1. Introduction
Handball is a team sport that places considerable physical demands on its players. It is a high-intensity game marked by rapid, high-impact movements, which significantly elevate the risk of musculoskeletal injuries, especially to the knee joint. During play, athletes engage in accelerations, directional changes, throws, jumps, and frequent physical contact, as noted in [
1,
2]. Sports injuries among basketball, handball, and volleyball players focused on frequency, nature, and gender/position variations. Lower limb injuries were most prevalent across all three sports. Basketball players commonly had knee and ankle injuries, handball players suffered knee injuries, and volleyball players sustained knee and foot injuries [
3]. These elements contribute to a high incidence of injuries associated with the sport [
4]. Handball injuries are prevalent, with knee and ankle injuries being the most common [
4,
5,
6]. The injury incidence is higher during matches compared to training, ranging from 11.1 to 23.5 injuries per 1000 match hours [
4]. Contact is the dominant injury mechanism, accounting for 51.4% of injuries [
7]. Previous injuries and increased match frequency are risk factors for overuse injuries, while being female and increased training hours are associated with traumatic injuries [
8]. Injury patterns differ between genders, with females reporting more serious injuries [
9]. Players in wing and pivot positions experience the highest rate of contact-related injuries [
7]. The injury incidence is higher in international competitions compared to national leagues [
9]. These findings emphasize the need for targeted injury prevention strategies in handball. Injury surveillance data from the European Handball Federation indicate that knee injuries account for approximately 18–24% of all injuries sustained in both professional and amateur matches. In addition, ligament injuries, especially those affecting the anterior cruciate ligament (ACL), have been reported with incidences as high as 0.82 per 1000 player hours, often resulting in prolonged rehabilitation or even premature career termination.
Despite the high prevalence of knee injuries in handball, detailed studies on diagnostic and therapeutic strategies specific to this sport remain scarce compared to other high-impact sports such as soccer or basketball. Magnetic resonance imaging (MRI) has emerged as a critical diagnostic tool due to its superior ability to delineate complex musculoskeletal trauma. MRI not only provides precise visualization of injuries affecting the knee joint but also aids in identifying pathologies in adjacent structures, such as the thigh muscles, hamstrings, adductors, and the accessory navicular.
The hamstring muscles—comprising the biceps femoris, semitendinosus, and semimembranosus—originate from the ischial tuberosity and function as antagonists to the quadriceps muscle, playing a vital role in knee flexion and hip extension while enhancing the biomechanical stability of both the coxofemoral and knee joints [
10]. Similarly, the adductor muscles, located in the medial compartment of the thigh, are essential for thigh adduction and pelvic stabilization, engaging intensely during pivots, accelerations, and rapid changes of direction inherent to handball.
The navicular, or tarsal scaphoid, is a key bone in the foot that supports the arch through the insertion of the tibialis posterior muscle, which acts as a strong adductor and supinator of the foot [
11]. The accessory navicular, an anatomical variant, is classified into three types: type 1 is small and round, residing within the posterior tibialis tendon; type 2 is larger and connected to the navicular via a cartilage bridge; and type 3 is the most prominent, fusing to the navicular bone via a bony bridge and forming a horn-shaped structure [
12].
Given the high incidence of these injuries and the critical role of early diagnosis in ensuring effective recovery, this study aims to evaluate the use of MRI in diagnosing handball-related musculoskeletal trauma and to assess the outcomes of conservative treatment approaches. We specifically focus on four case studies involving male players from the “Politehnica” Timișoara team, providing a detailed examination of injury patterns and the effectiveness of various conservative therapeutic interventions, despite the greater success of surgical therapy in this context.
4. Discussion
In this case series of elite handball players, MRI proved indispensable for the accurate diagnosis of high-impact musculoskeletal injuries that were either mischaracterized or undetected by initial clinical assessment and radiography. Across four distinct injury patterns—including vastus lateralis tears, proximal hamstring avulsions, adductor complex strains, and accessory navicular impingement—MRI not only enabled precise anatomical localization and severity grading but also guided the implementation of tailored conservative treatment protocols. These individualized approaches, comprising rest, NSAIDs, physiotherapy, and progressive kinesitherapy, led to full recovery and a timely return to play in each case. Our findings underscore the pivotal role of advanced imaging in optimizing non-operative management strategies for handball-related trauma and highlight the potential to reduce misdiagnosis and rehabilitative delays in high-performance sports.
Muscle tears are defined as a type of shear strain involving both myofibrils and the associated endomysial sheaths. They are classified as grades I, II, and III, according to the number of disrupted fibers. Grade I strains have few torn myofibers, with associated edema minor discomfort, and minimal loss of strength or range of motion. Grade II strains are characterized by clearly reduced strength due to the high number of torn myofibers, whereas grade III strains represent a complete tear of the muscle and myofascial sheaths, resulting in a complete loss of contractile function, often accompanied by a palpable injury [
13,
14].
Muscle damage can result in substantial hematomas due to the rupture of intramuscular vessels. Heamatomas are considered intramuscular if the epimysium contains the hematoma or intramuscular if the muscle fascia becomes discontinuous. Once the muscular fascia is torn, hematomas tend to fuse inside the adjacent anatomical regions.
Intramuscular hematomas are considered much more severe because the intact fascia leads to increased pressure, which compresses the capillary system as bleeding progresses, generating compartment syndrome with hypoxia and secondary muscle necrosis. Consequently, the prognosis for intramuscular hematomas is much more severe than that for intermuscular hematomas, and experts believe that they should be treated with extreme caution to avoid other complications such as traumatic ossifying myositis [
13,
14,
15].
