
Home-Based Community Elderly Care Quality Indicators in China: A Systematic Literature Review
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
- Articles published in English or Chinese to capture local and international insights.
- Focused specifically on populations aged 60 years and older.
- Studies developing and implementing quantitative tools or instruments for measuring quality indicators of community eldercare in mainland China.
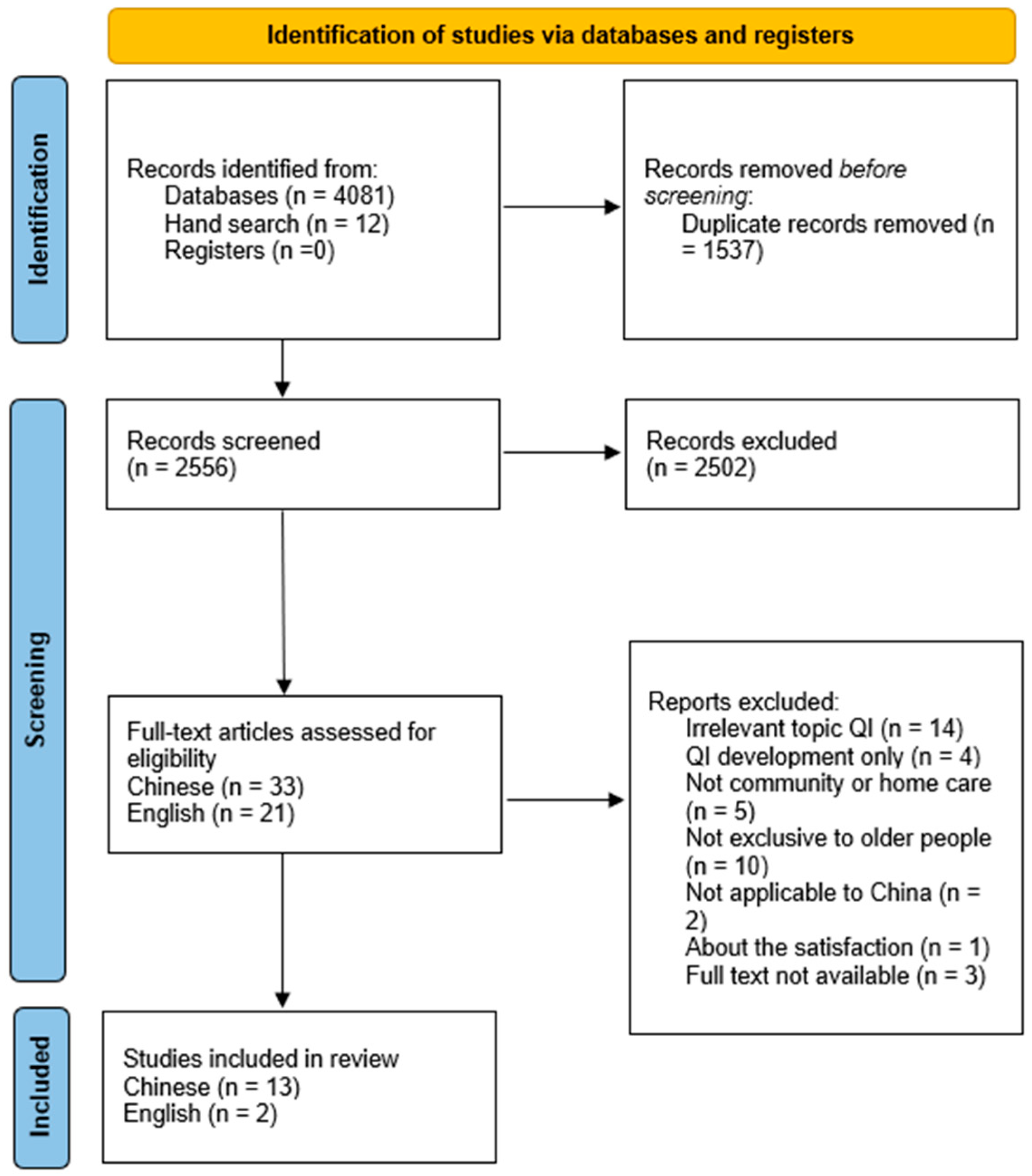
- Identification: Initial database searches yielded 4081 articles. An additional 12 articles were identified through reference list checks (snowballing technique). After removing duplicates, 2556 articles remained for further screening.
- Screening: Titles and abstracts of the 2556 articles were screened by one researcher. Of these, 2502 articles were excluded due to irrelevance or failure to meet the initial inclusion criteria.
- Eligibility: Full-text screening was conducted by two independent reviewers on the remaining 54 articles (33 Chinese, 21 English). Articles were excluded due to irrelevant topics, exclusive QI development without empirical testing, focus on non-community- or non-home-based care, non-exclusive focus on older people, not applicable to mainland China, satisfaction studies unrelated to quality indicators, and inaccessible full texts.
- Included: Fifteen quantitative studies met the inclusion criteria. Inter-reviewer agreement at the full-text inclusion stage was very high, achieving a kappa statistic of 0.83 [18].
