


Effectiveness of Leisure-Focused Occupational Therapy Interventions in Middle-Aged and Older People with Mild Cognitive Impairment: A Systematic Review
 , , , , ,
, , , , ,  ,
,  , and
, and
Abstract
1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information and Database Search Process
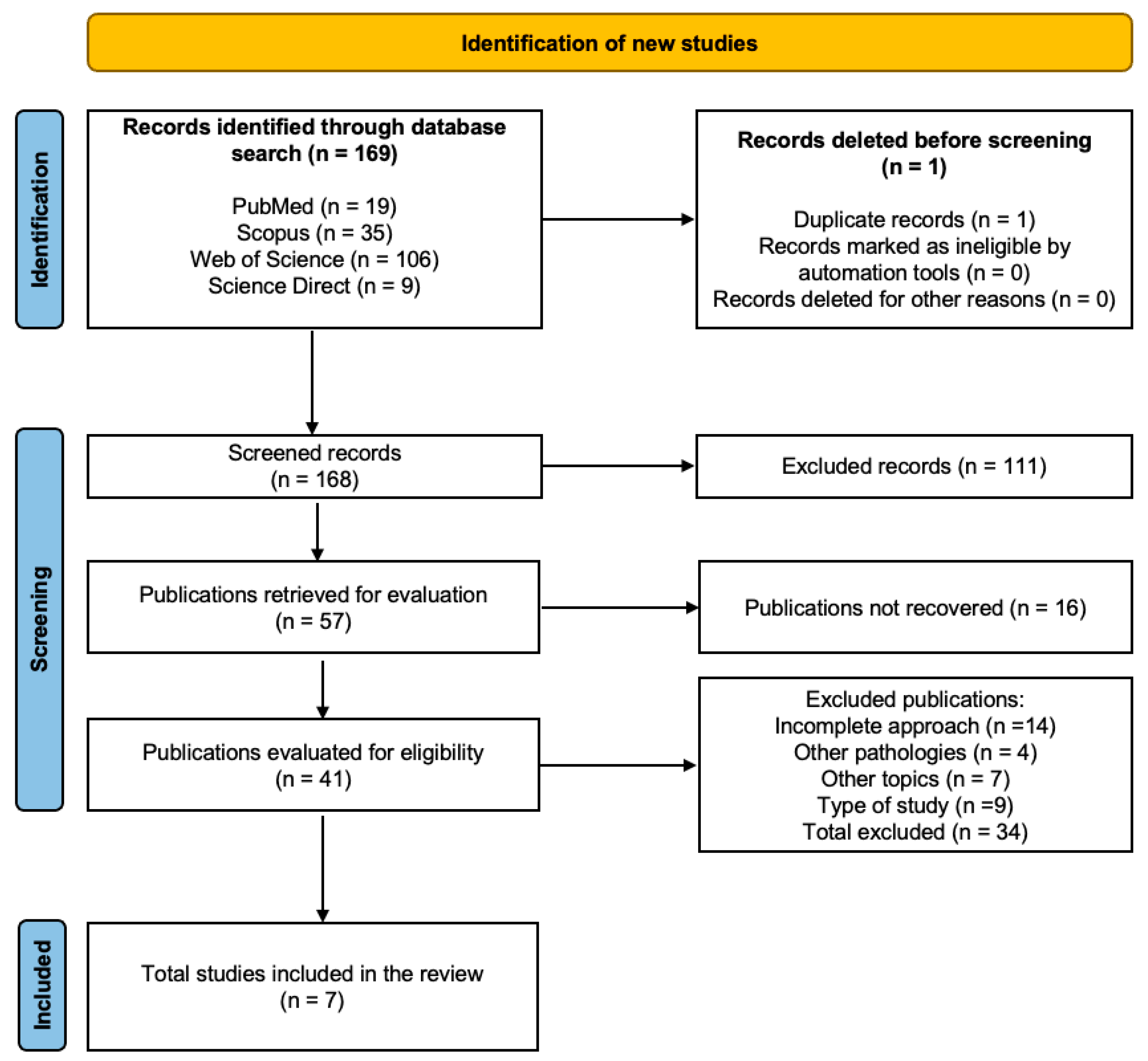
2.4. Study Selection and Data Collection Process
2.5. Methodological Quality Evaluation
2.6. Data Collection Process
2.7. Risk of Bias Assessment
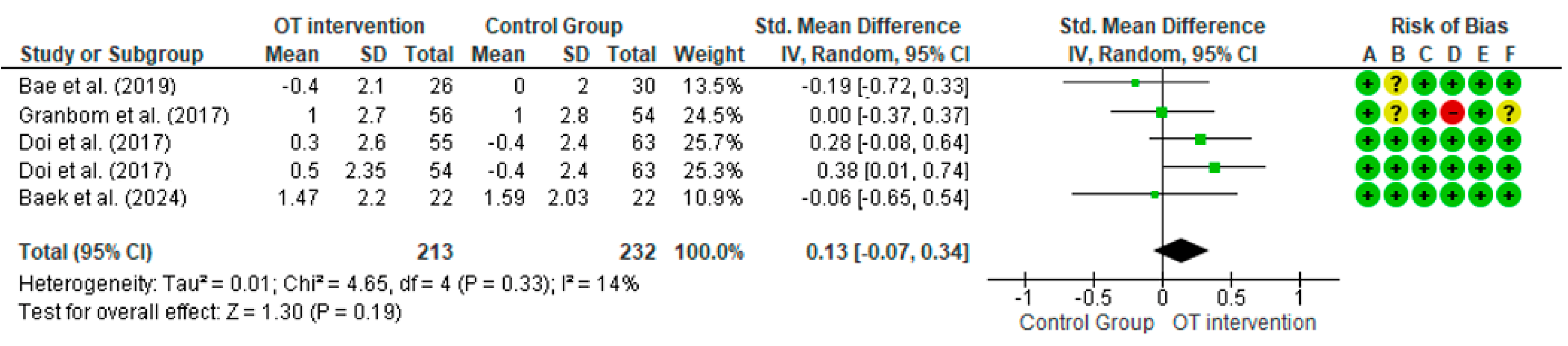
2.8. Measures for Meta-Analysis