The quadriceps muscle contains four muscle groups: vastus lateralis (originating from the lateral part of the intertrochanteric line, the margin of the greater trochanter, the lateral margin of the gluteal tuberosity, the lateral lip of the linea aspera), vastus medialis (originating from the medial part of the intertrochanteric line, pectineal line, medial lip of the linea aspera), vastus intermedius (originating from the proximal part of the anterolateral femoral diaphysis), and rectus femoris (with its two-headed tendon, the direct tendon inserted on the anterosuperior iliac spine, and the reflected tendon, inserted inferior and superior on the rim of the acetabulum). The four muscles converge in the occipital tendon, which contains the patella that forms the patellar tendon and is inserted into the tibial tuberosity. The four quadriceps muscle groups function as hip flexors and knee extensors [
16]. Eckard et al. reported the incidence of quadriceps muscle damage among college national association players, noting it was less common than hamstring injuries but three times more frequent among female players. During pre-season training sessions, non-contact injuries accounted for 63%, overexertion injuries made up 22%, and the relapse rate was approximately 7.2% in women’s basketball and men’s football [
17].
Isolated damage of the vastus lateralis has been reported in the literature as being more common in male players, and in cases of muscle avulsion, reinsertion surgery is recommended. It is relevant that female players seem to have different degrees of muscle damage risk compared to male players, due to anatomical and biomechanical differences [
18].
Souza et al., Voight et al. and Cowan et al. suggested, based on electromyography studies, that the altered contractile models of the quadriceps can perturb the dynamic of the patellofemoral joint. LaBore and Weiss suggested that damage to the vastus lateralis impairs the dynamics of the patellofemoral joint. Conservative treatment includes kinetotherapy; however, prophylaxis is the most important treatment, mainly for professional sportspeople. One of the protocols used was the one published by Daneshjoo et al., who recommended both the FIFA +11 and the prevention programs of the HarmoKnee training exercises that combine strength, neuromuscular control, balance, and correct kinematic models without resorting to special equipment, focusing mainly on the isometric strength of the quadriceps [
19,
20,
21,
22].
Special attention should be paid to muscle damage acquired during professional sports and an approach should be developed based on the prophylaxis and management of these injuries, including gender-specific training programs, biomechanical assessment, and personalized recuperation strategies [
23].
Muscle injuries are common among both genders, yet physiological and biomechanical differences call for gender-specific training programs. In elite athletes, the ACL is frequently injured, with females being significantly more susceptible up to eight times more likely than males [
24]. Male athletes, on the other hand, tend to experience more hamstring injuries due to their increased muscle mass during high-intensity sports [
25].
Gender-specific training programs should focus on:
