Abstract
Promoting active lifestyles among adolescents is essential due to their short-, medium-, and long-term contributions to young people’s holistic development and overall health. Beyond physical well-being, Physical Education foster physical activity, autonomy, social connectedness, motivation and emotional well-being, thus constituting a key dimension of quality education. Background/Objectives: The “Estilos de Vida Activos (EVA)” project is a school-based intervention designed to foster adolescent agency and motivation in adopting active habits. Grounded in the salutogenic model, self-determination theory, and the health-based Physical Education pedagogical model, this protocol describes the design and implementation strategies of a participatory intervention in secondary schools. Methods: A variety of research methods will be used to collect quantitative and qualitative data before, during, and after the intervention. Validated questionnaires will assess active commuting, socioeconomic status, satisfaction of basic psychological needs, motivation, levels and intention to engage in physical activity. Qualitative data include interviews with teachers, Photovoice sessions with students, observation notes, and programme materials. Intervention: The EVA intervention is collaboratively developed by students, teachers, and researchers using participatory action research. It includes needs analysis, participatory activities, and co-design of tailored physical activity programmes. The intervention is described using the Template for Intervention Description and Replication checklist (TIDieR) to enhance transparency and replicability. Conclusions: This protocol presents a theoretically grounded and participatory approach to school-based health promotion. By integrating educational and collaborative strategies, it offers a replicable model that promotes adolescent active lifestyles, from contextual relevance, and pedagogical coherence, serving as a guide for inclusive and sustainable interventions in school settings.
1. Introduction
Despite the well-documented benefits of physical activity (PA), a significant proportion of adolescents remain physically inactive. Globally, over 80% of adolescents fail to meet the World Health Organisation (WHO) PA recommendation of at least 60 min of moderate-to-vigorous physical activity per day [], and in Spain the situation is comparable, particularly among girls and older adolescents []. This public health concern has prompted the WHO’s Global Action Plan on PA 2018–2030, calling for coordinated, multisectoral interventions to increase PA participation [].
Schools are widely recognised as ideal environments for promoting PA behaviours due to their broad reach, structured routines, and influence from key social agents such as teachers, peers, and families []. Within these settings, Physical Education (PE) plays a key role in developing health-related knowledge, attitudes, and behaviours []. However, most school-based interventions have been designed within a biomedical paradigm that emphasises behaviour modification through prescriptive and often top-down methodologies [,]. Although some have reported short-term increases in PA [,,], their long-term effectiveness and behavioural transfer to adolescents’ daily lives remain questionable []. In this sense, the salutogenic perspective emerges as a more appropriate approach as it shifts the focus from disease prevention to the identification and mobilisation of individual and environmental resources that support health and well-being [,].
This lack of sustained impact may also be explained by the limited involvement of adolescents in the design and implementation of these interventions. Many continue to treat students as passive recipients rather than active contributors, resulting in programmes misaligned with their lived experiences, motivations, and contexts []. In contrast, participatory and asset-based approaches seek to empower youth by recognising their strengths, needs, and aspirations. These approaches privilege youth perspectives, grounded in children’s rights discourses—particularly Article 12 of the United Nations Convention on the Rights of the Child (United Nations, 1989)—which affirms their right to express views on matters affecting them [,]. According to Sandford et al. (2023) [], voice can be understood as how youth are able to communicate their thoughts and feelings and, in doing so, play an active role in society. This voice refers not only to verbal expression but also to diverse communicative forms, including art, writing, and even silence, acknowledging the varied ways youth articulate their experiences [,].
Then, schools aiming at promoting healthy lifestyles need to find strategies to involve students to discover their perspectives and to empower them for action. On one hand, it will respect their agency, i.e., active subjects, in understanding and influencing their behaviours and school context []. On the other hand, students are the real experts on their own lives and contexts, and their perspectives will provide pivotal information to design health promotion interventions []. In this sense, methods aimed to stimulate dialogue and to build shared meanings among equals are needed for enhancing self-driven learning process among children and adolescents [].
