
Community-Based Interventions in People with Palliative Care Needs: An Integrative Review of Studies from 2017 to 2022

 ,
,  ,
,  ,
,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Design and Sources of Information
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
- Scientific papers published in the last 5 years, to focus on the latest evidence.
- Papers written in Spanish and English.
- Papers that include interventions applicable to patients in need of palliative care and at a community level.
- Papers directed towards both the paediatric and adult populations.
- Qualitative, descriptive and interventional studies, systematic and integrative reviews, meta-analyses and clinical cases.
- Research papers not applicable at a community level.
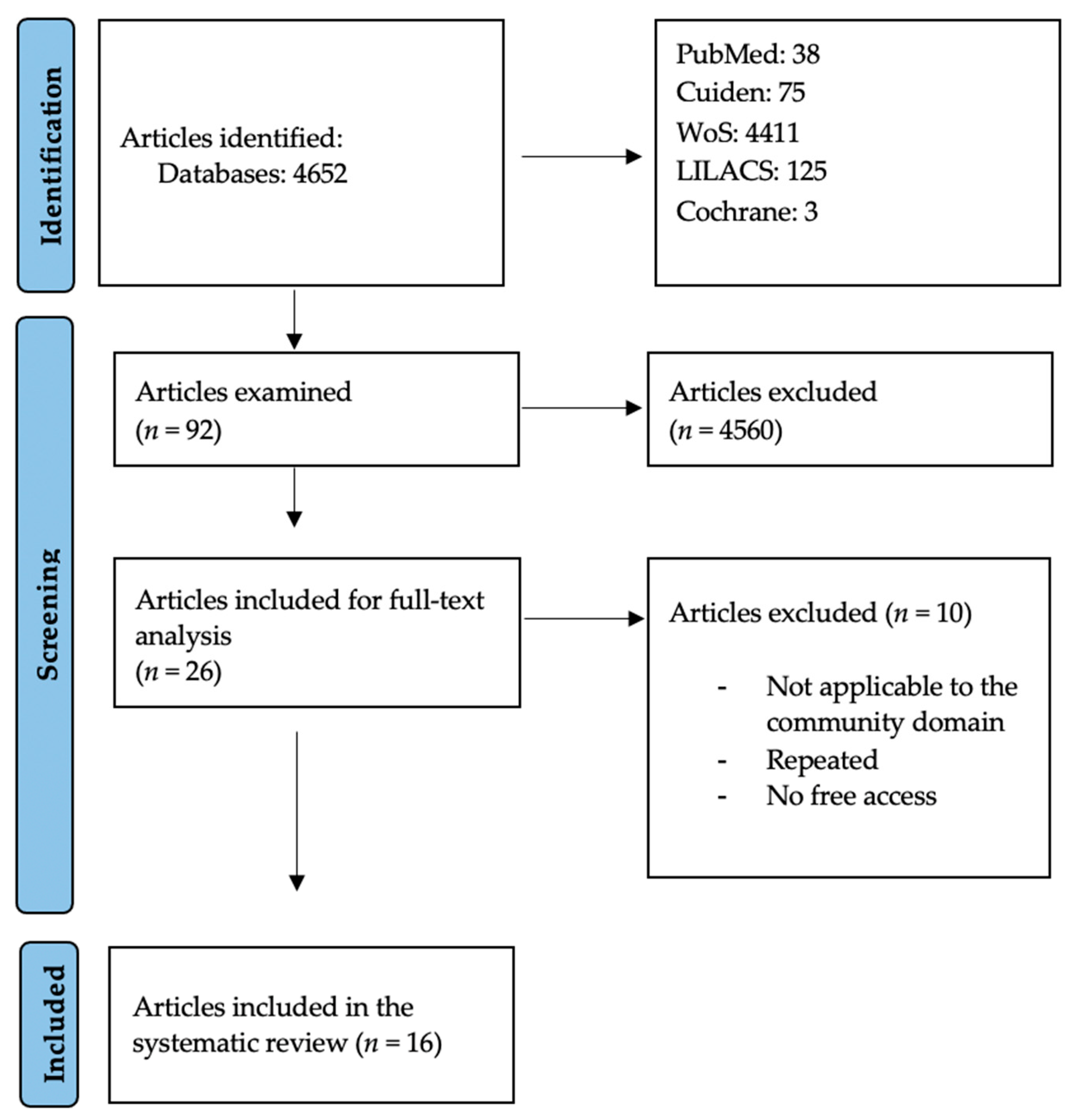
2.4. Study Selection
2.5. Studies Quality Assessment: Detection of Possible Biases
2.6. Results Extraction
2.7. Data Analysis
2.8. Ethics Approval and Consent to Participate
3. Results
3.1. Thematic Synthesis
3.1.1. Music Therapy
3.1.2. Laughter Therapy
3.1.3. Cognitive Interventions
3.1.4. Aromatherapy
3.1.5. Interdisciplinary Community-Based Teams
3.1.6. Advance Care Planning
3.2. Community, Volunteering, Telemedicine and Care Mapping
4. Discussion
4.1. Study Limitations
4.2. Implications for Nursing and Health Policies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Palliative Care. Available online: https://www.who.int/news-room/fact-sheets/detail/palliative-care (accessed on 15 July 2024).