2.9. Certainty of Evidence
3. Results
3.1. Methodological Quality
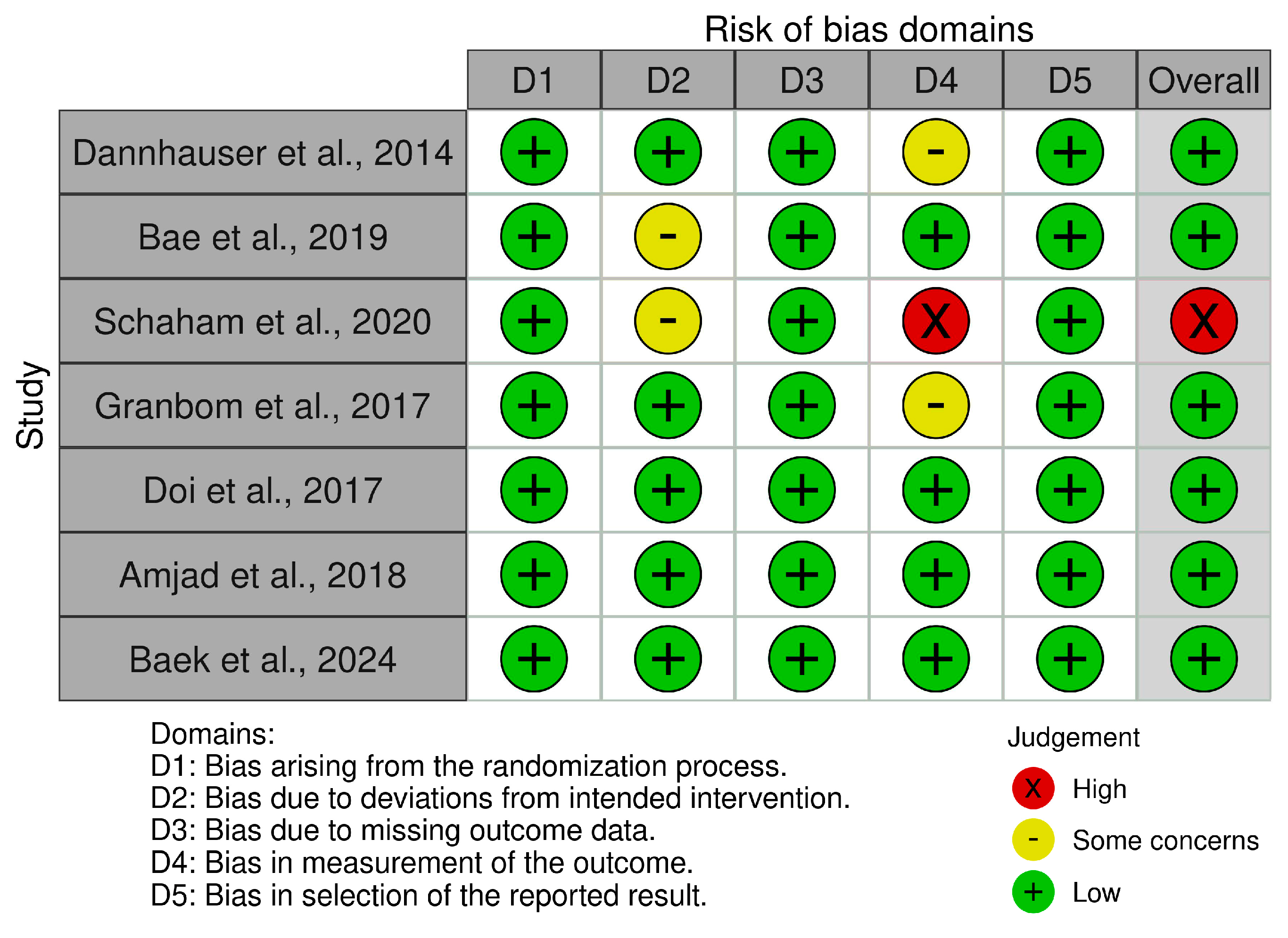
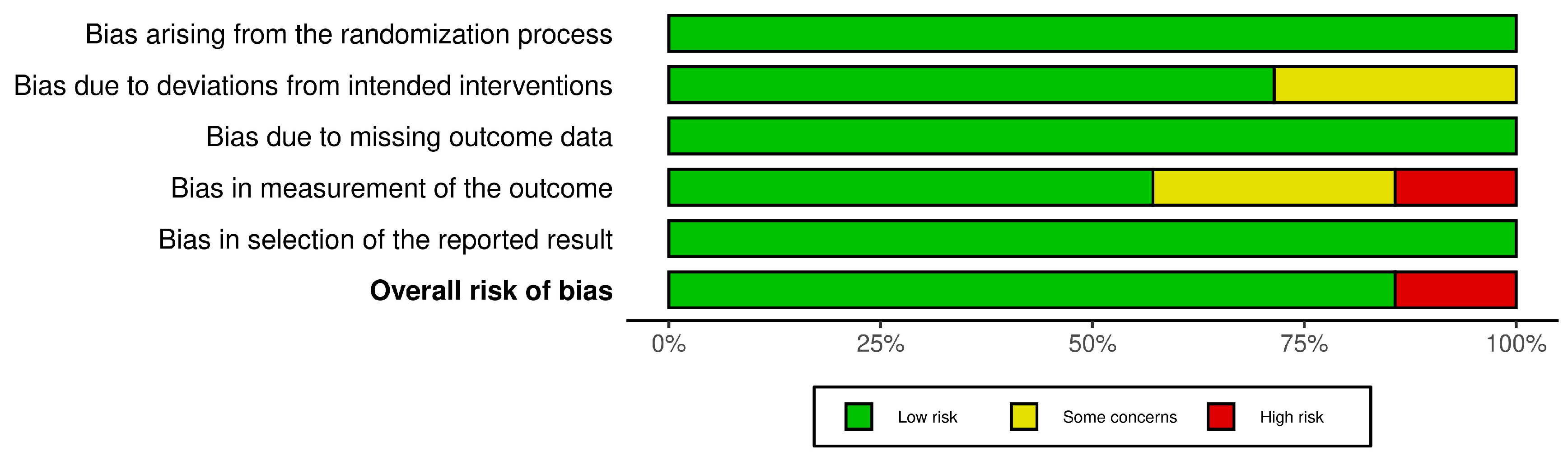
3.2. Risk of Bias
3.3. Characteristics of the Studies
3.4. Sample Characteristics
3.5. Dosages and Interventions Performed
3.6. Activities of Daily Living
3.7. Cognitive Function
3.8. Certainty of Evidence
3.9. Adverse Effects and Adherence
4. Discussion
4.1. Leisure Activities
4.2. Activities of Daily Living
4.3. Cognitive Function
4.4. Strengths and Limitations
4.5. Practical Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Ageing and Health. 2022. Available online: https://www.who.int/es/news-room/fact-sheets/detail/ageing-and-health (accessed on 18 August 2024).
- World Health Organization. World Report on Ageing and Health. 2021. Available online: https://www.who.int/publications/i/item/9789241565042 (accessed on 1 October 2024).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2018. [Google Scholar]
- World Health Organization. Dementia. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 5 October 2024).
