
Long-Term Follow-Up of HRQoL up to Six Years after Outpatient Phase-II Cardiac Rehabilitation

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
Variables and Measures
3. Results
3.1. Clinical Characteristics
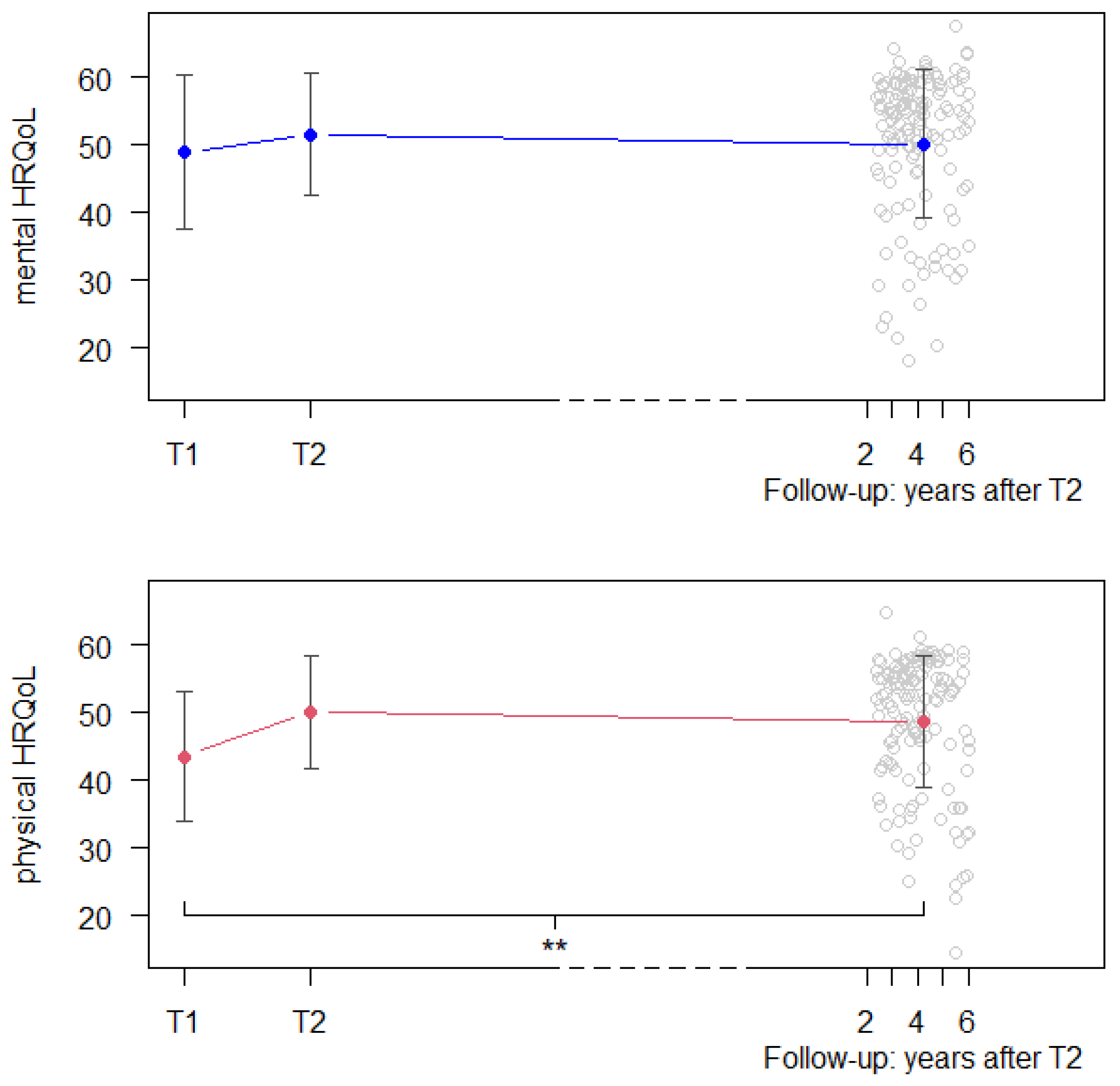
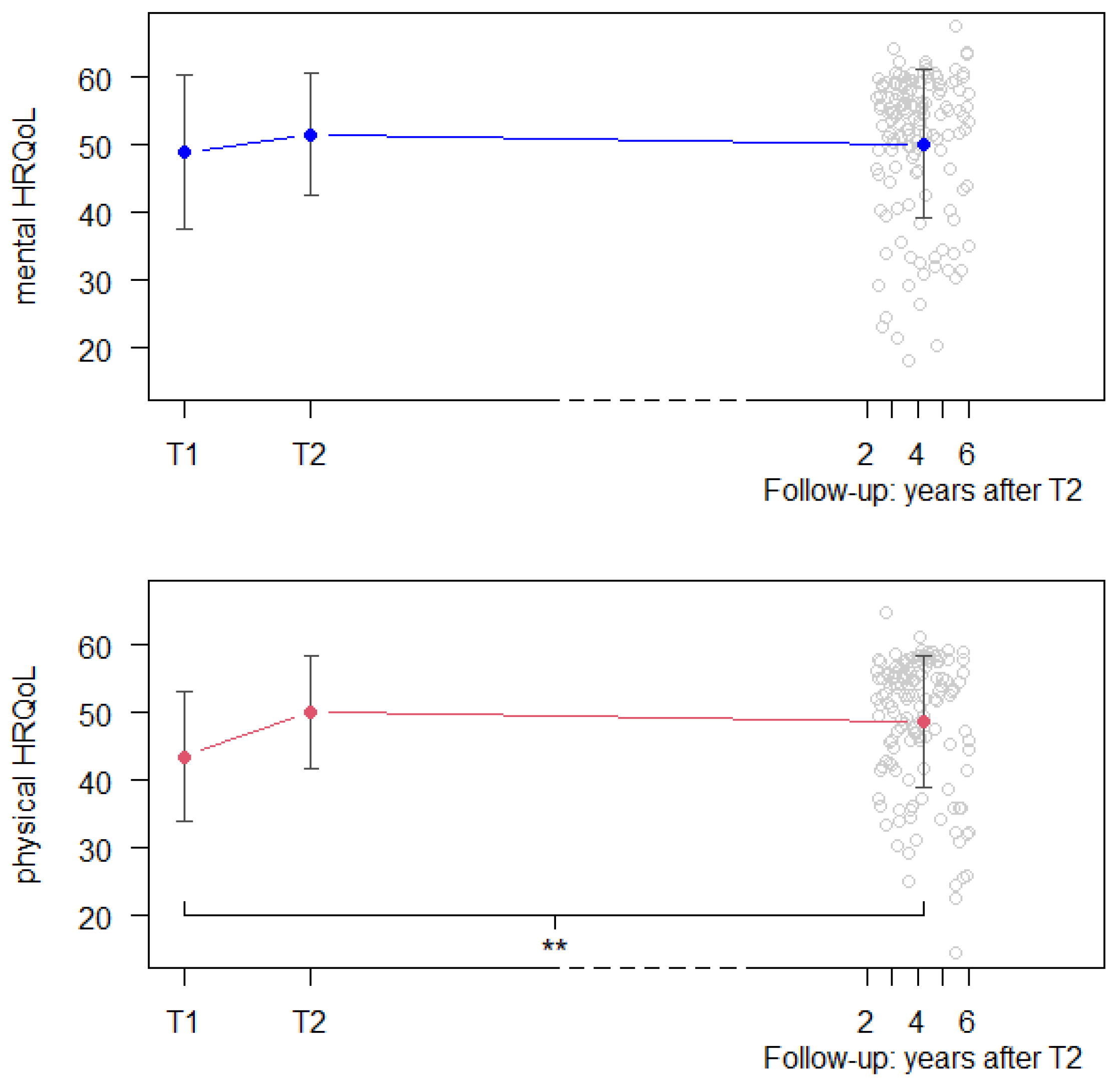
3.2. HRQoL Changes over Time
3.3. Predictors of HRQoL at Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mortality and Global Health Estimates 2019 [Internet]. 2019. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates (accessed on 8 September 2023).