2.3. Data Extraction and Analysis
2.4. Quality Assessment
2.5. Protocol and Registration
3. Results
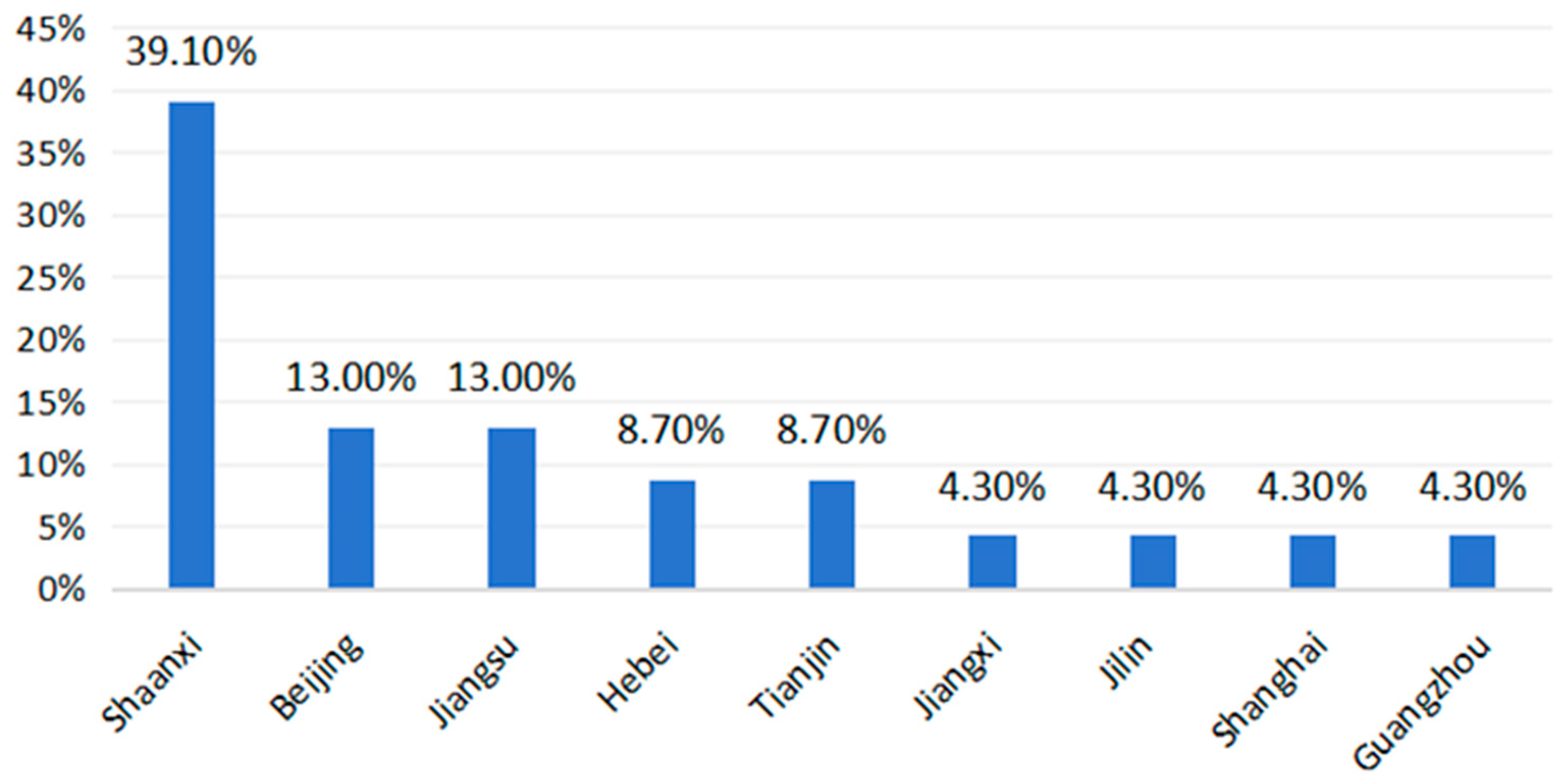
3.1. Geographical Distribution
3.2. Description of the Studies
3.3. Characteristics of the Quality Indicators
4. Discussion
4.1. Theoretical Foundations and Cultural Relevance
4.2. Integration with Healthcare Services
4.3. Methodological Approaches to Indicator Weighting
4.4. Scope and Application of Indicator Systems
4.5. Comparative Frameworks and International Standards
5. Conclusions
- Develop culturally grounded theoretical models that integrate local norms with internationally recognized best practices, ensuring relevance and global alignment.
- Expand and standardize indicator systems to include medical care components, safety tracking (e.g., fall rates), health outcomes, individual preferences, autonomy, care pathway integration, equity, and access.
- Utilize advanced methodological approaches combining subjective expert insights and objective data-driven strategies to improve the reliability and validity of evaluations.
