05 | 0.0007 | −0.116 | 9.41 |
| 111 | MALI | 1.61 | 0.64 | 0.0158 | −0.100 | 0.97 | 7.78 | 0.0148 | −0.115 | - |
| 112 | MALTA | 4.46 | 1.06 | 0.0712 | −0.114 | 1.29 | 0.99 | 0.0536 | −0.330 | 8.96 |
| 113 | MAURITANIA | 1.66 | 1.76 | −0.0033 | −0.055 | 0.82 | 1.14 | 0.0362 | −0.037 | 4.58 |
| 114 | MAURITIUS | 5.40 | 4.49 | −0.0209 | −0.120 | 9.32 | 0.35 | −0.0032 | −0.143 | 5.83 |
| 115 | MAYOTTE | - | 5.46 | 0.0129 | −0.103 | - | 1.05 | 0.0065 | −0.154 | - |
| 116 | MEXICO | 2.03 | 0.86 | 0.1759 | −0.100 | 0.98 | 2.53 | 0.0117 | −0.109 | 5.37 |
| 117 | MOLDOVA | 2.03 | 1.03 | 0.0324 | −0.086 | 0.83 | 0.36 | −0.0037 | −0.127 | 6.60 |
| 118 | MONACO | 5.48 | 3.15 | −0.0044 | −0.147 | 1.66 | 0.54 | 0.0134 | −0.136 | 1.60 |
| 119 | MONGOLIA | 3.12 | 10.25 | 0.0116 | −0.204 | 1.98 | 0.68 | 0.0195 | −0.127 | 3.79 |
| 120 | MONTENEGRO | 8.16 | 1.37 | −0.0114 | −0.171 | 1.07 | 0.66 | 0.0040 | −0.085 | 8.42 |
| 121 | MOROCCO | 2.05 | 0.90 | 0.1161 | −0.114 | 0.84 | 0.95 | −0.0159 | −0.065 | 5.31 |
| 122 | MOZAMBIQUE | 2.14 | 0.72 | 0.0260 | −0.109 | 1.59 | 0.70 | 0.0152 | −0.068 | 8.17 |
| 123 | MYANMAR | 2.70 | 1.12 | −0.0028 | −0.113 | 0.83 | 1.15 | −0.0137 | −0.050 | 4.79 |
| 124 | NAMIBIA | 2.10 | 0.68 | 0.0315 | −0.049 | 1.03 | 1.22 | 0.0315 | −0.039 | 7.95 |
| 125 | NEPAL | 2.28 | 0.74 | 0.2070 | −0.035 | 0.91 | 0.78 | −0.0264 | −0.065 | 5.84 |
| 126 | NETHERLAND | 2.40 | 1.19 | 0.2485 | −0.043 | 0.92 | 1.04 | 0.0002 | −0.074 | 9.97 |
| 127 | NEW CALEDONIA | - | 5.00 | - | - | - | 1.00 | - | - | - |
| 128 | NEW ZEALAND | 5.63 | 0.74 | −0.0426 | −0.087 | 1.89 | 0.72 | 0.0140 | −0.099 | 9.21 |
| 129 | NICARAGUA | 5.76 | 0.97 | - | - | 1.39 | 1.02 | - | - | 8.56 |
| 130 | NIGER | 2.58 | 0.63 | −0.0231 | −0.083 | 0.96 | 2.21 | 0.0390 | −0.048 | 7.33 |
| 131 | NIGERIA | 1.91 | 1.13 | 0.0502 | −0.046 | 1.06 | 1.02 | 0.0333 | −0.047 | 3.89 |
| 132 | MACEDONIA | 1.84 | 0.74 | 0.0858 | −0.092 | 0.87 | 0.74 | 0.0528 | −0.230 | 6.58 |
| 133 | NORWAY | 2.40 | 0.77 | 0.2716 | −0.055 | 1.14 | 2.13 | 0.0052 | −0.145 | 10.05 |
| 134 | OMAN | 1.73 | 3.70 | 0.0972 | −0.092 | 1.13 | 9.80 | 0.0936 | −0.130 | 4.13 |
| 135 | PAKISTAN | 1.90 | 1.22 | 0.1301 | −0.060 | 1.02 | 1.19 | 0.0113 | −0.047 | 3.20 |
| 136 | PALESTINE | - | 0.96 | −0.0053 | −0.202 | - | 1.06 | 0.0063 | −0.050 | - |
| 137 | PANAMA | 2.08 | 0.96 | 0.1443 | −0.063 | 1.13 | 0.79 | 0.1195 | −0.070 | 7.27 |
| 138 | PAPAU NEW G. | 1.95 | 0.49 | −0.0081 | −0.115 | 2.45 | 0.88 | - | - | 2.37 |