- Livingstone, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Brayne, C.; Fox, N.C.; Perri, C.P.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef] [PubMed]
- Thyrian, J.R.; Hertel, J.; Wucherer, D.; Eichler, T.; Michalowsky, B.; Dreier-Wolfgramm, A.; Zwingmann, I.; Kilimann, I.; Teipel, S.; Hoffmann, W. Effectiveness and safety of dementia care management in primary care: A randomized clinical trial. JAMA Psychiatry 2017, 74, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Tang, D.; Wang, Y.; Jiang, S.; Liu, X. Community support and promoting cognitive function for the elderly. Front. Psychol. 2022, 13, 942474. [Google Scholar] [CrossRef]
- Herold, F.; Törpel, A.; Schega, L.; Müller, N.G. Functional and/or structural brain changes in response to resistance exercises and resistance training lead to cognitive improvements: A systematic review. Eur. Rev. Aging Phys. Act. 2019, 16, 10. [Google Scholar] [CrossRef]
- Schnell-Inderst, P.; Conrads-Frank, A.; Stojkov, I.; Krenn, C.; Kofler, L.M.; Siebert, U. Occupational therapy for persons with cognitive impairments. Ger. Med. Sci. 2023, 21, Doc02. [Google Scholar]
- Mendoza Holgado, C.; García González, M. Una aproximación clínica al deterioro cognitivo leve: Intervención desde terapia ocupacional. TOG 2018, 15, 127–133. [Google Scholar]
- Pérez, A.F. Métodos de cribaje del deterioro cognitivo leve en atención primaria. Rev. Esp. Geriatr. Gerontol. 2017, 52, 15–19. [Google Scholar] [CrossRef]
- Spínola, M.; Câmara, J.; Ferreira, L.; Faria, A.L.; Badia, S.B.i. Customizing a Cognitive Stimulation Program for Individuals with Dementia through a Participatory Design Approach. Appl. Sci. 2022, 12, 11612. [Google Scholar] [CrossRef]
- González, L.; Rosende, I. Ocupaciones de ocio, calidad de vida y envejecimiento activo: Un análisis desde las percepciones de ciudadanos mayores autónomos. TOG 2018, 5, 10–18. [Google Scholar]
- Patterson, I.; Pegg, S. Serious leisure and people with intellectual disabilities: Benefits and opportunities. Leis. Stud. 2009, 28, 387–402. [Google Scholar] [CrossRef]
- Alban, D.A.R.; Ugsha, S.C.T.; Mejía, M.C.; Atiaga, D.R.M. El tiempo libre y el ocio en el mejoramiento de la calidad de vida del adulto mayor. Dom. Cien. 2021, 7, 83. [Google Scholar]
- DeBoer, K.; Kleindl, C.; Nyakoe, M. The Link between Occupational Therapy Interventions, Quality of Life, and Social and Leisure Participation in Adults with Chronic Conditions. Crit. Apprais. Top. 2022, 49. Available online: https://commons.und.edu/cat-papers/49 (accessed on 11 October 2024).
- American Occupational Therapy Association. Occupational Therapy in the Promotion of Health and Well-Being through Leisure Activities. Am. J. Occup. Ther. 2023, 74, 7403420010p1–7403420010p14. Available online: https://research.aota.org/ (accessed on 8 June 2024).
- Cancino, M.; Rehbein, L. Anticipatory signs and risk factors for Mild Cognitive Impairment (MCI): A synoptic view. Ter. Psicol. 2016, 34, 183–189. [Google Scholar] [CrossRef]
- Johnson, J.D.; Whitlatch, C.J.; Menne, H.L. Activity and well-being of older adults: Does cognitive impairment play a role? Res. Aging 2014, 36, 147–160. [Google Scholar] [CrossRef] [PubMed]
- Parikh, P.K.; Troyer, A.K.; Maione, A.M.; Murphy, K.J. The impact of memory change on daily life in normal aging and mild cognitive impairment. Gerontologist 2016, 56, 877–885. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Savovic, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Chapter 8: Assessing Risk of Bias in a Randomized Trial. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.4; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons: Chichester, UK, 2023. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Alonso-Fernández, S. Declaración PRISMA 2020: Una guía actualizada para la publicación de revisiones sistemáticas. Rev. Esp. Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef]
- Vásquez, E.; Huenchuquen, C.; Ferrón, C. Effectiveness of Intervention Focused on Leisure as an Occupation in People with Mild Cognitive Impairment from an Occupational Therapy Perspective: Systematic Review. PROSPERO 2023, CRD42023472129. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023472129 (accessed on 30 July 2024).