- Include diverse stakeholder perspectives—elderly individuals, caregivers, healthcare providers, and management—and adopt mixed methods approaches for a more comprehensive and nuanced understanding of eldercare quality.
- Promote comparative evaluations both horizontally (across regions) and vertically (across service tiers), incorporating risk adjustment mechanisms to account for demographic and regional variations.
- Alignment with International Standards: Integrate elements from established international frameworks, such as the OECD’s long-term care quality indicators, to enhance comprehensiveness and facilitate global benchmarking.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HCEC | Home-based Community Elderly Care |
| Qis | Quality Indicators |
| CNKI | China National Knowledge Infrastructure |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| LTC | Long-term Care |
| AHP | Analytic Hierarchy Process |
| KPIs | Key Performance Indicators |
| SERVQUAL | Service Quality |
| SPO | Structure, Process, and Outcome |
Appendix A

{kind=link}
{kind=link}
| 1st Author, Year of Publication, Title | City/Region | Study Aim | Sample Size | Name of QI Set | Number of Indicators | Development and Validation Process of the QI Sets | Theoretical Model | Indicator Weighting Method |
|---|---|---|---|---|---|---|---|---|
| Xiaoqin Li 2016 [21] Fuzzy Comprehensive Evaluation of Aged Community Home Care Service Quality Based on AHP | Nanchang | To develop community home care QIs based on AHP | 20 communities | Fuzzy comprehensive evaluation of aged community home care QI set | Total: 25 Structure: 0 Process: 25 Outcome: 0 | 1. Development of CHC-QIs via extensive literature reviews, policy, and expert reviews 2. Selection and review of CHC-QIs 3. Empirical testing of QIs based on Nanchang aged community home care data | N/A | AHP |
| Jinrong Hu 2022 [22] An Evaluation Index System of Basic Elderly Care Services Based on the Perspective of Accessibility | Not specify a particular city in China | To develop basic elderly care QIs based on the Perspective of Accessibility | 20 experts | Fuzzy comprehensive evaluation of basic elderly care QI set (home-based community aged care, institutional aged care and administrative services) | Total: 24 Structure: 7 Process: 3 Outcome: 14 | 1. Development of BEC-QIs via extensive literature reviews, policy, and expert reviews 2. Selection and review of BEC-QIs | “5A” theoretical analysis framework of Penchansky and Thomas | AHP |
| Luo Yu 2018 [23] Construction of evaluation index system of geriatric pension services in community health service center under concept of integrated care | Not specify a particular city in China | To develop geriatric pension services in community health service center QIs based on AHP | 30 experts | QI set of geriatric pension services evaluation in community health service center | Total: 9 Structure: 3 Process: 4 Outcome: 2 | 1. Development of QIs via extensive literature reviews, policy, and expert reviews 2. Selection and review of QIs | N/A | AHP |
| Cai Zhonghua 2016 [24] The Quality Evaluation of Urban Community Elderly Care: Data Mining Based on Rough Set Method | Jilin | To develop urban community elderly care QIs based on rough set method | 1802 older people (>60) in 22 communities | Evaluation of urban community elderly care QI set | Total: 17 Structure: 0 Process: 17 Outcome: 0 | 1. Development of QIs via policy, and expert reviews 2. Selection and review of QIs 3. Empirical testing of QIs based on Jilin urban community elderly care data | N/A | Rough Set Method |
| Li Congrong 2019 [25] The quality of aged community home care services in Xi’an city from the perspective of the supply side | Xi’an | To develop community home care QIs based on fuzzy comprehension evaluation method | 100 communities | Fuzzy comprehensive evaluation of aged community home care QI set | Total: 26 Structure: 12 Process: 14 Outcome: 0 | 1. Development of QIs via policy 2. Selection and review of QIs 3. Empirical testing of QIs based on Xi’an community home care data | N/A | Fuzzy sets |
| Hao Li 2015 [37] Evaluation index system for community elderly care service development based on 3C elements | Tianjin | To develop community elderly care QIs based on 3C elements | N/A | Evaluation for community elderly care QI set based on 3C elements (life care, healthcare and social connection) | Total: 52 Structure: 34 Process: 15 Outcome: 3 | 1. Development of QIs via policy, and expert reviews 2. Selection and review of Qis | 3C (life care, healthcare and social connection) | N/A |
| Song Fengxuan 2014 [27] Urban community elderly care service quality evaluation and improvement strategies based on the SERVQUAL model | Baoding | To develop community elderly care QIs based on SERVQUAL model | 204 older people | Urban community elderly care evaluation QI set based on the SERVQUAL model | Total: 20 Structure: 4 Process: 8 Outcome: 8 | 1. Development of QIs via extensive literature reviews, and policy 2. Selection and review of CHC-QIs 3. Empirical testing of QIs based on Baoding aged community home care data | SERVQUAL model | N/A |