From this perspective, the salutogenic and positive approach to health development prioritises the creation of conditions that enhance personal growth, agency, and meaningful engagement in health-promoting activities, rather than focusing solely on the reduction in risk behaviours. In the context of adolescent health, this perspective underscores the importance of strengthening protective resources—such as resilience, perceived competence, and social connectedness—which are central to supporting the adoption and maintenance of active and healthy lifestyles [,]. This orientation aligns closely with contemporary pedagogical models in PE—such as health-based Physical Education (HBPE) []—which draw on the principles of Self-Determination Theory (SDT). Within adolescence, SDT provides a particularly valuable framework as it highlights the role of autonomy, competence, and relatedness in fostering intrinsic motivation and sustained behaviour change []. Recent contributions have also emphasised novelty as an additional psychological need that may be especially relevant during adolescence, a developmental stage characterised by the search for new and stimulating experiences []. Together, these theoretical perspectives inform educational approaches that seek to create enjoyable, meaningful, and transferable learning experiences, thereby fostering health-promoting behaviours within and beyond the school context []. In this sense, participatory action research (PAR) methodologies, such as Structured Interview Matrix (SIM) and Photovoice, have shown promise in enhancing student agency, generating contextually grounded knowledge, and co-creating interventions that are meaningful and feasible [,,]. These strategies have been successfully applied in school-based studies with adolescents [,], where they have supported the development of positive, realistic, and sustainable health practices by encouraging students to identify assets, share narratives, and reflect collectively [].
This article presents the protocol of the EVA (Estilos de Vida Activos; Active Lifestyles) project, a school-based pilot intervention co-designed and implemented with students and teachers in Spanish secondary schools. EVA was based on the SALVO project (Stimulating Active Lifestyles in Vocational Training), an initiative originally developed in the Netherlands to promote student agency in PA through participatory methodologies in secondary vocational education settings []. SALVO emphasises the importance of empowering students to shape meaningful PA experiences by recognising their personal assets and fostering autonomy. The EVA project adapts these principles to the Spanish educational context, integrating participatory action research (PAR) strategies within the PE curriculum to foster adolescents’ active participation in the promotion of healthy behaviours. Therefore, the central research question guiding this study is as follows: How can the participatory identification of health assets contribute to the design of school-based interventions that support adolescents in adopting, maintaining, and committing to more active and healthier lifestyles? Specifically, the objectives of the EVA project are (i) to support teachers and students in identifying and mobilising the health assets available in their contexts that facilitate the adoption of active and healthy lifestyles; (ii) to accompany participants in the planning, development, and evaluation of PA and health programmes from a participatory perspective; and (iii) to explore which elements participants consider transferable to their daily lives. Given the limited application of such approaches within curricular PE, this study could offer a relevant contribution by aligning with current international evidence-based recommendations on school-based health promotion policies [].
2. Materials and Methods
2.1. Study Context and Participants
The EVA project was implemented in two public secondary schools located in the Region of Valencia, Spain, as part of the PE curriculum during the 2020–2021 and 2021–2022 academic years. Participants included 130 students (aged 13 to 16), four PE teachers, and the two school management teams. The intervention was integrated into regular PE classes and approved by the school councils. Schools were selected through convenience sampling, following a prior teacher training programme in which several schools had participated. Two schools were chosen based on their willingness to engage more intensively in the project and the research team’s capacity to provide close follow-up, with the additional criterion of including one school located in a large urban area and another in a smaller municipality.
2.2. Overall Study Procedure
The intervention was developed collaboratively between the research team and the participating schools from October 2020 to May 2022 and included five main phases (see Figure 1). It comprised a series of co-designed, school-based activities aimed at promoting healthy lifestyles through active and participatory pedagogical strategies. Specifically, collaboration was embedded throughout the process and included (i) obtaining consent and offering a structured training programme, as well as several preparatory meetings to tailor the intervention to the context of each school, prior to implementation; (ii) jointly identifying health assets through SIM sessions; (iii) co-designing and implementing PA and health-related PE programmes; (iv) evaluating these programmes using PAR strategies; and (v) maintaining an ongoing dialogue between researchers, teachers and students through meetings, interviews and group discussions.
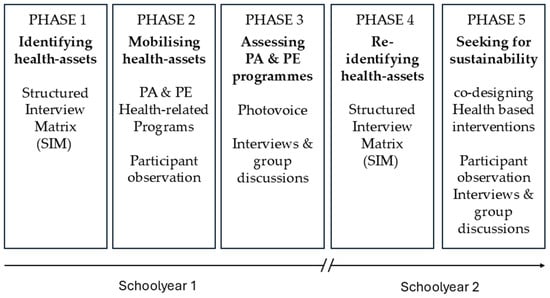
Figure 1.
EVA project intervention phases.
2.3. Research Design
To ensure a transparent, systematic and replicable description of the intervention, the Template for Intervention Description and Replication checklist (TIDieR) [] was employed (Table 1). This reporting guideline was specifically designed to improve the quality of intervention protocols, particularly in complex and context-dependent settings such as schools [,]. Unlike frameworks such as the Replicating Effective Programmes Framework (REP) [], which focus on the adaptation and implementation of previously validated programmes, TIDieR allows for a comprehensive description of novel interventions during their design and pilot phases []. It also serves as a structured guide to describe and implement the intervention components and was selected due to its suitability for participatory educational interventions that are still in the pilot phase of development. Therefore, it was considered the most appropriate framework to structure the methodology of the EVA project.