Female athletes: Emphasize knee stabilization exercises, neuromuscular control drills, and balance training to reduce valgus forces. Plyometric exercises can improve knee stability. Training intensity should consider menstrual cycle-related hormonal factors.
Male athletes: Focus on hamstring strengthening, particularly eccentric exercises like Nordic hamstring curls, alongside agility drills to improve muscular endurance and flexibility.
Regular biomechanical assessments should be conducted to identify movement patterns that may lead to injury, including gait analysis and functional movement screening during high-stress activities.
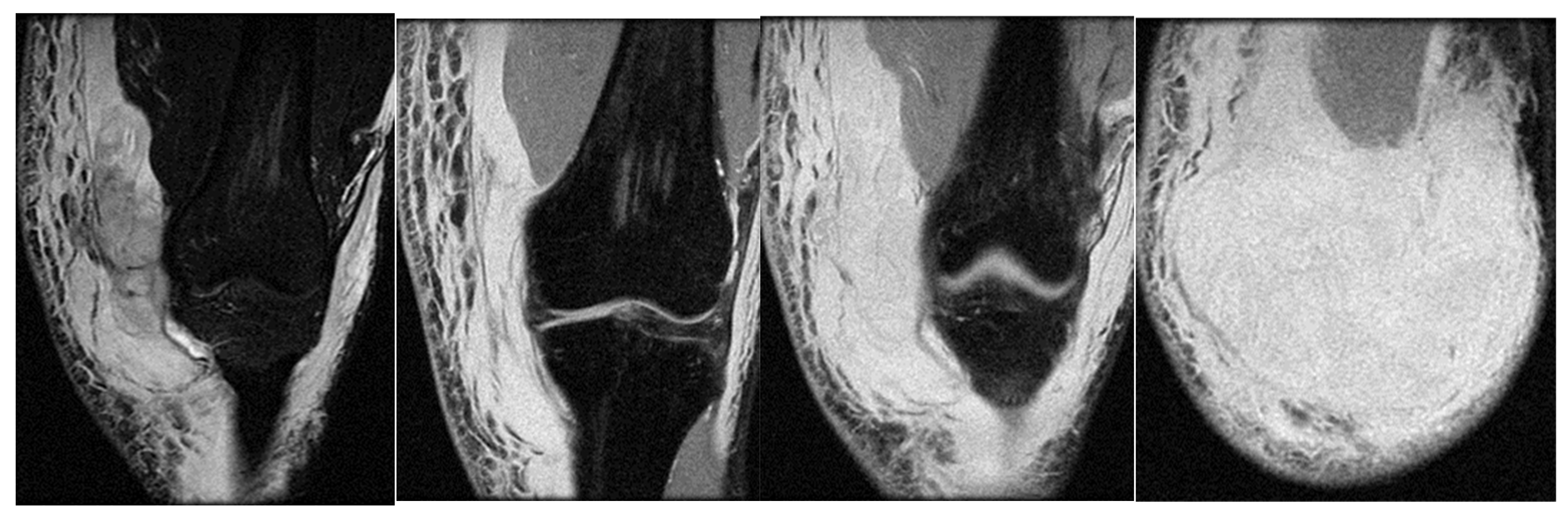
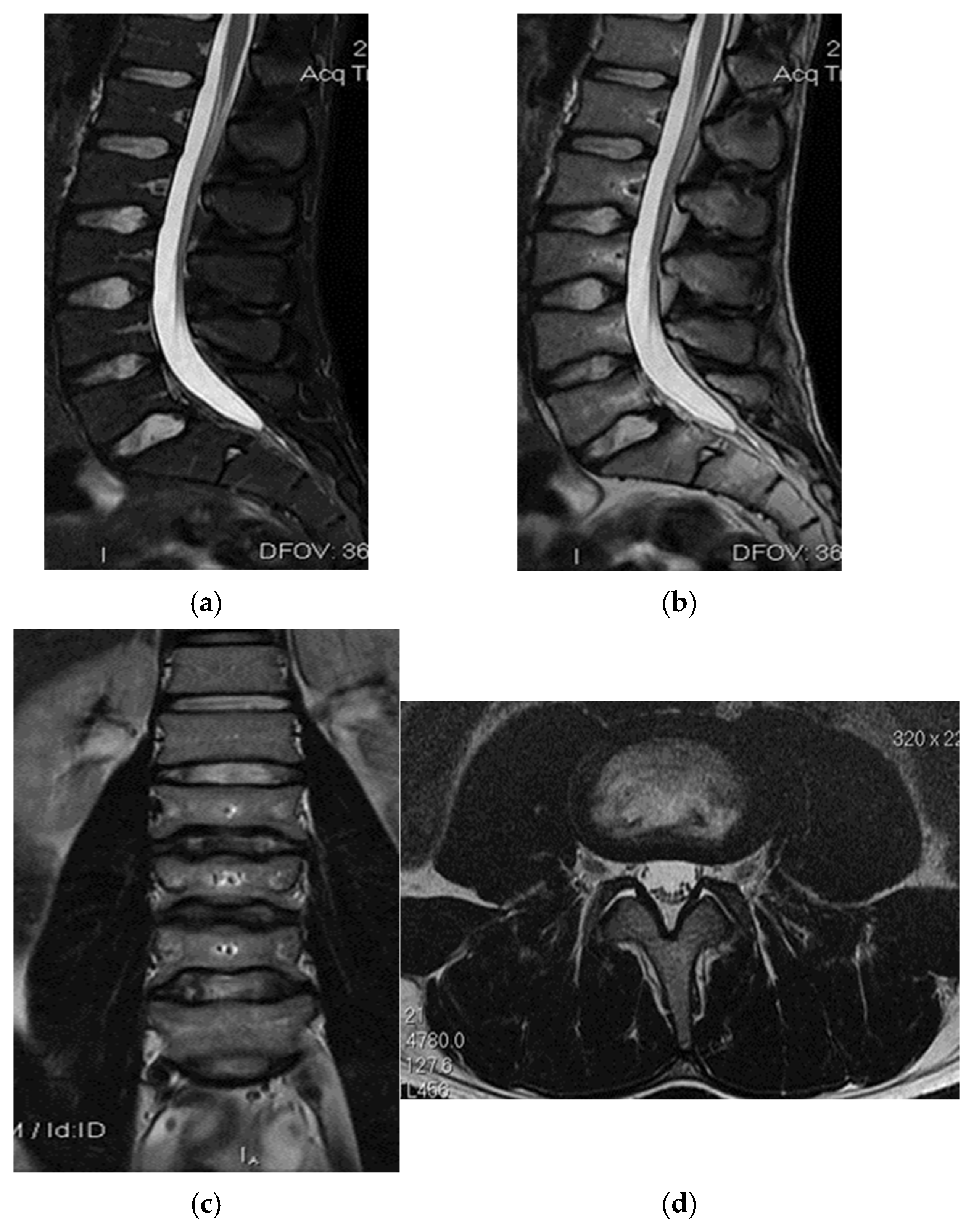
The ischial calf muscles contribute to hip extension, pelvic stabilization, and knee flexion [
26]. In sportspeople, damage to the ischial-calf muscles is the most common type of injury, and its incidence ranges between 3 and 4.1/1000 h of competition. Injuries may vary from muscle elongation to complete tendon tears and are most common at the musculotendinous junction. Among all ischial-calf damage cases, proximal avulsion occurred in 12%, and complete avulsion occurred in 9%. These injuries are treated conservatively using functional recuperation if the retraction is <2 cm or if a single tendon is involved. However, surgery is recommended when the damage involves two or more tendons and retraction is greater than 2 cm [
27,
28].
Injuries to the proximal part of the ischial calf muscles, which are more common in teenagers and less frequent in adults, can lead to avulsion fractures of the ischial tuberosity. While these injuries are typically managed conservatively, similar to adults with purely tendinous damage, surgery is preferred when there are tears with significant secondary retraction. In acute injuries, surgical management usually consists of open reduction and internal fixation (ORIF) of fractures. In certain cases, these injuries can be mistakenly diagnosed, leading to delayed care and, subsequently, to a chronic lack of consolidation [
29].
In the case of chronic unconsolidated lesions, conservative treatment can be initiated, including nonsteroidal anti-inflammatory drugs, physical therapy, and progressive resumption of activity. If this approach fails, then surgery should be considered [
29].
Avulsion fractures of the ischial tuberosity are rare injuries that usually occur in players with immature skeletons as a consequence of the eccentric contraction of the ischial-calf muscles caused by sudden and forced flexion of the hip while the knee is extended. Untreated fractures with displacement lead to the development of pseudoarthritis and fibrosis of the proximal ischial calf muscles, resulting in chronic pain, a reduced range of active and passive movements, and altered locomotor biomechanics. The number of reported cases of surgical fixation for these fractures is low. Bone plate fixation offers a stable result but usually requires an extensive Kocher–Langenbeck approach, with possible subsequent damage to the femoral head and blood vessels of the proximal femoral epiphysis. Biodegradable suture anchors can also be used, but failed cases have been reported because of weakening of the suture. Cannulated screws are an alternative with a higher success rate in acute injuries where the displacement of the avulsion fragment is less than 15 mm. However, the results of delayed surgery were less effective than those of immediate posttraumatic fixation [
30].