- Oxford Centre for Evidence-based Medicine. Centre for Evidence Based Medicine—Levels of Evidence. Available online: http://www.cebm.net/index.aspx?o=1025 (accessed on 22 July 2024).
- Manterola, C.; Zavando, D. Cómo interpretar los “Niveles de Evidencia” en los diferentes escenarios clínicos. Rev. Chil. Cir. 2009, 61, 582–595. [Google Scholar] [CrossRef]
- Verhagen, A.P.; de Vet, H.C.; de Bie, R.A.; Boers, M.; van den Brandt, P.A. The art of quality assessment of RCTs included in systematic reviews. J. Clin. Epidemiol. 2001, 54, 651–654. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Davey, J.; Turner, R.M.; Clarke, M.J.; Higgins, J.P. Characteristics of meta-analyses and their component studies in the Cochrane Database of Systematic Reviews: A cross-sectional, descriptive analysis. BMC Med. Res. Methodol. 2011, 11, 160. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.B. Estimating effect sizes from pretest-posttest-control group designs. Organ. Res. Methods 2008, 11, 364–386. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.X.; Machado, G.C. Clinimetrics: Grading of Recommendations, Assessment, Development and Evaluation (GRADE). J. Physiother. 2021, 67, 66. [Google Scholar] [CrossRef]
- Dannhauser, T.M.; Cleverley, M.; Whitfield, T.J.; Fletcher, B.C.; Stevens, T.; Walker, Z. A complex multimodal activity intervention to reduce the risk of dementia in mild cognitive impairment—ThinkingFit: Pilot and feasibility study for a randomized controlled trial. BMC Psychiatry 2014, 14, 129. [Google Scholar] [CrossRef]
- Bae, S.; Lee, S.; Lee, S.; Jung, S.; Makino, K.; Harada, K.; Shinkai, Y.; Chiba, I.; Shimada, H. The effect of a multicomponent intervention to promote community activity on cognitive function in older adults with mild cognitive impairment: A randomized controlled trial. Complement. Ther. Med. 2019, 42, 164–169. [Google Scholar] [CrossRef]
- Schaham, N.; Vitek, H.; Donda, N.; Elbo Golan, I.; Buckman, Z.; Rand, D. The Development and Feasibility of TECH: Tablet Enhancement of Cognition and Health, a Novel Cognitive Intervention for People with Mild Cognitive Impairment. Games Health J. 2020, 9, 346–352. [Google Scholar] [CrossRef]
- Granbom, M.; Re, G.; Jenkins, G.R.; Fristedt, S.; Seppänen, A.; Iwarsson, S. Randomized controlled trial of home-based interventions for older adults focused on social participation and leisure activities. J. Aging Health 2017, 29, 1230–1246. [Google Scholar]
- Doi, T.; Verghese, J.; Makizako, H.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Suzuki, T.; Shimada, H. Effects of cognitive leisure activity on cognition in mild cognitive impairment: Results of a randomized controlled trial. J. Am. Med. Dir. Assoc. 2017, 18, 686–691. [Google Scholar] [CrossRef]
- Amjad, I.; Toor, H.; Niazi, I.K.; Bashir, S.; Ahmad, A.; Gilani, S.A. Xbox 360 Kinect Cognitive Games Improve Slowness, Cognitive improvement and EEG activity changes following exergaming in older adults with mild cognitive impairment: A randomized controlled trial. J. NeuroEng. Rehabil. 2018, 15, 1–12. [Google Scholar]
- Baek, J.E.; Hyeon, S.J.; Kim, M.; Cho, H.Y.; Hahm, S.C. Effects of dual-task resistance exercise on cognition, mood, depression, functional fitness, and activities of daily living in older adults with cognitive impairment: A single-blinded, randomized controlled trial. BMC Geriatr. 2024, 24, 369. [Google Scholar] [CrossRef]
- Haddaway, N.; Page, M.; Pritchard, C.; McGuinness, L. PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell Syst. Rev. 2022, 18, e1230. [Google Scholar] [CrossRef] [PubMed]
- Mandolesi, L.; Polverino, A.; Montuori, S.; Foti, F.; Ferraioli, G.; Sorrentino, P.; Sorrentino, G. Effects of physical exercise on cognitive functioning and wellbeing: Biological and psychological benefits. Front. Psychol. 2018, 9, 509. [Google Scholar] [CrossRef] [PubMed]