| 139 | PARAGUAY | 2.22 | 0.59 | 0.0196 | −0.147 | 0.97 | 1.20 | 0.0032 | −0.168 | 6.65 |
| 140 | PERU | 2.35 | 0.89 | 0.0915 | −0.010 | 1.26 | 0.53 | −0.0077 | −0.111 | 5.24 |
| 141 | PHILLIPPINES | 2.29 | 1.15 | 0.1627 | −0.082 | 0.91 | 1.54 | 0.1772 | −0.174 | 4.40 |
| 142 | POLAND | 2.17 | 0.92 | 0.1562 | −0.079 | 0.99 | 1.31 | 0.0094 | −0.072 | 6.33 |
| 143 | POLYNESIA | - | 0.66 | - | - | - | 0.21 | - | −0.075 | - |
| 144 | PORTUGAL | 2.92 | 1.56 | 0.0301 | −0.140 | 1.15 | 3.89 | 0.0431 | −0.190 | 9.41 |
| 145 | QATAR | 2.61 | 0.80 | 0.0694 | −0.070 | 1.16 | 1.03 | −0.0019 | −0.094 | 2.49 |
| 146 | ROMANIA | 2.26 | 0.88 | 0.0218 | −0.056 | 0.91 | 0.95 | −0.0072 | −0.121 | 5.56 |
| 147 | RUSSIA | 2.41 | 1.07 | 0.0775 | −0.020 | 1.00 | 0.87 | 0.0046 | −0.037 | 5.32 |
| 148 | RWANDA | 2.03 | 1.80 | 0.0615 | −0.146 | 1.26 | 0.14 | 0.0382 | −0.064 | 7.54 |
| 149 | SAO TOME | 3.09 | 1.44 | −0.0218 | −0.153 | 3.33 | 2.67 | 0.0162 | −0.127 | 6.27 |
| 150 | SAN MARINO | 5.88 | 5.10 | −0.0157 | −0.137 | 1.14 | 0.26 | −0.0028 | −0.154 | 7.14 |
| 151 | SAUDI ARABIA | 2.31 | 0.90 | 0.0607 | −0.060 | 0.90 | 0.98 | −0.0138 | −0.029 | 6.36 |
| 152 | SENEGAL | 2.02 | 0.72 | 0.0351 | −0.047 | 1.24 | 1.59 | 0.0387 | −0.047 | 3.98 |
| 153 | SERBIA | 2.13 | 1.62 | 0.0042 | −0.053 | 0.79 | 0.82 | 0.0123 | −0.038 | 8.54 |
| 154 | SEYCHELLES | 2.68 | 0.48 | - | - | 1.94 | 0.54 | 0.0313 | −0.134 | 5.11 |
| 155 | SIERRA LEONE | 1.50 | 2.23 | 0.0143 | −0.107 | 1.52 | 1.37 | 0.0291 | −0.063 | 16.06 |
| 156 | SINGAPORE | 2.06 | 1.33 | 0.0551 | −0.030 | 1.52 | 2.83 | 0.0641 | −0.080 | 4.46 |
| 157 | SLOVAK | 1.74 | 0.99 | −0.0286 | −0.123 | 0.92 | 0.74 | 0.0028 | −0.193 | 6.69 |
| 158 | SLOVENIA | 1.78 | 0.75 | −0.0345 | −0.079 | 1.08 | 0.64 | −0.0004 | −0.263 | 8.30 |
| 159 | SOLOMON ISL. | - | - | - | - | - | 0.29 | - | - | 4.47 |
| 160 | SOMALIA | 1.95 | 1.18 | −0.0085 | −0.091 | 2.55 | 1.49 | - | - | - |
| 161 | SOUTH AFRICA | 2.54 | 0.87 | 0.257 | −0.110 | 1.15 | 1.72 | 0.0303 | −0.039 | 8.25 |
| 162 | SOUTH SUDAN | 2.99 | 0.58 | 0.0007 | −0.152 | 1.59 | 0.51 | 0.0095 | −0.133 | 6.40 |
| 163 | SPAIN | 3.85 | 0.38 | 0.3350 | −0.035 | 1.16 | 0.79 | 0.0029 | −0.080 | 8.98 |
| 164 | SRI LANKA | 4.14 | 2.13 | 0.0144 | −0.159 | 1.04 | 1.07 | 0.1347 | −0.160 | 3.76 |
| 165 | ST KITTS NEVIS | - | 2.00 | - | - | - | 1.00 | - | - | 5.31 |
| 166 | ST LUCIA | 1.34 | 1.13 | - | - | 2.86 | 0.69 | 0.0157 | −0.082 | 4.40 |
| 167 | ST VINCENT | 5.86 | 0.04 | - | - | 2.17 | 2.00 | 0.0407 | −0.080 | 4.47 |