Ferlic et al. described the successful use of three 4 mm cannulated screws in fractures with ischial tuberosity displacement, with immediate post-trauma surgery using a transversal incision, with the patient lying on their side. They reported a case of ischial tuberosity avulsion in a 14-year-old patient who underwent surgery 12 months after the initial injury. Postoperatively, the patient continued to feel pain while sitting, and was never able to resume his sporting activity. Patients with a displacement of <15 mm were treated conservatively, with excellent results [
30]. Kaneyama et al. described the use of two 4 mm cannulated screws using a subgluteal approach to successfully treat an acute ischial tuberosity fracture in a 16-year-old patient at a 3-hour interval post-injury. The sciatic nerve was not exposed directly. The recovery time necessary to fully resume sporting activity was 4 months. An alternative approach to avoid metal insertion involves the use of biodegradable suture anchors. Biedert et al. described this technique in three players with ischial tuberosity avulsion fractures during training. However, of the three players, one failed because of suture deterioration [
31].
Most authors agree that displacements greater than 15 mm require surgical treatment for ischial tuberosity avulsion fractures, with possible complications entailed by conservative treatment in these patients, including pseudoarthritis and chronic pain secondary to leg shortening and fibrosis at the origin of the ischial calf muscles, with the impossibility of sitting down for longer periods of time. However, the type of surgery best suited for these cases remains a matter of debate [
30,
32].
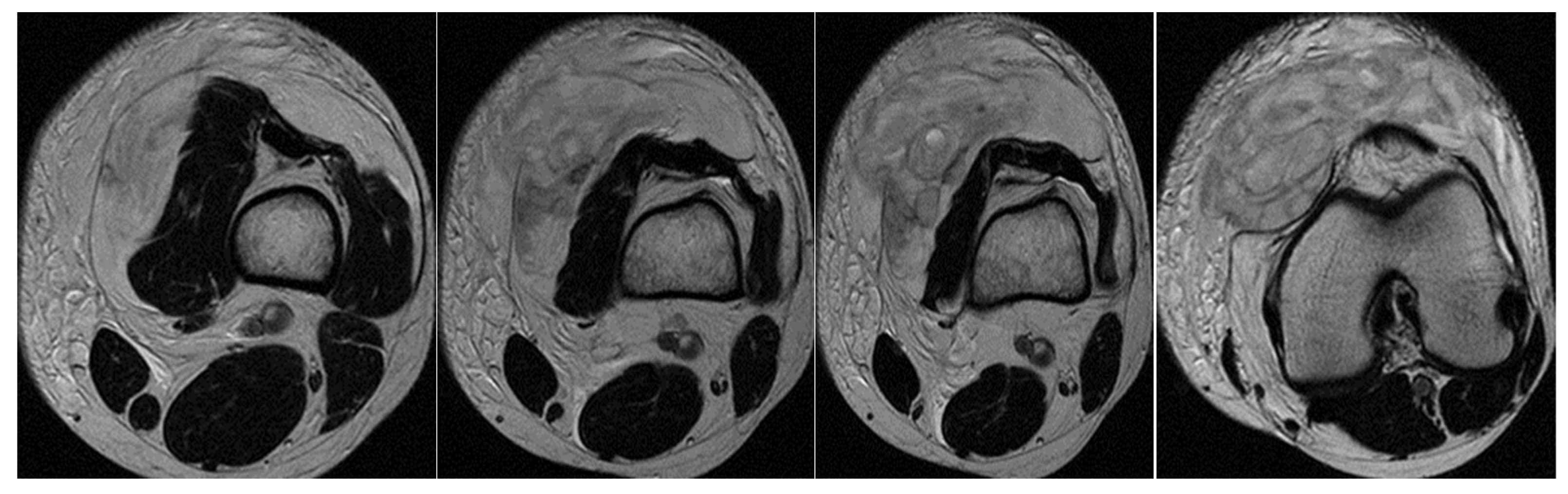
The adductor brevis muscle is part of the adductor muscle group, which also includes the pectineus, adductor magnus, gracilis, and adductor longus. The pectineus, adductor brevis, and adductor longus are collectively known as the “short adductors,” connecting the pelvis to the femur. In contrast, the gracilis and adductor magnus, referred to as the “long adductors,” extend from the pelvis to the knee. The main function of these muscles is to bring the pelvic limbs closer together. They also act while sprinting, twisting, or hitting objects.
The adductor brevis originates on the anterior surface of the inferior pubic branch, which is inferior to the origin of the adductor longus. It was inserted into the pectineal line to the superior part of the medial lip of the linea aspera. It is innervated by the branches of the obturator nerve. The obturator and medial femoral circumflex arteries ensured the necessary blood supply to the muscle. Its function is to adduct and flex the thigh and to contribute to lateral rotation [
33].
The adductor magnus, pectineus, adductor longus, and adductor brevis muscles can perform both interior and exterior rotations of the thigh. Their rotation function depends on the specific flexion–extension and abduction–adduction positions of the hip joint. Flexion and abduction intensify the lateral rotation function of these muscles, while extension and adduction intensify the medial rotation function.
Clinically, the muscle strain of the adductor group of muscles was as follows: grade 1, slight discomfort, slight sensitivity at a certain point, no swelling; grade 2: greater pain, swelling, tenderness to palpation, reduced movement amplitude, and impaired running; grade 3: very painful, increased swelling, and total loss of running or even walking capability [
34].
The commonest causes of pain in the inguinal area are described as being connected to the adductors, the iliopsoas, and inguinal muscles. However, external rotator muscle injuries can also cause pain in the inguinal area and should be considered. Several mechanisms of the damage have been described, but none are very specific, and the injuries described more often involve movements made by the player: swift and unstable changes in speed and load associated with flexion and internal rotation. Despite the various mechanisms described, this damage is believed to develop because of attempts to stabilize the hip during a stressing activity that involves a combination of forces that act on the coxofemoral joint [
33,
34].