| Wen Haihong 2019 [28] Quality and Influencing Factors of Home-based Community Care Service-Based on Survey Data of Three Cities in Shaanxi | Xi’an, Baoji, Yan’an | 1. To develop home-based community care QIs based on SERVQUAL model. 2. Explore its influencing factors from five dimensions including system, economy, technology, personnel and individuals by using factor analysis and ordinal multiple logistic regression. | 324 older people (>60) | Home-based community care evaluation QI set based on SERVQUAL model | Total: 15 Structure: 3 Process: 6 Outcome: 6 | 1. Development of QIs via extensive literature reviews 2. Selection and review of QIs 3. Empirical testing of QIs based on Shaanxi aged community home care data | SERVQUAL model | N/A |
| Yong Lan 2018 [29] Access to Home Care Community Service for the Elderly: Conceptual Model, Index System and Comprehensive Evaluation | Beijing, Nanjing, Xianyang | To develop community elderly care accessibility indicators based on Penchansky & Thomas’s 5A model | 1465 older people (>60), Beijing (501), Nanjing (467), Xianyang (497) | Community elderly care accessibility indicators set based on Penchansky & Thomas’s 5A model | Total: 23 Structure: 6 Process: 4 Outcome: 13 | 1. Development of indicators via extensive literature reviews, policy, and expert reviews 2. Selection and review of indicators 3. Empirical testing of indicators based on Beijing, Nanjing and Xianyang aged community home care data | “5A” theoretical analysis framework of Penchansky and Thomas | AHP |
| Gan Lu 2023 [30] Research on the construction of evaluation index system for high-quality development of community home-based elderly care services | Not specify a particular city in China | To develop community home-based elderly care QIs based on SERVQUAL model | 19 experts | Community home-based elderly care evaluation QI set based on SERVQUAL model | Total: 36 Structure: 6 Process: 19 Outcome: 11 | 1. Development of QIs via extensive literature reviews, policy, and expert reviews 2. Selection and review of QIs | SERVQUAL model | Delphi method |
| Zhang Xiaoyi 2012 [31] Research on the community home care services for the elderly’s performance evaluation index system | Shanghai | To develop community home-based elderly care performance indicators based on 4E model (economy, efficiency, effectiveness, equity) | 12 experts | Community home-based elderly care performance evaluation indicators set based on 4E model | Total: 8 Structure: 0 Process: 6 Outcome: 2 | 1. Development of QIs via literature reviews and expert reviews 2. Selection and review of QIs | 4E model (economy, efficiency, effectiveness, equity) | AHP |
| Ma Duoduo 2023 [32] The Accessibility of Home-community Elderly Care Service and Its Influencing Factors | Yan’an, Baoji, Hanzhong, Nanjing, Wuxi | 1. To develop home-community care accessibility indicators based on Penchansky & Thomas’s 5A model. 2. Explore its influencing factors from four dimensions, including eldercare belief, personal resources, family resources, and community resources (Andersen’s behavioral model), by using SEM. | 773 older people | Home-community elderly care accessibility indicators set based on Penchansky & Thomas’s 5A model | Total: 23 Structure: 5 Process: 5 Outcome: 13 | 1. Development of indicators via extensive literature reviews 2. Selection and review of indicators 3. Empirical testing of indicators based on Yan’an, Baoji, Hanzhong, Nanjing, and Wuxi aged community home care data | Penchansky & Thomas’s 5A model | N/A |
| Xu Qiang 2019 [33] Assessment of performance and analysis of factors impacting the quality of community home elderly care services | Guangzhou | 1. To develop community home care QIs. 2. Using logistic regression, investigate the factors that affect eldercare satisfaction from two perspectives: environmental facilities and project content. | 586 older people | Community home elderly care evaluation QI set | Total: 5 Structure: 2 Process: 3 Outcome: 0 | 1. Development of QIs via extensive literature reviews and policy 2. Selection and review of QIs 3. Empirical testing of QIs based on Guangzhou aged community home care data | N/A | N/A |
| Wen Haihong 2017 [34] The Establishment and Application of the Evaluation System Concerning Community Elderly Care Policies -Take Xi’an as an Example | Xi’an | 1. To develop community home care indicators. 2. Using logistic regression, investigate the factors that affect eldercare satisfaction from two perspectives: environmental facilities and project content. | 12 experts, 290 older people | Assessment of the implementation indicators set of community elderly care policies | Total: 40 Structure: 9 Process: 10 Outcome: 21 | 1. Development of indicators via extensive literature reviews and policy, and expert reviews 2. Selection and review of indicators 3. Empirical testing of indicators based on Xi’an aged community care data | KPIs | Delphi method |
| Zhu Liang 2019 [35] Development of the Evaluation Index System of the Supply Service Quality of the Community-home Aged Care Center with Medical Care | Beijing, Tianjin, Hebei | To develop community home care with medical care QIs based on Delphi method | 23 experts | Evaluation of community home elderly care with medical care QI set | Total: 64 Structure: 24 Process: 29 Outcome: 11 | 1. Development of QIs via extensive literature reviews, policy, and expert reviews 2. Selection and review of QIs | SPO | Delphi method |
References
- World Population Prospects: Summary of Results. Available online: https://population.un.org/wpp/assets/Files/WPP2024_Summary-of-Results.pdf (accessed on 11 May 2025).