| 168 | SUDAN | 1.97 | 0.36 | 0.0193 | −0.094 | 0.24 | 1.63 | 0.0407 | −0.039 | 4.51 |
| 169 | SURINAME | 1.41 | 10.34 | 0.0214 | −0.061 | 1.27 | 1.21 | 0.0379 | −0.042 | 7.97 |
| 170 | SWEDEN | 2.10 | 0.56 | 0.2572 | −0.106 | 1.05 | 0.28 | 0.0123 | −0.162 | 10.90 |
| 171 | SWITZERLAND | 2.86 | 1.21 | 0.2388 | −0.044 | 0.95 | 0.18 | −0.0082 | −0.041 | 11.88 |
| 172 | SYRIA | 2.80 | 1.43 | 0.0311 | −0.030 | 1.06 | 0.66 | 0.0086 | −0.041 | - |
| 173 | TAIWAN | 3.42 | 1.88 | 0.0036 | −0.084 | 1.84 | 1.49 | 0.0053 | −0.123 | - |
| 174 | TAJIKISTAN | 1.68 | 1.02 | 0.0418 | −0.066 | 0.54 | 1.89 | −0.0016 | −0.131 | 7.24 |
| 175 | TANZANIA | 5.00 | 0.91 | 0.1205 | −0.125 | 18.4 | - | - | - | 3.63 |
| 176 | THAILAND | 3.42 | 0.69 | −0.0201 | −0.055 | 1.63 | 2.71 | 0.0496 | −0.100 | 3.79 |
| 177 | TIMOR LESTE | - | 5.00 | - | - | - | 1.33 | - | - | 4.33 |
| 178 | TOGO | 2.09 | 0.08 | 0.0093 | −0.084 | 1.41 | 1.14 | 0.0083 | −0.112 | 6.17 |
| 179 | TRINIDAD | 5.35 | 0.32 | −0.0025 | −0.139 | 1.30 | 0.55 | −0.0102 | −0.113 | 6.93 |
| 180 | TUNISIA | 2.64 | 1.53 | −0.0122 | −0.084 | 1.15 | 2.77 | 0.0053 | −0.117 | 7.29 |
| 181 | TURKEY | 4.32 | 1.15 | 0.0120 | −0.040 | 0.81 | 2.21 | 0.0078 | −0.030 | 4.12 |
| 182 | UAE | 2.33 | 0.97 | 0.0484 | −0.080 | 1.22 | 1.15 | 0.0085 | −0.055 | 4.23 |
| 183 | UGANDA | 2.18 | 0.95 | - | - | 0.88 | 0.64 | 0.0047 | −0.154 | 6.53 |
| 184 | UKRAINE | 2.16 | 0.96 | 0.0325 | −0.130 | 0.89 | 0.30 | −0.0032 | −0.093 | 7.72 |
| 185 | UK | 2.89 | 0.76 | 0.2223 | −0.037 | 1.25 | 1.03 | 0.0106 | −0.035 | 10.00 |
| 186 | USA | 3.85 | 8.42 | 0.2882 | −0.030 | 0.99 | 0.49 | 0.0121 | −0.060 | 16.89 |
| 187 | URUGUAY | 2.76 | 0.63 | −0.0228 | −0.086 | 1.15 | 1.03 | 0.0389 | −0.039 | 9.20 |
| 188 | UZBEKISTAN | 1.82 | 0.95 | 0.1231 | −0.088 | 0.71 | 0.90 | 0.0238 | −0.170 | 5.29 |
| 189 | VENEZUELA | 2.57 | 1.54 | 0.0389 | −0.073 | 0.94 | 0.82 | 0.0002 | −0.134 | 3.56 |
| 190 | VIETNAM | 3.59 | 3.29 | −0.0166 | −0.158 | 1.94 | 1.43 | −0.0040 | −0.158 | 5.92 |
| 191 | VIRGIN ISLANDS | - | 0.51 | - | - | - | 0.33 | - | - | - |
| 192 | WEST GAZA | 3.73 | 1.00 | - | - | 0.87 | 0.98 | - | - | - |
| 193 | YEMEN | 1.57 | 0.70 | 0.0049 | −0.164 | 2.84 | 1.50 | 0.0006 | −0.150 | - |
| 194 | ZAMBIA | 2.80 | 0.75 | 0.0265 | −0.134 | 1.73 | 1.12 | 0.0372 | −0.046 | 4.93 |
| 195 | ZIMBABWE | 1.98 | 1.44 | 0.0367 | −0.087 | 1.40 | 1.62 | 0.0438 | −0.045 | 4.73 |
References
- Worldbank. 2021. Available online: https://data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS (accessed on 12 February 2021).