- Quigley, A.; MacKay-Lyons, M.; Eskes, G. Effects of exercise on cognitive performance in older adults: A narrative review of the evidence, possible biological mechanisms, and recommendations for exercise prescription. J. Aging Res. 2020, 2020, 1407896. [Google Scholar] [CrossRef] [PubMed]
- Voss, M.W.; Nagamatsu, L.S.; Liu-Ambrose, T.; Kramer, A.F. Exercise, brain, and cognition across the life span. J. Appl. Physiol. 2011, 111, 1505–1513. [Google Scholar] [CrossRef]
- Al-Yahya, E.; Dawes, H.; Smith, L.; Dennis, A.; Howells, K.; Cockburn, J. Cognitive motor interference while walking: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2011, 35, 715–728. [Google Scholar] [CrossRef]
- Seidler, R.D.; Bernard, J.A.; Burutolu, T.B.; Fling, B.W.; Gordon, M.T.; Gwin, J.T.; Kwak, Y.; Lipps, D.B. Motor control and aging: Links to age-related brain structural, functional, and biochemical effects. Neurosci. Biobehav. Rev. 2010, 34, 721–733. [Google Scholar] [CrossRef]
- Wollesen, B.; Wildbredt, A.; van Schooten, K.S.; Lim, M.L.; Delbaere, K. The effects of cognitive-motor training interventions on executive functions in older people: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2020, 17, 9. [Google Scholar] [CrossRef]
- Metzger, L.; Henley, L.; Smallfield, S.; Green, M.; Rhodus, E.K. Interventions Within the Scope of Occupational Therapy to Improve Cognitive Performance for Individuals with Dementia and Mild Cognitive Impairment (2018–2022). Am. J. Occup. Ther. 2023, 77 (Suppl. S1), 7710393260. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Inclusion | Exclusion |
|---|---|---|
| Population | Studies on a population with a mean age of 45 years or more and with MCI [2]. They were functionally independent and free of comorbid conditions or other debilitating social problems. | Studies with populations whose main pathology is different from MCI (chronic diseases, physical deterioration, or social problems) and under 45 years of age. |
| Intervention | Studies involving occupational therapy interventions or leisure-focused programs from 4 weeks onwards. | Studies whose main focus of intervention was not related to occupational therapy programs focused on leisure activities. |
| Comparison | Interventions with an experimental group focused on leisure activities and activities of daily living. | Lack of reference and/or follow-up data. Absence of control group. |
| Outcome | At least one assessment of cognitive functions and leisure and free time. | It does not present any assessment of these variables. |
| Study design | Experimental design studies (randomized controlled trial) with pre- and post-assessment. | Non-randomized, cross-sectional, retrospective, and prospective controlled studies. |
| Level of evidence | 1a | 1b, 2a, 2b, 3a, 3b, 4, and 5 |
| Study | Country | Study Design | Sample’s Initial Health | Participants (n) | Mean Age (Years) | Type of Intervention and Control Groups | Training Volume | Training Intensity | ADLs (Assessment) | Cognitive Function (Assessment) | Main Outcomes | Effect Size | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Weeks | Frequency (Sessions/Week) | Session Duration (Minutes) | ||||||||||||
| [32] | Germany | RCT | Subjects diagnosed with MCI | EG: 32 CG: 35 | 73.9 | ThinkingFit Program (EG) vs. Individual cognitive stimulation training (CG) | 12 | 3 | 30 | Low to moderate | Katz ADL Index | MMSE, MoCA | EG ↑ Significant improvements in physical fitness (p < 0.005). ↑ Improvement in cognitive outcomes after the intervention period. ↑ Significant improvements in quality of life (p < 0.05). CG ↔ Stable cognitive performance during the control period. ↔ No significant changes in quality of life during the control period. | Cognitive function, EG vs. CG, d: 0.465 |