- Statistical Communiqué of the People’s Republic of China on the 2024 National Economic and Social Development. Available online: https://www.stats.gov.cn/sj/zxfb/202502/t20250228_1958817.html (accessed on 12 May 2025).
- Lodi Rizzini, C.; Maino, F.; De Tommaso, C.V. Ageing in Place, Healthy Ageing: Local Community Involvement in the Prevention Approach to Eldercare. Soc. Incl. 2024, 12, 1–12. [Google Scholar] [CrossRef]
- Su, B.; Li, D.; Xie, J.; Wang, Y.; Wu, X.; Li, J.; Prieto-Alhambra, D.; Zheng, X. Chronic disease in China: Geographic and socioeconomic determinants among persons aged 60 and older. J. Am. Med. Dir. Assoc. 2023, 24, 206–212.e5. [Google Scholar] [CrossRef]
- Chen, Y.; Ji, H.; Shen, Y.; Liu, D. Chronic disease and multimorbidity in the Chinese older adults’ population and their impact on daily living ability: A cross-sectional study of the Chinese Longitudinal Healthy Longevity Survey (CLHLS). Arch. Public Health 2024, 82, 17. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Chen, Y.; Zhang, L. Elderly people with disabilities in China. J. Am. Geriatr. Soc. 2019, 67, 858–859. [Google Scholar] [CrossRef]
- Peng, X. An analysis of the use of long-term care services for the disabled elderly in China—An empirical study based on the Anderson Health Behavior Model. Popul. Res. 2017, 7, 46–50. [Google Scholar]
- He, Y.; Wei, B. The impact of using community home-based elderly care services on older adults’ self-reported health: Fresh evidence from China. Front. Public Health 2023, 11, 1257463. [Google Scholar] [CrossRef] [PubMed]
- Ying, Y.; Dong, L.; Zhang, L.; Kong, F.; Yang, J.; Huang, X. Rural–urban differences in the association between home-based community care services satisfaction and mental health among older adults in Zhejiang, China. Front. Public Health 2024, 12, 1449670. [Google Scholar] [CrossRef]
- Asian Development Bank. Improving Home- and Community-Based Elder Care Service Delivery in the People’s Republic of China; Asian Development Bank: Manila, Philippines, 2023; Available online: https://www.adb.org/sites/default/files/project-documents/57102/57102-001-tar-en.pdf (accessed on 16 May 2025).
- Yao, X. Studying on the satisfaction degree of the urban elderly on community home-based care service and its influencing factors. Chin. Health Serv. Manag. 2021, 7, 496–498. [Google Scholar]
- Qing, L. The unique value, main mode and development policies of the community pension services. Acad. J. Zhongzhou 2016, 5, 77–83. [Google Scholar]
- Wen, H.; Zhang, Y.; Wen, C. The analysis on the status of Shaanxi urban community service for supporting the aged and the construction of its system: Based on Xi’an research. J. Northwest Univ. (Philos. Soc. Sci. Ed.) 2013, 43, 134–139. [Google Scholar] [CrossRef]
- Liu, Z.; Ouyang, C. Systematic review of Chinese and international research on service quality evaluation index systems of elderly care institutions. Chin. J. Health Policy 2020, 5, 72–81. [Google Scholar] [CrossRef]
- OECD. Health at a Glance 2023: OECD Indicators; OECD Publishing: Paris, France, 2023. [Google Scholar] [CrossRef]
- Kelley, E.; Hurst, J. Health Care Quality Indicators Project: Conceptual Framework Paper. In OECD Health Working Papers; No. 23; OECD Publishing: Paris, France, 2006. [Google Scholar] [CrossRef]
- Arah, O.A.; Westert, G.P.; Hurst, J.; Klazinga, N.S. A conceptual framework for the OECD Health Care Quality Indicators Project. Int. J. Qual. Health Care 2006, 18 (Suppl. S1), 5–13. [Google Scholar] [CrossRef] [PubMed]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar]
- Foong, H.Y.; Siette, J.; Jorgensen, M. Quality indicators for home- and community-based aged care: A critical literature review to inform policy directions. Australas. J. Aging 2022, 41, 383–395. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.; Schaffert, R.; Möckli, N.; Zúñiga, F.; Dratva, J. Home care quality indicators based on the Resident Assessment Instrument-Home Care (RAI-HC): A systematic review. BMC Health Serv. Res. 2020, 20, 366. [Google Scholar] [CrossRef]
- Li, X.; Wang, J. Fuzzy Comprehensive Evaluation of Aged Community Home-Care Service Quality Based on AHP. In Proceedings of the 2016 International Conference on Advances in Management, Arts and Humanities Science, Taichung, Taiwan, 10–11 December2016; pp. 109–113. [Google Scholar] [CrossRef]
- Hu, J.; Zhang, Y.; Wang, L.; Shi, V. An evaluation index system of basic elderly care services based on the perspective of accessibility. Int. J. Environ. Res. Public Health 2022, 19, 4256. [Google Scholar] [CrossRef]
- Luo, Y.; Wang, D.; Luo, Y. Construction of evaluation index system of geriatric pension services in community health service center under concept of integrated care. Nurs. Res. 2018, 67, 863. [Google Scholar]
- Cai, Z.; Wang, Y.; Dong, G. The Quality Evaluation of Urban Community Elderly Care: Data Mining Based on Rough Set Method. Popul. Econ. 2016, 4, 82–90. [Google Scholar]