- Worldometers. 2021. Available online: https://www.worldometers.info/coronavirus/ (accessed on 12 February 2021).
- Demongeot, J.; Oshinubi, K.; Seligmann, H.; Thuderoz, F. Estimation of Daily Reproduction Rates in COVID-19 Outbreak. MedRxiv 2021. [Google Scholar] [CrossRef]
- Renkulab. 2021. Available online: https://renkulab.shinyapps.io/COVID-19-Epidemic-Forecasting/_w_e213563a/?tab=ecdc_pred&country=France (accessed on 22 February 2021).
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Demongeot, J.; Flet-Berliac, Y.; Seligmann, H. Temperature decreases spread parameters of the new covid-19 cases dynamics. Biology (Basel) 2020, 9, 94. [Google Scholar] [CrossRef] [PubMed]
- Seligmann, H.; Iggui, S.; Rachdi, M.; Vuillerme, N.; Demongeot, J. Inverted covariate effects for mutated 2nd vs 1st wave Covid-19: High temperature spread biased for young. Biology (Basel) 2020, 9, 226. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.; Wang, X.; Li, Q.; Bragazzi, N.L.; Tang, S.; Xiao, Y.; Wu, J. Estimation of the Transmission Risk of the 2019-nCoV and Its Implication for Public Health Interventions. J. Clin. Med. 2020, 9, 462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.T.; Leung, K.; Bushman, M.; Kishore, N.; Niehus, R.; de Salazar, P.M.; Cowling, B.J.; Lipsitch, M.; Leung, G.M. Estimating clinical severity of COVID-19 from the transmission dynamics in Wuhan, China. Nat. Med. 2020, 26, 506–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griette, Q.; Demongeot, J.; Magal, P. A robust phenomenological approach to investigate COVID-19 data for France. Math. Appl. Sci. Eng. 2021, 2, 14031. [Google Scholar]
- Demongeot, J.; Noury, N.; Vuillerme, N. Data fusion for analysis of persistence in pervasive actimetry of elderly people at home. In Proceedings of the IEEE ARES-CISIS’ 08, Barcelona, Spain, 4–7 March 2008; pp. 589–594. [Google Scholar]
















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oshinubi, K.; Rachdi, M.; Demongeot, J. Analysis of Reproduction Number R0 of COVID-19 Using Current Health Expenditure as Gross Domestic Product Percentage (CHE/GDP) across Countries. Healthcare 2021, 9, 1247. https://doi.org/10.3390/healthcare9101247
Oshinubi K, Rachdi M, Demongeot J. Analysis of Reproduction Number R0 of COVID-19 Using Current Health Expenditure as Gross Domestic Product Percentage (CHE/GDP) across Countries. Healthcare. 2021; 9(10):1247. https://doi.org/10.3390/healthcare9101247
Chicago/Turabian StyleOshinubi, Kayode, Mustapha Rachdi, and Jacques Demongeot. 2021. "Analysis of Reproduction Number R0 of COVID-19 Using Current Health Expenditure as Gross Domestic Product Percentage (CHE/GDP) across Countries" Healthcare 9, no. 10: 1247. https://doi.org/10.3390/healthcare9101247
APA StyleOshinubi, K., Rachdi, M., & Demongeot, J. (2021). Analysis of Reproduction Number R0 of COVID-19 Using Current Health Expenditure as Gross Domestic Product Percentage (CHE/GDP) across Countries. Healthcare, 9(10), 1247. https://doi.org/10.3390/healthcare9101247