Table 1.
TIDieR checklist for the description and replication of the EVA project intervention (adapted from Hoffmann et al., 2014 []).
2.4. Research Instruments and Procedures
A variety of methods will be employed to gather data before, during, and after the intervention. Quantitative data will be collected at two time points: baseline (one week before the intervention) and post-intervention (one week after its completion) through validated questionnaires. All student participants will complete the questionnaires; teachers will not participate in this component. Specifically, basic psychological needs will be assessed using the Basic Psychological Needs in Exercise Scale (BPNES), adapted to Physical Education [], and complemented with items from the Novelty Need Satisfaction Scale (NNSS) []. Motivational regulation will be measured using the Spanish version of the Perceived Locus of Causality Scale (PLOC) [], while participants’ intention to engage in future PA will be assessed through an ad hoc 3-item questionnaire developed by the research team. PA levels will be assessed using the Spanish short version of the International Physical Activity Questionnaire (IPAQ) [], and active commuting habits will be evaluated through the Mode of Commuting to and from School Questionnaire []. Socioeconomic status will be determined through the Family Affluence Scale III (FAS III) []. Response scales varied across instruments, ranging from 5-point Likert scales (e.g., for BPNES and PLOC) to categorical frequency-based options (e.g., for IPAQ and commuting habits) (see Supplementary File).
Qualitative data will be collected using a range of complementary strategies to ensure methodological triangulation across data sources and participant groups, thereby enhancing the credibility and depth of the findings [,]. These will include semi-structured interviews with PE teachers conducted before and after the intervention, field notes recorded by researchers and facilitators during programme implementation, and group discussions with students following the Photovoice sessions. Interview and focus group guides will be structured around key themes including perceptions of health and PA, barriers and facilitators to engagement, experiences with the co-designed programmes and reflections on learning and empowerment. In addition, documentary materials—particularly the student portfolios and pedagogical tools developed throughout the intervention—will be analysed as artefacts to understand the learning processes and the relevance of the co-designed PA and health PE programmes.
2.5. Data Analysis Plan
Quantitative data will be analysed with SPSS version 28 (IBM, New York, NY, USA). Descriptive statistics will be used to summarise baseline characteristics and outcome variables. To assess changes between pre- and post-intervention measures, inferential tests such as repeated measures tests or their non-parametric equivalents will be applied, depending on data distribution. Analyses will be conducted separately for each participating school, and where appropriate, comparisons between schools will be explored to identify contextual differences. These analyses are aligned with the project’s objectives, particularly in evaluating the impact of co-designed programmes on students’ motivation, PA levels, and perceived transferability of learnings.
Qualitative data from SIM method, Photovoice murals, individual interviews and group discussions will be analysed using thematic analysis, following Braun and Clarke’s approach []. Coding will be performed inductively through NVIVO version 14. Emerging themes will be developed through iterative cycles of coding and discussion among the research team and contrasted with participants to enhance credibility. Given that the two schools implemented the EVA intervention in idiosyncratic ways, the study will employ a cross-case comparison to identify specific units of analysis and systematically explore similarities, differences, and emerging patterns. Following Stake’s approach to case study research [], this comparative analysis will include a vertical dimension in which the main features, contexts and processes of each case are examined in detail. This approach is particularly useful for understanding how contextual conditions, as well as teacher–student interactions and decision-making, shape the development and outcomes of the EVA intervention, thereby explaining variations in strengths and weaknesses between the two schools. To ensure the rigour of the research, strategies such as prolonged engagement, member checking, peer debriefing and methodological triangulation will be embedded throughout the study design and implementation.
2.6. Ethical Considerations
The study protocol was reviewed and approved by the Ethics Committee of the Universitat de València (UV-INV_ETICA-1189475). All participants (schools’ staff, students and their families) received detailed information about the study and provided written informed consent. Anonymity and confidentiality were guaranteed throughout the research process, and the intervention was aligned with the principles of equity, inclusion and voluntary participation. The participatory methods used in the EVA project were implemented with attention to power dynamics and the active involvement of students in shaping the process. In this regard, as mentioned above, students play a central role in the intervention and actively participate in all phases of the project: identifying health assets in their school and community, prioritising which assets to mobilise, co-designing and implementing physical activity and health programmes tailored to their needs, and reflecting on the transferability of acquired learning to their daily lives.
3. Discussion
3.1. Contextualising the EVA Project Intervention: Adaptation and Complementarity with the SALVO Project
The EVA project draws its foundational structure and inspiration from the Dutch SALVO initiative, a school-based health promotion intervention grounded in the salutogenic approach and PAR strategies such as the SIM and Photovoice []. The replication of effective interventions in different settings requires achieving a balance between fidelity to core elements and contextual adaptation [,]. In the case of EVA, fidelity was ensured by preserving the intervention’s participatory logic, health asset-based assessment and integration within the school community.