- Blay, C.; Martori, J.C.; Limón, E.; Oller, R.; Vila, L.; Gómez-Batiste, X. Search for your 1%: Prevalence and mortality in a community cohort of people with advanced chronic disease and palliative needs. Atención Primaria 2019, 51, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Boudy, C.-A.; Bouchez, T.; Caprini, D.; Pourrat, I.; Munck, S.; Barbaroux, A. Home-based palliative care management: What are the useful resources for general practitioners? a qualitative study among GPs in France. BMC Fam. Pract. 2020, 21, 222. [Google Scholar] [CrossRef] [PubMed]
- General Law of Health. Organic Law 14/1986 (BOE 102 del 25-4-1986). Oficial State Gazette: Madrid. 1986. Available online: https://www.boe.es/buscar/act.php?id=BOE-A-1986-10499 (accessed on 15 July 2024).
- Law 16/2003, of May 28, 2003, on Cohesion and Quality of the National Health System. Official State Gazette. 2003. Available online: https://www.boe.es/buscar/pdf/2003/BOE-A-2003-10715-consolidado.pdf (accessed on 15 July 2024).
- Daban, F.; Pasarín, M.I.; Borrell, C.; Artazcoz, L.; Pérez, A.; Fernández, A.; Porthé, V.; Díez, E. Barcelona Salut als Barris: Twelve years’ experience of tackling social health inequalities through community-based interventions. Gac. Sanit. 2021, 35, 282–288. Available online: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0213-911 (accessed on 13 February 2022). [CrossRef] [PubMed]
- Law 33/2011, General Law of Public Health. Official State Gazette. 2011. Available online: https://www.boe.es/buscar/pdf/2011/BOE-A-2011-15623-consolidado.pdf (accessed on 15 July 2024).
- Law 4/2017, of March 9, on the Rights and Guarantees of Persons in the Process of Dying. Official State Gazette. 2017. Available online: https://www.boe.es/buscar/pdf/2017/BOE-A-2017-7178-consolidado.pdf (accessed on 15 July 2024).
- Chang, H.-T.; Lin, M.-H.; Kuo, W.-H.; Chen, C.-K.; Chen, T.-J.; Hwang, S.-J. Willingness of primary care staff to participate in compassionate community network and palliative care and the barriers they face: A mixed methods study. BMJ Open 2021, 11, e046961. [Google Scholar] [CrossRef] [PubMed]
- Larrañaga, I.; Millas, J.; Soto-Gordoa, M.; Arrospide, A.; San Vicente, R.; Irizar, M.; Lanzeta, I.; Mar, J. Impact of patient identification in a palliative care program in the Basque Country. Primary Care 2019, 51, 80–90. [Google Scholar] [CrossRef]
- Xing, B.; Liang, G.; Zhang, J.; Zhang, J.; Jiang, Z.; Miao, Q. Qualitative assessment of the intention of Chinese community health workers to implement advance care planning using theory of planned behavior. BMC Palliat. Care 2021, 20, 187. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Maetens, A.; Beernaert, K.; De Schreye, R.; Faes, K.; Annemans, L.; Pardon, K.; Deliens, L.; Cohen, J. Impact of home-based palliative care support on quality and costs of end-of-life care: A population-level matched cohort study. BMJ Open 2019, 9, e025180. [Google Scholar] [CrossRef] [PubMed]
- Pessalacia, J.D.R.; Silva, A.E.; Quadros Araújo, D.H.; De Lacerda, M.A.; Dos Santos, K.C. Caregivers’ experiences in palliative care and support networks. Rev. Enferm. UFPE Online 2018, 12, 2916. [Google Scholar] [CrossRef]
- Kelley, A.S.; Morrison, R.S. Palliative care for the seriously ill. N. Engl. J. Med. 2015, 373, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Meier, D.E.; Beresford, L. Palliative care’s challenge: Facilitating transitions of care. Health Aff. 2008, 27, 1347–1358. [Google Scholar] [CrossRef]
- Watanabe, S.M.; Fairchild, A.; Pituskin, E.; Borgersen, P.; Hanson, J.; Fassbender, K. Improving access to palliative care through interdisciplinary telehealth: A palliative care team project. J. Palliat. Med. 2013, 16, 703–707. [Google Scholar]
- PRISMA. Prisma-statement.org. Available online: https://prisma-statement.org//PRISMAStatement/FlowDiagram.aspx (accessed on 27 June 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cabello López, J.B. Critical Reading of Clinical Evidence, 1st ed.; Lectura Crítica de la Evidencia Clínica; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Choi, S.O.; Kim, S.N.; Shin, S.H.; Ryu, J.S.; Baik, J.W.; Kim, J.R.; Kim, N.H. Evaluation of Outcomes of the Busan Community-based Palliative Care Project in Korea. Asian Nurs. Res. (Korean Soc. Nurs. Sci.) 2018, 12, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Silva e Sousa, A.D.R.; Silva, L.F.; Paiva, E.D. Nursin interventions in palliative care in Pediatric Oncology: An integrative review. Rev. Bras. Enferm. 2019, 72, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Santos, F.R.; Pinto, S.; Pessalacia, J.D.R.; Luchesi, B.M.; Silva, L.A.; Marinho, M.R. Effects of activities with clowns in patients eligible for palliative care in primary health care. Rev. Bras. Enferm. 2021, 74, e20200431. [Google Scholar] [CrossRef] [PubMed]