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef] [PubMed]
- Rumsfeld, J.S.; Alexander, K.P.; Goff, D.C., Jr.; Graham, M.M.; Ho, P.M.; Masoudi, F.A.; Moser, D.K.; Roger, V.L.; Slaughter, M.S.; Smolderen, K.G.; et al. Cardiovascular health: The importance of measuring patient-reported health status: A scientific statement from the American Heart Association. Circulation 2013, 127, 2233–2249. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.R.; Yu, C.M. Quality of life in patients with coronary heart disease-I: Assessment tools. Health Qual. Life Outcomes 2003, 1, 42. [Google Scholar] [CrossRef] [PubMed]
- Hofer, S.; Benzer, W.; Oldridge, N. Change in health-related quality of life in patients with coronary artery disease predicts 4-year mortality. Int. J. Cardiol. 2014, 174, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Conradie, A.; Atherton, J.; Chowdhury, E.; Duong, M.; Schwarz, N.; Worthley, S.; Eccleston, D. Health-Related Quality of Life (HRQoL) and the Effect on Outcome in Patients Presenting with Coronary Artery Disease and Treated with Percutaneous Coronary Intervention (PCI): Differences Noted by Sex and Age. J. Clin. Med. 2022, 11, 5231. [Google Scholar] [CrossRef] [PubMed]
- Price, K.J.; Gordon, B.A.; Bird, S.R.; Benson, A.C. A review of guidelines for cardiac rehabilitation exercise programmes: Is there an international consensus? Eur. J. Prev. Cardiol. 2016, 23, 1715–1733. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-Based Cardiac Rehabilitation for Coronary Heart Disease: Cochrane Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2016, 67, CD001800. [Google Scholar] [CrossRef] [PubMed]
- Jellestada, L.; Auschraa, B.; Zuccarella-Hackla, C.; Principa, M.; von Känela, R.; Eulera, S.; Hermannb, M. Sex and age as predictors of HRQOL change in phase-II cardiac rehabilitation. Eur. J. Prev. Cardiol. 2022, 30, 128–136. [Google Scholar] [CrossRef]
- Francis, T.; Kabboul, N.; Rac, V.; Mitsakakis, N.; Pechlivanoglou, P.; Bielecki, J.; Alter, D.; Krahn, M. The Effect of Cardiac Rehabilitation on Health-Related Quality of Life in Patients with Coronary Artery Disease: A Meta-analysis. Can. J. Cardiol. 2019, 35, 352–364. [Google Scholar] [CrossRef]
- Dibben, G.; Faulkner, J.; Oldridge, N.; Rees, K.; Thompson, D.R.; Zwisler, A.D.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2021, 11, Cd001800. [Google Scholar] [CrossRef]
- Yu, C.-M.; Li, L.S.-W.; Ho, H.H.; Lau, C.-P. Long-term changes in exercise capacity, quality of life, body anthropometry, and lipid profiles after a cardiac rehabilitation program in obese patients with coronary heart disease. Am. J. Cardiol. 2003, 91, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Engblom, E.; Korpilahti, K.; Hämäläinen, H.; Rönnemaa, T.; Puukka, P. Quality of life and return to work 5 years after coronary artery bypass surgery. Long-term results of cardiac rehabilitation. J. Cardiopulm. Rehabil. 1997, 17, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Qualitätsanforderungen für die Kardiovaskuläre Prävention und Rehabilitation der SCPRS [Internet]. 2018. Available online: https://www.scprs.ch/public/richtlinien/richtlinien_deutsch.html (accessed on 8 September 2023).