However, significant adaptations were necessary to integrate the programme into the Spanish educational context. Whereas SALVO operated at a whole-school level, EVA was designed to be embedded within the PE curriculum. This choice responds to the reality that in Spain—and particularly in the Valencian region—health promotion efforts in schools are still predominantly led by PE departments [,]. Starting within PE allowed the intervention to capitalise on existing structures and professional expertise while maintaining potential for future school-wide expansion. Furthermore, the use of PAR strategies was also adapted. While SIM was retained for identifying health assets, Photovoice was reconceptualised as a reflective evaluation tool during the implementation phase, allowing students to document and assess their own learning and behavioural changes. This use of visual and narrative inquiry aligns with the pedagogical potential of portfolios as tools for student reflection and engagement [,].
Overall, this flexible and context-sensitive approach reinforces the replicability of EVA in similar settings, supporting the idea that sustainable health promotion interventions require both fidelity to essential components and adaptive integration within specific cultural and curricular frameworks [,].
3.2. Methodological Contributions: Participatory Approaches in Educational Health Promotion
One of the most distinctive contributions of the EVA protocol lies in its use of participatory strategies that give voice to students and teachers as co-creators of health-promoting environments. Traditional health interventions have often prioritised biomedical frameworks; however, alternative approaches increasingly emphasise student agency and the co-construction of meaningful learning experiences. For instance, Whitley et al. [] highlighted how co-creation with marginalised youth in community sport-for-development programmes facilitated not only participation but also empowerment and positive identity formation. In school contexts, Casey and Goodyear [] demonstrated how pedagogical models that emphasise student agency and the co-construction of learning tasks can foster more autonomous and active identities. Complementing these approaches, Bachouri-Muniesa et al. [] developed a multilevel, multicomponent school-based intervention through a stakeholder-driven co-creative process, engaging teachers, families, and policymakers to enhance contextual adaptation, ownership, and sustainability. Collectively, these studies illustrate the growing importance of co-creation as a pedagogical and methodological principle in designing interventions that aim to nurture active identities in youth. In this sense, EVA aligns with this evolving paradigm by fostering collaboration and shared responsibility among educational stakeholders.
In particular, the EVA project is underpinned by pedagogical models such as HBPE [,], which integrates the principles of SDT [] to create motivational climates that support autonomy, competence, relatedness and novelty, four key psychological needs that underpin intrinsic motivation and long-term behavioural adherence []. Therefore, these models not only position health as a holistic construct embedded in the school curriculum, linking physical activity with students lived experiences and cultural contexts, but also provide a pedagogical framework for transforming PE into a meaningful, student-centred learning space. In fact, this approach is not only consistent with international health promotion frameworks [] but may also be regarded as a precursory initiative to the most recent Spanish guideline on Health-Promoting Schools [].
By involving students in identifying health assets and co-designing action plans, EVA not only promotes engagement and ownership but also enhances contextual relevance and cultural appropriateness. As supported by the recent literature, participatory methodologies are essential for generating long-term behavioural changes and building sustainable school health initiatives [,]. Furthermore, the integration of SIM and Photovoice supports deeper understanding of students’ perceptions and motivations, offering valuable insights for educators and policymakers alike. Based on a previous study [], both methods not only provided richer qualitative data but also fostered active student agency by creating safe and structured spaces, both within the school and in community settings, where adolescents could articulate their needs, values and experiences. Moreover, amplifying students’ voices empowers them to co-construct meaningful health-related knowledge, thereby strengthening the relevance and transferability of school-based interventions.
3.3. Potential of a Plurality of Research Method in School-Based Interventions
The adoption of a variety of research methods represents another strength of the EVA protocol. While quantitative data enable the measurement of behavioural changes, motivational profiles, and socioeconomic differences across diverse student groups, qualitative data provide contextual depth and explanatory power. This methodological complementarity allows for a more holistic understanding of how and why interventions succeed or fail in different settings [,].
The process evaluation component, incorporating students’ portfolios, teachers’ interviews, and observational data, serves not only to assess the implementation fidelity but also to capture the dynamic nature of behaviour change in adolescence. Moreover, the triangulation of data sources and informants—teachers, students and researchers—enhances the validity and credibility of findings and supports the transferability of the intervention to other educational contexts [,].
Nonetheless, future research directions could focus on the implementation of mixed-methods approaches which, as highlighted in the literature, not only enhance the rigour and adaptability of interventions but are particularly valuable for developing multicomponent, multilevel and context-sensitive strategies aimed at addressing the multifactorial nature of adolescent health behaviours [,].