In most cases, players with injuries of the external obturator complain of pain in the anterior part of the hip and rarely of pain in the gluteal region, which could result from any other pathology more common than external obturator damage. This type of injury is often misdiagnosed as injury of the adductor muscles due to the location of the pain that can be connected to the joint innervation of these muscles by branches of the obturator. The most suggestive clinical sign is considered acute or subacute pain in the anterior hip, triggered by instability in highly demanding sports, associated with pain during passive rotation of the hip or against hip resistance at 90
° flexion. Another important characteristic is the absence of pain on palpation, because the external obturator is located deep. Despite these characteristics, clinical diagnosis remains a challenge, and ultrasound seldom has sufficient resolution to provide a correct diagnosis. Consequently, MRI is the gold standard for properly assessing the location and severity of the damage. The clinical signs and physical examination findings are non-specific; therefore, diagnosis is ultimately a diagnosis that excludes the most common causes. It requires a well-documented presumptive clinical diagnosis as well as MRI confirmation [
35,
36].
There is currently no established consensus on rehabilitation protocols for muscle damage at this level. Rehabilitation programs usually last for 2–3 weeks, starting with relative rest and pain control and progressing to range of motion (ROM) and muscle hypertonicity recuperation from static to dynamic exercises, according to the patient’s tolerance. Subsequently, training is resumed with sport-specific exercises until the player is ready to (return to play). Strengthening muscle tone and aerobic training are also important during this process. A structured rehabilitation approach used in these cases is summarized in
Table 1 [
37].