- Brown, K. A review to examine the use of SF-36 in cardiac rehabilitation. Br. J. Nurs. 2003, 12, 904–909. [Google Scholar] [CrossRef]
- Smart, N.A.; King, N.; Lambert, J.D.; Pearson, M.J.; Campbell, J.L.; Risom, S.S.; Taylor, R.S. Exercise-based cardiac rehabilitation improves exercise capacity and health-related quality of life in people with atrial fibrillation: A systematic review and meta-analysis of randomised and non-randomised trials. Open Heart 2018, 5, e000880. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.; Snoww, K.; Ma, K.; Bg, G. SF36 Health Survey: Manual and Interpretation Guide; Quality Metric, Inc.: Lincoln, RI, USA, 1993. [Google Scholar]
- Rasekaba, T.; Lee, A.L.; Naughton, M.T.; Williams, T.J.; Holland, A.E. The six-minute walk test: A useful metric for the cardiopulmonary patient. Intern. Med. J. 2009, 39, 495–501. [Google Scholar] [CrossRef] [PubMed]
- van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 48. [Google Scholar] [CrossRef]
- Shoemaker, M.J.; Curtis, A.B.; Vangsnes, E.; Dickinson, M.G. Triangulating Clinically Meaningful Change in the Six-minute Walk Test in Individuals with Chronic Heart Failure: A Systematic Review. Cardiopulm. Phys. Ther. J. 2012, 23, 5–15. [Google Scholar] [CrossRef]
- Holland, A.E.; Nici, L. The return of the minimum clinically important difference for 6-minute-walk distance in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2013, 187, 335–336. [Google Scholar] [CrossRef]
- Taylor, R.S.; Walker, S.; Smart, N.A.; Piepoli, M.F.; Warren, F.C.; Ciani, O.; Whellan, D.; O’Connor, C.; Keteyian, S.J.; Coats, A.; et al. Impact of Exercise Rehabilitation on Exercise Capacity and Quality-of-Life in Heart Failure: Individual Participant Meta-Analysis. J. Am. Coll. Cardiol. 2019, 73, 1430–1443. [Google Scholar] [CrossRef]
- Bahall, M.; Khan, K. Quality of life of patients with first-time AMI: A descriptive study. Health Qual. Life Outcomes 2018, 16, 32. [Google Scholar] [CrossRef]
- Hartman, E.M.J.; Dulfer, K.; Utens, E.M.W.J.; van den Berge, J.C.; Daemen, J.; van Domburg, R.T. Gender differences in quality of life after PCI attenuate after a 10year follow-up. Int. J. Cardiol. 2014, 176, 1179–1180. [Google Scholar] [CrossRef]
- Herlitz, J.; Brandrup-Wognsen, G.; Caidahl, K.; Haglid, M.; Karlson, B.W.; Hartford, M.; Karlsson, T.; Sjöland, H. Improvement and factors associated with improvement in quality of life during 10 years after coronary artery bypass grafting. Coron. Artery Dis. 2003, 14, 509–517. [Google Scholar] [CrossRef]
- Vaccarino, V.; Badimon, L.; Bremner, J.D.; Cenko, E.; Cubedo, J.; Dorobantu, M.; Duncker, D.J.; Koller, A.; Manfrini, O.; Milicic, D.; et al. Depression and coronary heart disease: 2018 position paper of the ESC working group on coronary pathophysiology and microcirculation. Eur. Heart J. 2019, 41, 1687–1696. [Google Scholar] [CrossRef] [PubMed]
- Lichtman, J.H.; Froelicher, E.S.; Blumenthal, J.A.; Carney, R.M.; Doering, L.V.; Frasure-Smith, N.; Freedland, K.E.; Jaffe, A.S.; Leifheit-Limson, E.C.; Sheps, D.S.; et al. Depression as a risk factor for poor prognosis among patients with acute coronary syndrome: Systematic review and recommendations: A scientific statement from the American Heart Association. Circulation 2014, 129, 1350–1369. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Ciani, O.; Piepoli, M.; Smart, N.; Uddin, J.; Walker, S.; Warren, F.C.; Zwisler, A.D.; Davos, C.H.; Taylor, R.S. Validation of Exercise Capacity as a Surrogate Endpoint in Exercise-Based Rehabilitation for Heart Failure: A Meta-Analysis of Randomized Controlled Trials. JACC Heart Fail. 2018, 6, 596–604. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Total | |