4. Conclusions
This article has presented the protocol of the EVA project, a school-based intervention grounded in a salutogenic perspective and designed through active and participatory methodologies. By embedding health promotion within the PE curriculum, the project offers a context-sensitive and pedagogically sound approach that enhances student engagement and agency in promoting active lifestyles.
Beyond its methodological robustness, EVA represents a coherent and potentially replicable model of intervention tailored to the challenges of health promotion in secondary education. Its emphasis on student voice, interdisciplinary collaboration, and iterative development underscores its relevance for both educational practice and public health research.
At the same time, participatory methodologies also involve practical challenges, such as limited teacher availability, resistance to innovation, and fluctuating levels of student engagement. Recognising these constraints is key to strengthening the feasibility and impact of future interventions. Moreover, combining quantitative and qualitative approaches provides a comprehensive understanding of how such programmes operate and how they can be adapted to diverse educational contexts.
In sum, the EVA protocol offers a theoretically grounded and contextually adaptable framework for fostering active lifestyles in schools. Future research will evaluate its effectiveness and capacity to promote meaningful and sustainable behavioural change among adolescents, with the ultimate goal of informing broader educational and health policy initiatives.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/healthcare13182362/s1, File S1. EVA project research instruments.
Author Contributions
Conceptualization, J.L., and C.P.-V.; methodology, J.L., A.V.-P. and R.F.; validation, A.V.-P. and R.F.; resources: J.L., C.P.-V. and R.F.; writing—original draft preparation, J.L.; writing—review and editing, A.V.-P. and R.F.; supervision, C.P.-V.; project administration, J.L.; funding acquisition, J.L., A.V.-P. and C.P.-V. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Generalitat Valenciana. Conselleria d’Innovació, Universitats, Ciència i Societat Digital (grant number GV/2020/062) and Conselleria d’Educació, Investigació, Cultura i Esport (grant number BEST/2017/094).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki. This study has been approved by the Ethics Committee of the Universitat de València (ID reference: UV-INV_ETICA-1189475), approved on 7 November 2019.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data and procedures supporting the reported results are available upon request to the corresponding author.
Acknowledgments
We thank all the participating students, as well as teachers and headmasters who have helped us conduct this study. During the preparation of this work, J.L. used Chat GPT to improve the readability and language of the manuscript. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| WHO | World Health Organisation |
| PA | Physical Activity |
| PE | Physical Education |
| HBPE | Health-Based Physical Education |
| SDT | Self-Determination Theory |
| SIM | Structured Interview Matrix |
| PV | Photovoice |
| EVA | Estilos de Vida Activos (Active lifestyles) |
| PAR | Participatory Action Research |
| TIDieR | Template for Intervention Description and Replication |
| FITTPV | Frequency, Intensity, Time, Type of Activity, Progression and Variety |
| SALVO | Stimulating Active Lifestyles in Vocational Training |
| IPAQ | International Physical Activity Questionnaire |
| PLOC | Perceived Locus of Causality Scale |
| BPNES | Basic Psychological Needs in Exercise Scale |
| NNSS | Novelty Need Satisfaction Scale |
| FAS III | Family Affluence Scale III |
References
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1.6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Agencia Española de Seguridad Alimentaria y Nutrición (AESAN). Estudio ALADINO 2023: Alimentación, Actividad Física, Desarrollo Infantil y Obesidad en España; Ministerio de Derechos Sociales, Consumo y Agenda 2030: Madrid, Spain, 2024; Available online: https://www.observatoriodelainfancia.es/oia/esp/descargar.aspx?id=8793&tipo=documento (accessed on 30 June 2024).
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; WHO: Geneva, Switzerland, 2019; Available online: https://iris.who.int/bitstream/handle/10665/272722/9789241514187-eng.pdf (accessed on 14 September 2019).