| [33] | Republic of Korea | RCT | Subjects diagnosed with MCI | EG: 41 CG: 42 | 75.5 | Healthy activities in “Kenkojichi” (EG) vs. Health education (CG) | 24 | 2 | 90 | Moderate | not reported | TMT-A, TMT-B, MMSE | EG ↑ Cognitive activities associated with better overall cognitive performance (p = 0.678). ↔ Participation in social activities delays the onset of dementia and decreases the risk of MCI. ↑ Performing “favorite” activities plays a motivating and crucial role in the intervention. CG ↔ No significant changes in cognitive performance or MCI progression. | Cognitive function, EG vs. CG, d: 0.195 |
| [34] | Israel | RCT | Subjects diagnosed with MCI | EG: 15 CG: 13 | 68.9 | Cognitive stimulation program through TECH (EG) vs. Traditional cognitive training (CG) | 6 | 1 | 30–60 | Low to moderate | not reported | MoCA | EG ↑ TECH, a self-reported intervention, improves cognition and prevents MCI in adults. ↑ The intervention was engaging and motivating, aligned with participants’ interests. CG ↔ No significant improvements in cognition or MCI prevention without the intervention. | Cognitive function, EG vs. CG, d: 1.24 |
| [35] | Sweden | RCT | Subjects diagnosed with MCI | EG: 80 CG: 73 | 81.4 | Home-based interventions focused on social participation (EG) vs. Traditional home-based interventions (CG) | 12 | 1 | 60 | Low | Katz ADL Index | MMSE | EG ↔ No significant differences in social participation compared to CG (p = 0.114). ↔ No significant changes in important leisure activities (p = 0.601). CG ↔ Similar outcomes in social participation (p = 0.114). ↔ No significant differences in important leisure activities (p = 0.601). | Cognitive function, EG vs. CG, d: 0.17 |
| [36] | Japan | RCT | Subjects diagnosed with MCI | EG: 134 CG: 67 | 76.2 | Cognitive leisure activities (dance or music) (EG) vs. Health education (CG) | 40 | 1 | 60 | Low | not reported | TMT-A, TMT-B, MMSE | EG ↑ Greater improvement in MMSE scores compared to CG (dance: p = 0.026, music: p = 0.008). ↔ No significant differences in TMT-A and TMT-B scores compared to CG. CG ↔ No significant changes in MMSE scores. ↔ Similar outcomes in TMT-A and TMT-B scores. | Cognitive function, EG dance vs. CG, d: 0.080 Cognitive function, EG music vs. CG, d: 0.040 |
| [37] | Pakistan | RCT | Subjects diagnosed with MCI | EG: 22 CG: 22 | 79.2 | Xbox 360 Kinect cognitive games (EG) vs. Range of motion exercises (CG) | 6 | 5 | 25 | Low to moderate | not reported | MMSE, MoCA, TMT-A, TMT-B | EG ↑ Significant improvement in delta waves (0.673–0.029; p = 0.013). ↑ Significant improvement in theta waves (0.129–0.013; p = 0.002). ↑ Significant improvement in beta2 waves (0.044–0.009; p = 0.046). ↑ EEG complexity increased (0.051–0.042; p = 0.016). ↑ MMSE scores significantly improved (26.25–0.347 vs. 23.722–0.731; p = 0.003). ↑ MoCA scores significantly improved (25.65–0.310 vs. 22.00–0.504; p = 0.0001). ↑ TMT-A scores improved (1.429–0.234 vs. 2.225–0.259; p = 0.028). ↑ TMT-B scores improved (2.393–0.201 vs. 3.780–0.195; p = 0.0001). CG ↔ No significant changes in the above metrics. | Cognitive function, EG vs. CG, MMSE d: 2.528 MoCA d: 3.650 TMT-A d: 0.796 TMT-B d: 1.387 |
| [38] | Republic of Korea | RCT | Subjects diagnosed with MCI | EG: 22 CG: 22 | 82.4 | Dual-task resistance exercise (EG) vs. Resistance exercise (CG) | 6 | 3 | 40 | Low to moderate | Korean version of ADL | MMSE | EG (Intervention Group: Dual-Task Resistance Exercise and Resistance Exercise) ↑ Significant improvement in cognitive function (p < 0.001). ↑ Significant improvement in mood (p < 0.001). ↑ Significant improvement in depression (p < 0.001). ↑ Significant improvement in functional fitness (p < 0.001). ↑ Significant improvement in ADLs (p < 0.001). CG ↔ No significant changes compared to intervention groups. | Cognitive function, EG vs. CG, d: −0.02 |
| Certainty of Evidence | Nº of Patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nº of Studies | Study Design | Risk Assessment | Inconsistency | Indirect Evidence | Vagueness | Other Considerations | [Conventional Therapy plus Virtual Reality] | [Conventional Therapy] | Relative (95% CI) | Absolute (95% CI) | ||