- Li, C.; Liu, F. The quality of aged community home care services in Xi’an city from the perspective of the supply side. Chin. J. Gerontol. 2019, 12, 3059–3062. [Google Scholar] [CrossRef]
- Li, Y. Enlightenment of Western nursing theory construction on nursing theory research in China. Chin. J. Nurs. 2015, 50, 986–990. [Google Scholar]
- Song, F.; Ding, Y.; You, Y. Urban community elderly care service quality evaluation and improvement strategies based on the SERVQUAL model. Rev. Econ. Res. 2014, 52, 34–39. [Google Scholar]
- Wen, H.; Wang, Y. Quality and influencing factors of home-based community care service—Based on survey data of three cities in Shaanxi. J. Hebei Univ. (Philos. Soc. Sci.) 2019, 44, 139–148. [Google Scholar]
- Yong, L.; Wang, Z.; Zhang, D. Access to home care community service for the elderly: Conceptual model, index system, and comprehensive evaluation. Popul. Econ. 2018, 4, 1–11. [Google Scholar]
- Gan, L.; Zhou, L.; Xu, X. Research on the construction of evaluation index system for high-quality development of community home-based elderly care services. Chin. J. Health Policy 2023, 16, 40–47. [Google Scholar]
- Zhang, X.; Mei, Q. Research on the community home care services for the elderly’s performance evaluation index system. Stat. Decis. 2012, 24, 73–75. [Google Scholar]
- Ma, D. The accessibility of home-community elderly care service and its influencing factors—Empirical analysis based on survey data of two provinces of five cities. Soc. Secur. Stud. 2023, 2, 33–46. [Google Scholar]
- Xu, Q.; Zhou, Y. Assessment of performance and analysis of factors impacting the quality of community home elderly care services. J. Guangdong Inst. Public Adm. 2019, 5, 77–86. [Google Scholar]
- Wen, H.; Wang, Y. The establishment and application of the evaluation system concerning community elderly care policies—Take Xi’an as an example. Soc. Secur. Stud. 2017, 1, 14–22. [Google Scholar]
- Zhu, L.; Yang, X.; Zhang, Q.; Wang, F. Development of the evaluation index system of the supply service quality of the community-home aged care center with medical care. Chin. Gen. Pract. 2019, 22, 199. [Google Scholar]
- Donabedian, A. The quality of care: How can it be assessed? JAMA 1988, 260, 1743–1748. [Google Scholar] [CrossRef]
- Hao, L.; Yan, C.; Yang, X. Evaluation index system for community elderly care service development based on 3C elements. Chin. J. Gerontol. 2015, 24, 7281–7284. [Google Scholar] [CrossRef]
- Liu, X. Systematic evaluation of nursing quality evaluation index system in elderly care institutions. J. Nurs. Manag. 2017, 17, 156–159. [Google Scholar]
- Guo, H. Construction of service quality evaluation index system for elderly care institutions. Chin. J. Nurs. 2014, 49, 394–398. [Google Scholar]
- Han, Z. A method for determining index weight based on attribute value state. J. Kunming Univ. Sci. Technol. (Sci. Eng. Ed.) 2010, 35, 106–107. [Google Scholar]
- Wu, M. Research progress on the evaluation index system of nursing quality in elderly care institutions. Chin. J. Nurs. 2018, 53, 1127–1131. [Google Scholar]
- Tang, J. Service quality of elderly care institutions: Standards, management, and evaluation. Adm. Forum 2018, 25, 29–33. [Google Scholar]
- Guo, H. Comprehensive evaluation of service quality of 59 nursing homes in Beijing. Med. J. Chin. People’s Health 2014, 26, 1–4. [Google Scholar]
| ID | Author | Year |
|---|---|---|
| 1 | Xiaoqin Li | 2016 [21] |
| 2 | Jinrong Hu | 2022 [22] |
| 3 | Luo Yu | 2018 [23] |
| 4 | Cai Zhonghua | 2016 [24] |
| 5 | Li Congrong | 2019 [25] |
| 6 | Hao Li | 2015 [26] |
| 7 | Song Fengxuan | 2014 [27] |
| 8 | Wen Haihong | 2019 [28] |
| 9 | Yong Lan | 2018 [29] |
| 10 | Gan Lu | 2023 [30] |
| 11 | Zhang Xiaoyi | 2012 [31] |
| 12 | Ma Duoduo | 2023 [32] |
| 13 | Xu Qiang | 2019 [33] |
| 14 | Wen Haihong | 2017 [34] |
| 15 | Zhu Liang | 2019 [35] |
| Donabedian Model | Indicator Type | Quality Indicators | Articles 1 |
|---|---|---|---|
| Structure | Organizational characteristics | ∙ Financial resources (government funding, social assistance, and the proportion of general administrative expenses in total expenditure) ∙ Operating management of users (reasonable charging standards, personalized services, appointment system, formal service contracts and procedures, recording information of elderly individuals, complaint rate, implementation of preventive measures, emergency plan, implementation of government’s mandatory tasks, reports of accidents, supervise and feedback and evaluation system, information service system and database, WeChat platform, reputation, and visibility) ∙ Management of staff (receiving regular national inspection, providing staff training, clear service guidelines, service supervision and inspection mechanism, employee reward and punishment incentive mechanism, clear responsibilities of personnel, and complete rules and regulations) ∙ Older people (the elderly have the right to make decisions and participate in activities decision-making, the proportion of the elderly with pension) | 5, 9, 14, 15 |