- Bennett, A.E. Perspectives of primary school teachers on the capacity of schools to support post-pandemic health needs emerging among school-age children. Child Care Health Dev. 2024, 50, e13285. [Google Scholar] [CrossRef]
- Warburton, D.E.; Bredin, S.S. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Morgan, A.; Ziglio, E. Revitalising the evidence base for public health: An assets model. Promot. Educ. 2007, 14 (Suppl. 2), 17–22. [Google Scholar] [CrossRef] [PubMed]
- Nikooyeh, B.; Yari, Z.; Hariri, Z.; Baghdadi, G.; Yazdani, H.; Motlagh, M.E.; Neyestani, T.R. Which school-based interventions work better to combat obesity in children? A network meta-analysis. Syst. Rev. 2025, 14, 125. [Google Scholar] [CrossRef] [PubMed]
- de Meij, J.S.; Chinapaw, M.J.; van Stralen, M.M.; van der Wal, M.F.; van Dieren, L.; van Mechelen, W. Effectiveness of JUMP-in, a Dutch primary school-based community intervention aimed at the promotion of physical activity. Br. J. Sports Med. 2011, 45, 1052–1057. [Google Scholar] [CrossRef]
- Haerens, L.; De Bourdeaudhuij, I.; Maes, L.; Cardon, G.; Deforche, B. School-based randomized controlled trial of a physical activity intervention among adolescents. J. Adolesc. Health 2007, 40, 258–265. [Google Scholar] [CrossRef]
- Murillo-Pardo, B.; García-Bengoechea, E.; Generelo-Lanaspa, E.; Bush, P.; Zaragoza-Casterad, J.; Julián-Clemente, J.A.; García-González, L. Promising school-based strategies and intervention guidelines to increase physical activity of adolescents. Health Educ. Res. 2013, 28, 523–538. [Google Scholar] [CrossRef]
- Hynynen, S.; van Stralen, M.M.; Sniehotta, F.F.; Araujo-Soares, V.; Hardeman, W.; Chinapaw, M.J.M.; Vasankari, T.; Hankonen, N. A systematic review of school-based interventions targeting physical activity and sedentary behaviour among older adolescents. Int. Rev. Sport Exerc. Psychol. 2016, 9, 22–44. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. The salutogenic model as a theory to guide health promotion. Health Promot. Int. 1996, 11, 11–18. [Google Scholar] [CrossRef]
- McCuaig, L.; Quennerstedt, M. Health by stealth: Exploring the sociocultural dimensions of salutogenesis for sport, health and physical education research. Sport Educ. Soc. 2018, 23, 111–122. [Google Scholar] [CrossRef]
- Flavel, J.; Freeman, T.; Musolino, C.; Baum, F. Health promotion and the need to accelerate advocacy for health equity. Health Promot. Int. 2024, 39, daae040. [Google Scholar] [CrossRef]
- Lundy, L. ‘Voice’ is not enough: Conceptualising article 12 of the United Nations convention on the rights of the child. Br. Educ. Res. J. 2007, 33, 927–942. [Google Scholar] [CrossRef]
- Murdoch, D.C.; Mangiaracina, A.; Kefallinou, A. (Eds.) Voices Into Action—The Voices of Learners and Their Families in Educational Decision-Making: Literature Review; European Agency for Special Needs and Inclusive Education: Odense, Denmark, 2022. [Google Scholar]
- Sandford, R.; Hooper, O.; Chambers, F.C.; Schaefer, L. Navigating the challenging landscape of research with children and young people. In Research with Children and Young People in Physical Education and Youth Sport; Chambers, F.C., Sandford, R., Hooper, O., Schaefer, L., Eds.; Routledge: London, UK, 2023; pp. 3–15. [Google Scholar]
- Christensen, P.; James, A. Research with Children: Perspectives and Practices; Routledge: London, UK, 2008. [Google Scholar] [CrossRef]
- Hooper, O.; Sandford, R. Permission to speak freely? Facilitating young people’s voices in physical education and youth sport. In Proceedings of the International Association for Physical Education in Higher Education (AIESEP) Conference, Virtual, 7–10 June 2021. [Google Scholar]
- Lockyer, P.; Le Fevre, D.; Vickers, M. Implementation and sustainability of student peer-led physical activity programs in a school community. J. Prof. Cap. Community 2024, 9, 154–170. [Google Scholar] [CrossRef]
- Fricker, M. Epistemic Injustice: Power and the Ethics of Knowing; Oxford University Press: Oxford, UK, 2007. [Google Scholar]
- Boonekamp, G.M.; Dierx, J.A.; Van Hove, P.; Jansen, E. Interactive interviewing and imaging: Engaging Dutch PVE-students in dialogue. Educ. Action Res. 2020, 28, 807–822. [Google Scholar] [CrossRef]
- Bachouri-Muniesa, H.; Lhuisset, L.; Aibar, A.; Fabre, N.; Asún-Dieste, S.; Bois, J.E.; Zaragoza, J. Dissemination, implementation, and evaluation of an effective school-based intervention to promote physical activity in adolescents: A study protocol. Behav. Sci. 2023, 13, 290. [Google Scholar] [CrossRef]