| To analyze the effectiveness of the intervention focused on leisure as an occupation in people with MCI (follow-up: mean of 12 weeks; assessed with ANOVA) | ||||||||||||
| 1 | RCT | It is not serious | It is not serious | It is not serious | It is not serious | None | 63/63 (100%) | 0/63 (0.0%) | Not estimable | ++++ High | IMPORTANT | |
| To analyze the effectiveness of the intervention focused on leisure as an occupation in people with MCI (follow-up: mean of 24 weeks; assessed with TMT-A and TMT-B) | ||||||||||||
| 1 | RCT | It is not serious | It is not serious | It is not serious | It is not serious | None | 41/83 (49.4%) | 42/83 (50%) | Not estimable | ++++ High | IMPORTANT | |
| To analyze the effectiveness of the intervention focused on leisure as an occupation in people with MCI (follow-up: mean of six weeks) | ||||||||||||
| 1 | RCT | Serious | It is not serious | It is not serious | It is not serious | None | 28/28 (100%) | 0/28 (0.0%) | Not estimable | See comments | +++ Moderate | IMPORTANT |
| To analyze the effectiveness of the intervention focused on leisure as an occupation in people with MCI (follow-up: median of 12 years; assessed with Likert scale) | ||||||||||||
| 1 | RCT | Serious | It is not serious | It is not serious | It is not serious | None | 3544/3544 (100%) | 0/3544 (0.0%) | Not grouped | See comments | +++ Moderate | IMPORTANT |
| To analyze the effectiveness of the intervention focused on leisure as an occupation in people with MCI (follow-up: median of 1 year; assessed with multivariate regression model) | ||||||||||||
| 1 | RCT | It is not serious | It is not serious | It is not serious | It is not serious | None | 109/926 (11.8%) | 817/926 (88.2%) | Not estimable | ++++ High | IMPORTANT | |
| New outcome | ||||||||||||
| 1 | RCT | It is not serious | It is not serious | It is not serious | It is not serious | None | 134/201 (66.7%) | 67/201 (33.3.%) | Not estimable | See comments | ++++ High | IMPORTANT |
| To analyze the effectiveness of the intervention focused on leisure as an occupation in people with MCI (follow-up: median of 24 weeks; assessed with trend analysis) | ||||||||||||
| 1 | RCT | Serious | It is not serious | It is not serious | It is not serious | None | 14/29 (48.3%) | 14/29 (51.7%) | Not estimable | +++ Moderate | IMPORTANT | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vásquez-Carrasco, E.; Huenchuquen, C.; Ferrón, C.; Hernandez-Martinez, J.; Landim, S.F.; Helbig, F.; Carmine, F.; Valdés-Badilla, P.; Sandoval, C.; Gómez, C.S.; et al. Effectiveness of Leisure-Focused Occupational Therapy Interventions in Middle-Aged and Older People with Mild Cognitive Impairment: A Systematic Review. Healthcare 2024, 12, 2521. https://doi.org/10.3390/healthcare12242521
Vásquez-Carrasco E, Huenchuquen C, Ferrón C, Hernandez-Martinez J, Landim SF, Helbig F, Carmine F, Valdés-Badilla P, Sandoval C, Gómez CS, et al. Effectiveness of Leisure-Focused Occupational Therapy Interventions in Middle-Aged and Older People with Mild Cognitive Impairment: A Systematic Review. Healthcare. 2024; 12(24):2521. https://doi.org/10.3390/healthcare12242521
Chicago/Turabian StyleVásquez-Carrasco, Edgar, Camila Huenchuquen, Catalina Ferrón, Jordan Hernandez-Martinez, Síbila Floriano Landim, Fabiola Helbig, Florencia Carmine, Pablo Valdés-Badilla, Cristian Sandoval, Celia Sánchez Gómez, and et al. 2024. "Effectiveness of Leisure-Focused Occupational Therapy Interventions in Middle-Aged and Older People with Mild Cognitive Impairment: A Systematic Review" Healthcare 12, no. 24: 2521. https://doi.org/10.3390/healthcare12242521
APA StyleVásquez-Carrasco, E., Huenchuquen, C., Ferrón, C., Hernandez-Martinez, J., Landim, S. F., Helbig, F., Carmine, F., Valdés-Badilla, P., Sandoval, C., Gómez, C. S., & Moruno-Miralles, P. (2024). Effectiveness of Leisure-Focused Occupational Therapy Interventions in Middle-Aged and Older People with Mild Cognitive Impairment: A Systematic Review. Healthcare, 12(24), 2521. https://doi.org/10.3390/healthcare12242521