- Vanderstichelen, S.; Houttekier, D.; Cohen, J.; Van Wesemael, Y.; Deliens, L.; Chambaere, K. Palliative care volunteerism across the healthcare system: A survey study. Palliat. Med. 2018, 32, 1233–1245. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hidalgo-Andrade, P.; Martínez-Rodríguez, S. Development of a cognitive-existential intervention to decrease compassion fatigue in formal caregivers. Interdiscip. Rev. Psicol. Cienc. Afines 2020, 37, 239–251. [Google Scholar] [CrossRef]
- Martins Pereira, S.; Araújo, J.; Hernández-Marrero, P. Towards a public health approach for palliative care: An action-research study focused on engaging a local community and educating teenagers. BMC Palliat. Care 2018, 17, 89. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Menon, S.; Kars, M.C.; Malhotra, C.; Campbell, A.V.; van Delden, J.J.M. Advance Care Planning in a Multicultural Family Centric Community: A Qualitative Study of Health Care Professionals’, Patients’, and Caregivers’ Perspectives. J. Pain Symptom Manag. 2018, 56, 213–221.e4. [Google Scholar] [CrossRef] [PubMed]
- Saurman, E.; Lyle, D.; Wenham, S.; Cumming, M. Un estudio de mapeo para guiar un enfoque paliativo de la atención. Rural Remote Health 2019, 19, 4625. [Google Scholar] [CrossRef] [PubMed]
- Nyashanu, M.; Ikhile, D.; Pfende, F. Exploring the efficacy of music in palliative care: A scoping review. Palliat. Support Care 2021, 19, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Linge-Dahl, L.M.; Heintz, S.; Ruch, W.; Radbruch, L. Humor Assessment and Interventions in Palliative Care: A Systematic Review. Front. Psychol. 2018, 9, 890. [Google Scholar] [CrossRef] [PubMed]
- Candy, B.; Armstrong, M.; Flemming, K.; Kupeli, N.; Stone, P.; Vickerstaff, V.; Wilkinson, S. The effectiveness of aromatherapy, massage and reflexology in people with palliative care needs: A systematic review. Palliat. Med. 2020, 34, 179–194. [Google Scholar] [CrossRef] [PubMed]
- Broese, J.M.; de Heij, A.H.; Janssen, D.J.; Skora, J.A.; Kerstjens, H.A.; Chavannes, N.H.; Engels, Y.; van der Kleij, R.M. Effectiveness and implementation of palliative care interventions for patients with chronic obstructive pulmonary disease: A systematic review. Palliat. Med. 2021, 35, 486–502. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bruera, E.; Yennurajalingam, S. Palliative care in advanced disease: How to improve quality of life. CA Cancer J. Clin. 2012, 62, 373–380. [Google Scholar] [CrossRef]
- Calton, B.A.; Rabow, M.W.; Branagan, L.; Dionne-Odom, J.N.; Parker Oliver, D.; Bakitas, M. Top ten tips palliative care clinicians should know about telepalliative care. J. Palliat. Med. 2019, 22, 981–985. [Google Scholar] [CrossRef] [PubMed]
- Lynch, S.; Wittenberg, E.; Knapp, C.; Yin, Z.; Breuer, C. Communication in pediatric palliative care: A review of existing literature. J. Support Oncol. 2013, 11, 10–19. [Google Scholar]
- Ernesto, C.-M.; Rodrigo, R.-T. Salud comunitaria: Una revisión de los pilares, enfoques, instrumentos de intervención y su integración con la atención primaria. J. Negat. No Posit. Results 2021, 6, 393–410. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S2529-850X2021000200011&lng=es (accessed on 13 July 2024). [CrossRef]

{kind=link}
| Database | Search String |
|---|---|
| PubMed Cuiden Web of Science Cochrane LILACS | (“Community participation” OR “training community” “OR “home interventions”) AND “palliative care” “Quality of life AND palliative care” (“leisure activities” OR “alternative therapy” OR “spiritual therapy”) AND “palliative care” |
| Authors and Year of Publication | Study Type | Participants | Intervention Types | Results | Conclusions | Study Quality as per CASPe Tool |
|---|---|---|---|---|---|---|
| Boudy (2020) [3] | Qualitative study | 21 family doctors | Community home-based care. | The resources used by family doctors: Internal resources: medical experience, skills and education. | The promotion of palliative home care should be a matter of social responsibility, capable of improving the quality of life and the experiences throughout the illness. Strengthening community resources and reducing exhaustion in healthcare providers could be more important than medical knowledge. | 8/10 items |