| Infrastructure equipment | ∙ Basic facilities and equipment (walk assistant equipment, clean assistant, pager, safety protection measures and auxiliary use of notes, barrier free space, first aid facilities and equipment, numbers of beds, basic medical equipment, and observation room) ∙ Advanced facilities and equipment (spiritual comfort, fall prevention of corridors and stairs, emergency call system, information equipment, and smart bracelet) ∙ Timely inspection and maintenance ∙ The atmosphere of humanistic care | 2, 3, 5, 6, 8, 9, 10, 12, 13, 15 | |
| Environmental sanitation | ∙ The indoor environment (clean and comfortable, light and temperature and humidity are appropriate, the disinfection frequency, room layout is reasonable, and privacy) ∙ The surrounding environment (safe and quiet, the greening rate, the disinfection frequency, and accessibility of emergency traffic services) | 3, 7, 14, 15 | |
| Staff | ∙ Personal information (numbers, education background, welfare, contract of labor, turnover rate, satisfaction, and performance appraisal system) ∙ Work professionalism (professional certificate, professional knowledge and skills, professional dedication, warm respect for elderly individuals, trustworthy and patient and reliable, clean and tidy clothes, understand the needs of the elderly and their families, attach importance to the difficulties encountered by the elderly and are willing to help, provide services timely and actively and accurately, complete the promised services on time, safeguard the rights and dignity of elderly individuals, standardize the service process of the staff, and volunteer plan) ∙ Professional skills (psychological consultation and law assistant consultation) | 2, 5, 6, 7, 9, 10, 12, 14, 15 | |
| Community qualifications | ∙ Administrative license ∙ Food business license ∙ Medical qualification | 2, 14 | |
| Process | Day care and home care service | ∙ Day care (healthy and timely meal service from online and offline, walk assistant, laundry services, haircut and trim nails, transport assistant) ∙ Home care (laundry services, indoor cleaning, walk assistant, laundry services, haircut and trim the nails, wear clothes, assist toilet, emergency service, bath assistant service, number of baths per month, hotline service, full-time housekeeper service, elevator service, hourly worker service, milk delivery service, home care bed service, home appliance maintenance service, liquefied gas replacement services, and drains dredging services) | 1, 2, 4, 5, 7, 10, 13, 14, 15 |
| Entertainment services | ∙ Space (entertainment places, fitness facilities, outdoor area for activities) ∙ Outdoor activities (gentle sports, sight-seeing and tour) ∙ Cultural activities (reading, drawing, calligraphy, internet, cards, and handwork) ∙ Entertainment activities for the disabled elderly ∙ Records of entertainment activities | 1, 3, 4, 7, 13, 14, 15 | |
| Spiritual comfort | ∙ Communicate (company with the elderly and communicate with elderly individuals) ∙ Psychological (provide psychological counseling, evaluation of psychological problems of elderly individuals, formulation of psychological crisis intervention plan, degree of specialization of psychological counseling, and the number of psychological health lectures) ∙ Emotion (provide spiritual comfort services, emotional counseling, social meeting for single senior citizens services, hospice care services, and respect the cultural customs of the elderly and their families) ∙ Problems (incidence of insomnia, incidence of anorexia and hunger strike, incidence of self-abuse and suicide, and incidence of drug refusal) | 1, 4, 5, 7, 13, 14, 15 | |
| Elderly healthcare services | ∙ Nursing services (daily professional nursing services, acute disease nursing services, qualified rate of basic nursing, qualified rate of primary nursing, qualified rate of nursing staff with certificate, nursing station, nursing evaluation, grading nursing standards and grading nursing service specifications, qualified rate of nursing operative technique, correctly carry out relevant medical and nursing activities, rational use of drugs and home safety guidance services, assist the elderly to properly keep and use drugs according to the doctor’s advice, infection control, correct emergency treatment for common accidents or emergency, correctly assist the elderly to move their body position, correctly use wheelchairs and other walking aids, and medication guidance for chronic diseases) ∙ Health status (appearance, smell, clothes, mood, consciousness, weight monitoring, blood glucose monitoring, blood pressure monitoring, health risk assessment, reevaluation when the function changes, incidence rate of falls per year, incidence rate of other accidents per year, accurate record of physical condition, health record filing, and others in the minimum data set) | 1, 15 | |