The prognosis for injuries of the adductor group corroborated with the damage to the external obturator is generally good. The average return-to-play (RTP) duration typically ranges from 18.2 ± 3 days to 11.5 ± 8.8 days, although this may vary. This clinical case confirmed the player’s RTP within 23 days [
36,
38].
The objective was to achieve strength comparable to that of the uninjured muscles on both sides. The focus shifted to neuromuscular control and advanced strengthening exercises. More dynamic and plyometric exercises were introduced to prepare the players to fully resume their activities.
Once the strength and range of movement have been completely restored and pain is minimal or absent, players can gradually resume their sporting activity. The comeback was closely monitored to ensure that there were no signs of relapse [
37].
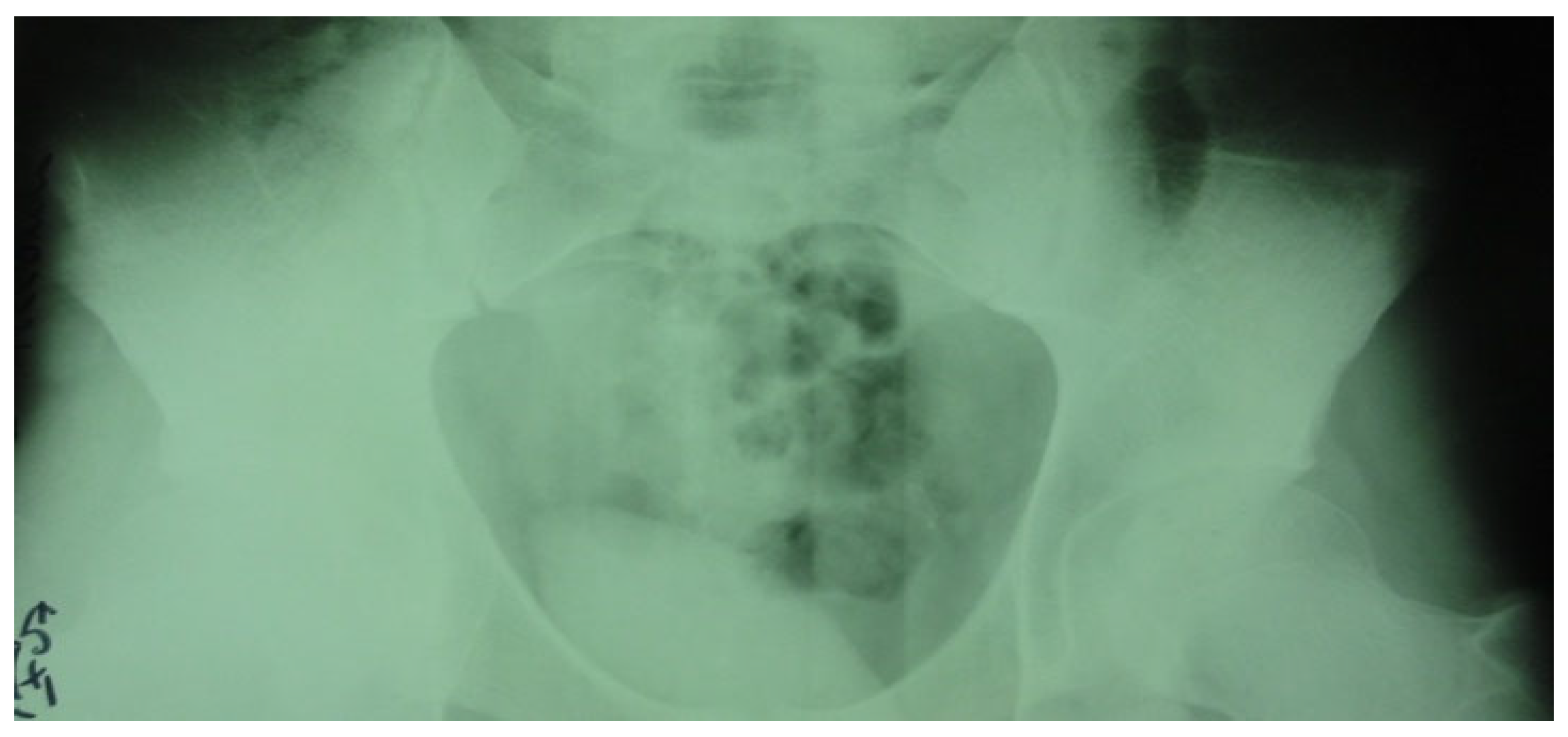
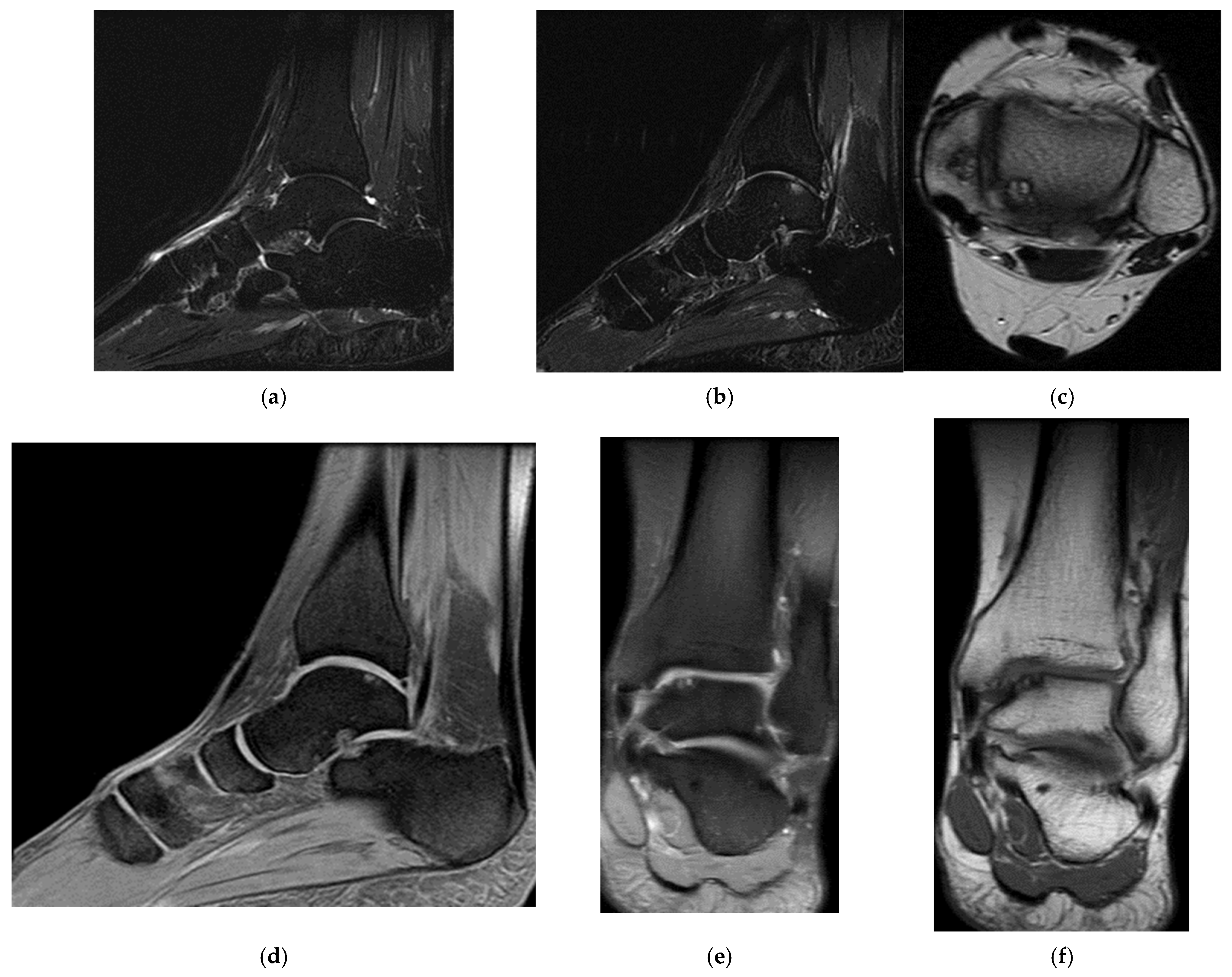
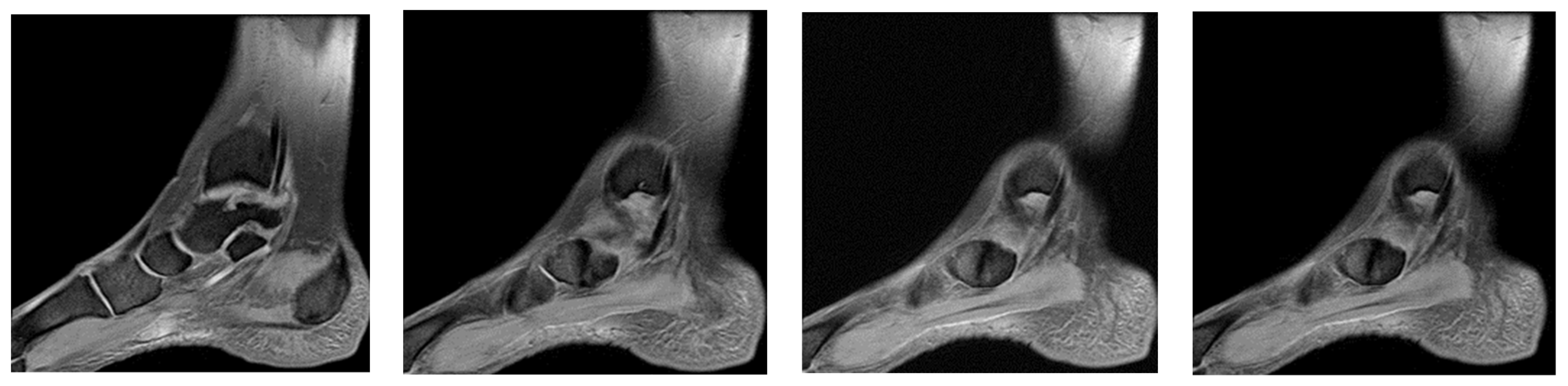
The accessory navicular is a common variant of the anatomy of the foot, characterized by supplementary ossification or bone prominence at the level of the navicular or tarsal scaphoid. The prevalence of the accessory navicular in children is estimated to be approximately 10–12%. The development of symptoms secondary to the presence of an accessory navicular was reported in 0.1% (1 in 1000) of the adult patients. When symptomatic, patients usually complain of a sensitive and erythematous bony prominence on the medial part of the foot, with exacerbated pain when walking, playing sports, wearing shoes, eversion, and plantar flexion. The diagnosis of an accessory navicular is typically confirmed by the presence of pain in the medial aspect of the foot, as observed on radiographic imaging, which reveals additional ossification of the navicular bone. Current guidebooks recommend an initial conservative treatment, including observation, anti-inflammatory drugs, orthosis, and walking boots; if symptoms persist despite conservative treatment, surgical removal or debriding is recommended [
39,
40].