| External resources: healthcare services, assistance platforms and workers. Home palliative care can be both a burden and, at the same time, a satisfying and meaningful activity. This balance may be more important than medical education. | ||||||
| Larrañaga (2019) [10] | Comparative cross-sectional study | 1023 (year 2012) and 1142 (year 2015) patients requiring palliative care | Common clinical pathways between primary and secondary care, training courses, patient classification. | The likelihood of being identified as a palliative care user is 2.4 times higher when the patient identification programme is applied, through McNamara’s minimum estimation. | Correct patient identification reduces the number of hospitalisations and improves clinical activity. | 9/10 items |
| Xing (2021) [11] | Phenomenological qualitative study | 13 community health services centres | Advance care planning, multicultural care. | Some of the factors that negatively affect the quality of palliative care include Chinese legislation, insufficient allocation of human resources and training, and deep-rooted traditional beliefs about death. | Advance care planning can improve the doctor–patient relationship in terms of communication and quality of care. | 8/10 items |
| Choi (2018) [20] | Longitudinal and cross-sectional comparative study | 100 patients: 50 patients in the experimental group who received continuous palliative care and 50 patients in the control group who received outpatient palliative care. | Education on palliative care, home care, promotion of care. | The Community-based Palliative Care Project was composed of a multidisciplinary team and, by establishing community networks, improved the quality of life of patients and raised awareness of such type of care. | Patients who receive palliative care have lower levels of anxiety, a higher quality of life and reduced health costs. | 9/10 items |
| Maetens (2019) [12] | Cohort study | 17,674 patients, of whom 11,149 received home palliative care support in the last 720-15 days of life. | Multidisciplinary home care. | 56% of people who used home palliative care support died at home, compared to 13.8% of those who did not use home palliative care support. Costs are reduced by avoiding unnecessary diagnostic testing and hospitalisations by about EUR 1617. | The support and care provided by palliative home care teams reduce health costs and improve the quality of life for both patients and their caregivers. | 10/11 items |
| Silva and Sousa (2019) [21] | Integrative review of evidence | 18 articles | Music therapy, massage, physical exercise, toys, early nursing intervention to treat a specific symptom, nurse education and training. | It was highlighted that these interventions showed excellent results to treat pain, anxiety and fatigue. | The promotion of nursing training was suggested in order to equip nurses with more skills and provide them with necessary emotional support when they are handling palliative care. | 8/10 items |
| Santos (2021) [22] | Quasi-experiment study | 16 patients from two units of the Family Health Strategy, who fulfilled the assigned inclusion criteria | Laughter therapy with clowns. | Improvement in quality of life and social support. | Clown therapy can improve the quality of life and the social support of people who need palliative care at home. | 9/10 items |
| Vanderstichelen (2022) [23] | Qualitative study | 254 answers | Trained volunteers, training and education on palliative care. | Eighty per cent of associations have volunteers. The most important difficulty is finding new and competent volunteers. Thirty-three per cent of the associations offer compulsory training on palliative care and nursing. | Organizations are encouraged to invest in training and providing support to volunteers. These actions are carried out with the aim of providing palliative care in the community to those who need it, while also benefiting the volunteer. | 10/10 items |
| Hidalgo-Andrade (2020) [24] | Mixed-methods study | 84 formal caregivers | Existential and cognitive therapy. | Rational emotive therapy and logotherapy promote social skills and human strengths. | These interventions improve the quality of life of caregivers, which in turn results in a better quality of care and support for people in need of palliative care. | 8/11 items |