| Combination of medical care | ∙ Basic treatment (outpatient treatment, drug injection, oral hygiene, dispensing medications, physical examination, patient compliance instruction, clear medical diagnosis, correct and effective treatment and nursing, health consultation, and basic emergency treatment) ∙ Further treatment (exclusive medical services, hierarchical diagnosis and treatment, timely contact and referral, comprehensive medical programs, whether it can diagnose and treat the severe elderly, whether it has built-in geriatric hospital, rehabilitation hospital, nursing home, and traditional Chinese medicine hospital or hospice care institution) ∙ Medical insurance (whether the built-in medical institution is included in the basic medical insurance and the proportion of the elderly with medical insurance) ∙ System of medical care (the convenience to apply for and obtain medical and nursing services, management and treatment and observation and record of chronic diseases, number of diseases that can provide medical services, two-week hospital visit rate, and whether the proportion of professional personnel is above 85%) | 1, 3, 4, 5, 6, 7, 13, 15 | |
| Rehabilitation healthcare | ∙ Facilities (the number of rehabilitation equipment, and rehabilitation healthcare room) ∙ Rehabilitation implementation (the elderly rehabilitation training (massage, exercise for power, physiotherapy), evaluate the elderly dysfunction, elderly rehabilitation guidance, postoperative rehabilitation nursing service, and rehabilitation activity times monthly) | 1, 3, 5, 13, 15 | |
| Education services | ∙ Health lectures (nutrition, regimen, prevention of common diseases, chronic disease, rehabilitation knowledge, and family care) ∙ Other lectures (law assistant, safety knowledge, and death education) ∙ Health education plans and implementation records, and the number of health education activities per year | 1, 4, 6, 14, 15 | |
| Accessibility | ∙ Distance and cost (community service center, elderly law assistant center, activity center, and elderly school) ∙ Convenience (community care and home care) ∙ Waiting time of appointment | 2, 9, 12 | |
| Outcome | Satisfaction | ∙ Satisfaction of environment (basic equipment, safety, public space, housing, and the planting of public area) ∙ Satisfaction of service (day care, healthcare, safeguard, cultural and sports, spiritual comfort, law assistant, charity, and staff and volunteer training) ∙ Satisfaction of emotion (community elderly culture, a sense of community, and social participation) ∙ Satisfaction of rights and interests protection ∙ Satisfaction of the elderly family members | 2, 3, 6, 12, 13, 14, 15 |
| Affordability | ∙ Day care (meal and walk assistant) ∙ Home care (meal, cleaning, and walk assistant) ∙ Healthcare ∙ Spiritual comfort ∙ Elderly association and elderly school | 2, 10, 12 | |
| Assessment | ∙ Completion rate ∙ Record ∙ Quality assessment and improvement | 3, 15 | |
| Expectation | ∙ Community service ∙ Community construction ∙ Community environment | 14 |
| OECD Indicator Domain | Typical OECD Indicators | Current Practice |
|---|---|---|
| Safety | Falls, pressure ulcers, avoidable hospitalizations | Limited focus; some mention of emergency plans, accident reports |
| Effectiveness | Pain management, functional status improvement | Some inclusion of health monitoring (e.g., BP and glucose); lacks systematic outcome tracking |
| Person-Centeredness | Satisfaction, respect for preferences, care planning | Satisfaction indicators present; few indicators on personalization or care plans |
| Coordination of Care | Health–social care integration, continuity of care | Rarely assessed; minimal integration of hospital and community data |
| Access and Equity | Timeliness, regional/economic disparities | Not systematically addressed; limited evidence of equity monitoring |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, X.; Ibrahim, R.; Lee, Y.F.; Hamid, T.A.; Chai, S.T. Home-Based Community Elderly Care Quality Indicators in China: A Systematic Literature Review. Healthcare 2025, 13, 1637. https://doi.org/10.3390/healthcare13141637
Chen X, Ibrahim R, Lee YF, Hamid TA, Chai ST. Home-Based Community Elderly Care Quality Indicators in China: A Systematic Literature Review. Healthcare. 2025; 13(14):1637. https://doi.org/10.3390/healthcare13141637
Chicago/Turabian StyleChen, Xi, Rahimah Ibrahim, Yok Fee Lee, Tengku Aizan Hamid, and Sen Tyng Chai. 2025. "Home-Based Community Elderly Care Quality Indicators in China: A Systematic Literature Review" Healthcare 13, no. 14: 1637. https://doi.org/10.3390/healthcare13141637
APA StyleChen, X., Ibrahim, R., Lee, Y. F., Hamid, T. A., & Chai, S. T. (2025). Home-Based Community Elderly Care Quality Indicators in China: A Systematic Literature Review. Healthcare, 13(14), 1637. https://doi.org/10.3390/healthcare13141637