So far, it remains unclear why the symptoms of the accessory navicular manifest only in some patients. Previous authors suggested as possible causes of pain the existence of concurrent posterior tibial tendonitis, the inflammation caused by the pressure on the bony prominence, lax ligaments, synchondrosis trauma, and the alteration of the middle foot biomechanics. The condition of flatfoot, also known as pes planus, has been linked to a symptomatic accessory navicular. Some researchers propose that this foot type may exert increased stress on the accessory navicular during load-bearing activities, although this hypothesis remains a subject of debate.
Patients seldom complain of pain before adolescence, and most report symptoms in their second decade of life. Studies that examined the association between skeletal maturity and accessory navicular development demonstrated that female patients become symptomatic much earlier than male patients. However, no study has definitively proved the association between the development of the accessory navicular and the onset of symptoms [
40].
The degree of skeletal maturity was directly correlated with the type of accessory navicular, indicating that the type of accessory navicular changes with skeletal development. Type II accessory navicular is histologically joined synchondrosis to the fibrocartilage. Type III is similar in shape and size, but the connection is made of bone and fused to the navicular. This connection may result from the development of type II fibrocartilaginous synchondroses. Longitudinal bone fusion was previously described by Knapik et al., who reported a ratio of natural fusion of 42% (
n = 8 of 19), and Nakayama et al. described a fusion ratio of 10% to 14% for the type II accessory navicular. Our data support these figures, indicating a decreasing tendency of the type II accessory navicular and an increase of the type III accessory navicular as skeletal maturity progresses. Extensive imaging is required to understand the pattern and natural development of accessory navicular subtypes [
41,
42].
Surgery remains the common treatment for accessory navicular, as 46% of the patients included in the study underwent at least one surgery (
n = 33/71). This percentage is lower than that reported by Jegal et al., where surgical treatment was performed in 89% of the patients (
n = 57/64), and that reported by Grogan et al., in which surgery was performed in 77% of the patients (
n = 17/22). However, Grogan et al. mentioned using conservative treatment in only 41% of patients with accessory navicular fractures (
n = 16/39). However, Jegal et al. recommended at least 6 months of conservative management, but 37% (
n = 29/79) of the patients were sports players who probably opted for surgery to speed up the improvement of the symptoms and to resume their sporting activity [
39,
41].
Posterior ankle impingement syndrome (PAIS) is a common injury in players with repeated plantar flexion. Although the two-portal posterior approach for the posterior foot has gained popularity, it remains a topic of considerable debate due to its technical complexity, relatively steep learning curve, and the challenges associated with performing simultaneous arthroscopy of the anterior ankle. The aim of a possible reassessment of the data presented in the literature is to offer comprehensive information about PAIS and to describe a systematic approach in four stages of two-portal posterior arthroscopy. Etiology, clinical presentation, and diagnostic strategies have been introduced from the beginning, followed by various conservative and surgical management options. The study continues with a detailed description of the arthroscopy of the posterior foot. This technique allows for a systematic examination of the anatomical structures and treatment of bone/soft tissue damage in four regions of interest of the posterior foot (superolateral, superomedial, inferomedial, and inferolateral). The review focuses on biological accessory therapy and postoperative rehabilitation and ends with a discussion about the latest clinical results of arthroscopy of the posterior foot in PAIS. Although clinical evidence suggests high short- and medium-term success rates after arthroscopy of the posterior foot, its use may be limited owing to the required technical abilities, which can be improved by the systematic approach of two-portal posterior arthroscopy [
43,
44,
45].
The findings of this study provide valuable insights into injury prevention and rehabilitation strategies for professional handball players. Coaches and sports scientists can apply the diagnostic and treatment approaches outlined in this research to enhance athlete performance and longevity.
Based on the frequent knee and muscle injuries identified, it is recommended that handball training programs integrate targeted strength and stability exercises. For instance, incorporating proprioceptive training—such as balance exercises using single-leg stances or unstable surfaces like BOSU balls—can enhance joint stability. Furthermore, neuromuscular control drills that involve controlled jump landings and lateral cutting exercises are crucial for improving dynamic knee stability. Emphasizing the strengthening of key muscle groups through eccentric hamstring exercises, quadriceps conditioning, and hip abductor training can help prevent muscle strains and maintain balanced joint support.
The conservative treatment methods discussed, particularly the use of MRI for accurate diagnosis and monitoring, underscore the importance of individualized rehabilitation plans. Coaches and rehabilitation experts should incorporate regular MRI diagnostics to assess injury severity accurately and track healing progress, especially when initial clinical evaluations are inconclusive. A structured, stage-based rehabilitation protocol—comprising acute, subacute, remodeling, and functional phases—ensures that athlete readiness for progressive load-bearing exercises is continuously assessed.