| Martins Pereira (2018) [25] | Mixed-methods study: action research study | 69 people from a community parish in Portugal | Awareness about palliative care, education, advancement and encouragement of compassionate communities. | The palliative care awareness programme was well received and left a positive message about community-based palliative care. | Educational intervention contributes to raising awareness about palliative care. Further research and interventions across all age groups are needed in order to promote engagement in care and to empower the population. | 9/11 items |
| Menon (2018) [26] | Qualitative study | 61 health providers, caregivers and patients | Establish advance care planning, empower families and people with palliative care needs, adapt advance planning to suit all cultures. | Healthcare providers, caregivers and patients were unaware of advance care planning and the legal framework governing it, but they were amazed about it and were willing to implement it. | Patients and caregivers need to be involved in decision-making and informed about it from the beginning of the illness, in order to improve the therapeutic relationship. | 7/10 items |
| Saurman (2019) [27] | Qualitative study | 15 interviews with health professionals | Community-based care, resource allocation and integration. | The importance of establishing networks between services and healthcare providers to improve communication and palliative care has been demonstrated. | Awareness of the network of care services and healthcare providers in the community can help health providers to improve the level of care they provide. | 8/10 items |
| Nyashanu (2021) [28] | Systematic review | 8 articles | Music therapy. | Music therapy improves quality of life, spirituality, happiness and hope, and reduces pain, anxiety and depression. | It was concluded that music therapy can be an effective psychosocial approach that positively impacts people’s biopsychosocial wellbeing. | 7/10 items |
| Linge-Dahl (2018) [29] | Systematic review | 13 studies | Humour, laughter therapy. | A positive effect of humour on patients, their caregivers and family has been recorded. | An appropriate use of humour can improve the quality of life of patients, their family and caregivers. Further studies to support this are needed. | 9/10 items |
| Candy (2020) [30] | Systematic review | 172 articles | Aromatherapy, reflexology and massage therapies. | The use of these interventions to reduce pain and anxiety, and to improve the quality of life, yielded some results, although these were inconclusive. Reduced sample size and number of studies. | The use of reflexology yielded good results. | 10/10 items |
| Broese (2021) [31] | Systematic review | 31 articles | Support with chronic obstructive disease and education about it, emotional management. | The patients widely accept these kinds of interventions thanks to the support for the care received. The main obstacle is the timing of referral. | Further high-quality studies are needed in order to assess the importance of palliative interventions in patients with chronic obstructive pulmonary disease. | 10/10 items |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vélez-López, A.; Carmona-Torres, J.M.; López-González, Á.; Laredo-Aguilera, J.A.; Callado-Pérez, D.; Rabanales-Sotos, J. Community-Based Interventions in People with Palliative Care Needs: An Integrative Review of Studies from 2017 to 2022. Healthcare 2024, 12, 1477. https://doi.org/10.3390/healthcare12151477
Vélez-López A, Carmona-Torres JM, López-González Á, Laredo-Aguilera JA, Callado-Pérez D, Rabanales-Sotos J. Community-Based Interventions in People with Palliative Care Needs: An Integrative Review of Studies from 2017 to 2022. Healthcare. 2024; 12(15):1477. https://doi.org/10.3390/healthcare12151477
Chicago/Turabian StyleVélez-López, Antonia, Juan Manuel Carmona-Torres, Ángel López-González, José Alberto Laredo-Aguilera, David Callado-Pérez, and Joseba Rabanales-Sotos. 2024. "Community-Based Interventions in People with Palliative Care Needs: An Integrative Review of Studies from 2017 to 2022" Healthcare 12, no. 15: 1477. https://doi.org/10.3390/healthcare12151477
APA StyleVélez-López, A., Carmona-Torres, J. M., López-González, Á., Laredo-Aguilera, J. A., Callado-Pérez, D., & Rabanales-Sotos, J. (2024). Community-Based Interventions in People with Palliative Care Needs: An Integrative Review of Studies from 2017 to 2022. Healthcare, 12(15), 1477. https://doi.org/10.3390/healthcare12151477