- Bowler, M.; Sammon, P.; Casey, A. Health-Based Physical Education: A pedagogical model in focus. In Physical Education Pedagogies for Health; Cale, L., Harris, J., Eds.; Routledge: London, UK, 2023; pp. 62–67. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-determination theory. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer International Publishing: Cham, Switzerland, 2024; pp. 6229–6235. [Google Scholar] [CrossRef]
- González-Cutre, D.; Sicilia, Á. The importance of novelty satisfaction for multiple positive outcomes in physical education. Eur. Phys. Educ. Rev. 2019, 25, 859–875. [Google Scholar] [CrossRef]
- Hagger, M.S.; Cameron, L.D.; Hamilton, K.; Hankonen, N.; Lintunen, T. The Handbook of Behavior Change; Cambridge University Press: Cambridge, UK, 2020. [Google Scholar] [CrossRef]
- Oliffe, J.L.; Gao, N.; Fernandez, C.C.; Sha, M.; Yap, C.Y.; Sharp, P.; McKenzie, S. Participatory action research and knowledge dissemination in virtual photovoice: Methodological insights. Qual. Health Res. 2024, 12, 10497323241290956. [Google Scholar] [CrossRef]
- Boonekamp, G.M.; Jansen, E.; O’Sullivan, T.; Dierx, J.A.; Lindström, B.; Perez-Wilson, P.; Álvarez-Dardet Díaz, C. The need for adolescents’ agency in salutogenic approaches shaping physical activity in schools. Health Promot. Int. 2022, 37, daab073. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Burris, M.A. Photovoice: Concept, methodology, and use for participatory needs assessment. Health Educ. Behav. 1997, 24, 369–387. [Google Scholar] [CrossRef]
- Kaluzeviciute, G.; Jessiman, T.; Burn, A.M.; Ford, T.; Geijer–Simpson, E.; Kidger, J.; Limmer, M.; Ramsay, S.E.; Spencer, L. Participatory action research on school culture and student mental health: A study protocol. Int. J. Qual. Methods 2021, 20, 16094069211047753. [Google Scholar] [CrossRef]
- Boonekamp, G.M.; Dierx, J.A.; Jansen, E. Shaping physical activity through facilitating student agency in secondary schools in The Netherlands. Int. J. Environ. Res. Public Health 2022, 19, 9028. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, United Nations Educational, Scientific and Cultural Organization. Making Every School a Health-Promoting School: Implementation Guidance; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240025059 (accessed on 1 September 2025).
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Jallow-Badjan, H.; Bagnall, A.M.; Apekey, T.A.; Tunkara Bah, H.; Crookes, H.; Janha, R.E.; Health Secure Partnership consortium. The Health-Secure Partnership: Study protocol for the development of a school-& community-based intervention for promoting healthy nutrition among rural adolescents in The Gambia. PLoS ONE 2025, 20, e0327164. [Google Scholar] [CrossRef]
- Murcia, S.; Pastor-Pastor, X.; Lizandra, J. Investigando el Proyecto Educativo Strava: Un análisis desde las teorías motivacionales, la satisfacción de las necesidades psicológicas básicas y la intención de práctica de actividad física. Aula Abierta 2023, 52, 127–137. [Google Scholar] [CrossRef]
- Kilbourne, A.M.; Neumann, M.S.; Pincus, H.A.; Bauer, M.S.; Stall, R. Implementing Evidence-Based Interventions in Health Care: Application of the Replicating Effective Programs Framework. Implement. Sci. 2007, 2, 42. [Google Scholar] [CrossRef]
- Hudek, N.; Carroll, K.; Semchishen, S.; Vanderhout, S.; Presseau, J.; Grimshaw, J.; Brehaut, J.C. Describing the content of trial recruitment interventions using the TIDieR reporting checklist: A systematic methodology review. BMC Med. Res. Methodol. 2024, 24, 85. [Google Scholar] [CrossRef]
- Dahlgren, G.; Whitehead, M. Policies and Strategies to Promote Social Equity in Health; Institute for Future Studies: Stockholm, Sweden, 1991; Volume 27, pp. 4–41. [Google Scholar]
- Moreno, J.A.; González-Cutre, D.; Chillón, M.; Parra, N. Adaptación a la educación física de la escala de las necesidades psicológicas básicas en el ejercicio. Rev. Mex. Psicol. 2008, 25, 295–303. [Google Scholar]
- Moreno, J.A.; González-Cutre, D.; Chillón, M. Preliminary validation in Spanish of a scale designed to measure motivation in physical education classes: The Perceived Locus of Causality (PLOC) Scale. Span. J. Psychol. 2009, 12, 327–337. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Herrador-Colmenero, M.; Pérez-García, M.; Ruiz, J.R.; Chillón, P. Assessing modes and frequency of commuting to school in youngsters: A systematic review. Pediatr. Exerc. Sci. 2014, 26, 291–341. [Google Scholar] [CrossRef]