By integrating these diagnostic tools and therapeutic strategies into daily practice, coaches can reduce the risk of recurring injuries and ensure a safer, more effective return to sport for handball players.
6. Future Directions
Building on the insights gained from our four-case series, future research should pursue several avenues to strengthen the evidence base for MRI-guided conservative management in elite handball:
First, prospective, multicentre cohort studies enrolling larger numbers of athletes will be essential to overcome the limitations of small sample sizes and single-center bias. Such studies should harmonize inclusion criteria, imaging protocols, and rehabilitation regimens across sites to facilitate pooled analysis.
Second, long-term follow-up extending beyond the initial six-week recovery period is needed to capture delayed complications, recurrence rates, and sustained functional outcomes. Regular clinical, functional (e.g., LEFS, isokinetic testing), and imaging (e.g., MRI edema quantification) assessments at 3, 6, and 12 months post-injury will provide a more comprehensive picture of rehabilitation durability.
Third, comparative trials contrasting conservative versus surgical interventions for specific injury types—such as high-grade muscle tears or avulsion fractures with >15 mm retraction—could delineate which lesions benefit most from non-operative care. Incorporating patient-reported outcomes (e.g., sport-specific questionnaires, quality of life scales) will ensure the athlete’s perspective guides treatment decisions.
Fourth, integrating advanced quantitative imaging biomarkers—such as diffusion-weighted MRI for muscle microstructure or T2-mapping for tendon integrity—may refine prognostic models and personalize rehabilitation intensity and duration.
Finally, mechanistic studies examining the interplay of neuromuscular control, biomechanical loading, and tissue healing in handball athletes can inform targeted injury-prevention programs. Collaboration between sports physicians, radiologists, physiotherapists, and performance scientists will be key to translating these future directions into improved athlete care.




 and
and 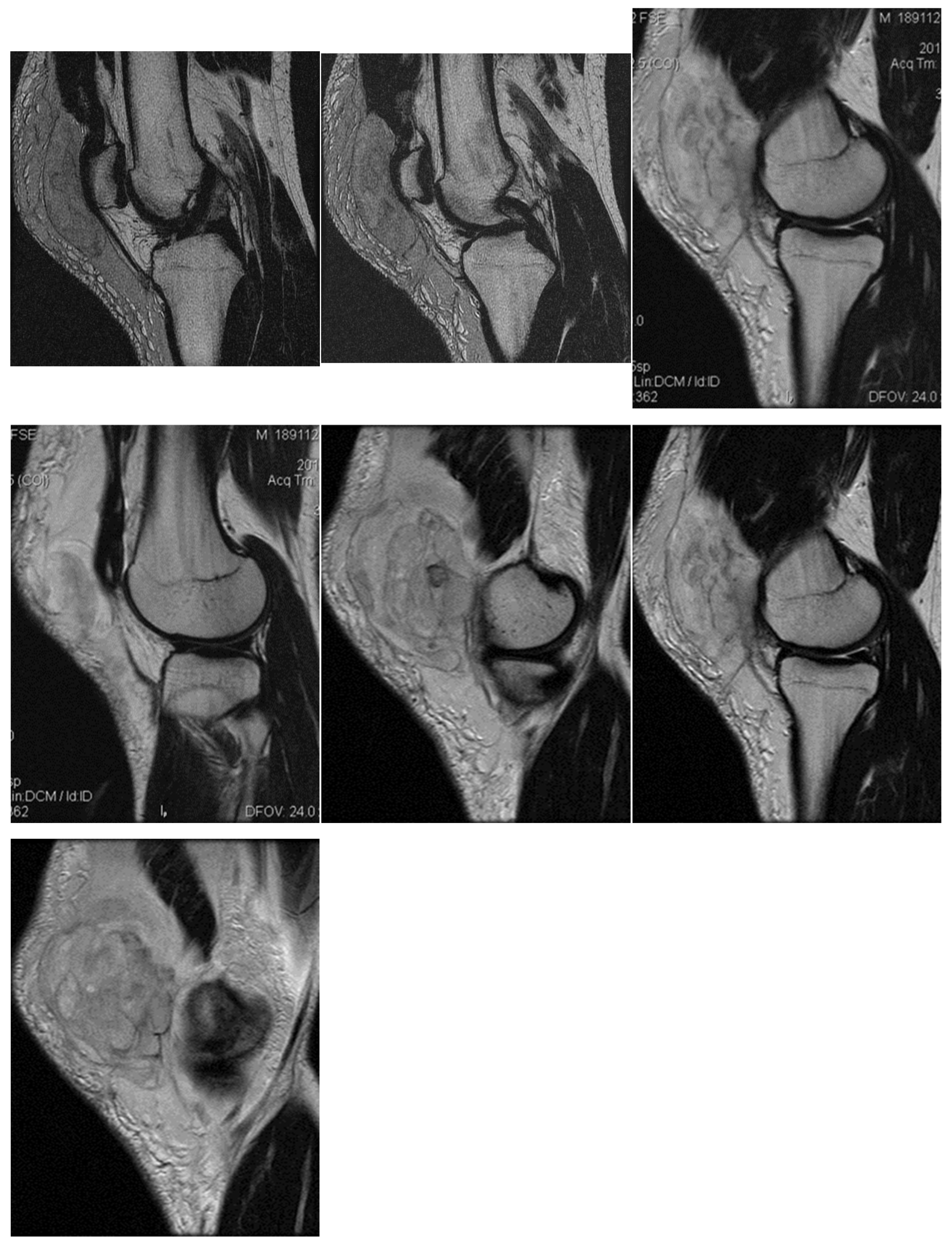






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}