|---|---|
| N | |
| Total | 153 |
| Male | 127 (83%) |
| Female | 26 (17%) |
| Time since CR (years) 1 | 4.00 (1.04) |
| CHD diagnosis | |
| Acute myocardial infarction | 117 (76.5%) |
| Unstable angina pectoris | 9 (5.9%) |
| Stable angina pectoris | 15 (9.8%) |
| Presence of arrythmia | 19 (12.4%) |
| Intervention | |
| PCI/stent | 145 (94.8%) |
| CABG | 10 (6.5%) |
| Valve procedure | 4 (2.6%) |
| Ejection fraction 1 | 54.44 (9.85) |
| Cardiovascular risk factors | |
| Hypertension | 97 (63.4%) |
| Dyslipidemia | 135 (61.9%) |
| Smoking | 78 (51.0%) |
| Diabetes mellitus type II | 20 (13.1%) |
| Obesity | 31 (20.2%) |
| Cardiac medication | |
| Beta-blocker | 102 (66.7%) |
| ACE-inhibitors | 98 (64.1%) |
| ARNI | 5 (3.3%) |
| SGLT-2 inhibitors | 7 (4.6%) |
| Charlson Comorbidity Index 1 | 3.24 (1.76) |
| Psychiatric disorder | 18 (11.8%) |
| 6MWT | |
| T1 (m) 1 | 539.44 (104.28) |
| T2 (m) 1 | 593.62 (102.29) |
| Change ratio T1 to T2 (%) 1 | 11.3 (14.9) |
| Mental HRQOL | Physical HRQoL | |||||||
|---|---|---|---|---|---|---|---|---|
| Estimate b | Standard Error | t | p | Estimate b | Standard Error | t | p | |
| Score T1 | −1.32 | 0.97 | −1.37 | 0.173 | −5.01 | 0.81 | −6.23 | <0.001 |
| Score T2 | 1.52 | 0.97 | −1.57 | 0.118 | 0.98 | 0.81 | 1.21 | 0.226 |
| Psychiatric Disorder | 10.87 | 2.38 | 4.57 | <0.001 | 2.47 | 2.01 | 1.23 | 0.222 |
| Sex | 1.11 | 1.92 | 0.58 | 0.564 | 1.17 | 1.63 | 0.72 | 0.472 |
| Age | −0.02 | 0.08 | −0.22 | 0.828 | 0.05 | 0.07 | 0.76 | 0.452 |
| 6MWT at T1 | 0.02 | 0.01 | 1.80 | 0.075 | 0.04 | 0.01 | 5.06 | <0.001 |
| Change ratio T1 to T2 | −1.36 | 5.90 | −0.23 | 0.818 | 7.78 | 4.99 | 1.56 | 0.122 |
| Time since CR discharge | 0.24 | 0.68 | 0.35 | 0.728 | −0.45 | 0.58 | −0.78 | 0.435 |
| Hypertension | 1.04 | 1.41 | 0.74 | 0.463 | −0.59 | 1.19 | −0.50 | 0.619 |
| Dyslipidemia | −4.26 | 1.44 | −2.97 | 0.004 | 0.57 | 1.21 | 0.47 | 0.640 |
| Obesity | −0.99 | 1.90 | −0.52 | 0.604 | −2.10 | 1.61 | −1.31 | 0.193 |
| Smoking | 0.83 | 1.40 | 0.60 | 0.553 | −0.38 | 1.19 | −0.32 | 0.747 |
| Diabetes mellitus type II | 3.09 | 2.74 | 1.36 | 0.177 | 1.06 | 1.93 | 0.55 | 0.583 |
| Charlson Comorbidity Index | 1.36 | 0.56 | 2.41 | 0.017 | −0.21 | 0.48 | −0.45 | 0.656 |
| Ejection fraction | −0.05 | 0.08 | −0.70 | 0.485 | 0.06 | 0.06 | 0.95 | 0.343 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Auschra, B.; Euler, S.; Zehnder, Y.; Fuentes Artiles, R.; Niederseer, D.; Zuccarella-Hackl, C.; von Känel, R.; Jellestad, L. Long-Term Follow-Up of HRQoL up to Six Years after Outpatient Phase-II Cardiac Rehabilitation. Healthcare 2024, 12, 357. https://doi.org/10.3390/healthcare12030357
Auschra B, Euler S, Zehnder Y, Fuentes Artiles R, Niederseer D, Zuccarella-Hackl C, von Känel R, Jellestad L. Long-Term Follow-Up of HRQoL up to Six Years after Outpatient Phase-II Cardiac Rehabilitation. Healthcare. 2024; 12(3):357. https://doi.org/10.3390/healthcare12030357
Chicago/Turabian StyleAuschra, Bianca, Sebastian Euler, Yara Zehnder, Rubén Fuentes Artiles, David Niederseer, Claudia Zuccarella-Hackl, Roland von Känel, and Lena Jellestad. 2024. "Long-Term Follow-Up of HRQoL up to Six Years after Outpatient Phase-II Cardiac Rehabilitation" Healthcare 12, no. 3: 357. https://doi.org/10.3390/healthcare12030357
APA StyleAuschra, B., Euler, S., Zehnder, Y., Fuentes Artiles, R., Niederseer, D., Zuccarella-Hackl, C., von Känel, R., & Jellestad, L. (2024). Long-Term Follow-Up of HRQoL up to Six Years after Outpatient Phase-II Cardiac Rehabilitation. Healthcare, 12(3), 357. https://doi.org/10.3390/healthcare12030357