- Torsheim, T.; Cavallo, F.; Levin, K.A.; Schnohr, C.; Mazur, J.; Niclasen, B.; Currie, C.; FAS Development Study Group. Psychometric validation of the revised Family Affluence Scale: A latent variable approach. Child Indic. Res. 2016, 9, 771–784. [Google Scholar] [CrossRef] [PubMed]
- Denzin, N.K. The Research Act: A Theoretical Introduction to Sociological Methods; Aldine Publishing Company: New York, NY, USA, 1970. [Google Scholar]
- Stake, R.E. Investigación con Estudio de Casos; Morata: London, UK, 2020; Available online: http://digital.casalini.it/9788471127709 (accessed on 14 September 2019).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Card, J.J.; Solomon, J.; Cunningham, S.D. How to adapt effective programs for use in new contexts. Health Promot. Pract. 2011, 12, 25–35. [Google Scholar] [CrossRef]
- Hasson, H. Systematic evaluation of implementation fidelity of complex interventions in health and social care. Implement. Sci. 2010, 5, 67. [Google Scholar] [CrossRef]
- Valencia-Peris, A.; Pérez-Herráez, I.; Lizandra, J.; Pérez-Gimeno, E.; Moya-Mata, I. Needs and teacher training assessment for active school coordinators. In Proceedings of the 2PASS4HEALTH Congress—How to Get Your School Moving, Tarbes, France, 1–2 December 2022. [Google Scholar]
- Ministry of Education, Culture and Sport. Decree 107/2022, of August 5, Establishing the Organization and Curriculum of Compulsory Secondary Education. DOGV. 2022, 9403. Available online: https://dogv.gva.es/datos/2022/08/11/pdf/2022_7573.pdf (accessed on 12 June 2025).
- Johnson, R.S.; Mims-Cox, J.S.; Doyle-Nichols, A. Developing Portfolios in Education: A Guide to Reflection, Inquiry, and Assessment; SAGE Publications: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Whitley, M.A.; Massey, W.V.; Camiré, M.; Boutet, M.; Borbee, A. Sport-based youth development interventions in the United States: A systematic review. BMC Public Health 2019, 19, 89. [Google Scholar] [CrossRef] [PubMed]
- Casey, A.; Goodyear, V.A. Can cooperative learning achieve the four learning outcomes of physical education? A review of literature. Quest 2015, 67, 56–72. [Google Scholar] [CrossRef]
- Julián-Clemente, J.A.; Peiró-Velert, C.; Zaragoza-Casterad, J.; Aibar-Solana, A. Educación física relacionada con la salud. In Modelos Pedagógicos en Educación Física: Qué, Cómo, Por Qué y Para Qué; Universidad de León: León, Spain, 2021; pp. 178–226. Available online: https://dialnet.unirioja.es/servlet/libro?codigo=855350 (accessed on 2 April 2025).
- Ministry of Health; Ministry of Education, Vocational Training, and Sports. Guía de Escuelas Promotoras de Salud [Guide for Health-Promoting Schools]; Ministry of Health: Madrid, Spain, 2023. [Google Scholar]
- Herlitz, L.; MacIntyre, H.; Osborn, T.; Bonell, C. The sustainability of public health interventions in schools: A systematic review. Implement. Sci. 2020, 15, 4. [Google Scholar] [CrossRef]
- Corral-Abós, A.; Aibar, A.; Julián, J.A.; Zaragoza, J.; Ibor, E. Applying the intervention mapping protocol to promote active transport to school in primary school students: The ProATs intervention. Retos 2022, 46, 76–92. [Google Scholar] [CrossRef]
- Creswell, J.W.; Clark, V.L.P. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Mertens, D.M.; Bledsoe, K.L.; Sullivan, M.; Wilson, A. Utilization of mixed methods for transformative purposes. In SAGE Handbook of Mixed Methods in Social & Behavioral Research, 2nd ed.; Tashakkori, A., Teddlie, C., Eds.; SAGE: Thousand Oaks, CA, USA, 2010; pp. 193–214. [Google Scholar]
- Onwuegbuzie, A.J.; Leech, N.L. Validity and qualitative research: An oxymoron? Qual. Quant. 2007, 41, 233–249. [Google Scholar] [CrossRef]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E.; et al. A New Framework for Developing and Evaluating Complex Interventions: Update of Medical Research Council Guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef] [PubMed]
- Sevil-Serrano, J.; García-González, L.; Abós, Á.; Aibar Solana, A.; Simón-Montañés, L. Orientaciones para la comunidad científica sobre el diseño, implementación y evaluación de intervenciones escolares sobre promoción de comportamientos saludables. Cult. Cienc. Deporte 2020, 15, 507–517. Available online: https://zaguan.unizar.es/record/99219 (accessed on 2 April 2025).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).